Psych · Consultation-liaison psychiatry
Endocrine psychiatry (thyroid, Cushing, Addison)
Also known as Thyroid psychiatry · Cushing psychosis · Steroid-induced psychiatric disorder · Myxoedema madness · Addison neuropsychiatry · Glucocorticoid mania
Exam-exhaustive fellowship topic on endocrine psychiatry for consultation-liaison practice — thyrotoxicosis and hypothyroidism including myxoedema psychosis, Cushing syndrome depression psychosis and cognitive change, Addison and adrenal insufficiency neuropsychiatry, exogenous corticosteroid-induced mania psychosis and depression, lithium–thyroid interactions, investigation algorithms, crisis care, and bridge psychopharmacology. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Examiners use endocrine stems to test organic differential, crisis recognition, dose-linked steroid toxicity, and shared care with endocrinology. A candidate who only recites primary MDD or bipolar criteria will fail when the stem is Graves irritability, Cushing depression, Addison delirium, or dexamethasone mania.[1][8][14]
Overview and definition
Endocrine psychiatry is the consultation-liaison discipline covering psychiatric syndromes caused or amplified by endocrine disease and by endocrine-active drugs (especially glucocorticoids and lithium-related thyroid change). Coding may use mental disorder due to another medical condition or medication-induced mental disorder; viva credit goes to mechanism, urgency, and correct medical co-management, not ICD pedantry alone.[2][11][14]
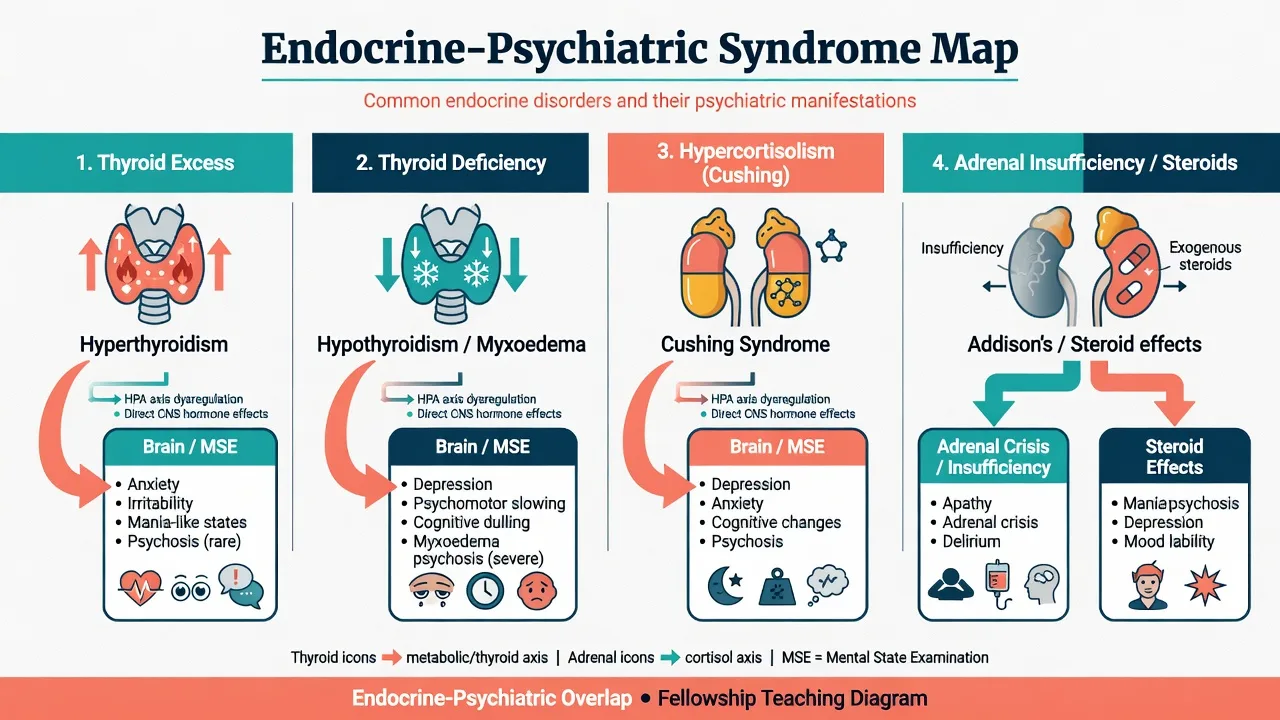
Core axes for fellowship exams are thyroid excess and deficiency (including rare myxoedema psychosis); endogenous hypercortisolism with depression, anxiety, cognition, and less often mania or psychosis; adrenal insufficiency with apathy, depression, and crisis delirium or psychosis; exogenous corticosteroids causing insomnia, mania or hypomania, depression, psychosis, or delirium; and psychotropic–endocrine interfaces including lithium–thyroid effects and antidepressant use after endocrine correction.[1][10][13][17][19]
Classification and syndrome map
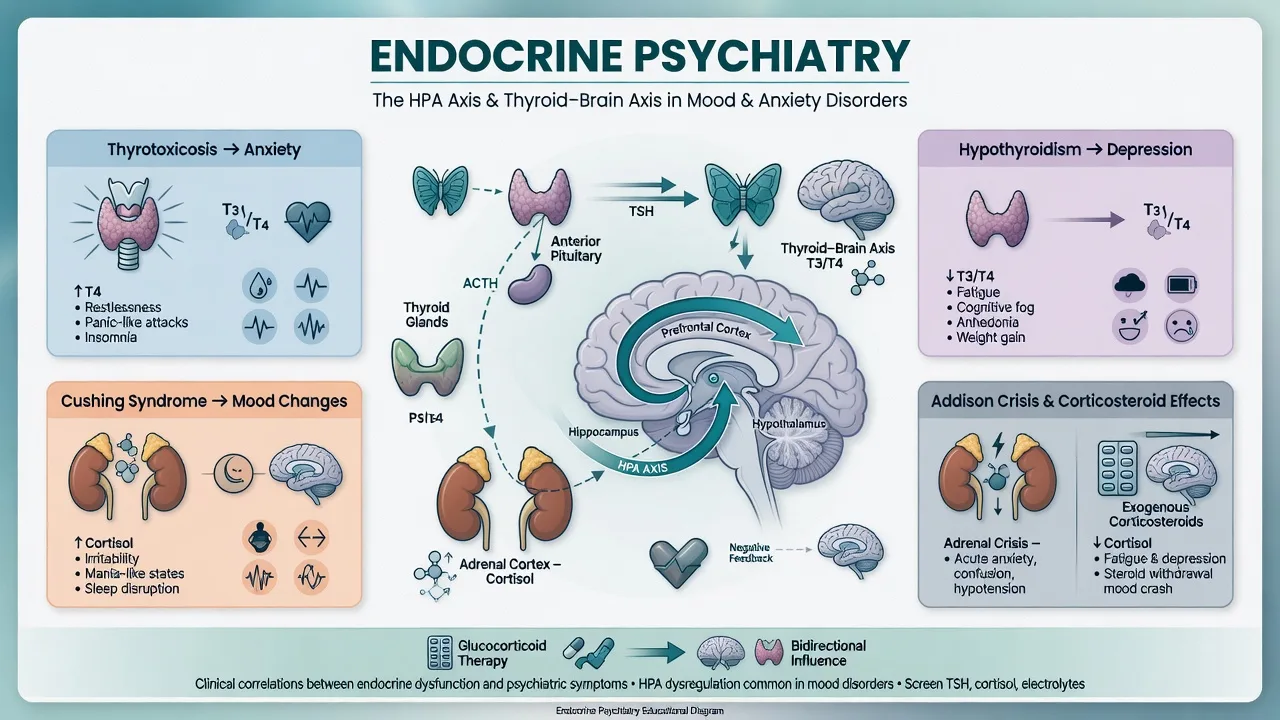
| Axis | Typical psychiatric pattern | Key medical anchors |
|---|---|---|
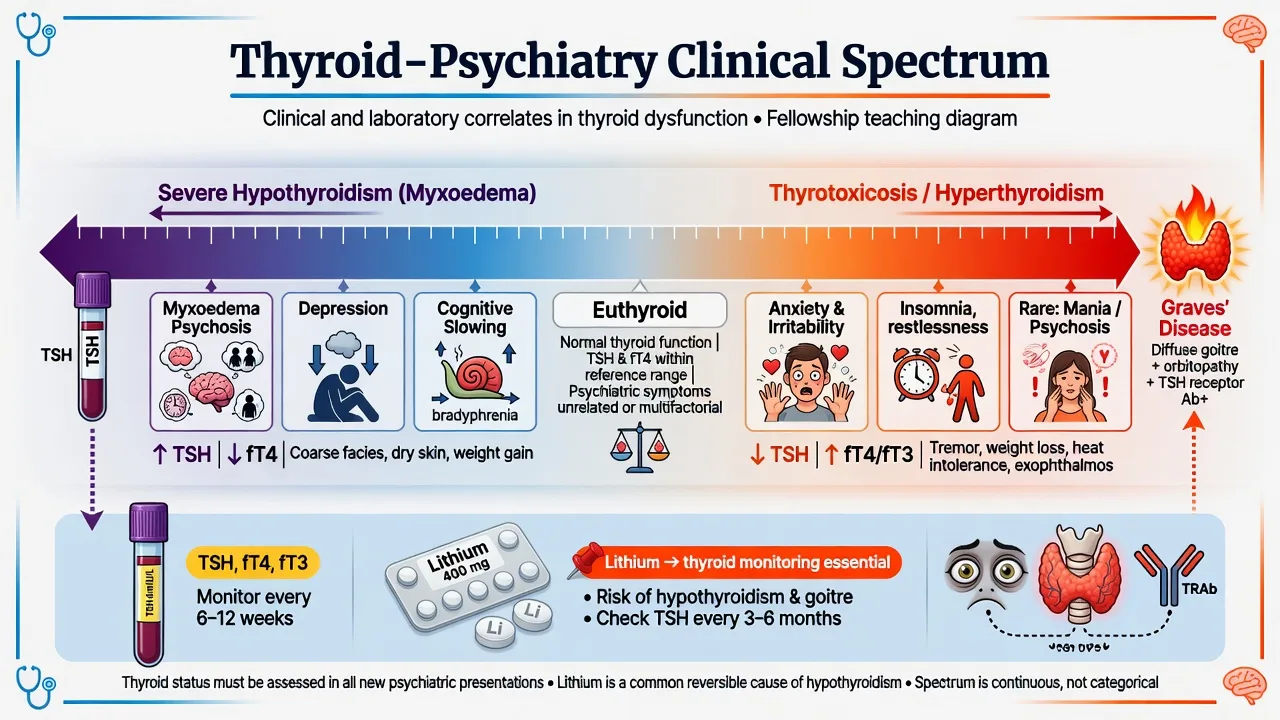
| Thyrotoxicosis | Anxiety, irritability, insomnia, panic-like spells; rare mania/psychosis | Tachycardia, tremor, heat intolerance, weight loss, suppressed TSH |
| Hypothyroidism | Depression, anergia, slowing, cognitive fog; rare myxoedema psychosis | Cold intolerance, myxoedema, raised TSH (primary), low free T4 |
| Cushing syndrome | Major depression common; anxiety; cognitive change; less often mania/psychosis | Central obesity, striae, hypertension, hypokalaemia (esp. ectopic) |
| Adrenal insufficiency | Fatigue, low mood, apathy; crisis delirium/psychosis | Hyponatraemia, hyperkalaemia (primary), hypotension, pigmentation (primary) |
| Exogenous steroids | Early euphoria/hypomania/insomnia; later depression; psychosis/delirium | Temporal link to high dose or escalation |
DSM-5-TR / ICD-11 allow medical and medication-induced mood, anxiety, and psychotic disorders. Discriminators that matter: tempo with hormone change, physical signs, laboratory confirmation, and improvement when the endocrine driver is corrected.[2][11][14]
Epidemiology and risk
In Cushing disease, major depression is frequent and associates with clinical severity markers in classic series; anxiety, manic features, psychosis, and cognitive impairment are also described across modern reviews.[7][8][10][12] Register data link hospitalised hyperthyroidism with increased risk of subsequent affective disorder, and bipolar hospitalisation with increased hyperthyroidism risk — bidirectional clinical vigilance, not proof of a single causal model.[15][24]
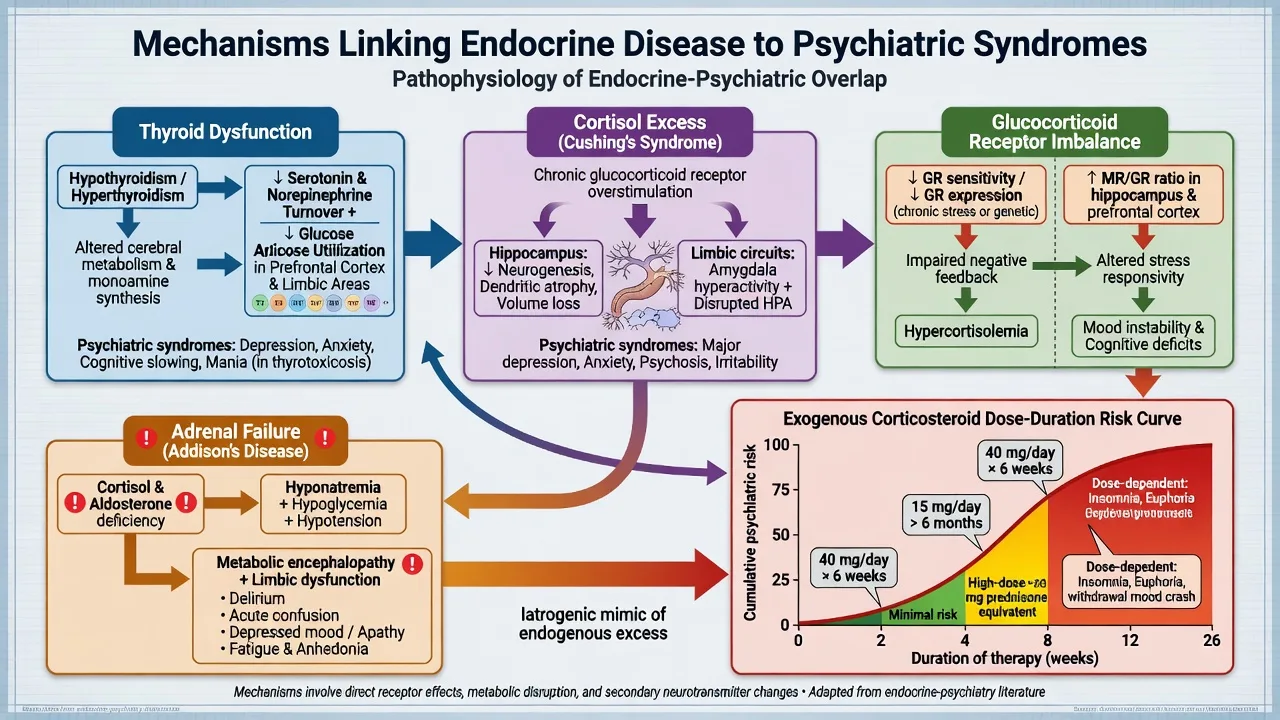
Exogenous glucocorticoids produce a spectrum of psychiatric adverse effects. Short-term exposure more often associates with euphoria or hypomania; longer therapy more often with depression; psychosis and delirium occur across contexts, with dose as a major risk factor in classic teaching reviews.[1][2][3][4] Mania specifically is supported by contemporary systematic review of corticosteroid-associated manic presentations.[6] Oncology steroid series reinforce that mental disorders are clinically important under high-dose protocols.[5]
Pathophysiology and mechanisms
Thyroid. Both excess and deficiency disturb mood and cognition. Hypothyroidism associates with altered cerebral glucose metabolism that can improve with replacement in imaging studies; clinical reviews link thyroid dysfunction tightly to depressive and anxiety phenotypes.[13][14][23] Thyroid hormone adjunct strategies in primary mood disorders are a related but separate literature (Bauer/Whybrow) — do not confuse adjunct T3/T4 for treatment-resistant depression with treating primary hypothyroidism.[21]
Hypercortisolism. Chronic cortisol excess affects hippocampus and fronto-limbic networks, sleep, and metabolic health, producing depression, anxiety, cognitive inefficiency, and less commonly mania or psychosis.[10][11][12] Exogenous glucocorticoids share receptor-level mechanisms; mineralocorticoid/glucocorticoid receptor imbalance models are used to explain vulnerability in steroid neuropsychiatry reviews.[2][4][11]
Adrenal insufficiency. Cortisol deficiency plus hyponatraemia, hypoglycaemia, and volume depletion can produce apathy, depression, delirium, and rare psychosis; crisis is a medical emergency first.[17][18]
Autoimmune and iatrogenic overlays. Thyroid autoimmunity is enriched in bipolar populations in systematic review; lithium associates with hypothyroidism classically and hyperthyroidism in an under-recognised systematic-review signal.[19][20]
Clinical presentation
Thyrotoxicosis
Expect anxious dysphoria, restlessness, irritability, insomnia, heat intolerance, tremor, and tachycardia. Panic-like episodes and apparent GAD are common mislabels when TSH is never checked. Frank mania or psychosis is less common but examinable, especially in severe Graves disease.[14][15]
Hypothyroidism
Expect depression, anergia, psychomotor slowing, and cognitive fog. Severe untreated disease can produce myxoedema psychosis (paranoia, delusions, sometimes delirium-like confusion) — rare, classic, and reversible with careful thyroid replacement under medical supervision.[13][14][16]
Cushing syndrome
Major depression is the flagship psychiatric comorbidity, often with irritability and anxiety; cognitive complaints (attention, memory) are common; mania and psychosis are less frequent but real.[7][8][10][12] Somatic cues (centripetal obesity, wide purple striae, proximal weakness, hypertension, diabetes, hypokalaemia) support the diagnosis — but psychiatric change can be prominent and ectopic ACTH may look less classically cushingoid early.[9][11]
Addison and adrenal insufficiency
Chronic: fatigue, anorexia, low mood, apathy. Crisis: collapse, abdominal pain, shock, hyponatraemia, hypoglycaemia, delirium, and occasionally psychotic features — treat as endocrine emergency.[17][18]
Steroid-induced syndromes
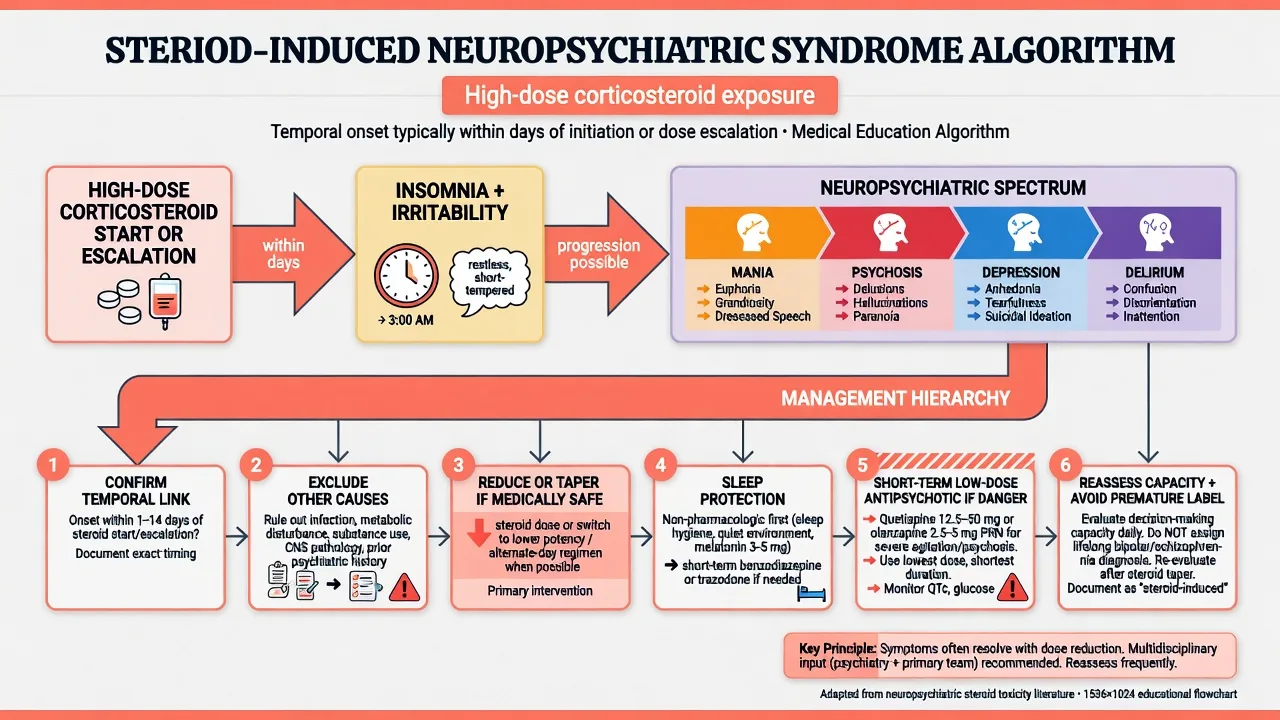
Onset often hours to a few days after high-dose initiation or escalation: insomnia and irritability first, then hypomania/mania, depression with longer exposure, or frank psychosis/delirium.[1][2][3][5][6]
Differential diagnosis — discriminators
- Temporal link to hormone change or steroid dose
- Physical signs and abnormal labs
- Improves when driver corrected
- May need only short-term psychotropics
- Capacity often fluctuates with organic state
- No endocrine driver after work-up
- Personal/family psychiatric trajectory
- Standard guideline psych care
- Endocrine labs normal or incidental
- Longitudinal course independent of hormones
- Acute fluctuating inattention
- Metabolic, infection, CNS, drugs
- CAM-positive logic
- Steroid or AI crisis may coexist
- Fix physiology first
Also hold: substance intoxication/withdrawal, autoimmune encephalitis, SREAT/Hashimoto encephalopathy (edge viva), brain metastases if cancer context, and primary psychosis. Discriminate steroid mania from bipolar I by drug link, absence of prior episodes, and improvement with taper — without refusing needed steroids for life-threatening disease.[2][5][6]
Assessment
- Endocrine history: known thyroid/adrenal/pituitary disease; steroid name, dose, route, start/escalation dates; lithium and other psychotropics; weight change; heat/cold intolerance; crises.
- MSE: mood valence, irritability, psychosis, attention (delirium screen), insight.
- Risk: suicide in severe depression (especially Cushing and profound hypothyroidism), agitation in thyrotoxicosis/steroid mania, medical collapse in AI crisis.[7][10][16]
- Capacity: decision-specific during organic psychosis or severe melancholia.
- Collateral from family and medical teams; do not rely on a single PHQ-9 score to exclude organic disease.
Investigations
Thyroid. TSH first; free T4; free T3 when thyrotoxic or if secondary thyroid disease is possible; TPO antibodies and TRAb when aetiology matters for endocrine management.[14]
Hypercortisolism (if clinical suspicion). Coordinate with endocrinology: late-night salivary cortisol, 24-hour urinary free cortisol, and/or 1 mg overnight dexamethasone suppression. Depression, alcohol use, and enzyme-inducing drugs cause false positives — do not self-diagnose Cushing from a single screen in a depressed outpatient.[9][11][12]
Adrenal insufficiency. Morning cortisol and ACTH; short Synacthen (cosyntropin) testing per Endocrine Society guidance. If crisis is suspected, treat immediately — do not wait for the perfect test panel.[17]
Supportive labs. Electrolytes, glucose, renal function, calcium, FBC; ECG for thyrotoxic arrhythmia risk and before antipsychotics with QTc concern.[14][17]
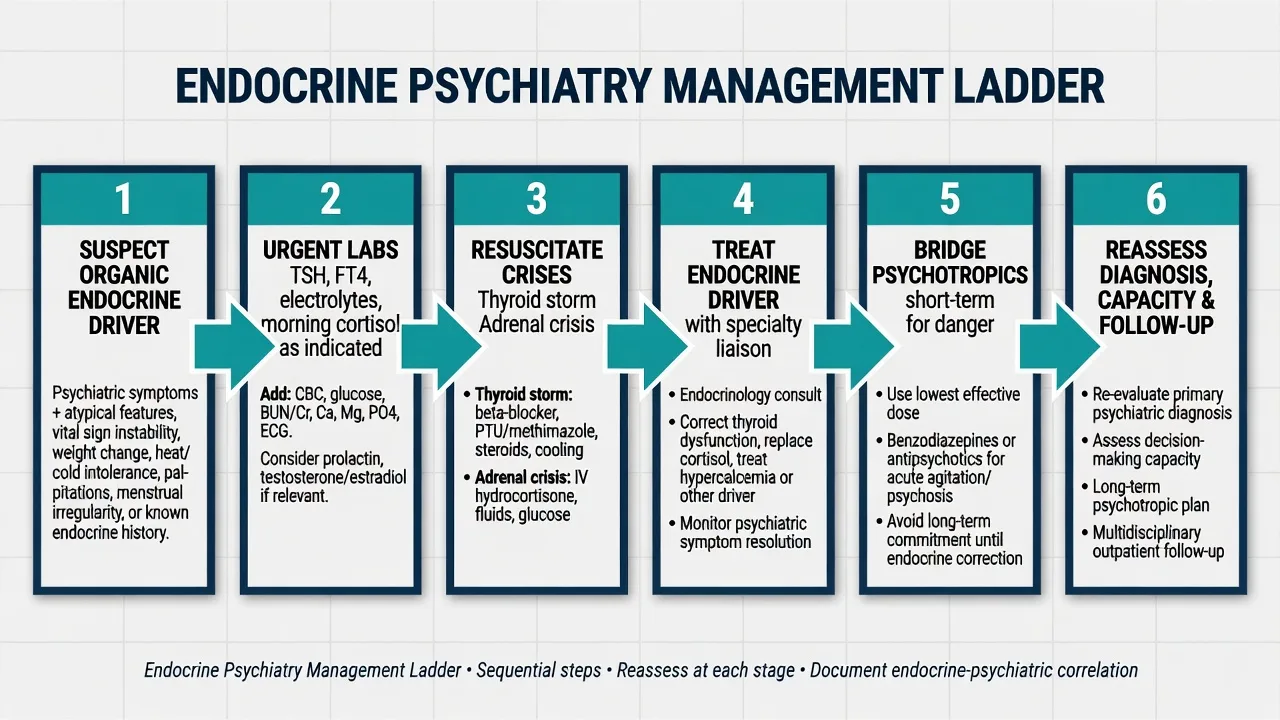
Acute management and red flags
Thyroid storm / severe thyrotoxic psychosis or agitation. Joint medical emergency care (antithyroid therapy and beta-blockade pathways per endocrine protocols), environmental safety, and short-term psychiatric containment only as needed.[14]
Dangerous steroid mania/psychosis. Reduce or taper glucocorticoids if the medical team agrees it is safe; use short-term low-dose antipsychotic for behavioural risk; protect sleep; reassess daily.[1][2][5]
Example cautious acute bridge dosing used in CL practice for severe organic behavioural disturbance (individualise; local formulary; ECG/EPS monitoring): olanzapine 2.5–5 mg oral (or appropriate parenteral pathway if essential) or haloperidol 0.5–2 mg, short duration, stop early when the endocrine or steroid driver is addressed.[2][5]
Definitive management
Treat the driver
- Thyrotoxicosis: antithyroid drugs, radioactive iodine, or surgery pathways with endocrinology/nuclear medicine; beta-blockade for adrenergic symptoms as medically indicated; psychiatric symptoms often improve toward euthyroidism.[14][15]
- Hypothyroidism: levothyroxine replacement under medical guidance; myxoedema psychosis requires concurrent psychiatric safety care while thyroid is restored carefully.[13][16]
- Cushing: definitive therapy directed at the source (transsphenoidal surgery for Cushing disease, adrenal or ectopic pathways as indicated); psychiatric syndromes frequently improve with cortisol control, but residual mood and cognitive symptoms can persist and need follow-up.[8][10][12]
- Primary adrenal insufficiency: glucocorticoid and usually mineralocorticoid replacement, sick-day rules, and crisis education per Endocrine Society guideline.[17]
Steroid-induced psychiatric syndromes
Hierarchy: (1) confirm dose–time relationship; (2) exclude infection, metabolic failure, CNS disease, substance withdrawal; (3) reduce/taper if disease control allows; (4) non-drug supports and sleep; (5) short-term antipsychotic or mood-stabilising strategies for severe mania/psychosis with risk; (6) reassess longitudinal psychiatric diagnosis after washout.[1][2][3][5][6]
Psychotropics as bridges, not substitutes
After medical stabilisation, residual major depression may warrant an SSRI (e.g. sertraline 25–50 mg oral daily titrating toward response, or escitalopram 5–10 mg oral daily) with the usual medical-illness cautions (hyponatraemia, interactions, QTc). Do not expect antidepressants alone to fix active Cushing hypercortisolism or untreated severe hypothyroidism.[8][13][21]
Subclinical hypothyroidism in older adults is not an automatic depression treatment target: randomised evidence (TRUST-related analysis) found levothyroxine did not meaningfully improve depressive symptoms versus placebo in that population — treat on endocrine indications, not mood hope alone.[22]
Lithium and thyroid
Monitor TSH (and free T4 when abnormal) at baseline and periodically. Manage hypothyroidism with levothyroxine in collaboration with endocrine/GP pathways. Remember lithium can also associate with hyperthyroidism in systematic review — do not assume every lithium–thyroid problem is hypo.[19][20]
Special populations
Older adults: delirium risk, lower psychotropic starts, careful steroid use, and humility about treating subclinical hypothyroidism purely for mood.[1][22] Pregnancy: coordinate obstetric–endocrine–psychiatry for Graves and hypothyroidism; avoid diagnostic overshadowing of mood disorders. Intellectual disability: behavioural change may be the only AI or thyroid signal. Cultural care: use interpreters; capacity remains decision-specific.
Evidence and regional notes
ANZ / FRANZCP. CL viva expects TSH in organic screens, steroid mania algorithms, Cushing depression prevalence teaching, and adrenal crisis priorities. Cite Warrington/Dubovsky for steroids and Sonino/Pivonello for Cushing.[1][2][7][10]
UK / MRCPsych. Paper and CASC stems often hide thyrotoxic anxiety or steroid psychosis in medical wards; NICE mental-health pathways still require medical differentials.[1][6][14]
US / ABPN. Endocrine Society primary adrenal insufficiency guideline (Bornstein) is the AI anchor; steroid neuropsychiatry and thyroid–mood questions are blueprint-friendly.[17]
MD/DNB / NEET-SS. Expect classic lists: myxoedema madness, Cushing depression rates, Addison crisis, and corticosteroid psychiatric adverse effects.[1][16][18]
Landmark names: Warrington, Dubovsky, Sirois, Brown, Ismail, De Bock (steroids); Sonino, Pivonello, Starkman, Piasecka (Cushing); Hage, Feldman, Thomsen, Krüger, Bauer (thyroid); Bornstein (AI guideline); Fairbrother (lithium hyperthyroidism); Wildisen (subclinical hypothyroidism and mood in older adults).[1][2][10][14][17][19][22]
Prognosis and disposition
Thyroid-related psychiatric symptoms often improve with restoration of euthyroidism, though recovery can lag physical stabilisation.[13][14][16] Cushing-related depression and cognition frequently improve after hypercortisolism control, but residual burden is common — plan psychiatric follow-up after cure.[9][10][12] Steroid syndromes often remit with dose reduction.[1][2] AI symptoms improve with adequate replacement and education.[17]
Disposition: shared endocrine–psychiatry or CL follow-up, crisis action plans (AI sick days; thyrotoxic relapse; steroid re-challenge warnings), lithium monitoring schedule, and clear documentation of whether a primary psychiatric diagnosis remains after the organic driver is gone.[1][10][17][19]
Exam pearls
References
- [1]Warrington TP, Bostwick JM Psychiatric adverse effects of corticosteroids Mayo Clin Proc, 2006.PMID 17036562
- [2]Dubovsky AN, Arvikar S, Stern TA, et al. The neuropsychiatric complications of glucocorticoid use: steroid psychosis revisited Psychosomatics, 2012.PMID 22424158
- [3]Sirois F Steroid psychosis: a review Gen Hosp Psychiatry, 2003.PMID 12583925
- [4]Brown ES An epidemiological approach to "steroid psychosis" Am J Psychiatry, 2012.PMID 22549201
- [5]Ismail MF, Lavelle C, Cassidy EM Steroid-induced mental disorders in cancer patients: a systematic review Future Oncol, 2017.PMID 29186986
- [6]De Bock M, Sienaert P Corticosteroids and mania: A systematic review World J Biol Psychiatry, 2024.PMID 38363330
- [7]Sonino N, Fava GA, Raffi AR, et al. Clinical correlates of major depression in Cushing's disease Psychopathology, 1998.PMID 9780396
- [8]Sonino N, Fava GA Psychiatric disorders associated with Cushing's syndrome. Epidemiology, pathophysiology and treatment CNS Drugs, 2001.PMID 11475942
- [9]Sonino N, Fallo F, Fava GA Psychosomatic aspects of Cushing's syndrome Rev Endocr Metab Disord, 2010.PMID 19960264
- [10]Pivonello R, Simeoli C, De Martino MC, et al. Neuropsychiatric disorders in Cushing's syndrome Front Neurosci, 2015.PMID 25941467
- [11]Starkman MN Neuropsychiatric findings in Cushing syndrome and exogenous glucocorticoid administration Endocrinol Metab Clin North Am, 2013.PMID 24011881
- [12]Piasecka M, Papakokkinou E, Valassi E, et al. Psychiatric and neurocognitive consequences of endogenous hypercortisolism J Intern Med, 2020.PMID 32181937
- [13]Hage MP, Azar ST The Link between Thyroid Function and Depression J Thyroid Res, 2012.PMID 22220285
- [14]Feldman AZ, Shrestha RT, Hennessey JV Neuropsychiatric manifestations of thyroid disease Endocrinol Metab Clin North Am, 2013.PMID 24011880
- [15]Thomsen AF, Kvist TK, Andersen PK, et al. Increased risk of affective disorder following hospitalisation with hyperthyroidism - a register-based study Eur J Endocrinol, 2005.PMID 15817908
- [16]Krüger J, Kraschewski A, Jockers-Scherübl MC Myxedema Madness - Systematic literature review of published case reports Gen Hosp Psychiatry, 2021.PMID 34419786
- [17]Bornstein SR, Allolio B, Arlt W, et al. Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline J Clin Endocrinol Metab, 2016.PMID 26760044
- [18]Abdel-Motleb M The neuropsychiatric aspect of Addison's disease: a case report Innov Clin Neurosci, 2012.PMID 23198275
- [19]Fairbrother F, Petzl N, Scott JG, et al. Lithium can cause hyperthyroidism as well as hypothyroidism: A systematic review of an under-recognised association Aust N Z J Psychiatry, 2019.PMID 30841715
- [20]Barbuti M, Carvalho AF, Köhler CA, et al. Thyroid autoimmunity in bipolar disorder: A systematic review J Affect Disord, 2017.PMID 28641149
- [21]Bauer M, Whybrow PC Role of thyroid hormone therapy in depressive disorders J Endocrinol Invest, 2021.PMID 34129186
- [22]Wildisen L, Feller M, Del Giovane C, et al. Effect of Levothyroxine Therapy on the Development of Depressive Symptoms in Older Adults With Subclinical Hypothyroidism: A Randomized Clinical Trial JAMA Netw Open, 2021.PMID 33566107
- [23]Bauer M, Silverman DH, Schlagenhauf F, et al. Brain glucose metabolism in hypothyroidism: a positron emission tomography study before and after thyroid hormone replacement J Clin Endocrinol Metab, 2009.PMID 19435829
- [24]Thomsen AF, Kessing LV Increased risk of hyperthyroidism among patients hospitalized with bipolar disorder Bipolar Disord, 2005.PMID 16026488