Psych · Consultation-liaison psychiatry
Cardiac psychiatry
Also known as Post-MI depression · Depression after acute coronary syndrome · Cardiovascular psychiatry · Psychocardiology · Heart failure depression · ACS-PTSD
Exam-exhaustive fellowship topic on cardiac psychiatry — post-ACS and CHD depression and anxiety, bidirectional risk and prognosis, landmark trials (SADHART, ENRICHD, CREATE, MIND-IT, SADHART-CHF, UPBEAT, MOSAIC), ACS-PTSD, ICD distress, Takotsubo interface, QTc-aware psychopharmacology, collaborative care and cardiac rehab. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Examiners reward named trials, honest hard-endpoint literacy, QTc-safe prescribing, and integrated rehab thinking rather than slogans that antidepressants "prevent reinfarction."[7][9][18]
Definition and classification
Cardiac psychiatry (psychocardiology) covers psychiatric morbidity and behavioural risk in ischaemic heart disease, heart failure, device therapy, and the interface with Takotsubo (stress) cardiomyopathy.[1][7][16] When major depressive features follow ACS and the cardiac illness is the aetiological context, DSM-5-TR framing is depressive disorder due to another medical condition; ICD-11 uses secondary mental or behavioural syndromes associated with diseases classified elsewhere.[1][7]
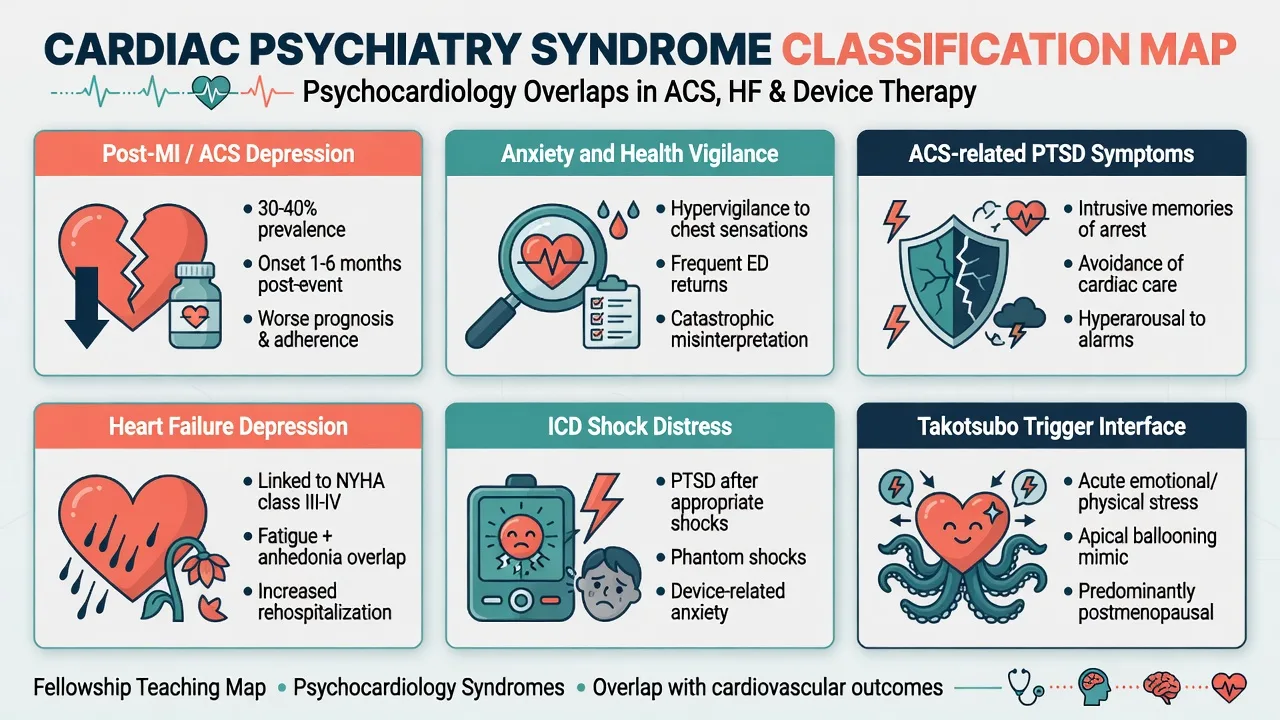
The working map includes post-ACS depression, anxiety, ACS-related PTSD symptoms, adjustment/demoralisation, ICD shock-related distress, and depression in HFrEF/HFpEF.[2][11][17] Takotsubo is a cardiac diagnosis with frequent emotional or physical precipitants — not a psychiatric label that replaces coronary work-up.[16]
| Clinical picture | Useful frame |
|---|---|
| Major depressive syndrome days–months after ACS | Depressive disorder due to another medical condition when causal link is clinical |
| Recurrent lifelong MDD with later CHD | Primary depression plus cardiac comorbidity — still treat both |
| Nightmares, re-experiencing the infarct, rehab avoidance | ACS-PTSD symptoms spectrum |
| Fatigue and anhedonia in HF | Depression vs pure HF symptom overlap — interview for psychological features |
| Anticipatory fear of ICD shocks | Device-related anxiety / trauma response |
| Acute LV dysfunction after bereavement | Takotsubo pathway first — psychiatry after stabilisation [7][16][17] |

Epidemiology and bidirectional risk
Frasure-Smith and colleagues' classic post-MI cohort showed depression as a significant predictor of 6-month cardiac mortality — the historical anchor examiners still expect.[3] In stable CAD, depression and anxiety predicted greater major adverse cardiac event risk over 2 years.[4] Meta-analyses by Barth (mortality in established CHD) and Nicholson (aetiologic and prognostic signals across large observational pools) support depression as clinically important while reminding candidates about residual confounding.[5][6]
AHA scientific statements synthesise screening, referral, and treatment recommendations (2008) and elevate depression as a risk factor for poor prognosis after ACS (2014).[1][2] Edmondson and colleagues' meta-analysis places clinically significant ACS-related PTSD symptoms in a moderately prevalent range with association to recurrence risk — use order-of-magnitude language, not false precision.[17]
Risk amplifiers: prior depression, greater cardiac severity and disability, low social support, non-adherence, substance use, sleep disruption, and socioeconomic stress.[2][7][18]
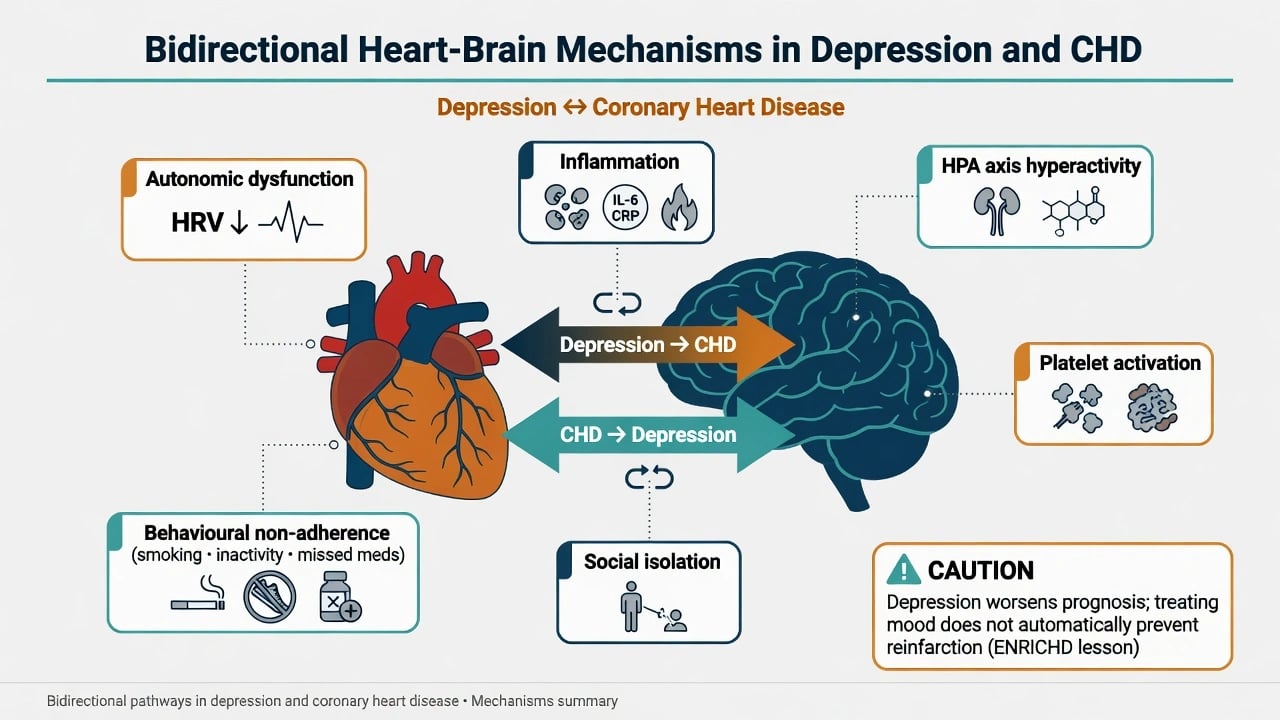
Mechanisms
Pathways are bidirectional: autonomic dysregulation (including reduced heart-rate variability), HPA-axis changes, inflammation and coagulation, endothelial dysfunction, and altered platelet reactivity sit alongside behavioural mediators — smoking, inactivity, diet, delayed help-seeking, and medication non-adherence.[7][18] ACS itself can act as a traumatic stressor producing fear conditioning, hyperarousal, and avoidance of exertion or hospitals.[17] Takotsubo registry data emphasise catecholamine-linked stress cardiomyopathy with emotional or physical triggers and female predominance among reported cases.[16]
Clinical presentations examiners expect
Post-ACS and CHD depression
Low mood, anhedonia, guilt, hopelessness, sleep and appetite change, and suicidality may be dismissed as "understandable" after infarction. Weight psychological depressive features and loss of engagement with rehab against pure somatic overlap from HF or deconditioning.[1][7][18]
Anxiety and health vigilance
Fear of recurrence, chest-pain catastrophising, and avoidance of exercise undermine cardiac rehab. Anxiety independently predicted events in stable CAD cohorts alongside depression.[4]
ACS-related PTSD symptoms
Re-experiencing the event, nightmares, hypervigilance, and avoidance are clinically important and associated with adverse cardiac signals in meta-analysis.[17]
Heart failure depression
Depression is common in HF and hard to separate from fatigue and dyspnoea. SADHART-CHF is the key trial literacy point (see management).[11]
ICD and device distress
Shock trauma, anticipatory anxiety, "phantom shocks," and body-image or role loss require device-clinic liaison, CBT approaches, and careful psychotropic choice if depression is comorbid.[7]
Takotsubo interface
Presentations mimic ACS; psychiatry contributes after medical stabilisation by mapping triggers, concurrent mood/anxiety disorders, and follow-up support without delaying coronary evaluation.[16]
Differential diagnosis
| Presentation | Prefer cardiac-psychiatric syndrome if… | Prefer alternative if… |
|---|---|---|
| Low mood week 2 post-MI | Anhedonia, guilt, SI, rehab withdrawal | Pure grief without depressive syndrome |
| Fatigue in HF | Depressive cognitions + functional withdrawal | Pure decompensated HF without mood features |
| Non-engagement | Anxiety/PTSD avoidance or depression | Pain, hypoxia, anaemia, sedation, delirium |
| New confusion on CCU | — | Delirium, infection, metabolic, stroke |
| Irritability | Mood episode or withdrawal | Hypoxia, retention, sleep debt, stimulant use |
| Discriminators | Tempo after ACS, collateral, adherence logs | Primary idiopathic syndrome only, no cardiac context [1][7][18] |
Challenge the exam myth that beta-blockers universally cause depression requiring automatic cessation of secondary prevention — review individually, treat depression on its merits, and protect evidence-based cardiology therapy unless a clear causal link and alternative exist.[1][7]
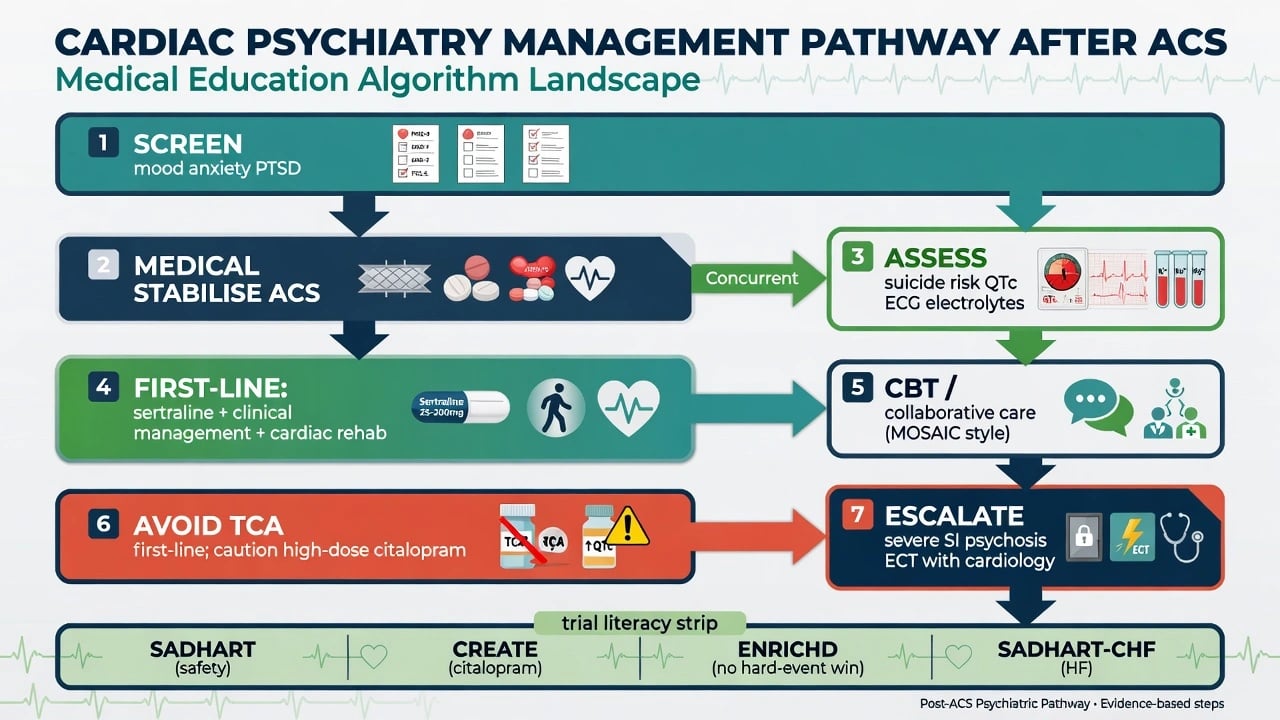
Assessment
Build a cardiac dossier: ACS phenotype, EF, devices (ICD/CRT), dual antiplatelet or anticoagulant regimen, antiarrhythmics, planned rehab, and prior psychiatric history.[1][2] Screen with PHQ-2/9 or HADS where useful; trial populations often used BDI — clinical interview remains the standard for major depression diagnosis.[1][18] Assess suicide risk, capacity for discharge and procedure consent, driving after ACS (local rules), substance use, sleep, and social support (ENRICHD's low perceived social support concept remains clinically useful even though the trial missed hard endpoints).[9][18] Screen for ACS-PTSD symptoms when presentations were terrifying or required resuscitation.[17]
Investigations
Before antidepressants in cardiac patients: ECG with QTc, electrolytes (especially sodium, potassium, magnesium), renal and hepatic function, and TSH when indicated.[1][8] Align with cardiology on recent arrhythmias and EF before QT-prolonging agents. Do not re-image the heart for psychiatry alone if the cardiology pathway is complete and the patient is stable.[1]
Acute and emergency management
Chest pain, arrhythmia, shock, and acute HF override psychiatric formulation.[1] For active suicidality: observation level, means restriction, and least-restrictive legal pathways under local law. Avoid heavy sedative loads that worsen delirium, respiratory status, and rehab participation.[18] Treat reversible medical drivers of agitation first; if short-term antipsychotic is required, use the lowest effective dose with QTc and fall monitoring.[1]
Definitive management and trial literacy
Antidepressants after ACS
SADHART randomised patients with major depression after ACS to sertraline versus placebo: sertraline was safe on cardiac measures and effective for recurrent depression in the eligible population — the fellowship first-line SSRI anchor after ACS.[8] Practical start: sertraline 25–50 mg oral daily, titrate toward 50–200 mg oral daily as tolerated, monitoring GI effects, hyponatraemia, bleeding with antithrombotics, sexual side effects, and rare QTc issues.[8][1]
CREATE (2×2 design) found citalopram superior to placebo for depression in CAD with clinical management, while interpersonal psychotherapy did not outperform clinical management alone — name this when asked about IPT after MI.[10] In older or QTc-vulnerable patients, many clinicians still prefer sertraline over high-dose citalopram/escitalopram given regulatory QTc warnings; if citalopram is used, respect dose ceilings and ECG context.[1][10]
MIND-IT found that an antidepressant treatment pathway after MI did not improve long-term depression status or cardiac prognosis at the population level — response heterogeneity and implementation matter; a nested mirtazapine RCT (Honig) supported efficacy and safety for post-MI depressive disorder in that substudy context.[12][13] Example when sedating antidepressant needed with cardiology agreement: mirtazapine 15 mg oral at night, titrate carefully (weight gain, sedation, rare agranulocytosis teaching point), not as universal first-line over SSRI.[13]
Avoid TCAs as first-line post-MI because of arrhythmia and overdose risk.[1][7]
Psychotherapy, exercise, collaborative care
ENRICHD treated depression and low social support after MI with CBT (plus antidepressant when indicated): psychosocial measures improved, but the primary composite of death or recurrent MI was not reduced — the defining hard-endpoint honesty examiners want.[9] UPBEAT showed supervised exercise and sertraline both reduced depressive symptoms versus placebo in CHD.[15] MOSAIC demonstrated that low-intensity collaborative care improved depression and anxiety after recent cardiac events.[14] Cardiac rehabilitation, smoking cessation, and adherence coaching are core psychiatric-relevant interventions, not optional extras.[1][18]
Heart failure
SADHART-CHF: sertraline was safe in significant HF but did not produce greater depression reduction than placebo — set expectations, optimise HF therapy, and intensify psychosocial/collaborative models rather than promising SSRI magic.[11]
Severe illness
Psychotic or melancholic depression, food/fluid refusal, or high suicide risk may need inpatient psychiatry and consideration of ECT with cardiology liaison (anaesthetic and arrhythmia risk counselling).[1][7]
Subtypes and high-yield scenarios
- Day 3 post-STEMI tearfulness with passive SI on dual antiplatelets — safety + SSRI planning + bleeding counselling.[8]
- Stable CAD clinic chronic depression with recurrent angina presentations — screen depression and adherence, not only stents.[4][18]
- HFrEF labelled "just the heart" — apply SADHART-CHF literacy and multimodal care.[11]
- Takotsubo after bereavement — medical first, then trigger and mood formulation.[16]
- ICD storm survivor avoiding leaving home — trauma-informed CBT and device-clinic partnership.[7][17]
- Request to stop all beta-blockers "because depression" — evidence-based challenge and mood treatment plan.[1]
Complications and pitfalls
Missing depression as "normal"; promising reinfarction prevention from antidepressants after ENRICHD; starting TCA or high-dose citalopram without QTc review; ignoring SSRI-antithrombotic bleeding; sedating non-engaged rehab patients; missing ACS-PTSD; automatic beta-blocker cessation.[1][8][9][17]
Prognosis and disposition
Depression after ACS worsens quality of life, adherence, and is linked to adverse cardiac prognosis signals in observational and AHA syntheses.[2][3][5] Treating depression improves psychiatric outcomes; hard cardiac event reduction is not consistently proven in large interventional trials — say that out loud in vivas.[9][12] Disposition links community mental health or GP collaborative care to cardiac rehab and secondary prevention follow-up; escalate for suicidality, psychosis, or dangerous non-adherence.[14][18]
Special populations
Older adults: hyponatraemia, falls, polypharmacy, lower citalopram ceilings.[1] Women: higher representation in Takotsubo series; peripartum cardiomyopathy is rare but high-stakes when depression coexists.[16] People with severe mental illness carry accelerated CVD risk — metabolic monitoring and primary prevention are dual duties of psychiatry.[7][18] Cultural safety and access barriers to rehab matter for Indigenous and diverse populations in ANZ practice and should be built into adherence and secondary-prevention planning alongside standard AHA-style screening and treatment pathways.[1][18]
Evidence, guidelines, and regional deltas
- AHA Lichtman 2008 advisory and 2014 poor-prognosis statement — core screening and risk framing.[1][2]
- SADHART / CREATE / ENRICHD / MIND-IT / SADHART-CHF / UPBEAT / MOSAIC — name endpoints correctly.[8][9][10][11][12][14][15]
- ANZ: adapt RANZCP mood guidance to cardiac safety (SSRI choice, QTc, bleeding) and local cardiac rehab / CL pathways under local mental health law when risk requires.[1][8]
- UK: map to NICE-style depression in chronic physical health problem framing plus cardiac rehab networks, with the same trial literacy (SADHART/ENRICHD/CREATE).[4][5][8]
- US: APA depression guidelines layered with AHA cardiac-specific statements on screening and poor-prognosis risk framing.[1][2]
ANZ practice emphasises CL integration with public cardiac rehab programmes and careful SSRI use on dual antiplatelets; US candidates should cite AHA statements by name; UK candidates should map to NICE chronic physical health depression pathways without inventing local cardiac psychiatry-only guidelines — the evidence spine remains SADHART safety, CREATE pharmacotherapy, and ENRICHD hard-endpoint honesty.[1][4][5][8]
Exam pearls
- SADHART = sertraline safety/efficacy after ACS depression — not a mortality megatrial win.[8]
- ENRICHD = psychosocial improvement without reduced death/recurrent MI.[9]
- CREATE = citalopram yes; IPT not superior to clinical management in that design.[10]
- SADHART-CHF = safety without depression superiority in HF.[11]
- Prefer sertraline when QTc risk is high; avoid TCA first-line post-MI.[1][8]
- ACS-PTSD is real and prognosis-relevant — screen when the story is traumatic.[17]
- Depression is an AHA-recognised poor-prognosis risk factor after ACS — treat it, integrate rehab, stay honest about hard endpoints.[2]
References
- [1]Lichtman JH, Bigger JT Jr, Blumenthal JA, et al. Depression and coronary heart disease: recommendations for screening, referral, and treatment: a science advisory from the American Heart Association Circulation, 2008.PMID 18824640
- [2]Lichtman JH, Froelicher ES, Blumenthal JA, et al. Depression as a risk factor for poor prognosis among patients with acute coronary syndrome: systematic review and recommendations: a scientific statement from the American Heart Association Circulation, 2014.PMID 24566200
- [3]Frasure-Smith N, Lespérance F, Talajic M Depression following myocardial infarction. Impact on 6-month survival JAMA, 1993.PMID 8411525
- [4]Frasure-Smith N, Lespérance F Depression and anxiety as predictors of 2-year cardiac events in patients with stable coronary artery disease Arch Gen Psychiatry, 2008.PMID 18180430
- [5]Barth J, Schumacher M, Herrmann-Lingen C Depression as a risk factor for mortality in patients with coronary heart disease: a meta-analysis Psychosom Med, 2004.PMID 15564343
- [6]Nicholson A, Kuper H, Hemingway H Depression as an aetiologic and prognostic factor in coronary heart disease: a meta-analysis of 6362 events among 146 538 participants in 54 observational studies Eur Heart J, 2006.PMID 17082208
- [7]Carney RM, Freedland KE Depression and coronary heart disease Nat Rev Cardiol, 2017.PMID 27853162
- [8]Glassman AH, O'Connor CM, Califf RM, et al. Sertraline treatment of major depression in patients with acute MI or unstable angina. JAMA, 2002.PMID 12169073
- [9]Berkman LF, Blumenthal J, Burg M, et al. Effects of treating depression and low perceived social support on clinical events after myocardial infarction: the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) Randomized Trial JAMA, 2003.PMID 12813116
- [10]Lespérance F, Frasure-Smith N, Koszycki D, et al. Effects of citalopram and interpersonal psychotherapy on depression in patients with coronary artery disease: the Canadian Cardiac Randomized Evaluation of Antidepressant and Psychotherapy Efficacy (CREATE) trial JAMA, 2007.PMID 17244833
- [11]O'Connor CM, Jiang W, Kuchibhatla M, et al. Safety and efficacy of sertraline for depression in patients with heart failure: results of the SADHART-CHF (Sertraline Against Depression and Heart Disease in Chronic Heart Failure) trial J Am Coll Cardiol, 2010.PMID 20723799
- [12]van Melle JP, de Jonge P, Honig A, et al. Effects of antidepressant treatment following myocardial infarction Br J Psychiatry, 2007.PMID 17541103
- [13]Honig A, Kuyper AM, Schene AH, et al. Treatment of post-myocardial infarction depressive disorder: a randomized, placebo-controlled trial with mirtazapine Psychosom Med, 2007.PMID 17846258
- [14]Huffman JC, Mastromauro CA, Beach SR, et al. Collaborative care for depression and anxiety disorders in patients with recent cardiac events: the Management of Sadness and Anxiety in Cardiology (MOSAIC) randomized clinical trial JAMA Intern Med, 2014.PMID 24733277
- [15]Blumenthal JA, Sherwood A, Babyak MA, et al. Exercise and pharmacological treatment of depressive symptoms in patients with coronary heart disease: results from the UPBEAT (Understanding the Prognostic Benefits of Exercise and Antidepressant Therapy) study J Am Coll Cardiol, 2012.PMID 22858387
- [16]Templin C, Ghadri JR, Diekmann J, et al. Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy N Engl J Med, 2015.PMID 26332547
- [17]Edmondson D, Richardson S, Falzon L, et al. Posttraumatic stress disorder prevalence and risk of recurrence in acute coronary syndrome patients: a meta-analytic review PLoS One, 2012.PMID 22745687
- [18]Whooley MA Depression and cardiovascular disease: healing the broken-hearted JAMA, 2006.PMID 16804154