Psych · Consultation-liaison psychiatry
Epilepsy and psychiatry
Also known as Postictal psychosis · Peri-ictal psychosis · Interictal psychosis · Forced normalisation · Forced normalization · Alternative psychosis · Epilepsy and depression · Psychiatric comorbidities of epilepsy · AED psychiatric side effects
Exam-exhaustive fellowship topic on the epilepsy–psychiatry interface: peri-ictal and postictal psychosis, interictal depression, forced normalisation, AED psychiatric adverse effects, psychotropics and seizure threshold, screening, suicide risk, and joint CL–neurology management. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Psychiatrists fail this topic when they treat every psychotic episode in a person with epilepsy (PWE) as primary schizophrenia, when they miss the lucid interval of postictal psychosis, or when they refuse antidepressants out of exaggerated seizure fear while leaving depression — the main quality-of-life and suicide driver — untreated.[3][7][13]
Overview and definition
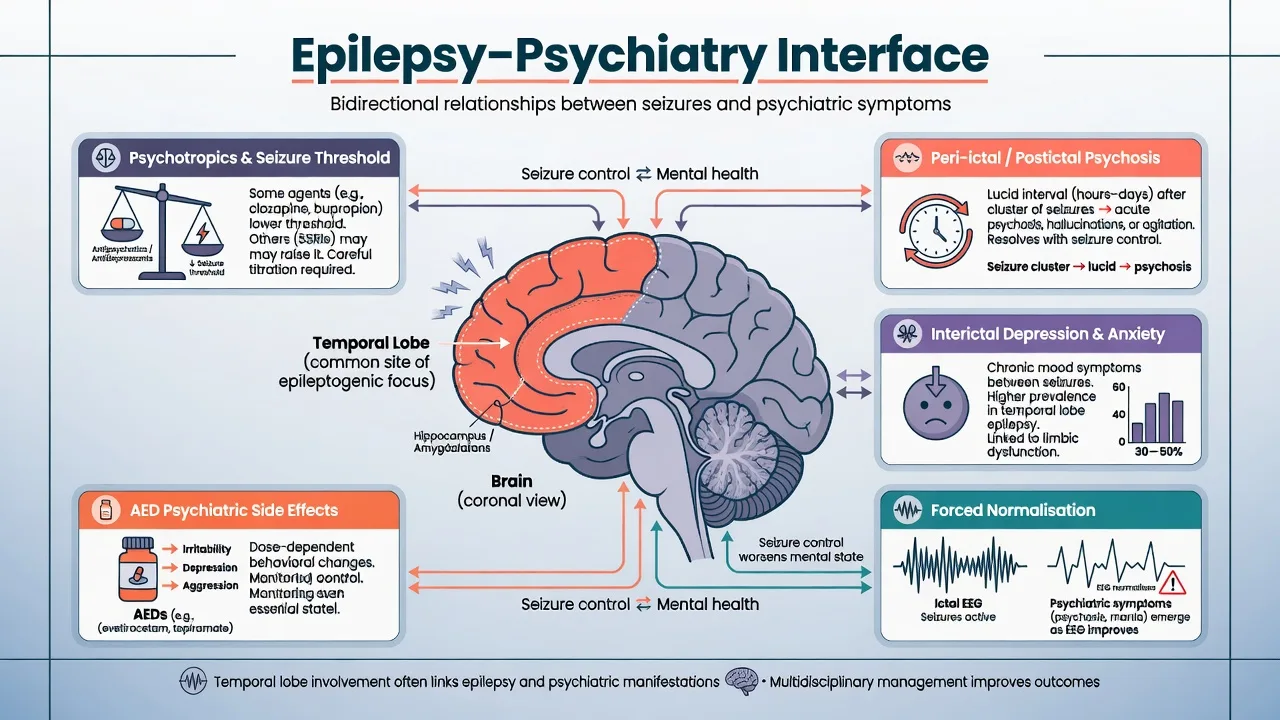
Epilepsy–psychiatry interface covers psychiatric syndromes that are temporally linked to seizures, chronic interictal comorbidity, treatment-emergent psychiatric effects of antiepileptic drugs (AEDs / antiseizure medications), and the effects of psychotropics on seizure threshold. In DSM-5-TR language many acute syndromes map to mental disorder due to another medical condition; ICD-11 emphasises mental disorders due to disorders of the nervous system. The clinical task is not the label alone — it is timing, EEG context, AED changes, risk, and joint care.[9][14]
Epidemiology and bidirectional risk
Community data show substantially higher rates of mood, anxiety, and other mental disorders in PWE than in people without epilepsy.[2] Systematic synthesis finds mood disorders (about one-third in pooled estimates) and anxiety disorders as the most frequent psychiatric comorbidities; psychosis is less common but still enriched, especially in temporal lobe epilepsy (TLE).[14] Meta-analysis estimates pooled psychosis prevalence around 5.6% in epilepsy, higher in TLE cohorts than in unselected samples.[3]
The relationship is not only consequence of chronic illness. Prior major depression and suicide attempt increase risk of subsequent unprovoked seizures, and bidirectional links among epilepsy, psychiatric disorders, and suicidality are well documented — examiners use this to reject purely psychosocial explanations of comorbidity.[5][6]
Classification by temporal relationship
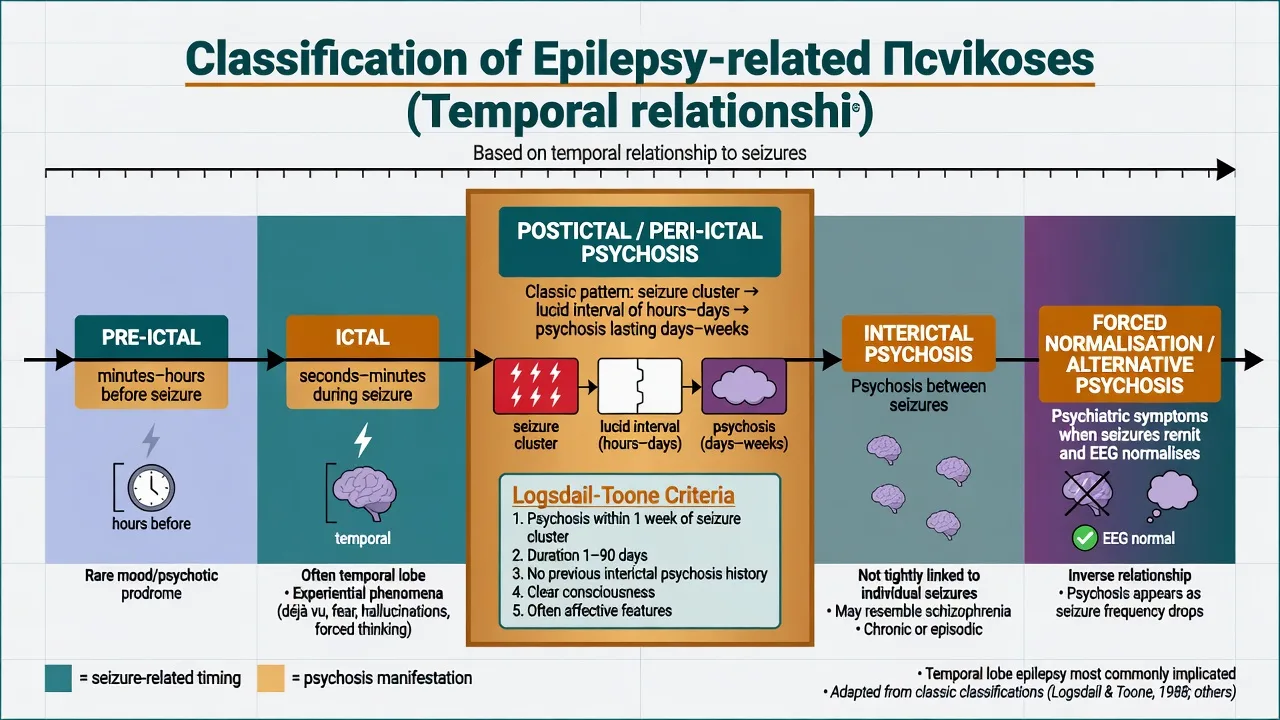
Examiners expect a clock-based classification, not a vague "epileptic personality" concept.[1][4]
| Timing | Typical window | Core features | Key discriminators |
|---|---|---|---|
| Pre-ictal | Minutes–hours before seizure | Mood change, irritability, rare psychotic prodrome | Resolves with or into the seizure |
| Ictal | Seconds–minutes during seizure | Experiential phenomena, fear, automatisms; rarely prolonged psychotic behaviour alone | EEG correlate; ends with seizure |
| Postictal / peri-ictal psychosis | Hours–days after seizures, often after lucid interval | Delusions, hallucinations, affective colouring; risk of violence | Logsdail–Toone framework; not mere confusion |
| Interictal | Between seizures, not tightly seizure-linked | Depression, anxiety, chronic or episodic psychosis | Can resemble primary psychiatric disorders |
| Forced normalisation | When seizures remit and EEG improves | Psychosis, mania, or other psychiatric worsening | Inverse seizure–psychiatry relationship |
Postictal (peri-ictal) psychosis — Logsdail–Toone
Postictal psychosis (PIP) remains the classic CL emergency. Logsdail and Toone described episodes of confusion or psychosis beginning immediately after a seizure or within about a week of return toward baseline mental state, lasting from about 24 hours up to about three months, with clouding/delirium, clear-consciousness psychosis, or a mix, after excluding AED toxicity, established interictal psychosis, nonconvulsive status, recent head injury, and intoxication as sole causes.[1]
Exam pattern: often a cluster of seizures (especially in chronic TLE) → lucid interval of hours to a few days → florid psychosis lasting days to weeks. Content is frequently affective, religious, or grandiose; insight is poor; aggression and self-harm can appear suddenly.[1][3] Immediate postictal confusion/delirium is not the same diagnosis — the lucid interval is the discriminator that examiners reward.
Risk factors repeatedly cited include long epilepsy duration, seizure clustering, bilateral independent discharges or temporal involvement, and prior PIP. Some patients later develop interictal psychosis; treat each acute episode as high risk even if historically self-limited.[3][15]
Interictal depression and anxiety
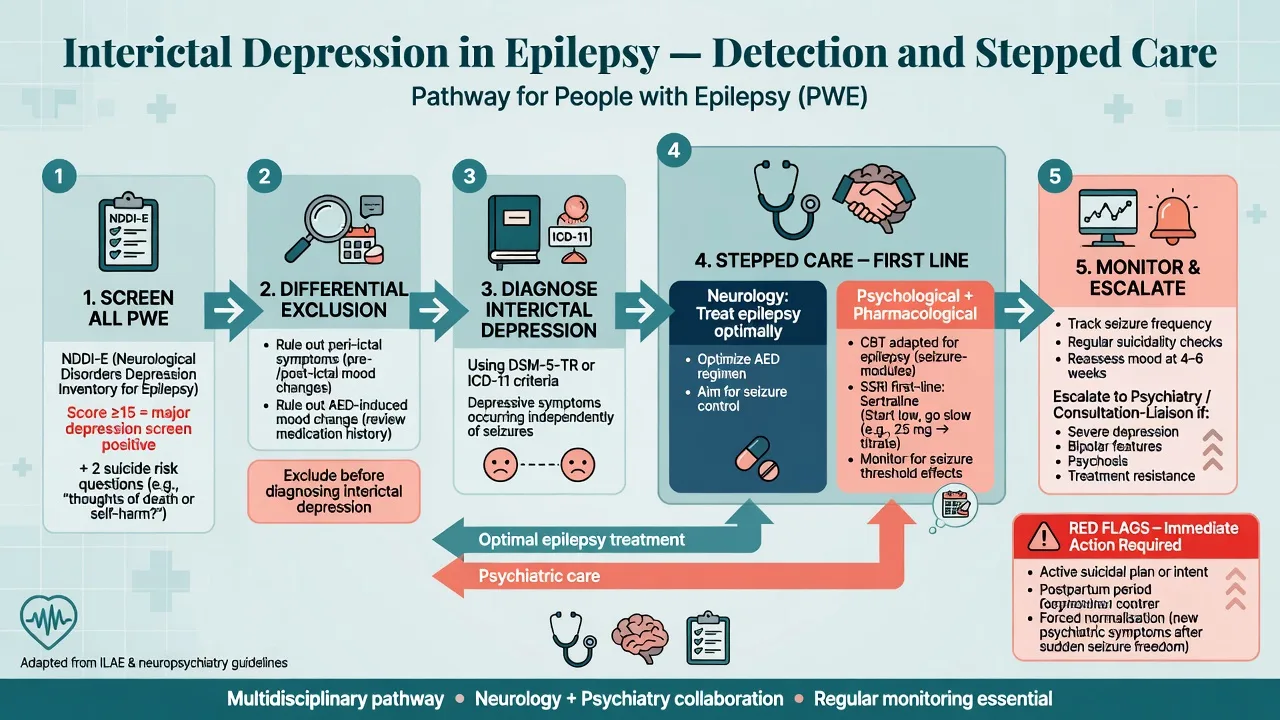
Interictal depression is the workhorse comorbidity: symptoms between seizures that meet criteria for major depression or other depressive disorders, not explained solely by peri-ictal mood swings. Anxiety disorders are similarly enriched. Depression strongly worsens quality of life, adherence, and suicide risk and must be screened for actively rather than assumed "understandable."[2][7][14]
Forced normalisation / alternative psychosis
Forced normalisation (Landolt concept; modern reviews by Krishnamoorthy, Trimble and colleagues) describes psychiatric deterioration — classically psychosis, also mania or other syndromes — when seizures improve and the EEG becomes more normal. Alternative psychosis is the clinical counterpart: psychiatric symptoms substitute for seizures. Recognition prevents the trap of congratulating seizure freedom while the patient is decompensating psychiatrically; management is multidisciplinary and may require careful trade-offs in seizure suppression versus psychiatric stability.[4]
Pathophysiology (viva depth)
Shared limbic and temporal network vulnerability links TLE to mood and psychosis. PIP has been conceptualised as a postictal inhibitory or network rebound state after intense epileptic activity; forced normalisation suggests an inverse electroclinical–psychiatric relationship rather than random coincidence.[1][4] Bidirectional epidemiology implies shared genetic, developmental, and stress-related pathways — depression is not merely reactive demoralisation.[5][6] AED mechanisms (e.g. SV2A modulation with levetiracetam; AMPA antagonism with perampanel; carbonic anhydrase/cognitive effects with topiramate) help explain behavioural adverse-effect profiles without requiring memorisation of every receptor for the exam.[12]
Clinical assessment for CL
Structure history around: seizure variables (type, frequency, clustering, last cluster, recent status, surgery candidacy); timeline of psychiatric symptoms relative to seizures and recovery of orientation; AED list (new starts, rapid titration, withdrawal, adherence, levels); psychotropic list (especially bupropion, clozapine, high-dose FGAs/TCAs); substance use, sleep deprivation, infection, head injury; risk (suicide, violence, vulnerability, parenting, driving); and capacity with jurisdiction-specific emergency legal frameworks (do not invent section numbers).[9][15]
MSE language should capture lucidity, orientation, affective colouring of delusions, catatonia, and fluctuating alertness that might signal NCSE or delirium rather than primary psychosis.[9][15]
Screening: NDDI-E
The Neurological Disorders Depression Inventory for Epilepsy (NDDI-E) is a brief validated screen designed to minimise contamination by AED side-effect language. In the multicentre development study, an NDDI-E score greater than 15 identified major depression with good sensitivity and specificity for clinical use as a screen (not a standalone diagnosis).[8] Pair with direct suicide questions every time.
Differential diagnosis
- Postictal confusion / delirium — immediate, resolves as postictal state clears; no delayed lucid-interval psychosis.
- Nonconvulsive status epilepticus — ongoing behavioural or cognitive change; needs EEG.
- AED toxicity or withdrawal.
- Primary psychotic or bipolar disorder coincidental with epilepsy.
- Substance-induced states; alcohol withdrawal seizures plus psychosis.
- Autoimmune encephalitis and other organic psychoses when tempo is subacute and neurologic red flags appear.
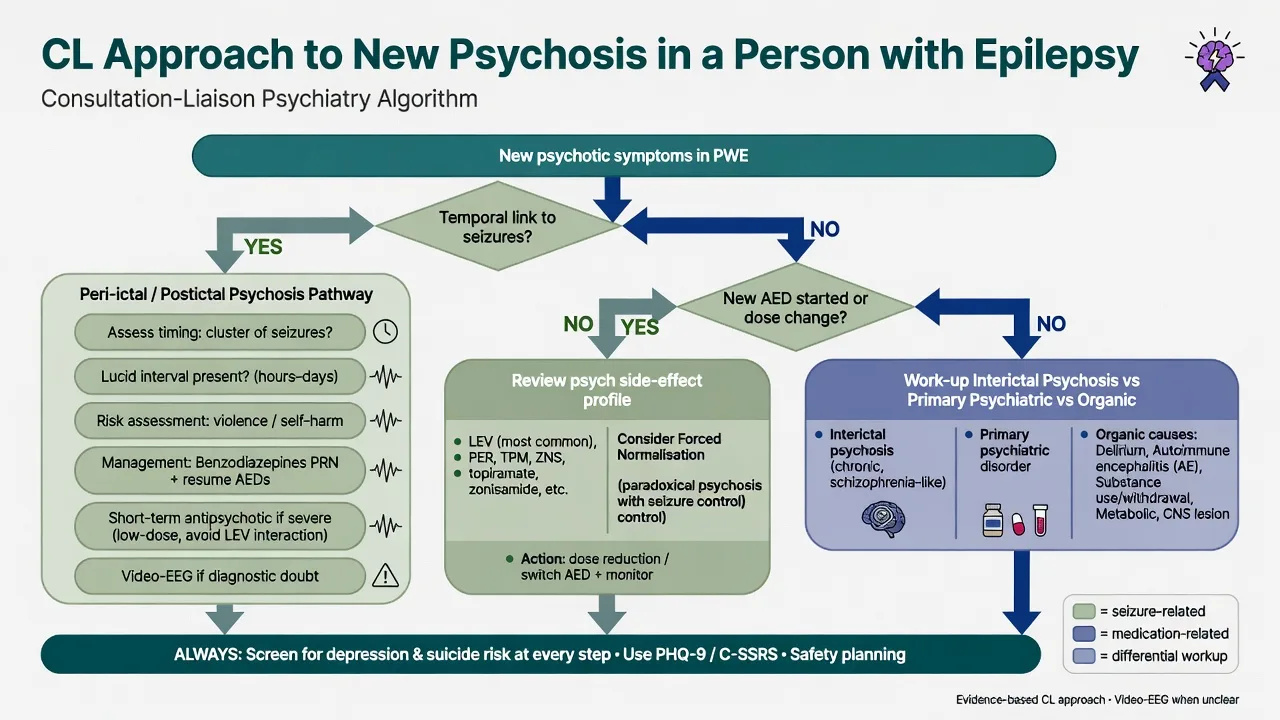
- Forced normalisation vs new AED psychiatric adverse effect vs true interictal psychosis — use timing, EEG, and drug history together.[4][9]
Investigations
Escalate with neurology when the presentation is atypical, progressive, or unsafe: EEG / video-EEG if NCSE, ictal psychosis, or diagnostic uncertainty; review MRI and epilepsy work-up (do not re-image every behavioural episode without indication); metabolic panel and infection screen as indicated; AED levels when non-adherence or toxicity suspected; standard psychotropic baselines (ECG, metabolic) before antipsychotics or cardiac-risk agents; pregnancy test when relevant before valproate discussions or teratogenic combinations.[9][15]
Acute management
Postictal psychosis
Acute PIP care: safety first (low-stimulus environment, continuous observation if risk high, treat medical complications of seizures); restore antiseizure coverage (missed doses and withdrawal are common precipitants — involve neurology early); benzodiazepines for agitation per local protocol and respiratory status; short-term antipsychotic if psychosis is severe or dangerous — lowest effective dose of a lower seizure-risk agent, with early review as PIP is often time-limited; exclude NCSE if consciousness remains impaired or the course is atypical; document capacity and use the least-restrictive legal pathway available in your jurisdiction if capacity is lacking.[15][11][1]
Forced normalisation
Do not automatically reverse all seizure gains. Coordinate with neurology: options include careful AED adjustment, treating the psychiatric syndrome with appropriate psychotropics, and addressing sleep, substances, and psychosocial stressors. The concept is a shared decision problem, not a single drug trick.[4][9]
Definitive management of interictal depression
Treat depression actively. Consensus statements support evaluation for affective disorders in all PWE and combined use of epilepsy optimisation, psychotherapy, and pharmacotherapy when indicated.[7][9] Cochrane review evidence for antidepressants in epilepsy is limited in trial volume but does not support therapeutic nihilism; clinical practice prefers SSRIs as first-line pharmacological options with monitoring of seizures and suicidality.[13]
Example starting approach (adult, non-pregnant, after interaction check): sertraline 25–50 mg oral daily, titrate slowly (e.g. toward 50–100 mg as tolerated; some patients need higher usual antidepressant range under review), reassess mood and seizures at 2–4 weeks, watch hyponatraemia and activation/suicidality especially early in treatment. Adapt agent choice for interactions with enzyme-inducing AEDs (carbamazepine, phenytoin, phenobarbital) which can lower some antidepressant levels.[7][12][13]
Psychological therapies (CBT adapted for epilepsy, behavioural activation) are appropriate first-line or adjunctive interventions, especially in mild–moderate depression and when patients prefer non-drug care.[7][9]
AED psychiatric adverse effects
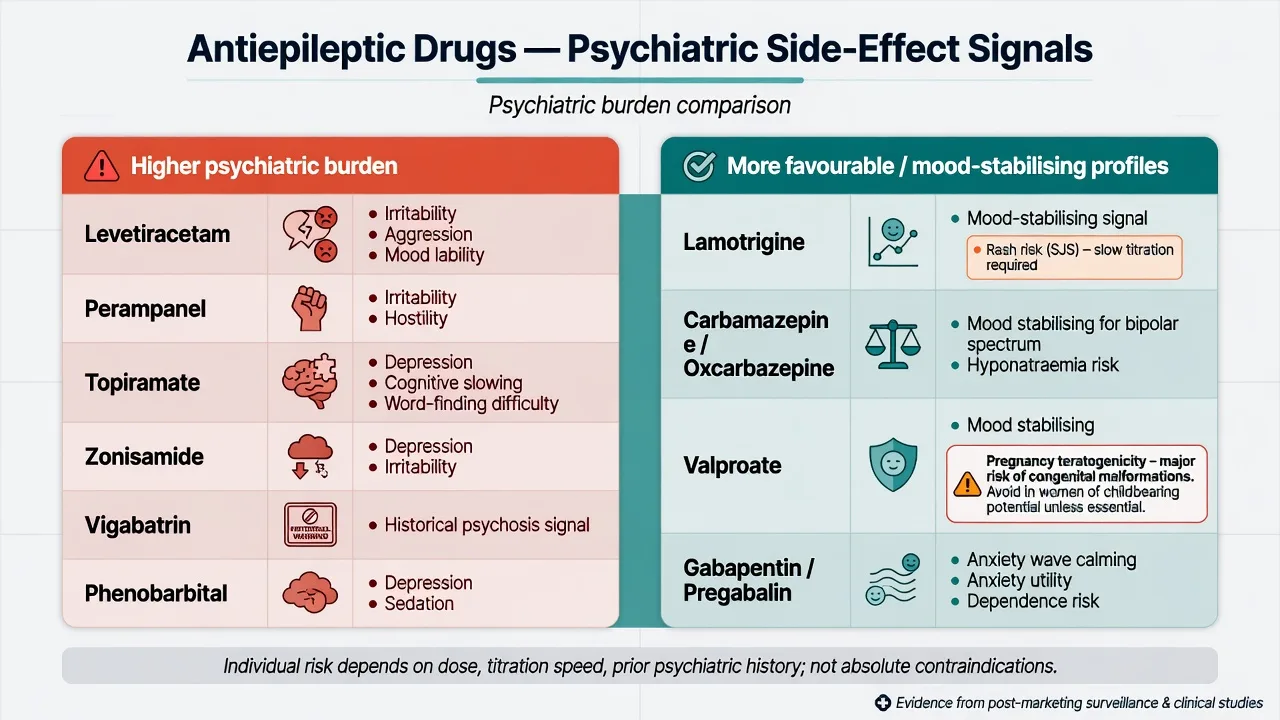
Psychiatric adverse effects are a major CL referral reason. Drug selection should consider both seizure syndrome and psychiatric vulnerability.[12]
Higher behavioural/psychiatric burden signals (not absolute bans) include levetiracetam (irritability, aggression, mood lability — common exam stem), perampanel (irritability, hostility, aggression especially with rapid titration or higher doses), topiramate (depression, cognitive slowing, word-finding difficulty, anorexia), zonisamide (mood and behavioural change in some patients), phenobarbital (depression, sedation, cognitive dulling), and vigabatrin (historical psychosis signal in some series).[12]
Often more favourable for mood (with major caveats): lamotrigine (mood-stabilising signal; slow titration mandatory for rash/SJS risk), carbamazepine / oxcarbazepine (mood-stabilising properties; hyponatraemia and interactions), valproate (effective mood stabiliser but high teratogenicity — avoid in people who can become pregnant unless no suitable alternative and robust pregnancy prevention under local rules), and gabapentin / pregabalin (anxiolytic utility; misuse/dependence risk).[12]
Rapid polytherapy changes, high doses, and prior psychiatric illness amplify risk. When psychiatric symptoms track an AED start or up-titration, dose reduction or switch with neurology often beats stacking antipsychotics alone.[12][16]
AEDs and suicidality labelling
Regulatory warnings have linked AEDs as a class to suicidal thoughts and behaviour. Updated clinical reviews emphasise clinical suicide assessment in context (depression, psychosis, psychosocial stress, forced normalisation) rather than automatic avoidance of needed AEDs. Treat the person, not the boxed warning alone.[16]
Psychotropics and seizure threshold
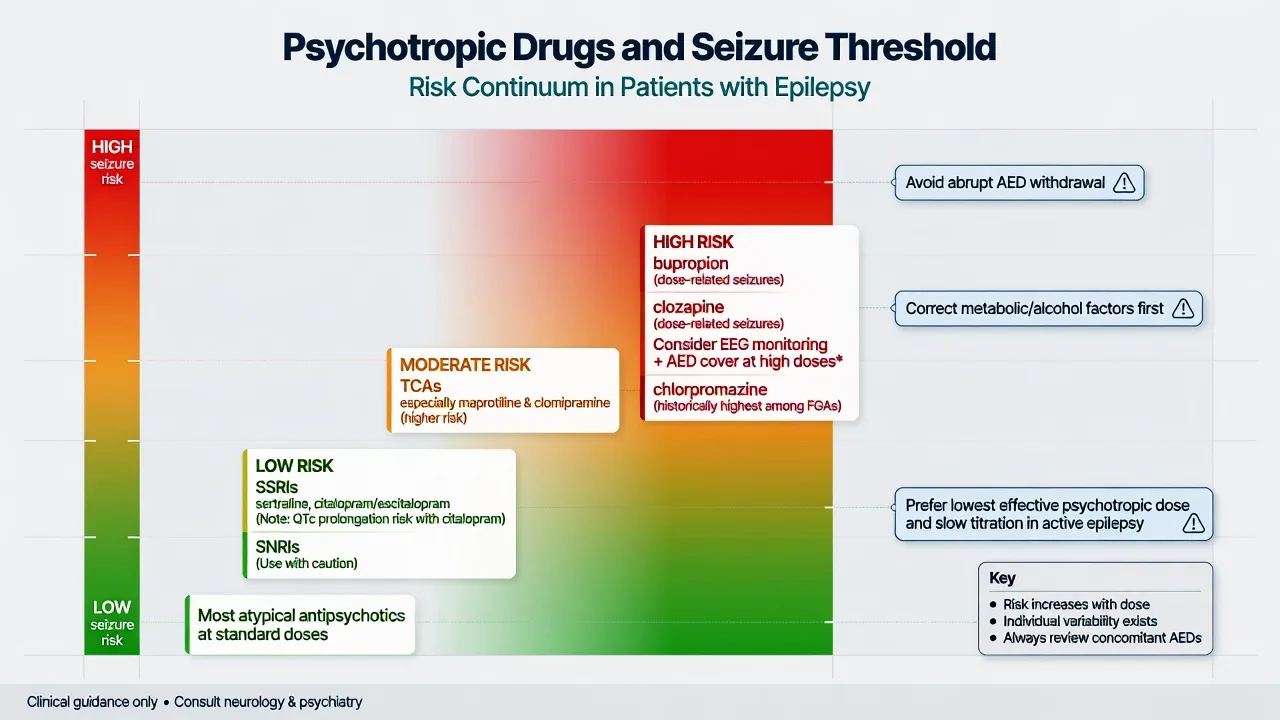
Not all psychotropics are equal. Analyses of FDA clinical trial datasets and clinical reviews place bupropion and clozapine among the highest seizure-association psychotropics; maprotiline and some TCAs also carry higher risk; SSRIs as a group are comparatively favourable at usual doses.[10][11]
Practical ladder for fellowship answers: prefer SSRIs (e.g. sertraline, citalopram/escitalopram with QTc attention) and many second-generation antipsychotics at standard doses when psychosis requires treatment; caution with SNRIs, higher-dose TCAs, and rapid titration of any agent; high concern for bupropion (especially IR/high dose), clozapine (dose-related seizures — consider EEG, slower titration, and AED cover with neurology when high dose is essential), and chlorpromazine among older FGAs. Always correct alcohol withdrawal, hyponatraemia, sleep deprivation, and AED non-adherence before blaming the psychotropic alone.[10][11][15]
Psychosis pharmacotherapy in epilepsy
Specialist consensus on pharmacotherapy for psychosis in PWE stresses individualised antipsychotic choice, attention to interactions with enzyme-inducing AEDs, avoidance of unnecessary polypharmacy, and close neurology collaboration — especially for clozapine or when epilepsy is unstable.[15]
Special populations
Special populations: intellectual disability (behavioural phenotypes, higher polypharmacy, communication barriers — carefully separate seizures, pain, and environment from challenging behaviour); adolescents (levetiracetam irritability is a frequent stem; involve family and school); older adults (delirium risk, hyponatraemia with CBZ/OXC, fall risk with sedating agents); pregnancy (valproate teratogenicity dominates; lamotrigine and levetiracetam are common epilepsy choices — coordinate perinatal psychiatry and neurology; do not stop AEDs abruptly); cultural formulations (seizure phenomena may be framed as spirit possession — still apply medical risk assessment while respecting explanatory models).[9][12]
Prognosis and disposition
PIP is often self-limited over days to weeks but recurs and can evolve toward interictal psychosis in a subset — plan follow-up, not only acute sedation.[1][3] Depression and suicide risk frequently outlast seizure control milestones; disposition should include epilepsy clinic plus mental health review, safety planning, and clear advice on alcohol, sleep, and AED adherence. Driving and occupational risk after psychosis or breakthrough seizures follow local legal standards, not examiner-invented rules.[7][9]
Regional notes
ANZ (FRANZCP): Co-manage with neurology/epilepsy services; use local Mental Health Act principles when capacity is lacking — name the need for jurisdiction-specific orders without inventing section numbers. Screen depression in epilepsy clinics; NDDI-E is widely taught. Valproate pregnancy prevention rules are high-stakes for CL advice. UK (MRCPsych): collaborative care and CASC explanation of PIP or AED side effects. US (ABPN): FDA AED suicidality labelling — answer with clinical suicide assessment and continued indicated AED therapy when benefits outweigh risks. South Asia (MD/DNB, NEET-SS): resource-variable EEG access; prioritise timing history, AED review, and safety; phenobarbital remains more visible in some formularies with depression/sedation effects.[8][9][16]
Exam pearls
POST-ICTAL
Summary
The epilepsy–psychiatry interface is a CL core competency: time the syndrome, treat PIP as a dangerous but often reversible emergency, screen and treat interictal depression without irrational antidepressant avoidance, recognise forced normalisation and AED behavioural toxicity, prescribe psychotropics with seizure-threshold awareness, and share ownership with neurology. A candidate who masters timing, Logsdail–Toone, NDDI-E, LEV/TPM/perampanel signals, and the bupropion/clozapine seizure ladder can answer the board questions that separate pass from distinction.[1][7][9][12][15]
References
- [1]Logsdail SJ, Toone BK Post-ictal psychoses. A clinical and phenomenological description Br J Psychiatry, 1988.PMID 3167343
- [2]Tellez-Zenteno JF, Patten SB, Jetté N, Williams J, Wiebe S Psychiatric comorbidity in epilepsy: a population-based analysis Epilepsia, 2007.PMID 17662062
- [3]Clancy MJ, Clarke MC, Connor DJ, Cannon M, Cotter DR The prevalence of psychosis in epilepsy; a systematic review and meta-analysis BMC Psychiatry, 2014.PMID 24625201
- [4]Krishnamoorthy ES, Trimble MR, Sander JW, Kanner AM Forced normalization at the interface between epilepsy and psychiatry Epilepsy Behav, 2002.PMID 12609326
- [5]Hesdorffer DC, Hauser WA, Olafsson E, Ludvigsson P, Kjartansson O Depression and suicide attempt as risk factors for incident unprovoked seizures Ann Neurol, 2006.PMID 16217743
- [6]Hesdorffer DC, Ishihara L, Mynepalli L, Webb DJ, Weil J, Hauser WA Epilepsy, suicidality, and psychiatric disorders: a bidirectional association Ann Neurol, 2012.PMID 22887468
- [7]Barry JJ, Ettinger AB, Friel P, et al. Consensus statement: the evaluation and treatment of people with epilepsy and affective disorders Epilepsy Behav, 2008.PMID 18502183
- [8]Gilliam FG, Barry JJ, Hermann BP, Meador KJ, Vahle V, Kanner AM Rapid detection of major depression in epilepsy: a multicentre study Lancet Neurol, 2006.PMID 16632310
- [9]Kerr MP, Mensah S, Besag F, et al. International consensus clinical practice statements for the treatment of neuropsychiatric conditions associated with epilepsy Epilepsia, 2011.PMID 21955156
- [10]Alper K, Schwartz KA, Kolts RL, Khan A Seizure incidence in psychopharmacological clinical trials: an analysis of Food and Drug Administration (FDA) summary basis of approval reports Biol Psychiatry, 2007.PMID 17223086
- [11]Pisani F, Oteri G, Costa C, Di Raimondo G, Di Perri R Effects of psychotropic drugs on seizure threshold Drug Saf, 2002.PMID 11888352
- [12]Mula M Epilepsy and Psychiatric Comorbidities: Drug Selection Curr Treat Options Neurol, 2017.PMID 29046989
- [13]Maguire MJ, Marson AG, Nevitt SJ Antidepressants for people with epilepsy and depression Cochrane Database Syst Rev, 2021.PMID 33860531
- [14]Lu E, Pyatka N, Burant CJ, Sajatovic M Systematic Literature Review of Psychiatric Comorbidities in Adults with Epilepsy J Clin Neurol, 2021.PMID 33835737
- [15]de Toffol B, Trimble M, Hesdorffer DC, et al. Pharmacotherapy in patients with epilepsy and psychosis Epilepsy Behav, 2018.PMID 30241054
- [16]Mula M Suicidality and antiepileptic drugs in people with epilepsy: an update Expert Rev Neurother, 2022.PMID 35394392