Psych · Consultation-liaison psychiatry
Functional neurological disorder in the medical setting
Also known as FND consultation-liaison · Functional neurological disorder ward · Conversion disorder medical setting · Functional seizures ED · Dissociative seizures hospital · PNES inpatient · Functional weakness ward · Neuropsychiatry liaison FND
Exam-exhaustive C-L fellowship leaf on functional neurological disorder in the medical setting — liaison role, positive rule-in diagnosis, bedside explanation as first treatment, ward and ED management of functional seizures and weakness, staff countertransference, stopping iatrogenesis, MDT discharge planning, dual pathology, and deliberate distinction from the general-adult FND clinic leaf. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
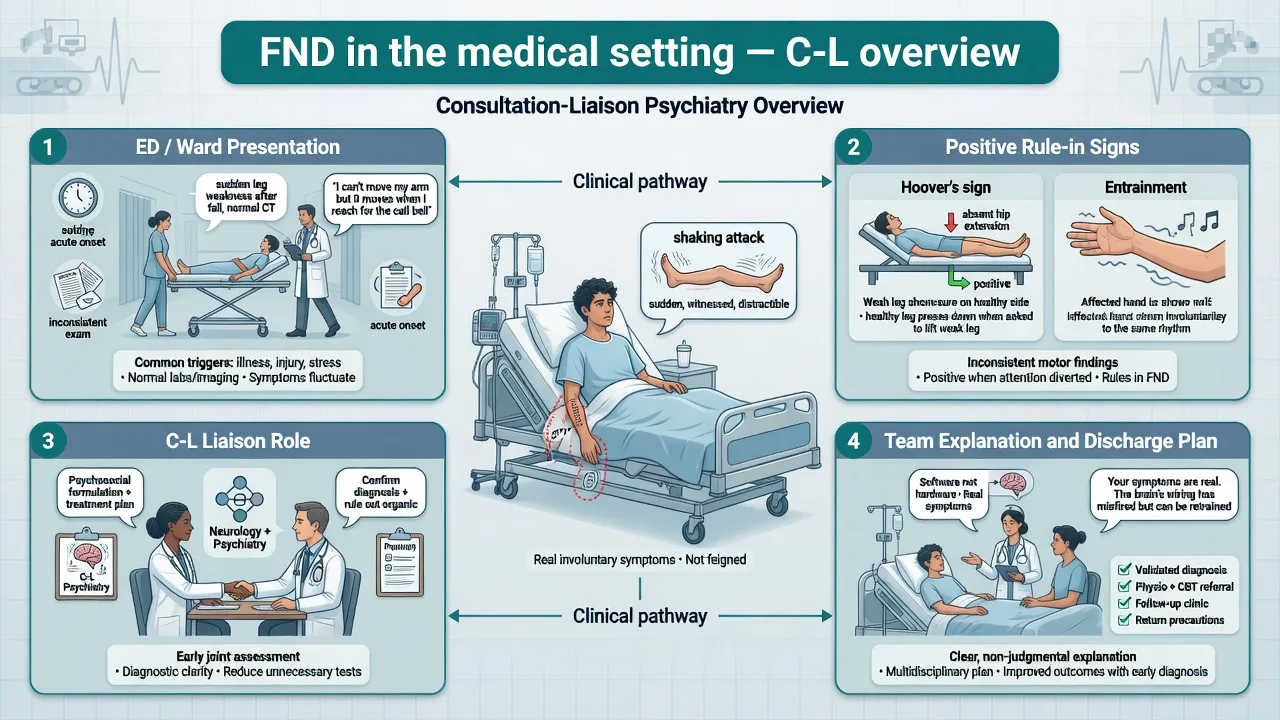
This leaf is the consultation-liaison companion to the general-adult FND clinic topic. Examiners want the registrar who can run a ward consult: clarify the referral question, keep emergency pathways open, name positive signs, repair pejorative language, and leave a written plan the medical team can own.[3][4][19]
Overview and definition (C-L framing)
Functional neurological symptom disorder (FNSD), commonly functional neurological disorder (FND), describes clinically recognisable alterations of voluntary motor or sensory function — weakness, movement disorders, sensory loss, speech change, or attacks resembling epilepsy — that are incompatible with recognised disease pathways yet cause genuine distress and disability.[1][2][3]
On medical, surgical, and emergency pathways the phenotype is the same as in outpatient neuropsychiatry, but the system context differs: fragmented teams, stroke and seizure pathways, staff countertransference, pressure to empty beds, and the risk that “psych consult” becomes a euphemism for discharge without explanation.[4][19]
Classification and C-L framework
DSM-5-TR and ICD-11
DSM-5-TR retains Functional Neurological Symptom Disorder (Conversion Disorder) with symptom-type specifiers (weakness/paralysis, abnormal movement, swallowing, speech, attacks/seizures, anaesthesia/sensory loss, mixed), acute versus persistent course, and with/without psychological stressor. A psychological stressor is not required for diagnosis.[1][3]
ICD-11 frames dissociative neurological symptom disorder, aligning with modern rejection of pejorative hysteria language while still locating the disorder among dissociative phenomena in classification space.[2][3]
How this leaf differs from general-adult FND
This C-L leaf emphasises ward systems, bedside explanation, and discharge interface rather than the full outpatient clinic catalogue covered in the general-adult FND topic.[3][4][19]
| Focus | General-adult FND leaf | This C-L leaf |
|---|---|---|
| Setting | Clinic / FND service | ED, ward, consult |
| Core skill | Full phenotype and trial depth | Liaison role, explanation, systems |
| Audience | Patient + outpatient MDT | Patient + medical team + nursing |
| Risk emphasis | Disability, driving, dual pathology | Hyperacute mimics, iatrogenesis, abandonment |
| Disposition | Specialist physio/psychology | Same pathway plus ward exit plan |
Epidemiology and service burden
Symptoms unexplained by organic disease are common in neurology practice; in a landmark Scottish outpatient cohort of 1144 new neurology patients, a substantial minority had symptoms unexplained by organic disease, with low rates of later reclassification to a different disease explanation at follow-up when the functional diagnosis was made carefully.[9]
These patients carry high disability, distress, and unemployment relative to many recognised neurological diseases — a key C-L talking point when teams minimise symptoms as “soft”.[10] Epidemiology reviews place FND among the commonest reasons for neurology referral after headache, with meaningful ED and inpatient footprint.[11]
Stressful life events and maltreatment are associated with FND in meta-analysis but are neither necessary nor sufficient; do not withhold diagnosis or force a trauma narrative on the ward.[12]
Mechanisms relevant to the ward
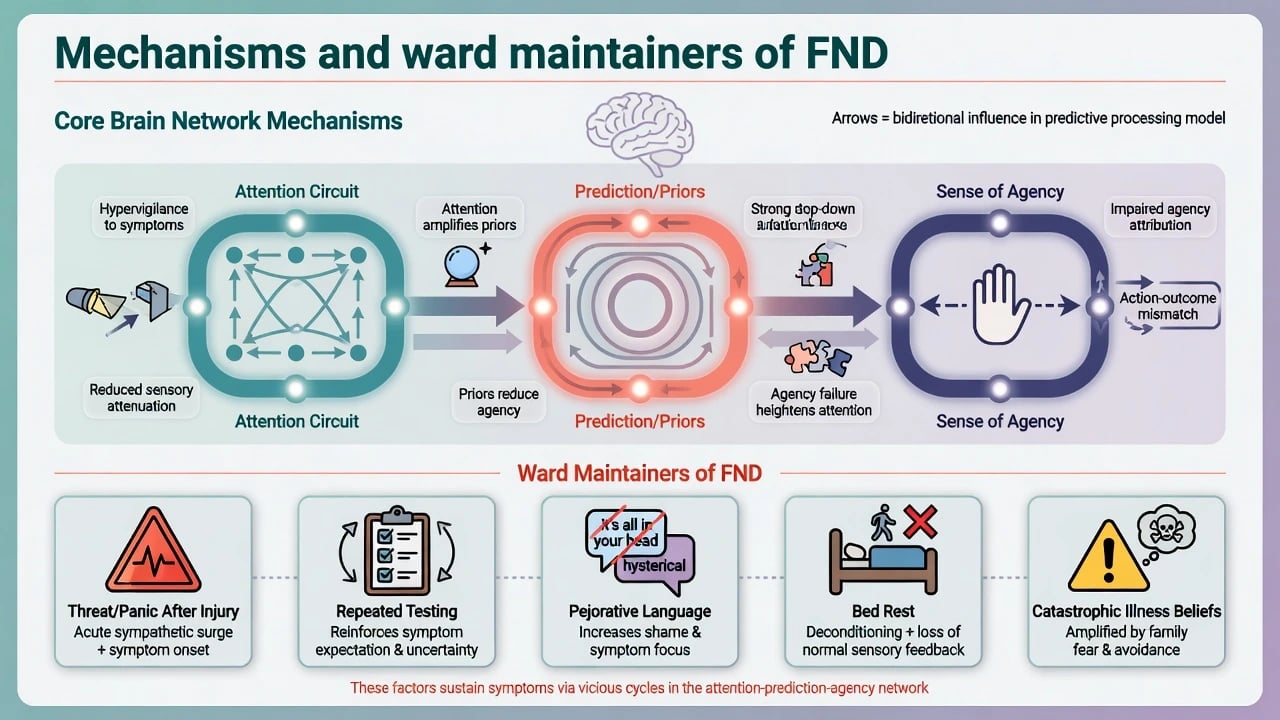
A Bayesian / predictive-coding account proposes abnormally precise prior beliefs about symptoms that override sensory evidence, producing involuntary motor and sensory phenomena without classic structural lesions explaining the phenotype.[7] Resting-state work in functional movement disorder has linked impaired self-agency to right temporoparietal junction network alterations — useful viva language, not a bedside biomarker.[8]
Shared mechanisms across functional seizures, functional motor phenotypes, and related functional neurological syndromes are synthesised in contemporary reviews.[2] On the ward, attention, expectation, dissociation, illness threat after injury or procedure, and medicalisation are practical maintaining factors the C-L psychiatrist can target in the formulation and team plan.[3][4][19]
Clinical presentation on medical pathways
Functional motor and sensory phenotypes
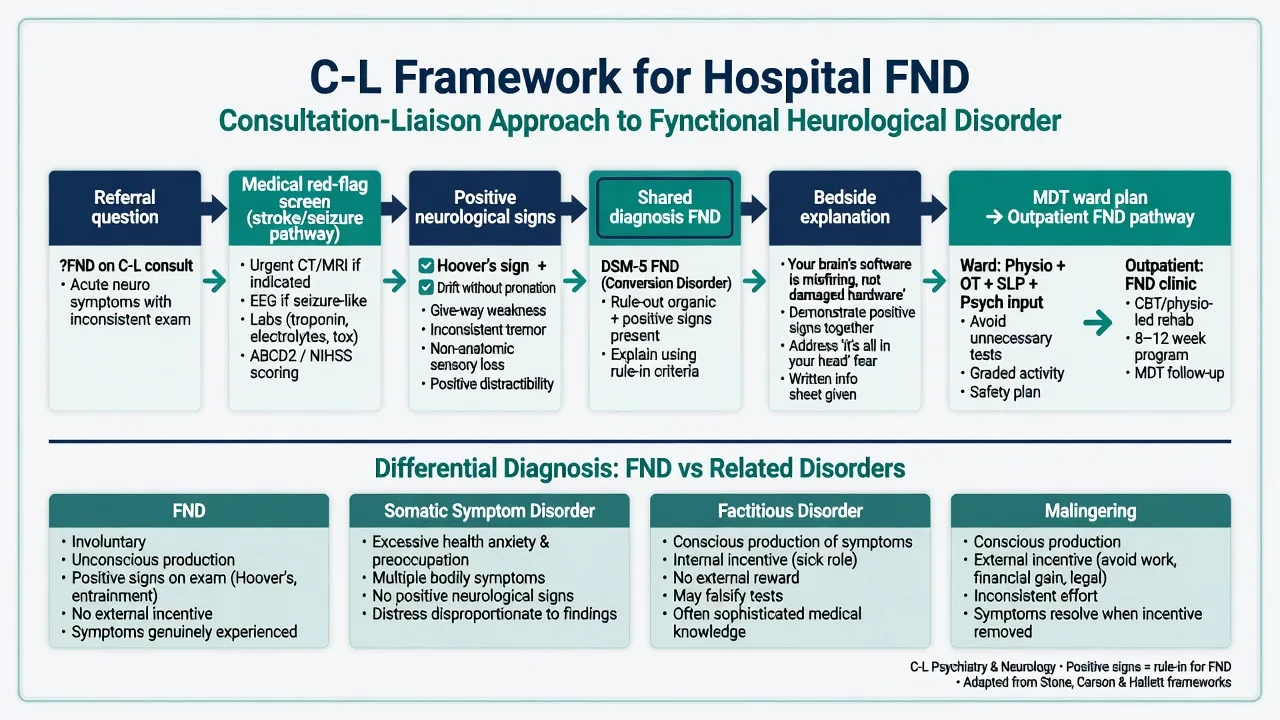
Look for internal inconsistency: Hoover’s sign and hip abductor sign in functional weakness; give-way weakness; tremor entrainment and distractibility; fixed functional dystonia after minor injury; gait patterns that fluctuate with attention; sensory loss that does not follow neuroanatomical boundaries yet is subjectively real.[5][6][1]
Functional / dissociative seizures
Common C-L and ED presentations include prolonged shaking, closed eyes, fluctuating responsiveness, and events in front of staff. No single bedside feature is pathognomonic; video-EEG of a typical event without epileptiform correlate is the reference standard when diagnosis is uncertain or dual epilepsy is possible.[1][3][15] Prefer language: functional seizures / dissociative seizures / FND with attacks rather than pejorative “pseudoseizure” used dismissively.[4]
C-L systems features
Document the patient’s illness beliefs, what they have already been told, family anxiety, nursing observations of inconsistency, and any pejorative language already in the chart — these often determine whether explanation will succeed.[4][19]
Differential diagnosis on the ward
Key discriminators for the ward differential include the following.[1][3][19]
- Stroke / TIA / spinal emergency — time-critical vascular and cord features override functional pattern-matching until cleared.[19]
- MS, myasthenia, GBS, MND — progressive UMN/LMN or fatigable patterns versus inconsistency and positive signs.[1]
- Epilepsy — dual diagnosis possible; video-EEG when needed.[3][15]
- Encephalitis, catatonia, metabolic/toxic encephalopathy, delirium — fever, fluctuating consciousness with medical drivers, or catatonic signs redirect the consult.[3]
- Factitious disorder / malingering — require evidence of intentional production or clear external secondary gain with deception; rare defaults that destroy alliance if misused.[1][3]
- Somatic symptom disorder and health anxiety — distress and preoccupation may co-travel but lack FND-specific positive motor signs.[3]
Assessment: the C-L consult structure
- Clarify the referral question — diagnosis support, risk, capacity, disposition, or “please take over” frustration? Reframe toward joint ownership with neurology/medicine.[4][19]
- Review what neurology has already found — positive signs, imaging, EEG; do not re-do a full negative work-up for its own sake.[5][9]
- History — onset (often sudden), triggers (injury, panic, procedure, bad news), fluctuations with attention, prior functional symptoms, psychiatric comorbidity, trauma carefully and non-coercively.[3][12]
- MSE and risk — mood, suicidality, dissociation, substance use; injury risk during attacks; driving; vulnerability; capacity for treatment decisions under local law (do not invent statute numbers).[3]
- Show positive signs when appropriate — transparent demonstration can be therapeutic when done respectfully with consent.[4][5]
Investigations
Investigations follow the differential, not a ritual to “prove” functional symptoms. MRI, EEG, labs, and video-EEG are indicated for red flags, atypical first presentations, or dual pathology — not as a substitute for clinical rule-in signs.[1][3][9] Absence of imaging abnormality is not itself the diagnostic criterion.[1][5]
C-L advocacy often means stopping non-indicated invasive tests while writing a clear safety-net for new red flags so the team does not feel abandoned into uncertainty.[4][19]
Acute ward and ED management
Functional seizures on the ward
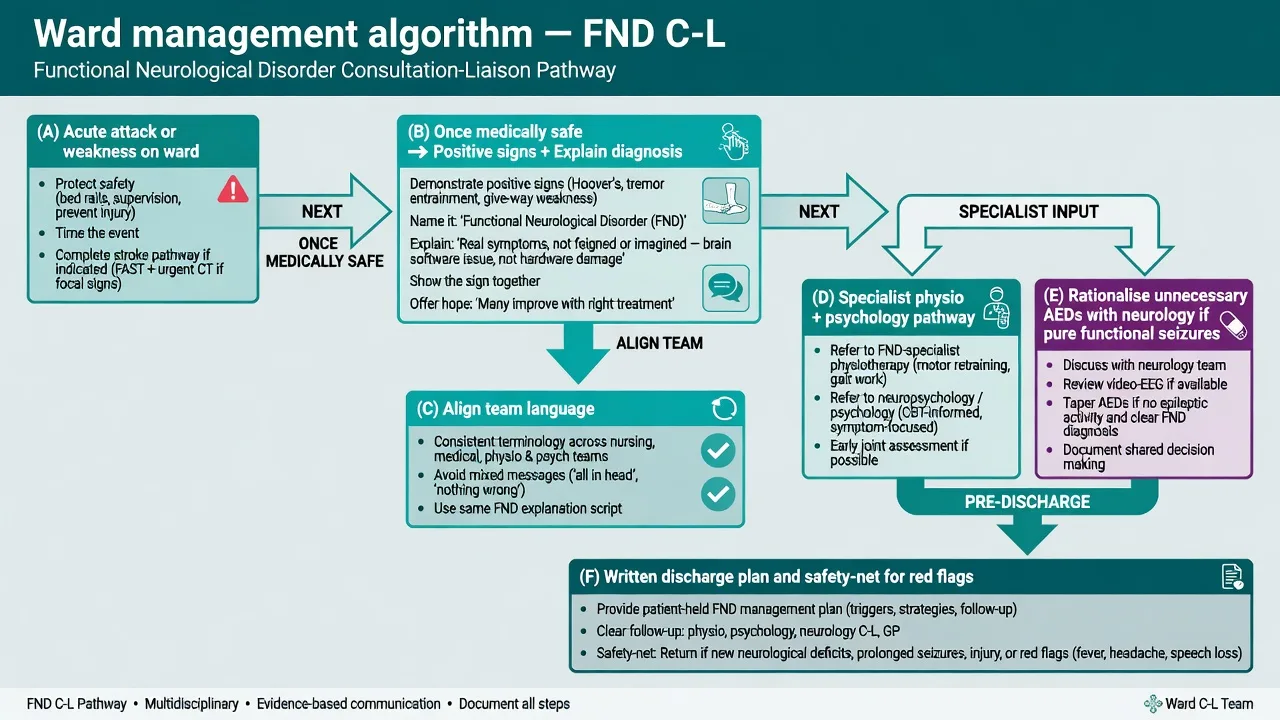
Protect from injury, time the event, reduce crowd and panic, support airway positioning as needed. Once the pattern is known and epilepsy is adequately addressed, avoid automatic high-dose benzodiazepine cascades and unnecessary ICU intubation for typical prolonged functional events, while still escalating if airway risk or diagnostic uncertainty appears.[3][15][16]
Functional weakness presentations
Complete stroke/spinal pathways when indicated. After medical clearance, use positive signs, early explanation, and early mobilisation principles rather than prolonged bed rest that consolidates disability.[5][13][19]
Stop iatrogenesis
Repeated ED attendances without a plan, escalating AED polypharmacy for pure functional seizures, and pejorative chart language are modifiable harms the liaison psychiatrist should name and reverse with the team.[3][4][16]
Definitive C-L management: explanation is treatment

Structured explanation — naming the condition, stating symptoms are real and involuntary, showing how positive signs demonstrate preserved pathways, offering a non-dualist mechanism metaphor, and outlining treatment — is the first and often most powerful intervention.[4][3] Align the medical team before a multi-voice bedside discussion so the patient does not hear three incompatible stories.[4][19]
Multidisciplinary pathway
- Specialist physiotherapy for functional motor disorder: education, reduce symptom-focused attention, retrain automatic movement, graded self-management (Nielsen consensus); Physio4FMD is the major pragmatic phase 3 specialist physiotherapy trial context in England and Scotland.[13][14]
- Psychological therapy: CBT-informed approaches for functional seizures — LaFrance multicenter pilot RCT; CODES pragmatic multicentre RCT of seizure-specific CBT plus standardised medical care versus standardised medical care alone — know primary seizure-frequency nuances and secondary benefits honestly.[15][16]
- Psychopharmacology: treat comorbid depression, anxiety, PTSD, or insomnia with standard agents and monitoring; there is no disease-modifying drug for core FND motor signs.[1][3]
- Team and discharge: shared formulation letter, attack safety plan, outpatient FND or neuropsychiatry follow-up, occupational graded return to function, family psychoeducation with consent.[3][4][19]
Subtypes and medical-setting scenarios
- ED hyperacute mimics — stroke and seizure pathways first; then rule-in and explanation.[19]
- Inpatient functional seizures after medical admission — video-EEG liaison; AED rationalisation with neurology when pure functional seizures are secure.[15][16]
- Post-injury / post-procedure functional motor disorder — common after minor trauma or surgery; early physio and explanation reduce chronicity risk framing.[13][3]
- Dual pathology — FND plus MS, epilepsy, or mild TBI is well recognised; treat both.[1][2]
- Paediatric hospital presentations — family systems, school, avoid blaming the child for “secondary gain.”[3]
Complications and pitfalls
Prognosis and disposition
Without treatment, prognosis is often guarded with persistent symptoms in many series.[17] Long-term follow-up of functional limb weakness shows low rates of later alternative disease explanation after expert diagnosis, yet substantial ongoing disability and excess mortality signals that demand active care rather than dismissal.[18] Better outcomes associate with early diagnosis, acceptance of the explanation, shorter duration, and therapeutic alliance.[17][3]
Disposition prefers outpatient FND pathways; use inpatient rehabilitation for severe disability; avoid discharging at night with only “anxiety” coded in the summary.[3][19]
Special populations
- Older adults — higher dual pathology risk; careful stroke and neurodegeneration exclusion.[19]
- Pregnancy — functional seizures versus eclampsia and other organic differentials; treat comorbidity with pregnancy-safe regimens via obstetric liaison.[3]
- Intellectual disability and autism — adapt communication; involve carers; avoid over-attribution of all neurological change to behaviour.[2]
- Cultural formulation — collaborative explanatory models; avoid pathologising culturally sanctioned trance while still diagnosing FND when positive signs fit.[4]
Evidence and regional practice
Landmark anchors for exams: Espay et al. JAMA Neurol 2018 current concepts; Hallett et al. Lancet Neurol 2022 subtypes and shared mechanisms; Aybek and Perez BMJ 2022 management review; Stone, Burton, and Carson BMJ 2020 on recognising and explaining FND; Bennett et al. practical review for general physicians.[1][2][3][4][19]
Intervention anchors: Nielsen physiotherapy consensus and Physio4FMD phase 3; LaFrance CBT-informed pilot for PNES; CODES CBT for dissociative seizures.[13][14][15][16]
In Australia and New Zealand, FND on medical wards is typically co-owned by neurology and C-L psychiatry with local neuropsychiatry pathways where available. Use non-pejorative documentation, joint explanation, and referral to specialist physio and psychology. Mental health legislation is used only for concurrent psychiatric risk meeting local criteria — FND itself is not a default involuntary treatment indication. Align language with DSM-5-TR / ICD-11 rather than outdated conversion-as-feigning myths.[3][4][19]
UK practice often routes motor FND toward specialist physiotherapy services informed by consensus recommendations and Physio4FMD-era evidence, and dissociative seizures toward neurology–psychology pathways informed by CODES-era care packages. NICE-aligned general principles favour timely diagnosis, clear explanation, and MDT care rather than prolonged diagnostic limbo.[13][14][16]
APA DSM-5-TR criteria language emphasises positive evidence of incompatibility. ABPN-style items often test rule-in signs, communication ethics, dual pathology, and trial names (CODES, Physio4FMD, LaFrance). Avoid equating FND with factitious disorder or malingering on board items.[1][3][15]
Exam pearls
- C-L gold: align the team, then explain once, then write the plan.[4]
- Rule-in not rule-out; stressor not required.[1][5]
- Name trials honestly: LaFrance 2014, CODES 2020, Physio4FMD 2024.[14][15][16]
- Stroke pathway first when indicated — even if the chart already says FND.[19]
- Functional seizures language over pejorative “pseudo” used to mean faking.[4]
- After expert FND diagnosis, later reclassification rates are low, but dual pathology still occurs — both facts can be true.[9][18]
Related topics
Cross-link the general-adult functional neurological disorder leaf for deeper outpatient clinic, positive-sign catalogue, and trial nuance; link epilepsy-and-psychiatry, pain-psychiatry-and-somatic-symptom, delirium, capacity-and-informed-consent, and factitious-disorder-and-malingering for adjacent C-L differentials.[1][3]
References
- [1]Espay AJ, Aybek S, Carson A, et al. Current Concepts in Diagnosis and Treatment of Functional Neurological Disorders JAMA Neurol, 2018.PMID 29868890
- [2]Hallett M, Aybek S, Dworetzky BA, et al. Functional neurological disorder: new subtypes and shared mechanisms Lancet Neurol, 2022.PMID 35430029
- [3]Aybek S, Perez DL Diagnosis and management of functional neurological disorder BMJ, 2022.PMID 35074803
- [4]Stone J, Burton C, Carson A Recognising and explaining functional neurological disorder BMJ, 2020.PMID 33087335
- [5]Daum C, Hubschmid M, Aybek S The value of 'positive' clinical signs for weakness, sensory and gait disorders in conversion disorder: a systematic and narrative review J Neurol Neurosurg Psychiatry, 2014.PMID 23467417
- [6]Daum C, Gheorghita F, Spatola M, et al. Interobserver agreement and validity of bedside 'positive signs' for functional weakness, sensory and gait disorders in conversion disorder: a pilot study J Neurol Neurosurg Psychiatry, 2015.PMID 24994927
- [7]Edwards MJ, Adams RA, Brown H, Pareés I, Friston KJ A Bayesian account of 'hysteria' Brain, 2012.PMID 22641838
- [8]Maurer CW, LaFaver K, Ameli R, et al. Impaired self-agency in functional movement disorders: A resting-state fMRI study Neurology, 2016.PMID 27385746
- [9]Stone J, Carson A, Duncan R, et al. Symptoms 'unexplained by organic disease' in 1144 new neurology out-patients: how often does the diagnosis change at follow-up? Brain, 2009.PMID 19737842
- [10]Carson A, Stone J, Hibberd C, et al. Disability, distress and unemployment in neurology outpatients with symptoms 'unexplained by organic disease' J Neurol Neurosurg Psychiatry, 2011.PMID 21257981
- [11]Carson A, Lehn A Epidemiology Handb Clin Neurol, 2016.PMID 27719864
- [12]Ludwig L, Pasman JA, Nicholson T, et al. Stressful life events and maltreatment in conversion (functional neurological) disorder: systematic review and meta-analysis of case-control studies Lancet Psychiatry, 2018.PMID 29526521
- [13]Nielsen G, Stone J, Matthews A, et al. Physiotherapy for functional motor disorders: a consensus recommendation J Neurol Neurosurg Psychiatry, 2015.PMID 25433033
- [14]Nielsen G, Stone J, Lee TC, et al. Specialist physiotherapy for functional motor disorder in England and Scotland (Physio4FMD): a pragmatic, multicentre, phase 3 randomised controlled trial Lancet Neurol, 2024.PMID 38768621
- [15]LaFrance WC Jr, Baird GL, Barry JJ, et al. Multicenter pilot treatment trial for psychogenic nonepileptic seizures: a randomized clinical trial JAMA Psychiatry, 2014.PMID 24989152
- [16]Goldstein LH, Robinson EJ, Mellers JDC, et al. Cognitive behavioural therapy for adults with dissociative seizures (CODES): a pragmatic, multicentre, randomised controlled trial Lancet Psychiatry, 2020.PMID 32445688
- [17]Gelauff J, Stone J Prognosis of functional neurologic disorders Handb Clin Neurol, 2016.PMID 27719869
- [18]Gelauff JM, Carson A, Ludwig L, Tijssen MAJ, Stone J The prognosis of functional limb weakness: a 14-year case-control study Brain, 2019.PMID 31167232
- [19]Bennett K, Diamond C, Hoeritzauer I, et al. A practical review of functional neurological disorder (FND) for the general physician Clin Med (Lond), 2021.PMID 33479065