Psych · Consultation-liaison psychiatry
Dementia and major neurocognitive disorder
Also known as Major neurocognitive disorder · Major NCD · Dementia · Alzheimer disease dementia · Vascular dementia · Dementia with Lewy bodies · Frontotemporal dementia · BPSD
Exam-exhaustive fellowship topic on dementia and major neurocognitive disorder — DSM-5-TR and ICD-11 nosology, mild versus major NCD, Alzheimer/vascular/DLB/FTD subtypes, assessment (MMSE, MoCA, NPI, collateral), delirium differential, BPSD and DICE framework, cholinesterase inhibitors and memantine with doses, antipsychotic mortality black-box caution (CATIE-AD, DART-AD, Schneider), capacity (Appelbaum), and disposition. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Dementia remains a high-stakes fellowship topic because examiners test nosology, subtype discrimination, delirium safety, BPSD judgement, cognitive-enhancer pharmacology, and capacity. The psychiatry registrar who only memorises "start donepezil" fails; the candidate who formulates aetiology, risk, and least-restrictive care passes.[9][28]
Overview and definition
In DSM-5-TR, major neurocognitive disorder (major NCD) requires: significant decline from a previous level of performance in one or more cognitive domains (complex attention, executive function, learning and memory, language, perceptual-motor, or social cognition); interference with independence in everyday activities; not exclusively in the context of delirium; and not better explained by another mental disorder. Severity is mild, moderate, or severe by functional dependence.[1][14]
Mild NCD (aligned with the clinical concept of mild cognitive impairment) is modest decline that does not interfere with independence, though compensatory strategies and greater effort may be required. Petersen and colleagues classically characterised amnestic MCI as a transitional state with elevated conversion risk to dementia — the independence hinge remains the practical clinical cut.[14]
ICD-11 still uses dementia as the clinical term for progressive multi-domain cognitive decline with functional interference. Fellowship answers should be bilingual: use major NCD when speaking DSM, dementia when speaking ICD or lay communication, and always name the aetiological subtype when evidence allows.[1]
Classification
Aetiological subtypes (exam core four)
| Subtype | Clinical signature | Key criteria anchor |
|---|---|---|
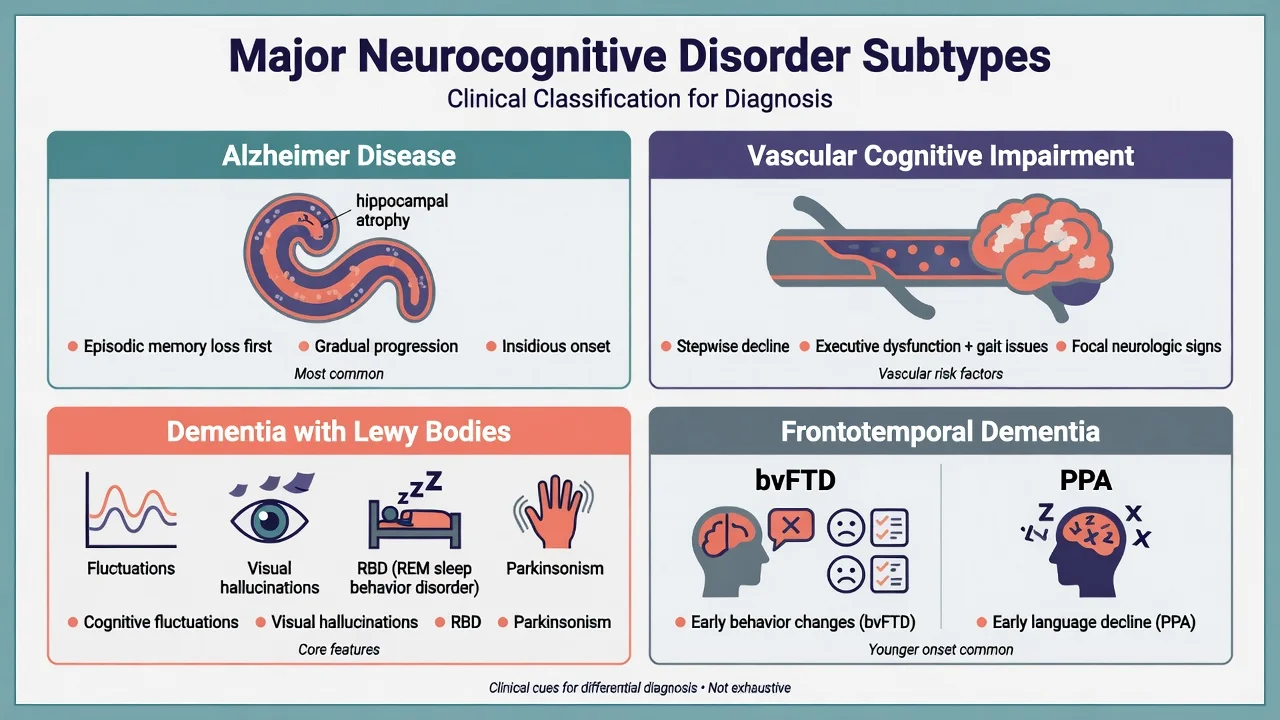
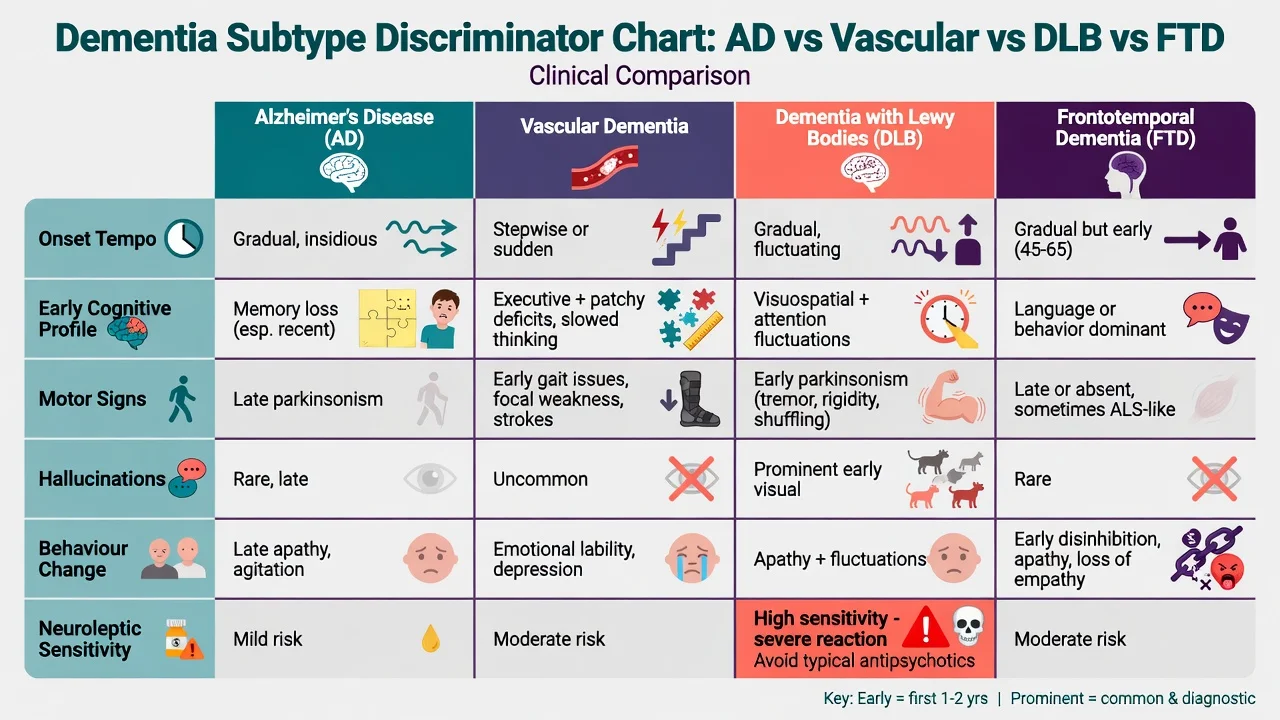
| Alzheimer disease | Insidious episodic memory then multi-domain; gradual | NIA-AA clinical diagnosis of dementia due to AD (McKhann 2011); research criteria (Dubois 2007) |
| Vascular cognitive disorder | Stepwise or subcortical executive/speed/gait; vascular risks | Historical NINDS-AIREN; VASCOG 2014 vascular cognitive disorders |
| Dementia with Lewy bodies | Fluctuations, well-formed visual hallucinations, RBD, spontaneous parkinsonism; neuroleptic sensitivity | DLB Consortium 3rd/4th reports |
| Frontotemporal | bvFTD behavioural syndrome or PPA language variants; often younger onset | Rascovsky bvFTD; Gorno-Tempini PPA |
Mixed pathology (especially AD plus vascular) is common in late life — do not force a pure label when the history is hybrid.[8][9]
Probable AD (clinical NIA-AA framing)
McKhann and colleagues require dementia criteria plus insidious onset, clear-cut history of worsening, and the most prominent early deficits either amnestic or non-amnestic (language, visuospatial, executive). Exclusion of substantial concomitant cerebrovascular disease explaining the deficits, core features of other dementias, and major medical/psychiatric alternatives supports probable AD dementia; atypical features lower certainty to possible.[1]
Epidemiology and risk factors
The Lancet Commissions (2017, 2020) synthesised life-course risk reduction: less education, hearing loss, hypertension, obesity, smoking, depression, physical inactivity, social isolation, diabetes, excessive alcohol, traumatic brain injury, and air pollution among others — roughly two-fifths of dementia cases might be theoretically preventable if risks were eliminated at population level (not a promise for any single patient).[9][10]
Non-modifiable risks include age, APOE ε4 (AD), and some monogenic FTD/AD mutations. Vascular risk factor control is both prevention and management of vascular cognitive impairment.[8][9]
Pathophysiology
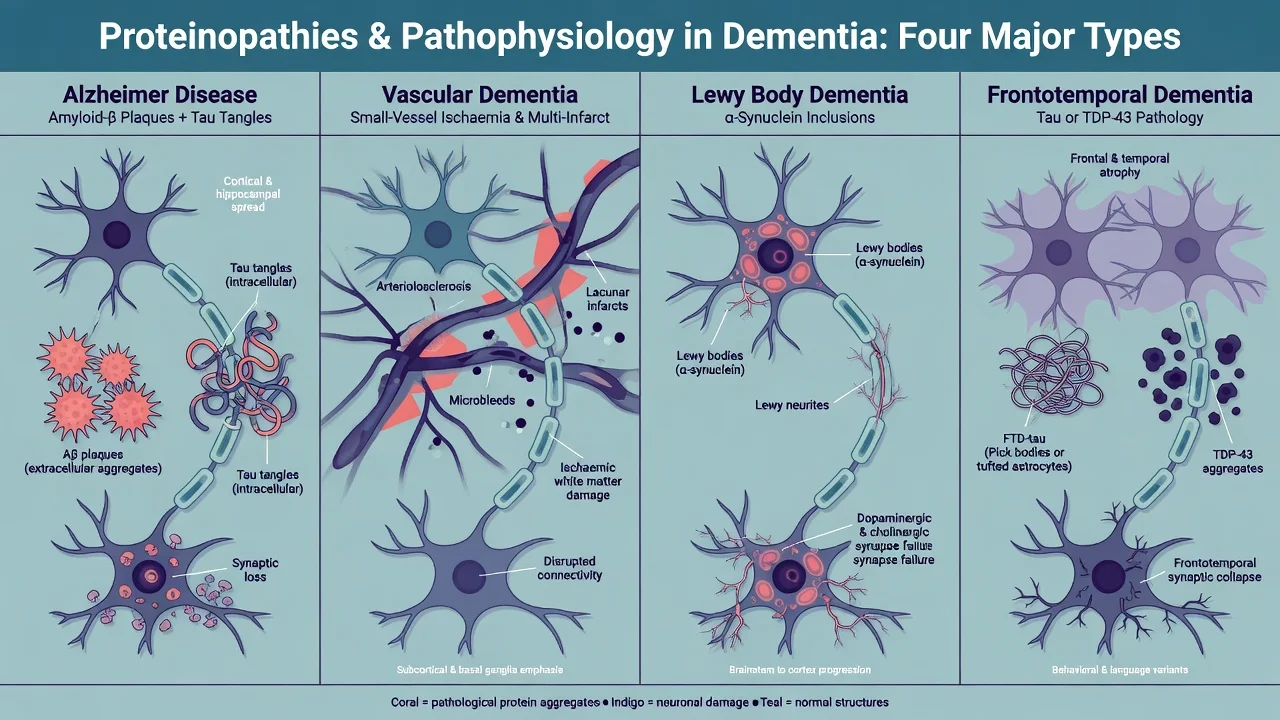
Alzheimer disease features extracellular amyloid-β plaques and intracellular hyperphosphorylated tau neurofibrillary tangles, with early involvement of medial temporal/hippocampal networks and progressive neocortical spread. Cholinergic basal forebrain degeneration underpins the symptomatic rationale for cholinesterase inhibitors.[1][2]
Vascular cognitive impairment spans multi-infarct disease, strategic single infarcts, and subcortical small-vessel disease (lacunes, white-matter hyperintensities) producing executive and processing-speed deficits, gait disorder, and urinary symptoms more than pure amnesia early on.[7][8]
Lewy body disease is an α-synucleinopathy. Clinical DLB and Parkinson disease dementia (PDD) share pathology; the one-year rule (dementia before or within one year of parkinsonism → DLB; established PD long preceding dementia → PDD) is a clinical convention, not a biological wall.[3][4]
FTD spectrum proteinopathies include tau, TDP-43, and FUS; genetics include MAPT, GRN, and C9orf72 expansions. Behavioural variant and language variants reflect network topography more than a single "memory disease."[5][6]
Clinical presentation
Alzheimer disease
Typical amnestic AD begins with insidious episodic memory failure (forgetting recent conversations, repeating questions), later language, visuospatial, and executive decline. Insight often erodes; depression and anxiety can appear early; psychosis and agitation become more common later.[1]
Vascular cognitive impairment
Tempo may be stepwise after strokes or gradual with subcortical ischaemic disease. Expect relative early executive dysfunction, slowed processing, focal neurological signs, gait disturbance, and vascular risk history. Emotional lability and depression are common.[7][8]
Dementia with Lewy bodies
Core clinical features emphasised by the DLB Consortium include fluctuating cognition (especially attention/alertness), recurrent well-formed visual hallucinations, REM sleep behaviour disorder, and spontaneous parkinsonism. Supportive features include neuroleptic sensitivity, postural instability, autonomic dysfunction, and hypersomnia. Cognitive profile often shows early attention and visuospatial deficits relative to pure amnesia.[3][4]
Frontotemporal spectrum
bvFTD (Rascovsky): progressive deterioration of behaviour and/or cognition with three or more of disinhibition, apathy/inertia, loss of sympathy/empathy, perseverative/compulsive behaviour, hyperorality, and a dysexecutive neuropsychological profile — with functional decline and exclusion of better explanations. Imaging or genetic support raises certainty.[5]
PPA (Gorno-Tempini): nonfluent/agrammatic, semantic, and logopenic variants — language-led syndromes that may link to FTD pathology or AD pathology (especially logopenic).[6]
BPSD
Behavioural and psychological symptoms of dementia (agitation, aggression, psychosis, depression, apathy, sleep disturbance, wandering) drive carer distress, hospitalisation, and residential placement. The Neuropsychiatric Inventory (NPI) structures domain assessment for exams and trials.[13][25]
Differential diagnosis
| Mimic | Discriminators |
|---|---|
| Depression ("pseudodementia") | Mood, anhedonia, effortful testing, "I don't know" answers; treat depression and reassess cognition |
| Medication effects | Anticholinergics, benzodiazepines, opioids, polypharmacy — deprescribe trial |
| Metabolic/endocrine | B12, thyroid, sodium, glucose, hepatic/renal failure |
| Sensory impairment | Hearing/vision loss inflates apparent cognitive scores |
| Normal pressure hydrocephalus | Gait, incontinence, cognitive change triad — imaging pathway |
| Autoimmune encephalitis / CJD | Subacute, seizures, movement, rapid course |
| Primary psychiatric psychosis | Younger onset history, less progressive multi-domain decline; still exclude DLB in late onset with visual hallucinations |
Clinical and bedside assessment
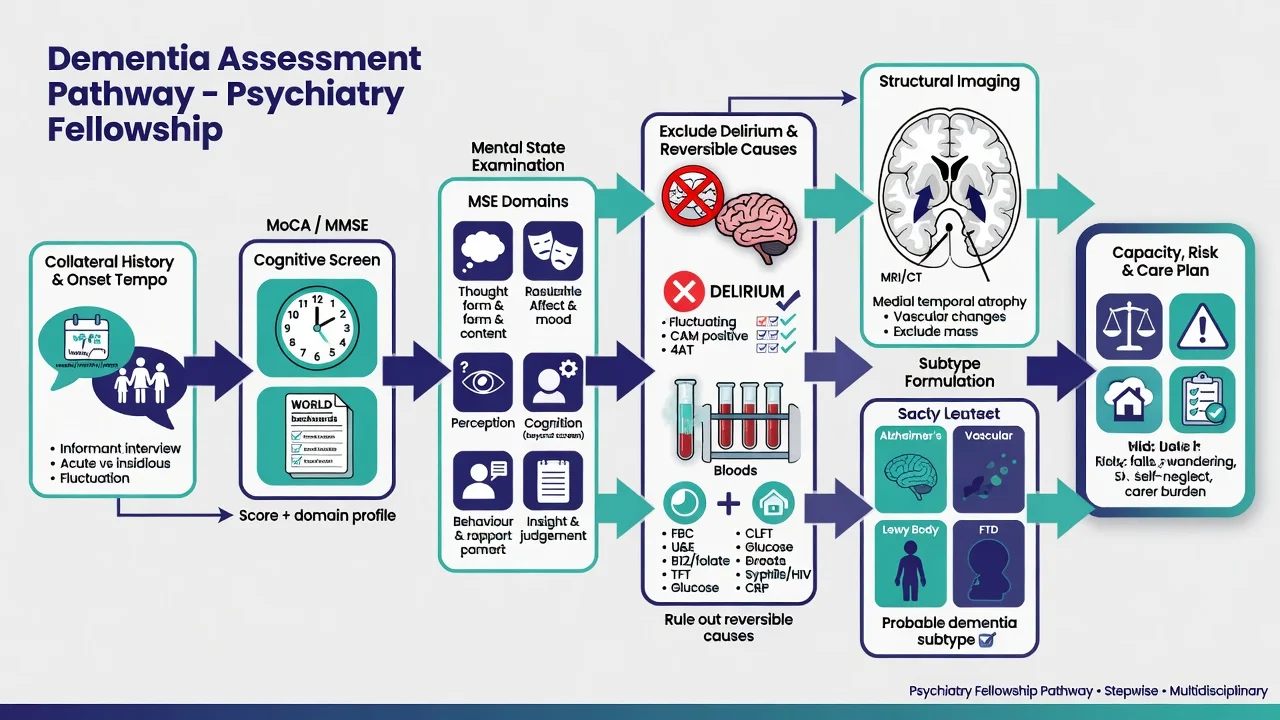
- Collateral history is mandatory — onset, tempo, domains, IADL/ADL loss, BPSD, sleep (dream enactment), falls, alcohol, drugs, head injury, vascular risks, family history.[1][3]
- MSE and bedside cognitive testing — orientation, attention (serial 7s / months reverse), memory, language, praxis, visuospatial (clock), frontal behaviours.
- Screens: MMSE is classic but education-sensitive and weak for mild executive/visuospatial deficits; MoCA is more sensitive for mild impairment (original cut-off framing around 26/30 requires education and cultural interpretation).[11][12]
- BPSD quantification — NPI or structured behavioural charting.[13]
- Neurologic exam — parkinsonism, focal signs, gait, myoclonus, primitive reflexes.
- Risk — driving, cooking/fire, wandering, financial abuse, falls, suicide (early insight), carer burnout.
- Capacity — decision-specific (see below).[27]
Investigations
- Bloods: FBC, electrolytes, renal/liver, glucose/HbA1c, B12, folate, TSH, calcium; consider syphilis/HIV if risk or atypical presentation.[28]
- Structural imaging (CT or preferably MRI once): exclude mass, large stroke, hydrocephalus; support patterns (medial temporal atrophy in AD-like disease; vascular burden; frontotemporal atrophy) without treating educational schematics as a specific patient's scan.[1][8]
- Specialist tests (pathway-dependent): DAT imaging support in DLB, FDG-PET, CSF or PET AD biomarkers where available — know indications, not every assay detail.[2][3]
- ECG before cholinesterase inhibitors when cardiac risk, bradycardia, or interacting drugs.[18][28]
Management — resuscitation and acute behavioural crisis
Acute "agitation in dementia" is a medical problem until proven otherwise: pain, infection (UTI, pneumonia), constipation, urinary retention, hypoxia, electrolyte disturbance, medication toxicity or withdrawal, sensory overload, and delirium on dementia.[25]
Immediate priorities: ensure safety with least-restrictive de-escalation and a calmer environment; examine and investigate delirium triggers; avoid reflexive IM antipsychotics; and if imminent risk of harm persists after non-drug measures, use the lowest effective dose for the shortest time, document risk–benefit including the mortality signal, and review daily for cessation.[21][25][26]
In DLB/PDD, antipsychotics can precipitate severe sensitivity reactions; if unavoidable, specialist low-dose strategies (historically quetiapine or clozapine in PD psychosis pathways) are preferred over high-potency D2 blockade — rivastigmine may help neuropsychiatric symptoms in PDD/DLB contexts.[3][20]
Management — definitive and stepwise
Non-pharmacological core
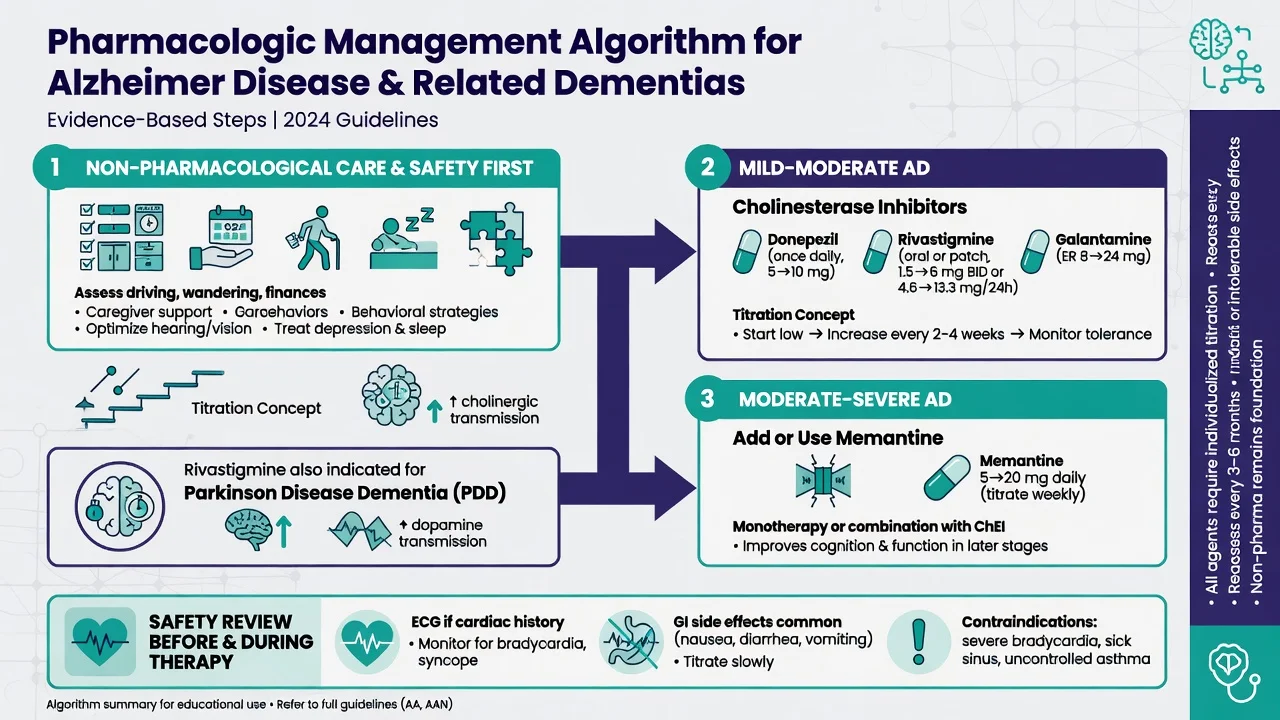
Person-centred care, carer education, structured routines, meaningful activity, sensory optimisation (hearing/vision), and advanced care and legal planning are first-line across guidelines and commissions.[9][25][28]
Cholinesterase inhibitors and memantine
| Agent | Typical adult dosing concept (oral unless noted) | Primary evidence niche |
|---|---|---|
| Donepezil | Start 5 mg PO once daily for 4 weeks, then 10 mg once daily if tolerated | Mild–moderate AD; continued benefit signal in moderate–severe (DOMINO-AD) |
| Rivastigmine | Oral start 1.5 mg twice daily, titrate every ≥2 weeks toward 3–6 mg twice daily; transdermal 4.6 mg/24 h then 9.5 mg/24 h (higher patch strengths per product information when indicated) | AD; PDD (Emre NEJM) |
| Galantamine | Immediate-release total daily dose commonly titrated from 8 mg/day toward 16–24 mg/day in divided doses (product-dependent XR once daily) | Mild–moderate AD |
| Memantine | Start 5 mg PO daily, increase by 5 mg weekly to target 10 mg twice daily (or XR 28 mg daily where available) | Moderate–severe AD; adjunct to donepezil (Tariot) |
Evidence snapshots examiners expect by name:[15][16][17][18][19][20]
- Reisberg 2003: memantine improved outcomes vs placebo in moderate–severe AD.[15]
- Tariot 2004: memantine added to stable donepezil better than donepezil plus placebo in moderate–severe AD.[16]
- Howard DOMINO-AD 2012: in moderate–severe AD, continued donepezil associated with cognitive and functional benefits over withdrawal; memantine effects were smaller/mixed depending on outcome.[17]
- Cochrane: donepezil has modest benefits on cognition and global measures; memantine shows small benefits in moderate–severe dementia of AD type with less clear benefit in mild disease.[18][19]
- Emre 2004: rivastigmine improved cognition and some neuropsychiatric measures in PDD vs placebo.[20]
Practical monitoring: nausea, vomiting, diarrhoea, anorexia, weight loss, vivid dreams/insomnia (donepezil timing), bradycardia/syncope, urinary urgency; memantine — dizziness, headache, confusion, dose-adjust in renal impairment per product information. Review benefit at 3 months and at least every 6–12 months; deprescribe if no meaningful benefit or harm.[18][28]
Cholinesterase inhibitors have limited or no established disease-modifying role in pure bvFTD and can worsen behaviour in some FTD patients — do not prescribe by habit.[5][28]
BPSD pharmacotherapy and the antipsychotic caution
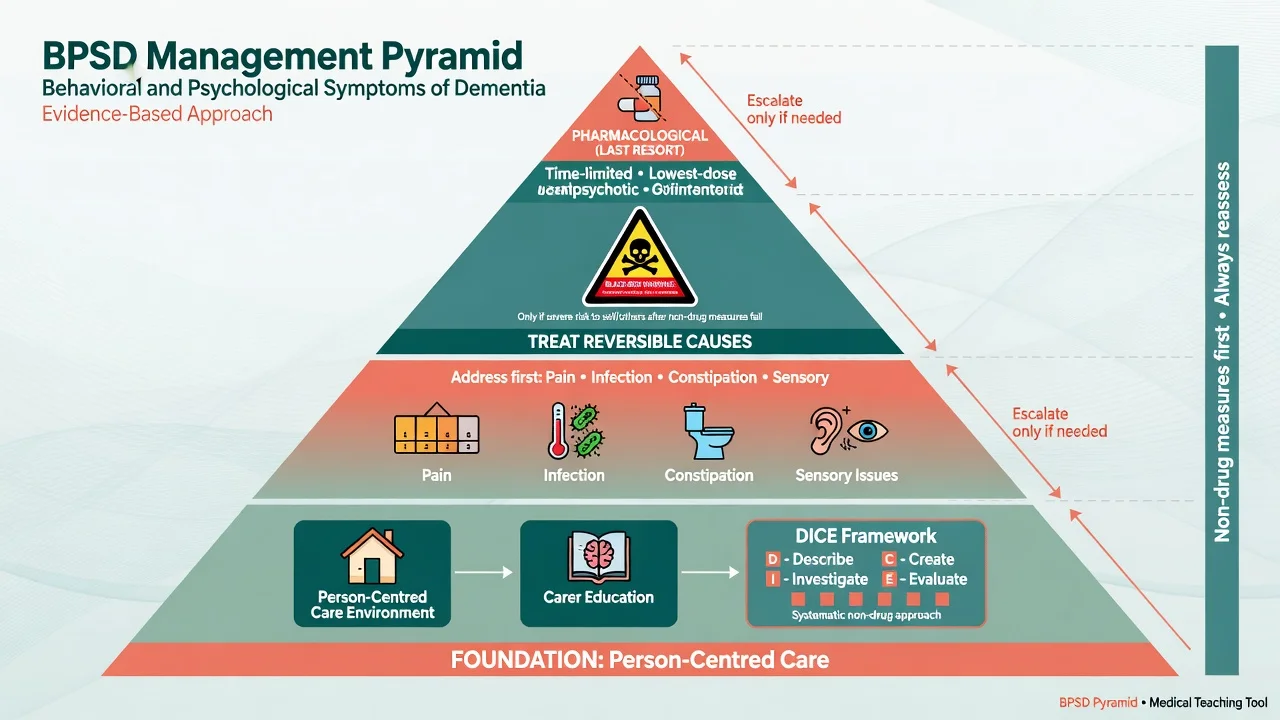
Kales and colleagues emphasise systematic assessment (e.g. DICE: Describe, Investigate, Create, Evaluate) before drugs.[25] Sink and colleagues documented limited and mixed pharmacological efficacy for many neuropsychiatric targets.[26]
Antipsychotic mortality signal (black-box-style caution):[21][22][23][24]
- Schneider meta-analysis (2005): atypical antipsychotics associated with increased death vs placebo in dementia RCTs (odds ratio about 1.5 in that analysis).[21]
- CATIE-AD (Schneider 2006): modest effectiveness of olanzapine, quetiapine, and risperidone for psychosis/aggression/agitation was offset by adverse effects; overall "no statistical difference" on main effectiveness endpoint vs placebo when discontinuations considered — clinical use requires careful selection.[22]
- DART-AD long-term follow-up (Ballard 2009): continuing antipsychotics associated with higher long-term mortality than withdrawal in many patients who could be withdrawn.[23]
- Maust 2015: absolute mortality risk estimates / NNH framing for antipsychotics (and other psychotropics) in dementia — use to counsel, not to create false precision in viva.[24]
If an antipsychotic is used after non-drug measures for severe distress or danger: choose one agent, start low (e.g. risperidone often studied around 0.5–1 mg/day total in dementia trials — follow local product information and geriatric dosing), reassess within days, and plan stop or taper by 6–12 weeks when possible. Avoid in DLB unless specialist-led last resort.[21][22][3]
SSRIs may help depression or some compulsive/behavioural features with attention to hyponatraemia and falls; chronic benzodiazepines generally worsen cognition and falls — avoid as BPSD maintenance.[26][28]
Specific subtypes and scenarios
- CL hospital consult: post-operative cognitive worsening is delirium until proven otherwise; establish baseline cognition from family and prior notes before labelling "new dementia."[25]
- Residential care BPSD crisis: environment, staffing, pain, and constipation before drugs; document least-restrictive plan.[25]
- Young-onset: broader differential, genetics counselling pathway, occupational and dependent-child impacts.[5][9]
- Mixed AD-vascular: treat vascular risks aggressively; cognitive enhancers may still be considered if AD phenotype is substantial.[8][28]
Complications and pitfalls
Classic exam pitfalls include missing delirium on dementia, starting antipsychotics for wandering or mild irritability, high-potency antipsychotics in DLB, automatic AChEI in pure FTD, ignoring anticholinergic burden, omitting driving advice, skipping capacity for placement or finances, and pathologising cultural or language-barrier performance on unvalidated screens.[3][5][21][25][27]
Prognosis and disposition
Course is progressive for neurodegenerative subtypes; tempo is faster on average in some FTD and DLB presentations than typical late-onset AD. Survival after diagnosis is highly variable (often several years) and is not a single exam number — emphasise function, comorbidity, and goals of care.[9]
Disposition ladder: optimise home supports and carer respite → package of care → residential aged care when night-time risk or carer collapse makes home unsafe. Involve memory clinic, old-age psychiatry, and GP shared care early. Advance care planning and enduring powers (jurisdiction-specific names) should be raised while residual capacity remains.[9][28]
Special populations
- Down syndrome: high lifetime AD risk; baseline function essential; care with consent frameworks for intellectual disability.[9]
- CALD and Indigenous peoples: use interpreters; do not over-interpret non-validated cut-offs; cultural formulation of behaviour.[9]
- End-of-life: deprescribe futile cognitive drugs; prioritise comfort, oral care, and carer support.[9]
Capacity and legal principles
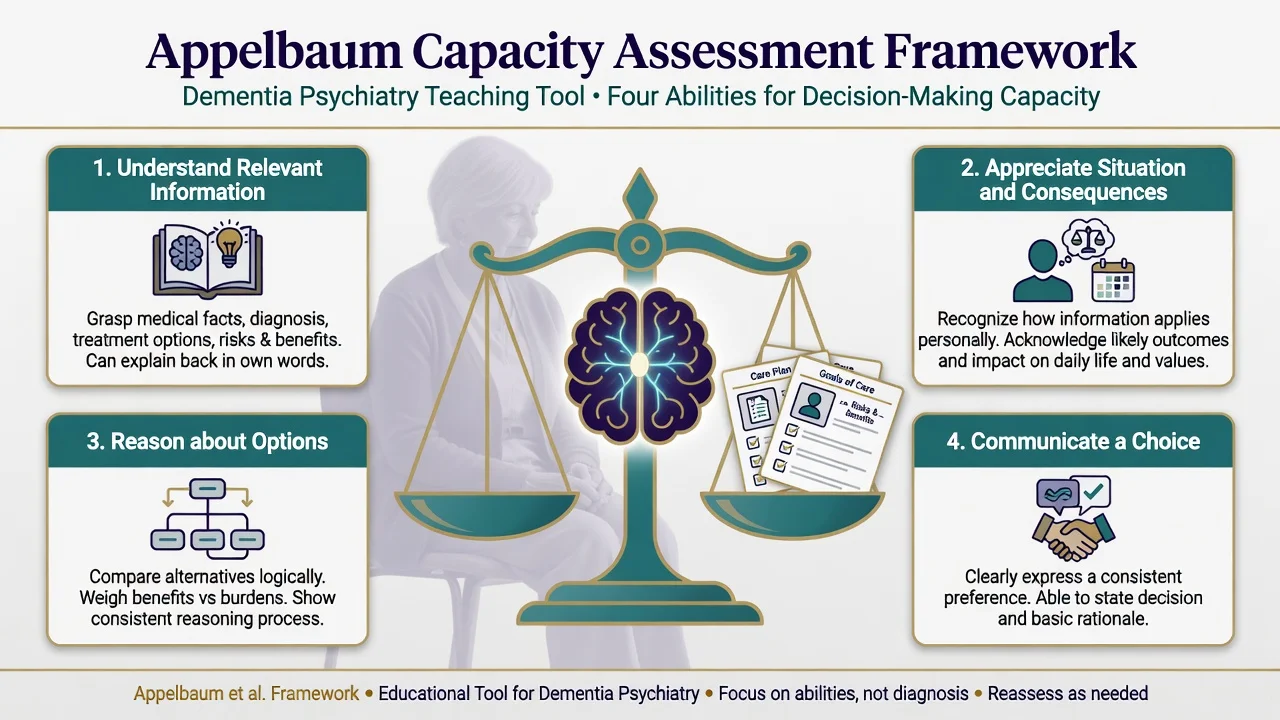
Appelbaum and Grisso summarise four abilities for treatment consent capacity: understand relevant information; appreciate the situation and consequences; reason about options; and communicate a stable choice.[27]
Capacity is not global. A person with major NCD may retain capacity for simple treatment choices while lacking capacity for complex financial or placement decisions. Document the decision tested, information given, abilities assessed, and supports provided (hearing aids, simplified language, quiet room). Guardianship, enduring powers, and mental health legislation thresholds are jurisdiction-specific — state principles and local Acts without inventing section numbers for every board.[27][28]
Evidence, guidelines, and regional differences
- Lancet Commissions frame prevention and multi-domain care.[9][10]
- NIA-AA / Dubois frame AD diagnosis research and clinical certainty language.[1][2]
- DLB Consortium, Rascovsky, Gorno-Tempini, VASCOG anchor subtypes.[3][5][6][8]
- APA Alzheimer guideline (2007) remains a structured US reference; contemporise with trial evidence and local formulary (NICE NG97 principles in UK; TGA/PBS listing and RANZCP old-age practice in ANZ).[28]
- Cognitive enhancers are symptomatic; disease-modifying anti-amyloid monoclonal antibodies are a separate, rapidly evolving specialty pathway with eligibility, ARIA risk, and access constraints — mention awareness without overselling as universal standard care in all regions as of this topic date.[9]
ANZ: PBS criteria and product information govern AChEI/memantine initiation and continuing authority; use local old-age psychiatry and geriatric medicine pathways; Mental Health Act vs guardianship for detention and substitute decision-making are state/territory-specific. UK: NICE dementia guidance emphasises non-drug care and structured AChEI/memantine pathways. US: APA guideline framework plus FDA boxed warning on antipsychotic mortality in dementia-related psychosis.[21][28]
Exam pearls
DLB core cluster
- Mild vs major NCD = independence, not a magic score.[14]
- Delirium first in any acute change.[25]
- Antipsychotics: OR ~1.5 mortality in Schneider meta-analysis; time-limited only.[21]
- CATIE-AD: modest benefit, high adverse-effect cost.[22]
- DART-AD: withdrawal often safer long-term when feasible.[23]
- Donepezil 5→10 mg; memantine titrate to 10 mg bd; rivastigmine for PDD.[17][15][20]
- Capacity: understand, appreciate, reason, communicate choice.[27]
- bvFTD can devastate behaviour with relatively preserved early MMSE — do not wait for amnesia.[5]
References
- [1]McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease Alzheimers Dement, 2011.PMID 21514250
- [2]Dubois B, Feldman HH, Jacova C, et al. Research criteria for the diagnosis of Alzheimer's disease: revising the NINCDS-ADRDA criteria Lancet Neurol, 2007.PMID 17616482
- [3]McKeith IG, Boeve BF, Dickson DW, et al. Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium Neurology, 2017.PMID 28592453
- [4]McKeith IG, Dickson DW, Lowe J, et al. Diagnosis and management of dementia with Lewy bodies: third report of the DLB Consortium Neurology, 2005.PMID 16237129
- [5]Rascovsky K, Hodges JR, Knopman D, et al. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia Brain, 2011.PMID 21810890
- [6]Gorno-Tempini ML, Hillis AE, Weintraub S, et al. Classification of primary progressive aphasia and its variants Neurology, 2011.PMID 21325651
- [7]Román GC, Tatemichi TK, Erkinjuntti T, et al. Vascular dementia: diagnostic criteria for research studies. Report of the NINDS-AIREN International Workshop Neurology, 1993.PMID 8094895
- [8]Sachdev P, Kalaria R, O'Brien J, et al. Diagnostic criteria for vascular cognitive disorders: a VASCOG statement Alzheimer Dis Assoc Disord, 2014.PMID 24632990
- [9]Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission Lancet, 2020.PMID 32738937
- [10]Livingston G, Sommerlad A, Orgeta V, et al. Dementia prevention, intervention, and care Lancet, 2017.PMID 28735855
- [11]Folstein MF, Folstein SE, McHugh PR "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician J Psychiatr Res, 1975.PMID 1202204
- [12]Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment J Am Geriatr Soc, 2005.PMID 15817019
- [13]Cummings JL, Mega M, Gray K, et al. The Neuropsychiatric Inventory: comprehensive assessment of psychopathology in dementia Neurology, 1994.PMID 7991117
- [14]Petersen RC, Smith GE, Waring SC, et al. Mild cognitive impairment: clinical characterization and outcome Arch Neurol, 1999.PMID 10190820
- [15]Reisberg B, Doody R, Stöffler A, et al. Memantine in moderate-to-severe Alzheimer's disease N Engl J Med, 2003.PMID 12672860
- [16]Tariot PN, Farlow MR, Grossberg GT, et al. Memantine treatment in patients with moderate to severe Alzheimer disease already receiving donepezil: a randomized controlled trial JAMA, 2004.PMID 14734594
- [17]Howard R, McShane R, Lindesay J, et al. Donepezil and memantine for moderate-to-severe Alzheimer's disease N Engl J Med, 2012.PMID 22397651
- [18]Birks JS, Harvey RJ Donepezil for dementia due to Alzheimer's disease Cochrane Database Syst Rev, 2018.PMID 29923184
- [19]McShane R, Westby MJ, Roberts E, et al. Memantine for dementia Cochrane Database Syst Rev, 2019.PMID 30891742
- [20]Emre M, Aarsland D, Albanese A, et al. Rivastigmine for dementia associated with Parkinson's disease N Engl J Med, 2004.PMID 15590953
- [21]Schneider LS, Dagerman KS, Insel P Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials JAMA, 2005.PMID 16234500
- [22]Schneider LS, Tariot PN, Dagerman KS, et al. Effectiveness of atypical antipsychotic drugs in patients with Alzheimer's disease N Engl J Med, 2006.PMID 17035647
- [23]Ballard C, Hanney ML, Theodoulou M, et al. The dementia antipsychotic withdrawal trial (DART-AD): long-term follow-up of a randomised placebo-controlled trial Lancet Neurol, 2009.PMID 19138567
- [24]Maust DT, Kim HM, Seyfried LS, et al. Antipsychotics, other psychotropics, and the risk of death in patients with dementia: number needed to harm JAMA Psychiatry, 2015.PMID 25786075
- [25]Kales HC, Gitlin LN, Lyketsos CG Assessment and management of behavioral and psychological symptoms of dementia BMJ, 2015.PMID 25731881
- [26]Sink KM, Holden KF, Yaffe K Pharmacological treatment of neuropsychiatric symptoms of dementia: a review of the evidence JAMA, 2005.PMID 15687315
- [27]Appelbaum PS, Grisso T Assessing patients' capacities to consent to treatment N Engl J Med, 1988.PMID 3200278
- [28]APA Work Group on Alzheimer's Disease and other Dementias, Rabins PV, Blacker D, et al. American Psychiatric Association practice guideline for the treatment of patients with Alzheimer's disease and other dementias. Second edition Am J Psychiatry, 2007.PMID 18340692