Psych · Consultation-liaison psychiatry
Delirium
Also known as Acute confusional state · Acute encephalopathy · ICU delirium · Postoperative delirium · Delirium superimposed on dementia · Organic brain syndrome
Exam-exhaustive fellowship topic on delirium for consultation-liaison psychiatry — DSM-5-TR/ICD-11, CAM/4AT/CAM-ICU algorithms, hyperactive/hypoactive/mixed motor subtypes, predisposing and precipitating causes, medical work-up, multicomponent non-drug care first, limited antipsychotic role with trial evidence (MIND-USA, AID-ICU, Agar), ICU delirium and ABCDEF/PADIS, capacity, and discrimination from dementia and depression. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Delirium is the consultation-liaison and old-age psychiatry interface problem that still kills and disables. Fellowship examiners want named diagnostic algorithms, motor-subtype literacy (especially missed hypoactive disease), a cause-and-work-up system, non-drug first management with trial-honest pharmacotherapy, ICU and capacity interfaces, and clean discrimination from dementia and depression.[5][6][7]
Overview and definition
Delirium is a clinical syndrome of acute onset (hours to days), fluctuating course, and core disturbance of attention and awareness, with additional cognitive change (memory, orientation, language, visuospatial ability, or perception), attributable to a direct physiological consequence of a medical condition, substance intoxication or withdrawal, toxin, or multiple etiologies.[5][6][7]
It is not a primary psychiatric diagnosis in the sense of schizophrenia-spectrum illness. Psychiatry owns detection, risk, capacity, behavioural safety, and CL coordination while medicine treats the precipitants. Synonyms in stems include acute confusional state and acute encephalopathy; use delirium when the syndrome is present.[7]
Classification and diagnostic criteria
DSM-5-TR (operational summary)
| Criterion | Content |
|---|---|
| A | Disturbance in attention (reduced ability to direct, focus, sustain, shift) and awareness (reduced orientation to the environment) |
| B | Develops over a short period (usually hours to a few days), represents a change from baseline, and tends to fluctuate in severity during the day |
| C | An additional disturbance in cognition (memory, orientation, language, visuospatial ability, or perception) |
| D | Not better explained by another neurocognitive disorder and does not occur solely in the context of a severely reduced level of arousal (e.g. coma) |
| E | Evidence from history, examination, or laboratory findings that the disturbance is a direct physiological consequence of another medical condition, substance intoxication or withdrawal, toxin exposure, or multiple etiologies |
ICD-11 frames delirium similarly as an acute neurocognitive disturbance with impaired attention and awareness. European Delirium Association commentary emphasises that arousal remains clinically fundamental even when criteria language shifts toward cognitive features — profound drowsiness still signals the syndrome when the rest fits.[7]
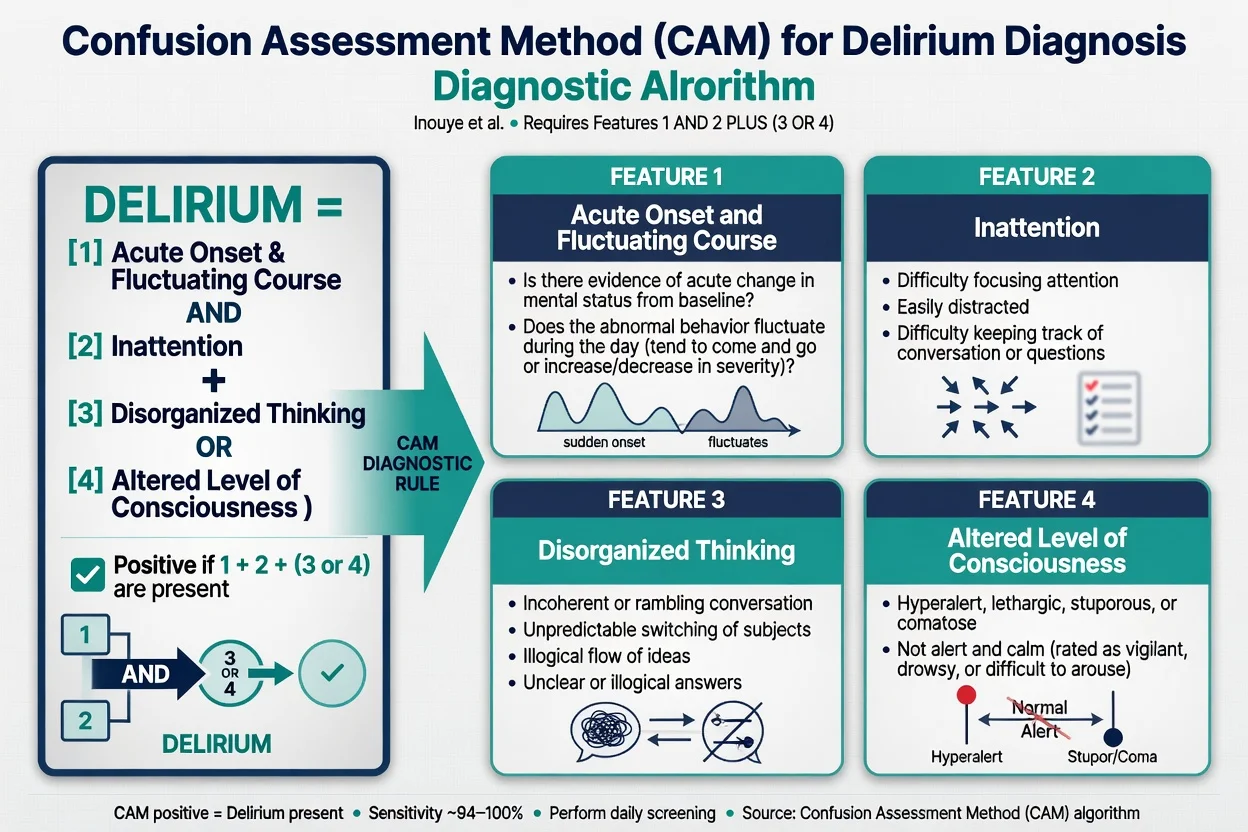
Confusion Assessment Method (CAM)
The CAM operationalises diagnosis for non-psychiatric clinicians. Positive when features 1 and 2 are present and either 3 or 4 is present: (1) acute onset and fluctuating course, (2) inattention, (3) disorganised thinking, (4) altered level of consciousness.[1]
Original validation showed high sensitivity and specificity for trained users; performance depends on training and on actually testing attention.[1] The 3D-CAM structures a roughly 3-minute interview with high accuracy against a reference standard.[17]
4AT (rapid screen)
Four items: Alertness, AMT4 (age, date of birth, place, current year), Attention (months of the year backward), and Acute change or fluctuating course. Score 4 or more suggests possible delirium and triggers full assessment; it is brief and usable at the bedside.[16]
Severity and ICU tools
- DRS-R-98: 13 severity items plus 3 diagnostic items — useful for severity tracking and research.[18]
- CAM-ICU: CAM adapted for non-verbal ICU patients after arousal assessment (RASS).[2][3]
- ICDSC: eight-item ICU checklist screening tool.[19]
Motor subtypes
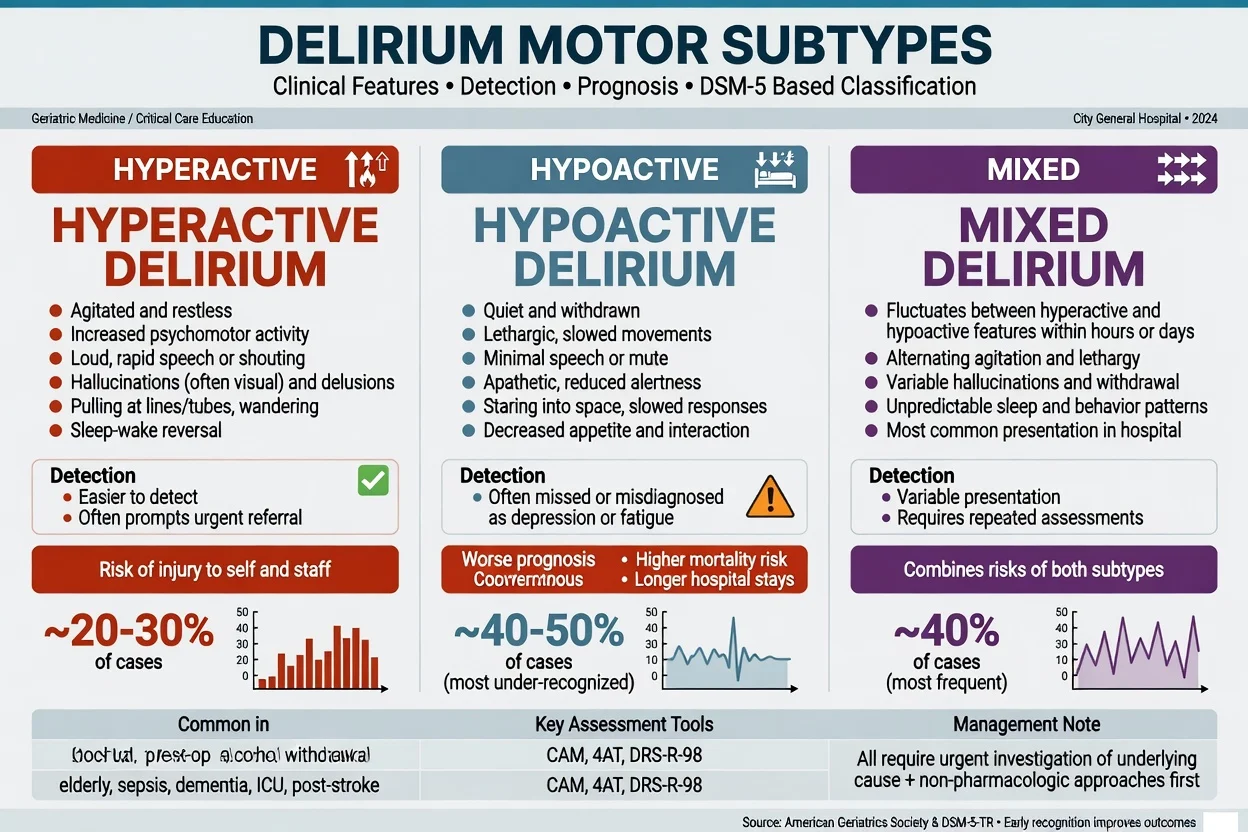
| Subtype | Bedside picture | Exam trap |
|---|---|---|
| Hyperactive | Agitation, restlessness, pulling lines, hallucinations | Over-treated with sedatives/antipsychotics without cause work-up |
| Hypoactive | Quiet, lethargic, poor intake, "good patient" | Most often missed; associated with worse prognosis in many series |
| Mixed | Fluctuates between hyper- and hypoactive | Most common longitudinal pattern in medical samples |
Meagher and colleagues showed motor subtype instability within an episode — reassess, do not lock a label for the whole admission.[20]
Epidemiology and risk factors
Predisposing factors (vulnerability): advanced age, pre-existing dementia or cognitive impairment, sensory impairment (vision/hearing), frailty, polypharmacy, prior delirium, alcohol use disorder, and reduced physiological reserve.[5][6][23]
Precipitating factors (Inouye model): a multifactorial load on a vulnerable brain. Classic precipitants include infection, medications (especially anticholinergics, benzodiazepines, opioids), surgery/anaesthesia, pain, hypoxia, metabolic disturbance, dehydration, constipation/urinary retention, stroke, and environmental disruption (ICU, sleep loss, restraints).[23][5][7]
Mnemonic frameworks examiners accept when expanded correctly include PINCH ME (Pain, Infection, Nutrition, Constipation, Hydration/Hypoxia, Medication, Environment) and I WATCH DEATH (Infection; Withdrawal; Acute metabolic; Trauma; CNS pathology; Hypoxia; Deficiencies; Endocrine; Acute vascular; Toxins/drugs; Heavy metals — the last is rare but keeps toxin breadth).[5][6]
Pathophysiology
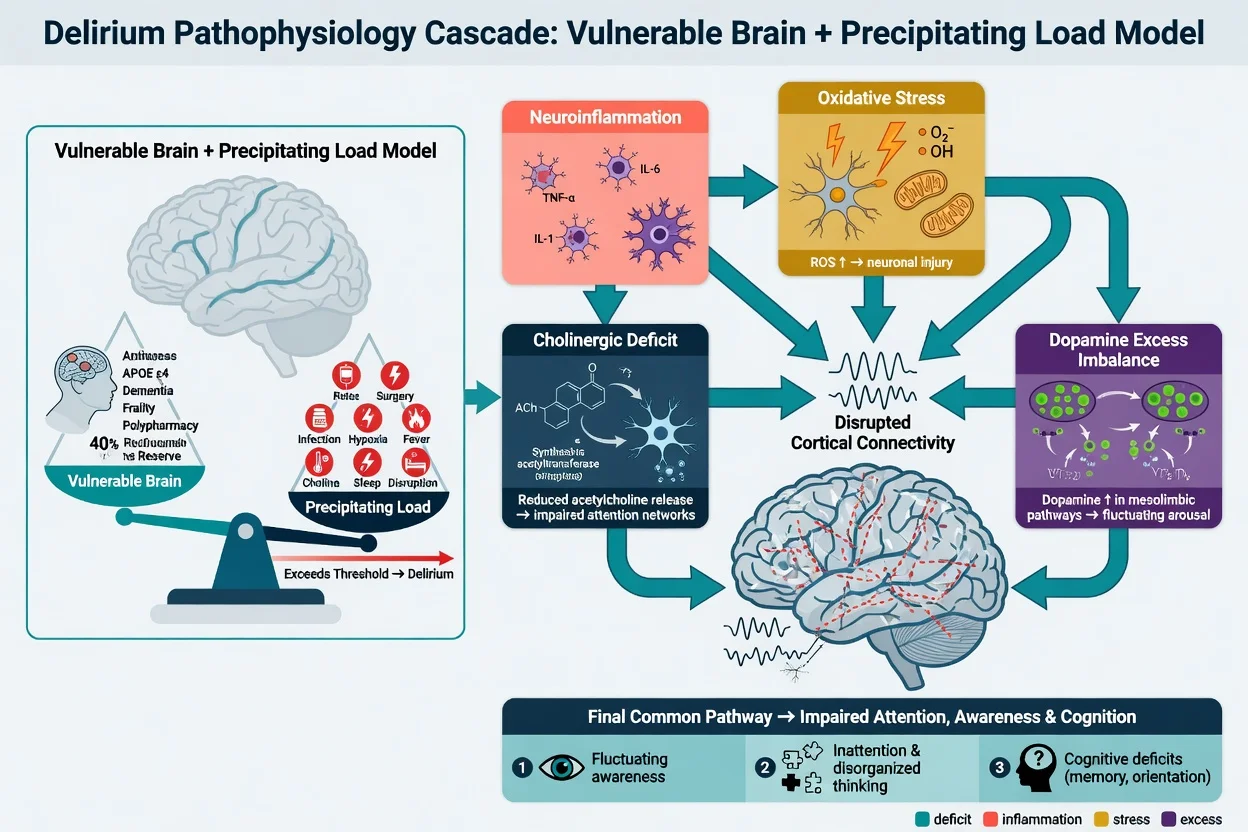
No single pathway explains all delirium. Converging models include neuroinflammation (cytokine signalling), cholinergic deficit, excess dopaminergic and other monoamine imbalance, oxidative stress and impaired cerebral metabolism, and disrupted large-scale cortical connectivity affecting attention and arousal networks. The practical clinical model is vulnerability times precipitating load — frail brains tip into delirium with smaller insults.[7][6][23]
Longer delirium duration associates with worse long-term cognition after critical illness (BRAIN-ICU cohort): treat duration as modifiable risk, not a cosmetic label.[14]
Clinical presentation
Tempo. Hours to a few days; family report of "not themselves last night" is gold. Fluctuation across a shift is typical — a single lucid moment does not exclude the diagnosis.[5][1]
Core signs. Inattention (cannot sustain conversation, fails simple attention tests), altered awareness (hypervigilant to drowsy), disorganised thinking, sleep-wake reversal, perceptual disturbance (especially visual hallucinations and illusions), emotional lability, and autonomic features when toxic/withdrawal causes dominate.[5][6][7]
Atypical and high-miss presentations. Hypoactive older adults labelled "depressed" or "tired"; postoperative "slow to wake"; palliative quiet confusion; delirium superimposed on dementia where baseline is already impaired — only serial comparison with collateral baseline detects change.[5][6]
Differential diagnosis — discriminators
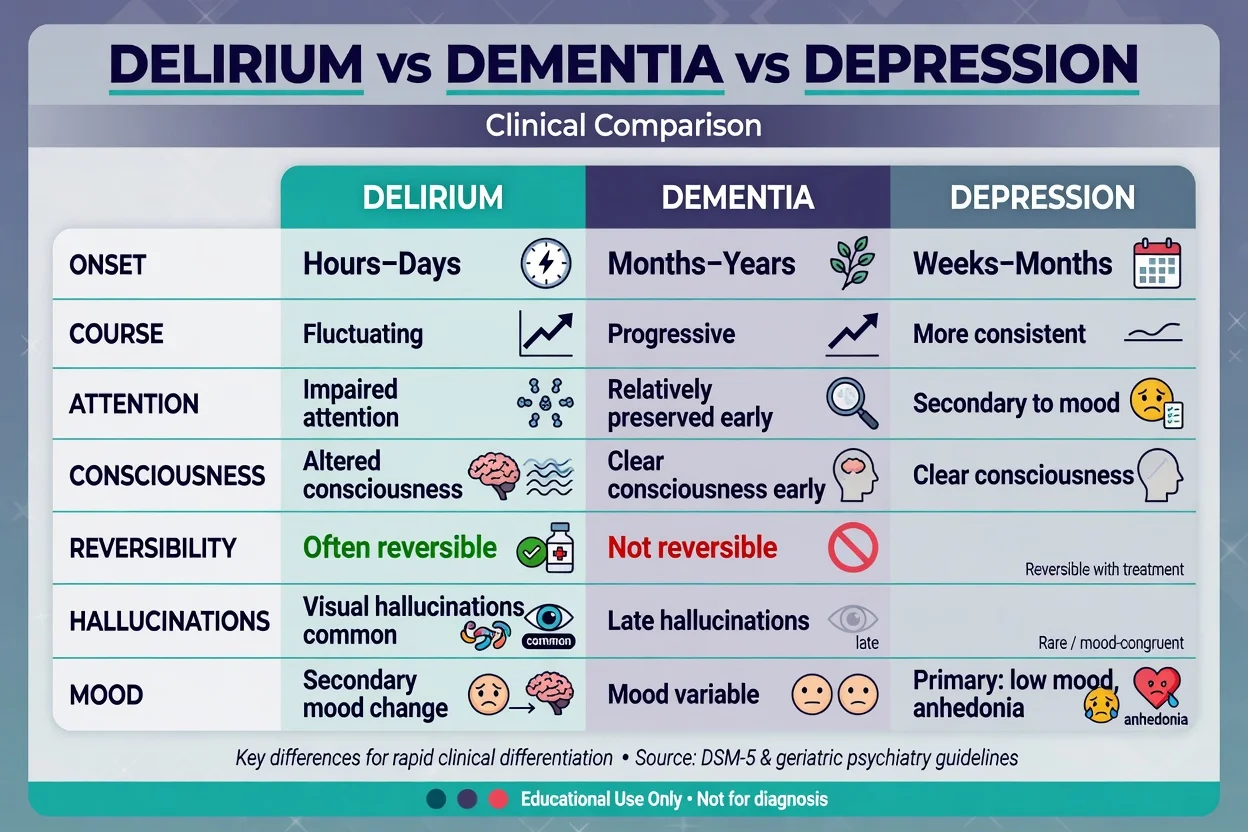
- Hours–days onset
- Fluctuating course
- Inattention prominent
- Altered awareness/arousal
- Often reversible if cause treated
- Visual hallucinations common
- Months–years onset
- Progressive course
- Attention relatively preserved early
- Clear consciousness early
- Not reversible as a rule
- Hallucinations later (e.g. DLB earlier)
- Weeks–months typical
- More consistent day-to-day
- Inattention secondary to mood/effort
- Clear consciousness
- Mood primacy (anhedonia, guilt)
- Pseudodementia can mimic but lacks fluctuating arousal
Also consider: primary psychotic disorder (clearer sensorium, non-medical course — still exclude organic first in late-onset or atypical cases); alcohol/benzodiazepine withdrawal (autonomic hyperactivity, tremor, seizures risk — benzodiazepine pathway); Wernicke encephalopathy (confusion, ophthalmoplegia, ataxia triad incomplete often); non-convulsive status epilepticus; autoimmune encephalitis; catatonia (Bush-Francis signs; benzodiazepine-responsive); manic agitation in known bipolar illness without medical precipitant.[5][6][7]
Clinical and bedside assessment
- ABCDE and immediate life threats (hypoxia, hypoglycaemia, sepsis, raised ICP signs).
- Collateral for baseline cognition and time of change.
- Structured screen: CAM, 3D-CAM, or 4AT on wards; CAM-ICU/ICDSC in ICU.[1][16][2][19]
- MSE: attention tests, orientation, thought form, perception, insight, risk (falls, violence, vulnerability, absconding).
- Medication reconciliation: anticholinergics, benzodiazepines, opioids, corticosteroids, antihistamines, dopamine agonists/antagonists, new starts and withdrawals.
- Capacity for each specific decision (below).
- Legal/least-restrictive framework under local mental health and guardianship law — state principles; do not invent foreign section numbers.[5][6]
Investigations
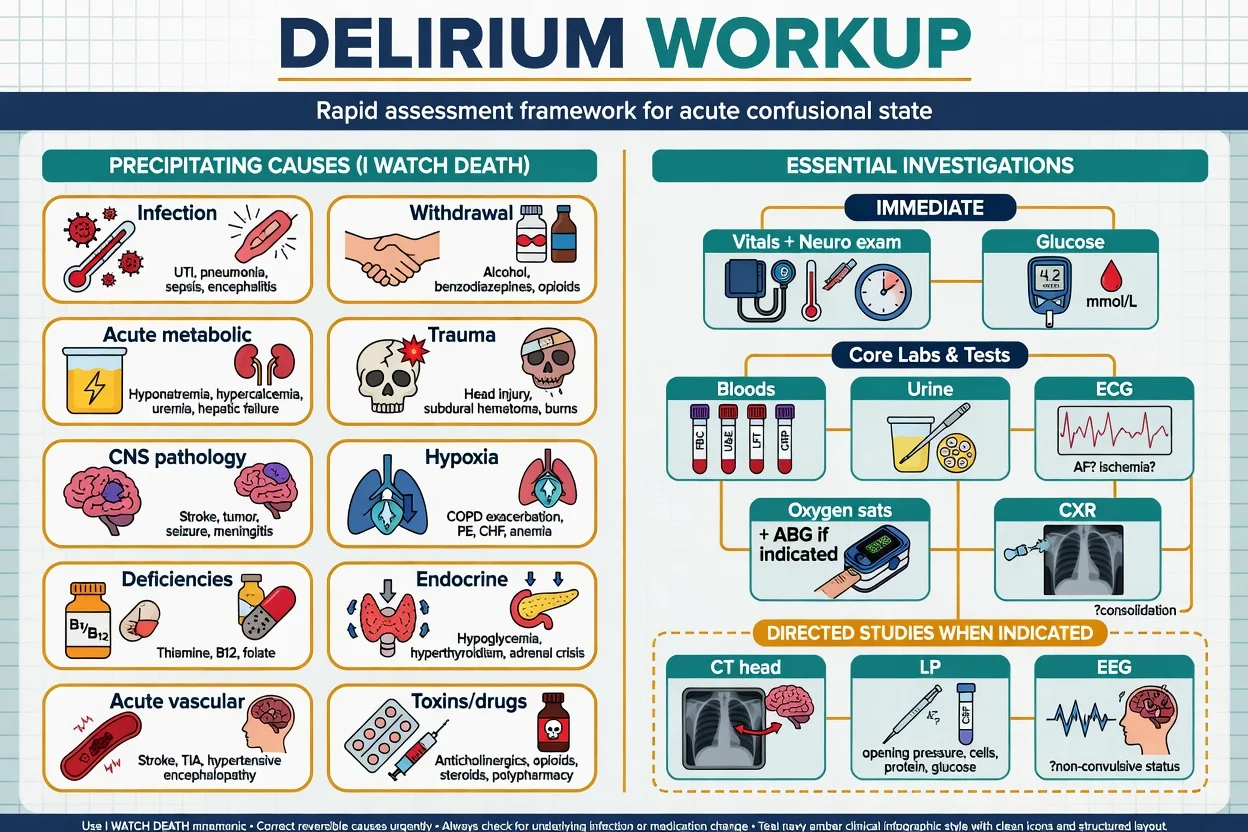
| Tier | Tests | When |
|---|---|---|
| Immediate | Vitals, capillary glucose, SpO2, ECG | All |
| Core bloods | FBC, U&E, Ca/Mg/PO4, LFT, CRP, glucose | All |
| Common directed | Urinalysis/culture, CXR, blood cultures, ABG/VBG | Infection/respiratory/metabolic clues |
| Metabolic/endocrine | TFT, B12/folate, ammonia if indicated | Cognitive risk, unexplained |
| Neuro when indicated | CT/MRI (focal signs, trauma, anticoagulation, new seizure), LP (meningitis/encephalitis), EEG (NCSE) | Neurological red flags |
| Tox | Directed toxicology, drug levels (e.g. digoxin, lithium, anticonvulsants) | Exposure history |
Treat the probable cause in parallel with testing. Normal CT does not exclude delirium.[5][6]
Management — resuscitation
Immediate bundle: oxygen and airway protection as needed; correct hypoglycaemia; broad sepsis pathway when indicated; stop or minimise deliriogenic drugs; treat severe pain; bladder scan for retention; relieve constipation; ensure hearing aids and glasses; safe environment with continuous observation if high risk; thiamine (parenteral) when malnutrition or alcohol risk before prolonged carbohydrate loads; if alcohol or benzodiazepine withdrawal, use a benzodiazepine protocol plus thiamine — not antipsychotic monotherapy.[5][6][24]
Management — definitive and stepwise
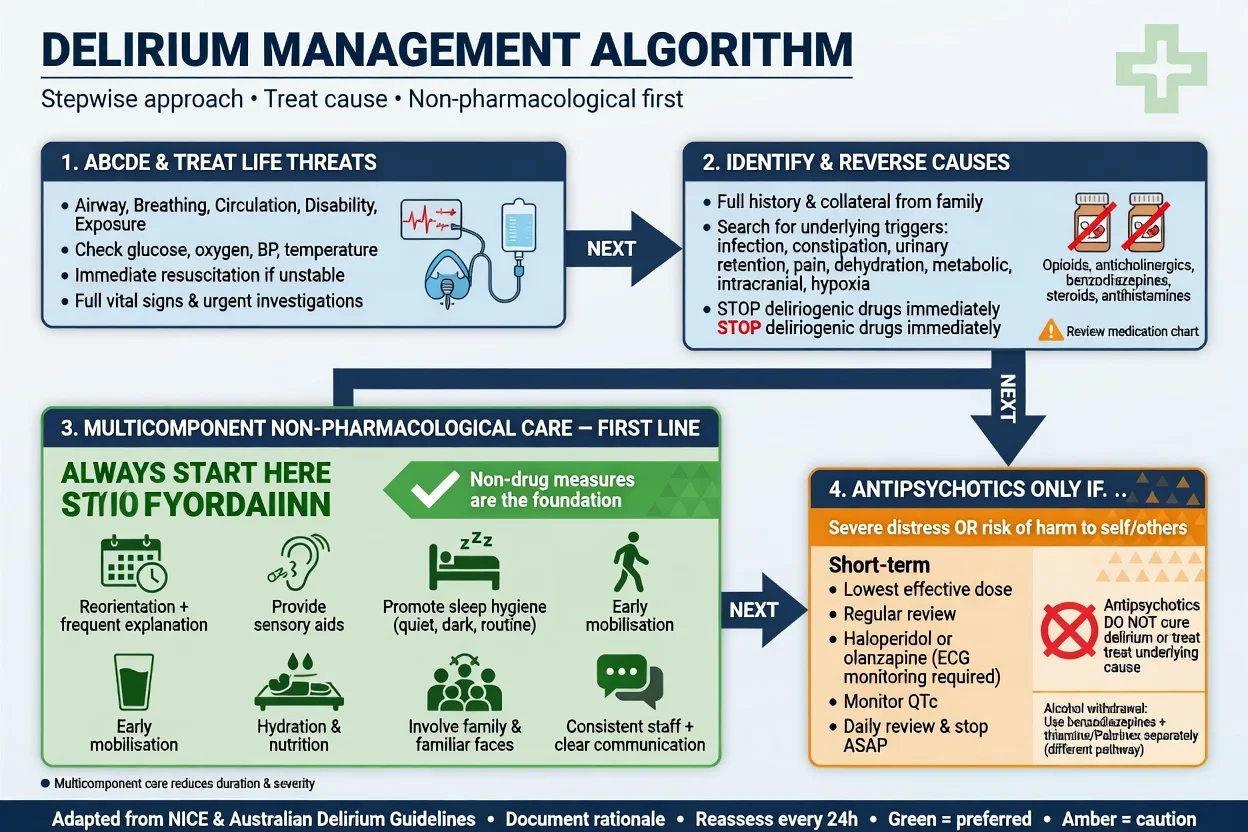
Non-pharmacological care is first-line
The Yale/HELP multicomponent model targets cognitive orientation, sleep, mobility, vision/hearing, and hydration. Inouye and colleagues showed reduced delirium incidence in hospitalised older adults with a structured multicomponent intervention.[4] Meta-analyses support multicomponent non-pharmacological strategies and HELP programme effectiveness for prevention and related outcomes.[21][22]
Practical ward package examiners expect: reorientation (clocks, calendars, name boards), family presence, day-night lighting, minimise overnight interruptions, early mobilisation, sensory aids, hydration and nutrition, avoid unnecessary catheters and restraints, constipation and retention protocols, and medication review.[4][5][6][21]
Pharmacotherapy — limited role
Antipsychotics do not treat delirium as a disease. Systematic reviews do not support routine antipsychotic prevention or treatment as primary therapy.[11][12] Landmark trials:
- MIND-USA (2018): in ICU patients with hypoactive or hyperactive delirium, haloperidol and ziprasidone did not significantly alter the number of days alive without delirium or coma versus placebo.[8]
- AID-ICU (2022): IV haloperidol did not improve days alive and out of hospital versus placebo in ICU delirium.[9]
- Agar et al. (2017): in palliative care, risperidone and oral haloperidol were associated with worse delirium symptom scores than placebo and more extrapyramidal effects.[10]
- Cochrane (Burry 2018): insufficient evidence that antipsychotics treat delirium in non-ICU hospitalised patients.[11]
When a short-term antipsychotic is still considered: severe agitation or distress posing imminent danger to self/others after non-drug measures and cause-directed care, and when not better explained by untreated pain, hypoxia, retention, or withdrawal. Use the lowest effective dose for the shortest time, review daily, and document target symptoms (safety/distress — not "cure confusion").[6][13]
Illustrative starting ranges used in geriatric practice (always check local formulary, ECG/QTc, EPS risk, and product information; start at the bottom of the range in frailty): haloperidol 0.25–0.5 mg PO/IM; olanzapine 2.5–5 mg PO (or IM where licensed/protocolised); quetiapine 12.5–25 mg PO — with QTc/EPS monitoring, avoid IM olanzapine plus parenteral benzodiazepines, and never use antipsychotic monotherapy for alcohol withdrawal.[6]
Avoid benzodiazepines for non-withdrawal delirium (worsen confusion) except for alcohol/BZD withdrawal, seizures, or selected palliative terminal distress pathways under specialist guidance.[5][6][24]
ANZ practice aligns with multicomponent prevention, cause treatment, and restricted antipsychotic use; follow local health-service delirium pathways, medication safety alerts, and jurisdiction-specific mental health / guardianship statutes for detention and substitute decision-making. Do not quote invented section numbers across states.[4][6]
Specific subtypes and scenarios
ICU delirium
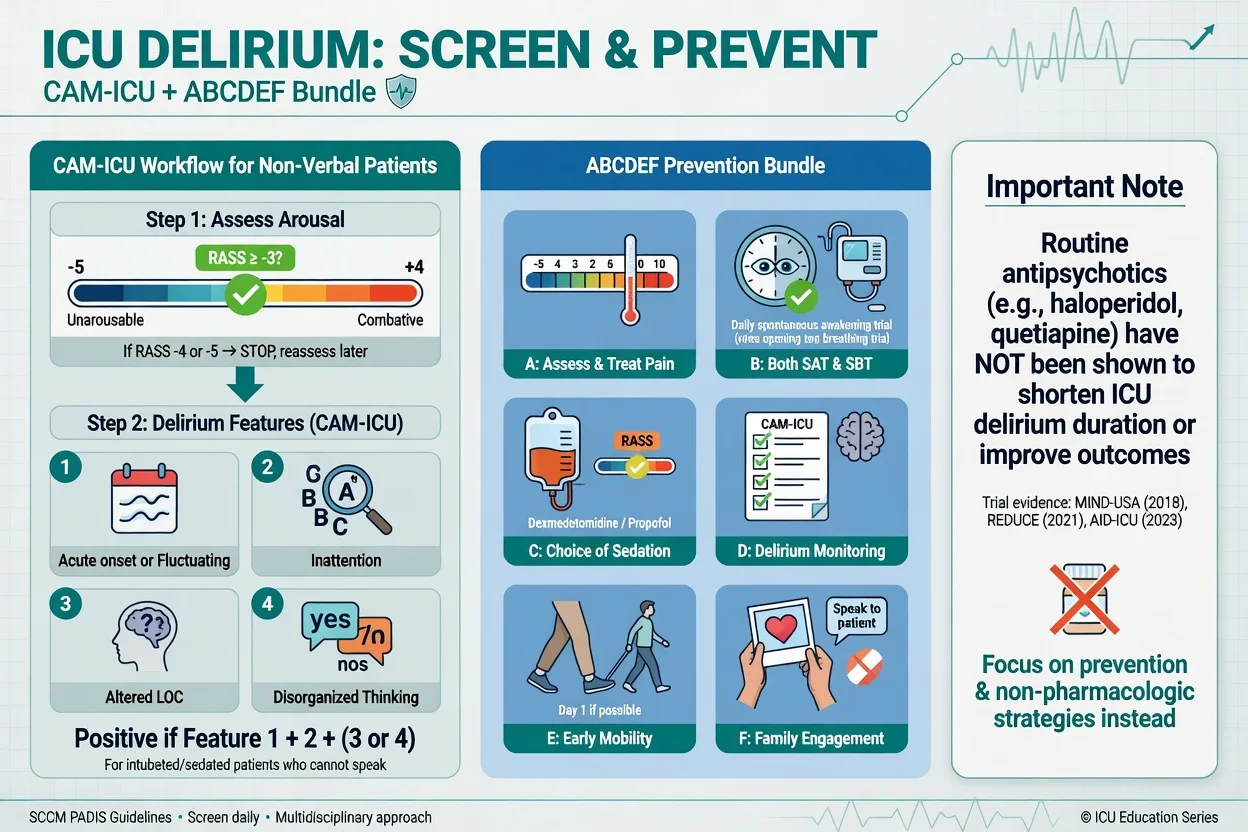
PADIS (2018) addresses pain, agitation/sedation, delirium, immobility, and sleep. Prevention leans on the ABCDEF bundle: Assess/treat pain; Both SAT and SBT; Choice of analgesia and sedation; Delirium monitoring; Early mobility; Family engagement. Prefer light sedation when safe; monitor with CAM-ICU or ICDSC.[13][2][19] MIND-USA and AID-ICU reshape viva answers: do not claim routine antipsychotics shorten ICU delirium.[8][9]
Postoperative delirium
Common in older surgical patients. Prevention: avoid deep unnecessary sedation, minimise benzodiazepines, optimise analgesia, early mobilisation, sensory aids, and geriatric co-management per AGS-style recommendations.[24][5]
Delirium superimposed on dementia (DSD)
Harder to detect. Require collateral baseline, serial CAM/4AT, and a low threshold for medical work-up when function drops acutely. Do not attribute every change to "progression of dementia."[5][6]
Palliative and terminal delirium
Treat reversible contributors when consistent with goals of care. For distressing terminal agitation, specialised palliative pathways apply; Agar trial cautions against assuming antipsychotics improve delirium scores in advanced illness.[10]
Alcohol withdrawal delirium
Distinct pathway: long-acting benzodiazepines titrated to symptoms, high-dose thiamine, electrolyte repletion, monitoring for seizures and Wernicke. Antipsychotics are adjuncts for severe perceptual disturbance only after benzos — never monotherapy.[5][6]
Complications and pitfalls
Classic pitfalls: missed hypoactive delirium; labelling as primary "psychosis" without medical work-up; benzodiazepines for non-withdrawal delirium; high-dose antipsychotics without non-drug care; physical restraint without de-escalation; missed Wernicke encephalopathy; capacity and discharge errors; ignoring sensory impairment and sleep disruption; and assuming a normal CT excludes organic disease.[5][6][12]
Prognosis and disposition
Delirium is often reversible if precipitants reverse, but recovery of cognition may lag medical recovery by days to weeks. Witlox meta-analysis: independent associations with mortality, institutionalisation, and dementia after discharge.[15] BRAIN-ICU: longer delirium linked to worse global cognition and executive function at 3 and 12 months.[14]
Disposition plan: treat causes to completion, fall-prevention, medication deprescribing, cognitive follow-up (especially new impairment), carer education on fluctuating course, and step-down geriatric/CL review when indicated.[5][6]
Special populations
Older adults have the highest prevalence — start low and go slow on any drug. In dementia, prioritise DSD detection with collateral. ICU care uses CAM-ICU, light sedation, and ABCDEF. Postoperative/frailty care centres on multicomponent prevention. Palliative care is goals-of-care guided with evidence-humble antipsychotics. Youth delirium is rarer but still medical-first. In pregnancy, treat the underlying cause with obstetric medicine involvement and reproductive-safety constraints on drugs.[5][6][13][24][10]
Evidence, guidelines, and regional differences
| Landmark | Message for viva |
|---|---|
| Inouye multicomponent RCT (1999) | Prevention works with structured non-drug care |
| HELP meta-analyses | Programmatic multicomponent care is effective |
| MIND-USA (2018) | ICU haldol/ziprasidone ≠ shorter delirium vs placebo |
| AID-ICU (2022) | ICU IV haldol ≠ better days alive out of hospital |
| Agar (2017) | Palliative risperidone/haloperidol not better than placebo for symptoms |
| Neufeld / Burry reviews | No support for routine antipsychotic Rx/prevention |
| PADIS 2018 | Bundle-based ICU prevention and monitoring |
| AGS postoperative guideline | Multicomponent prevention; limited antipsychotics |
Capacity, risk, and the CL role
Capacity is decision-specific and time-specific. Delirium commonly impairs understanding, retention, weighing, and communication for complex decisions (self-discharge, refusing IV antibiotics, financial acts). Document: the decision, information given, functional abilities demonstrated, and fluctuating course (reassess when lucid). Use least-restrictive emergency treatment principles under local law; involve substitute decision-makers when criteria met. Risk assessment covers falls, violence, sexual vulnerability, absconding, and self-harm while confused.[5][6]
CL psychiatry adds: syndrome confirmation, differential refinement, medication rationalisation, behavioural plan, capacity opinions, family communication, and liaison when mental health legislation is considered.[5][6]
Exam pearls
CAM+
Exam traps: hypoactive disease is the most missed presentation; antipsychotics are not disease-modifying; alcohol withdrawal is not a primary antipsychotic pathway; capacity can be lost even if the patient "agrees cheerfully"; and PINCH ME / I WATCH DEATH mnemonics only score if expanded accurately.[1][5][6][8]
References
- [1]Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the confusion assessment method. A new method for detection of delirium Ann Intern Med, 1990.PMID 2240918
- [2]Ely EW, Inouye SK, Bernard GR, et al. Evaluation of delirium in critically ill patients: validation of the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) Crit Care Med, 2001.PMID 11445689
- [3]Ely EW, Margolin R, Francis J, et al. Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU) JAMA, 2001.PMID 11730446
- [4]Inouye SK, Bogardus ST Jr, Charpentier PA, et al. A multicomponent intervention to prevent delirium in hospitalized older patients N Engl J Med, 1999.PMID 10053175
- [5]Marcantonio ER Delirium in Hospitalized Older Adults N Engl J Med, 2017.PMID 29020579
- [6]Oh ES, Fong TG, Hshieh TT, et al. Delirium in Older Persons: Advances in Diagnosis and Treatment JAMA, 2017.PMID 28973626
- [7]Wilson JE, Mart MF, Cunningham C, et al. Delirium Nat Rev Dis Primers, 2020.PMID 33184265
- [8]Girard TD, Exline MC, Carson SS, et al. Haloperidol and Ziprasidone for Treatment of Delirium in Critical Illness N Engl J Med, 2018.PMID 30346242
- [9]Andersen-Ranberg NC, Poulsen LM, Perner A, et al. Haloperidol for the Treatment of Delirium in ICU Patients N Engl J Med, 2022.PMID 36286254
- [10]Agar MR, Lawlor PG, Quinn S, et al. Efficacy of Oral Risperidone, Haloperidol, or Placebo for Symptoms of Delirium Among Patients in Palliative Care: A Randomized Clinical Trial JAMA Intern Med, 2017.PMID 27918778
- [11]Burry L, Mehta S, Perreault MM, et al. Antipsychotics for treatment of delirium in hospitalised non-ICU patients Cochrane Database Syst Rev, 2018.PMID 29920656
- [12]Neufeld KJ, Yue J, Robinson TN, et al. Antipsychotic Medication for Prevention and Treatment of Delirium in Hospitalized Adults: A Systematic Review and Meta-Analysis J Am Geriatr Soc, 2016.PMID 27004732
- [13]Devlin JW, Skrobik Y, Gélinas C, et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU Crit Care Med, 2018.PMID 30113379
- [14]Pandharipande PP, Girard TD, Jackson JC, et al. Long-term cognitive impairment after critical illness N Engl J Med, 2013.PMID 24088092
- [15]Witlox J, Eurelings LS, de Jonghe JF, et al. Delirium in elderly patients and the risk of postdischarge mortality, institutionalization, and dementia: a meta-analysis JAMA, 2010.PMID 20664045
- [16]Bellelli G, Morandi A, Davis DH, et al. Validation of the 4AT, a new instrument for rapid delirium screening: a study in 234 hospitalised older people Age Ageing, 2014.PMID 24590568
- [17]Marcantonio ER, Ngo LH, O'Connor M, et al. 3D-CAM: derivation and validation of a 3-minute diagnostic interview for CAM-defined delirium: a cross-sectional diagnostic test study Ann Intern Med, 2014.PMID 25329203
- [18]Trzepacz PT, Mittal D, Torres R, et al. Validation of the Delirium Rating Scale-revised-98: comparison with the delirium rating scale and the cognitive test for delirium J Neuropsychiatry Clin Neurosci, 2001.PMID 11449030
- [19]Bergeron N, Dubois MJ, Dumont M, et al. Intensive Care Delirium Screening Checklist: evaluation of a new screening tool Intensive Care Med, 2001.PMID 11430542
- [20]Meagher DJ, Leonard M, Donnelly S, et al. A longitudinal study of motor subtypes in delirium: frequency and stability during episodes J Psychosom Res, 2012.PMID 22325705
- [21]Hshieh TT, Yue J, Oh E, et al. Effectiveness of multicomponent nonpharmacological delirium interventions: a meta-analysis JAMA Intern Med, 2015.PMID 25643002
- [22]Hshieh TT, Yang T, Gartaganis SL, et al. Hospital Elder Life Program: Systematic Review and Meta-analysis of Effectiveness Am J Geriatr Psychiatry, 2018.PMID 30076080
- [23]Inouye SK, Charpentier PA Precipitating factors for delirium in hospitalized elderly persons. Predictive model and interrelationship with baseline vulnerability JAMA, 1996.PMID 8596223
- [24]American Geriatrics Society Expert Panel on Postoperative Delirium in Older Adults American Geriatrics Society abstracted clinical practice guideline for postoperative delirium in older adults J Am Geriatr Soc, 2015.PMID 25495432