Psych · Consultation-liaison — hepatic encephalopathy and advanced transplant psychiatry
Hepatic encephalopathy and advanced transplant psychiatry
Also known as Hepatic encephalopathy psychiatry · Covert hepatic encephalopathy · West Haven criteria · Liver transplant psychiatry · Alcohol-associated liver disease transplant · SIPAT liver · Psychotropics in cirrhosis · Valproate hyperammonaemic encephalopathy
Exam-exhaustive fellowship reference on hepatic encephalopathy for the C-L psychiatrist (West Haven and covert–overt classification, gut–liver–brain mechanisms, precipitants, discrimination from primary psychiatric illness, capacity and driving, lactulose/rifaximin, benzodiazepine risk) and advanced liver transplant psychiatry (psychosocial evaluation, alcohol-associated pathways including early LT after Mathurin, adherence and relapse risk, depression outcomes, CNI/steroid neurotoxicity, psychotropics in cirrhosis). FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
1 MCQ with explanations
Target exams
Red flags
Examiners use these stems to test organic differential, capacity under fluctuating cognition, psychotropic safety in cirrhosis, and ethics of listing. A candidate who only recites generic depression criteria fails when the stem is asterixis, sleep–wake inversion, recurrent HE admissions, early transplant after severe alcoholic hepatitis, or post-LT tacrolimus psychosis.[2][5][8]
Overview and definition
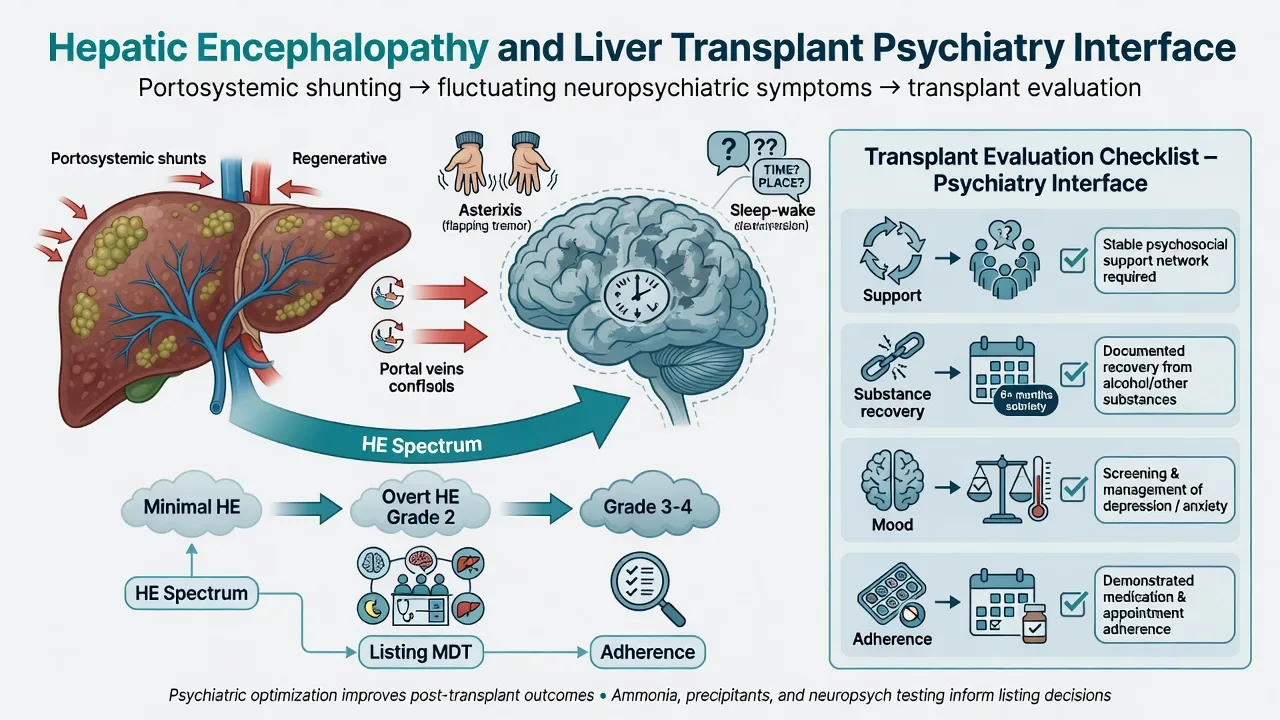
Hepatic encephalopathy (HE) is brain dysfunction caused by liver insufficiency and/or portosystemic shunting after other causes of altered mental status are considered; the Vienna working-party report fixed modern nomenclature and quantification language still used in exams.[1] AASLD/EASL 2014 practice guidance operationalises classification (type, grade, time course, precipitants) and management pillars for chronic liver disease.[2][3]
Advanced transplant psychiatry for liver candidates and recipients is C-L evaluation and longitudinal care across listing, peri-operative, and post-transplant phases — substance recovery structure, mood and capacity, adherence risk, immunosuppressant neuropsychiatry — building on structured psychosocial tools such as SIPAT and multidisciplinary recommendation frameworks (ISHLT/APM/AST-style domain logic is examinable even when written for cardiothoracic/MCS candidates).[13][14]
This leaf complements the broader transplant/ICU hub: depth here is HE neuropsychiatry + liver-specific listing and post-LT risk, not a second full PADIS/CAM-ICU monograph.[2][13]
Classification
| Construct | Exam meaning |
|---|---|
| Type A / B / C | A = acute liver failure; B = bypass without intrinsic disease; C = cirrhosis (most common C-L stem) |
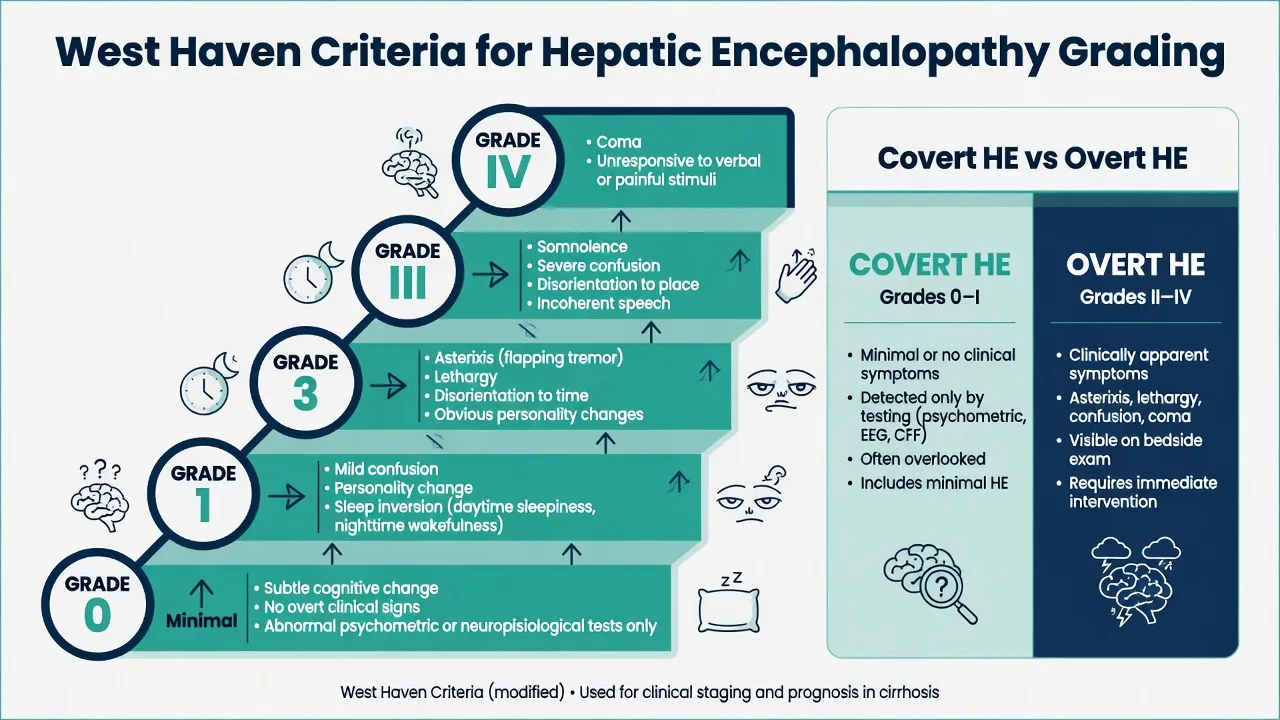
| West Haven 0–IV | Spectrum from normal exam through subtle change, asterixis/disorientation, somnolence, to coma |
| Covert vs overt | Covert = minimal HE + West Haven I; overt = II–IV — different detection tools and driving/risk conversations |
| Episodic / recurrent / persistent | Time course drives secondary prevention intensity and transplant urgency signal |
| Precipitated vs spontaneous | Hunt infection, bleed, constipation, electrolytes, drugs, TIPS |
Coding may use delirium due to another medical condition or other specified mental disorder due to medical condition. Viva credit goes to grade, precipitant, capacity statement, and medical co-management, not ICD pedantry alone.[1][2]
Epidemiology and risk
Alcohol-associated liver disease remains a major LT indication; structured substance assessment and post-LT relapse planning are core psychiatry skills, not optional extras.[9][10] Meta-analytic data show meaningful substance relapse risk after liver and other solid organ transplant that varies with pre-transplant factors — not destiny, not denial.[10]
Pathophysiology
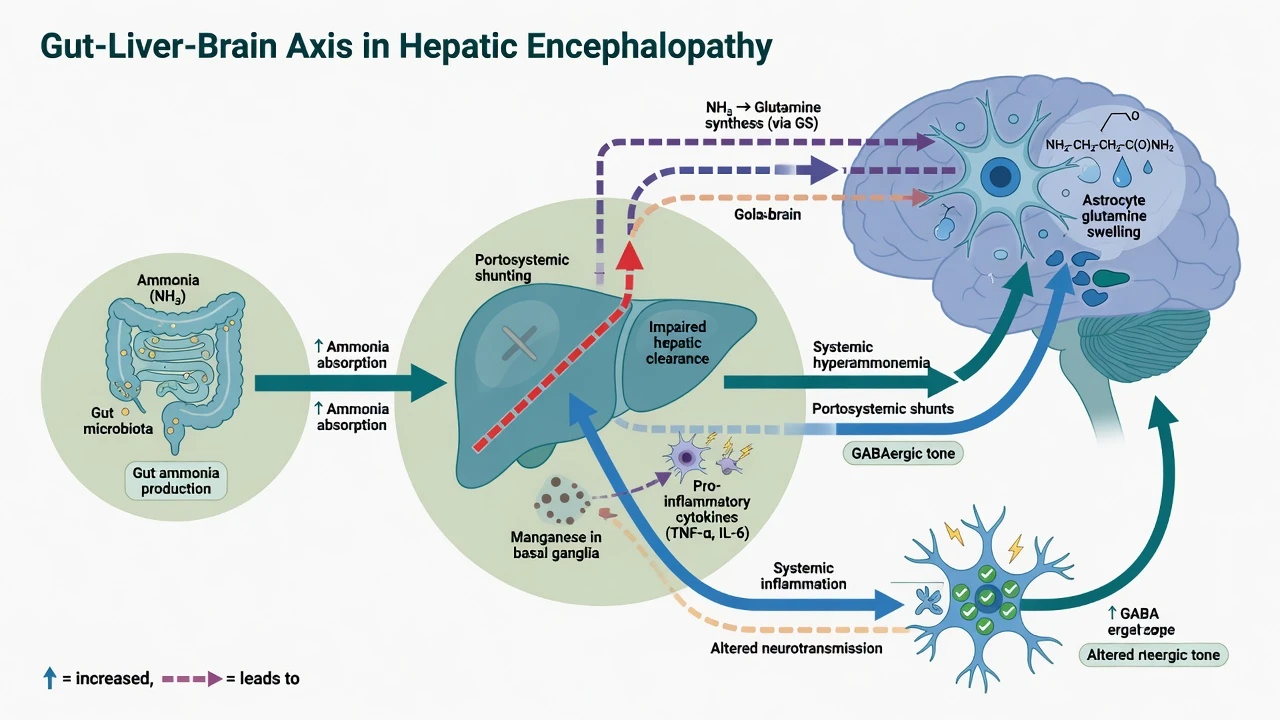
Fellowship-level mechanism map: impaired hepatic clearance of gut-derived nitrogenous products and other neurotoxins; portosystemic shunting; astrocyte glutamine accumulation and swelling; altered neurotransmission (including GABAergic tone); systemic inflammation; and chronic deposition phenomena (e.g. manganese-related basal ganglia T1 hyperintensity on imaging is a hepatology teaching point, not a psychiatry first test).[2][5][7]
Precipitants to recite under stress: infection (including SBP), gastrointestinal bleeding, constipation or excess dietary protein load in selected contexts, dehydration and electrolyte disturbance (especially hypokalaemia, hyponatraemia), diuretic overuse, benzodiazepines and other sedatives, and TIPS.[2][5][16]
Clinical presentation
Covert HE
Subtle attention and executive deficits, sleep–wake inversion, mild irritability or apathy, slowed psychomotor tempo. Casual conversation can look normal until psychometric testing or a careful cognitive screen. Patients may already be unsafe drivers or poor self-managers without meeting classic “confused” stereotypes.[5][6]
Overt HE
Asterixis, temporal disorientation, inappropriate behaviour, lethargy, then stupor and coma. Serial examination matters — HE fluctuates over hours.[1][2]
Psychiatric mislabels
Depression, “personality change,” psychosis, functional cognitive disorder, or primary mania. Discriminators: asterixis, sleep–wake inversion, known cirrhosis/shunt, precipitant, fluctuating inattention, and improvement with HE therapy.[2][5]
Transplant psychiatry stems
Pre-listing alcohol-associated disease with contested abstinence narratives; early LT pathway after severe alcoholic hepatitis (Mathurin paradigm); depression with DNA pattern; thin social support; post-LT nonadherence or relapse concern; CNI/steroid neuropsychiatric change.[8][9][11][12]
Differential — discriminators
- Cirrhosis or shunt context
- Asterixis, sleep inversion, fluctuating attention
- Precipitant often identifiable
- Improves with lactulose/precipitant control
- Ammonia supportive only
- Timeline from last drink; autonomic hyperactivity in withdrawal
- Wernicke: ophthalmoplegia, ataxia, confusion — give thiamine
- May coexist with HE in dual pathology
- Do not assume pure HE in malnourished AUD
- No liver failure driver after work-up
- Longitudinal psychiatric trajectory
- Lacks asterixis/precipitant pattern
- Still exclude HE before new lifelong labels in cirrhosis
- Valproate hyperammonaemic encephalopathy
- Tacrolimus/steroid neuropsych syndromes post-LT
- Benzodiazepine deepening of HE
- Chart review is diagnostic gold
Also hold: subdural haematoma, seizure, sepsis delirium without HE, severe hyponatraemia or hypoglycaemia, and intracranial infection when fever and focal signs dominate — alternative causes remain part of the HE work-up whenever atypical features appear.[2][5]
Assessment
- Liver and HE history: prior HE grades, admissions, lactulose adherence, TIPS, known precipitants, sedative/alcohol use.
- MSE: attention, orientation, speech coherence, asterixis, sleep–wake cycle; document time of assessment.
- Psychosocial (listing): readiness, support, psychopathology, substance engagement, adherence history, health literacy — SIPAT constructs organise risk without replacing clinical judgment.[13][14]
- Risk: suicide in decompensated disease and post-LT depression; agitation safety; caregiver burnout.
- Capacity: decision-specific four abilities after material disclosure; reassess when lucid — HE is the classic fluctuating incapacity exam stem.[18]
Investigations
Coordinate with hepatology/medicine: LFTs, INR, bilirubin, albumin, electrolytes, glucose, FBC, infection work-up (including ascitic fluid when indicated), and imaging/EEG/LP when alternative CNS disease is plausible. Triphasic waves are not pathognomonic. Covert HE may need specialised psychometric testing (PHES-class batteries) where available — do not invent universal cut-offs as local law.[2][5][7] Programme-indicated alcohol biomarkers and CNI levels when toxicity is suspected complete the transplant-facing panel.[9]
Acute management and red flags
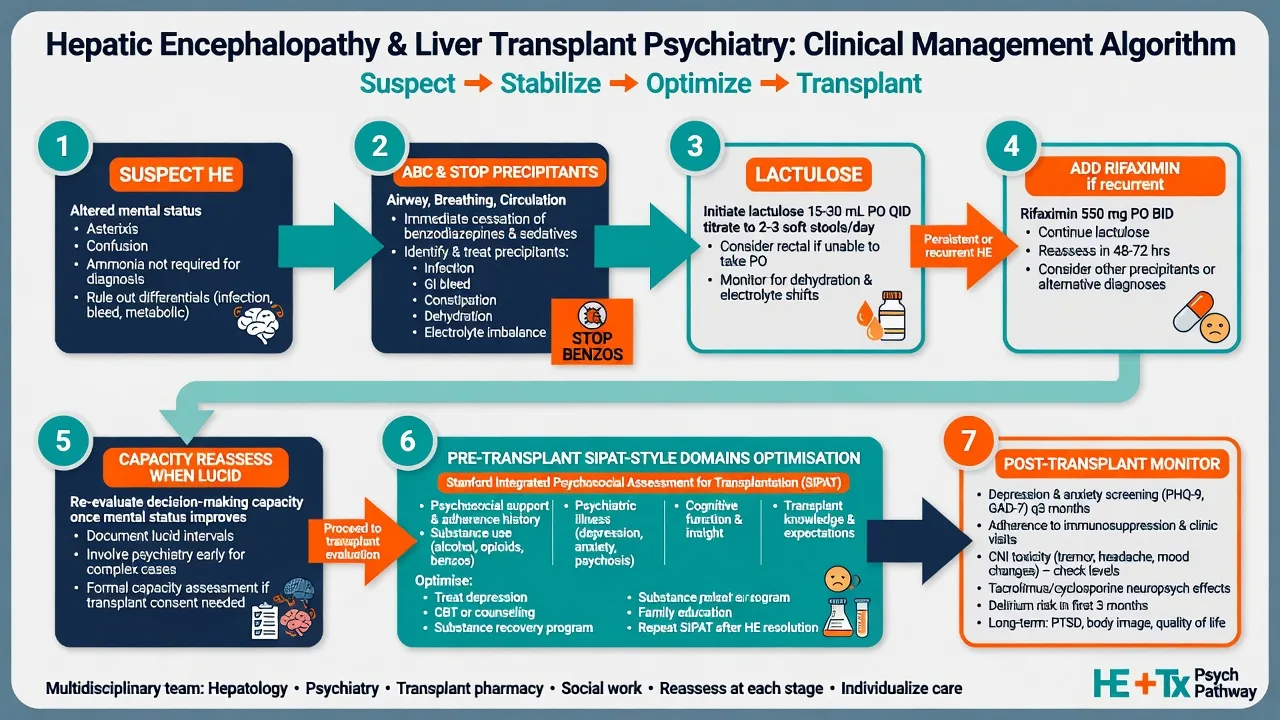
Overt HE emergency pathway: airway and nursing safety; treat precipitants; lactulose as cornerstone non-absorbable disaccharide therapy per AASLD/EASL-era practice (titrate toward soft bowel motions under medical ownership — typical adult oral regimens start in the 20–30 mL range two to four times daily and are adjusted; enemas if oral route fails); add rifaximin in the secondary prevention paradigm established by the Bass randomised trial (550 mg twice daily oral in that trial design for reduction of breakthrough HE in remitted patients on lactulose background).[2][3][4]
Short-term low-dose antipsychotic for severe behavioural danger only after cause hunt and with hepatic caution (e.g. olanzapine 2.5–5 mg oral or haloperidol 0.5–1 mg with ECG/EPS monitoring) — stop early as HE clears; this is a bridge, not definitive HE therapy.[2][15]
Definitive management
Secondary prevention of HE
Education on precipitants; lactulose adherence; rifaximin for recurrent HE after Bass-level evidence framing; nutrition liaison; review of sedating drugs; recognition that recurrent HE is a transplant-evaluation signal.[2][4][7]
Pre-transplant psychosocial optimisation
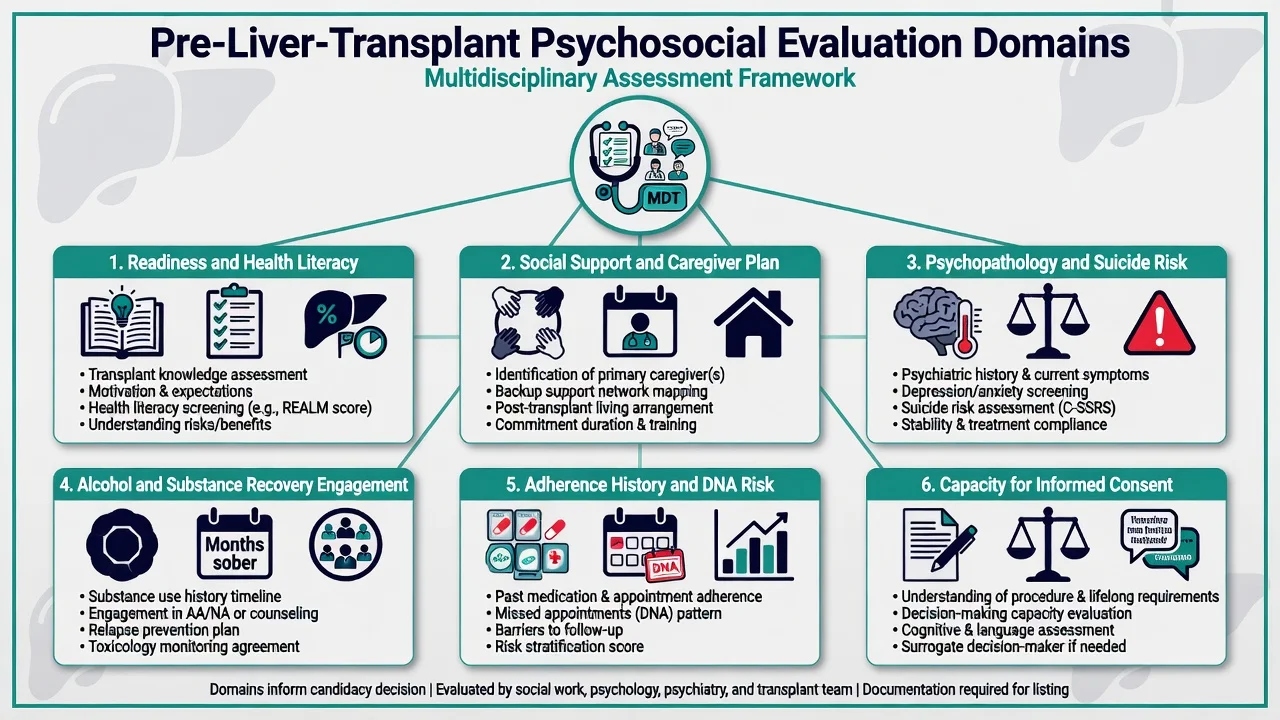
Structure interviews and collateral across readiness and health literacy; social support; current psychopathology and suicide risk; substance use history and treatment engagement; adherence behaviours (DNAs, regimen examples); and decision-specific capacity for lifelong immunosuppression after material disclosure.[13][14][18] Depression and anxiety after solid organ transplant associate with worse medical outcomes in meta-analysis — treat optimisable illness before framing “contraindication.”[12] Nonadherence is common enough across organs that programmes must plan for risk factors rather than express surprise after graft loss.[11]
Alcohol-associated disease and early LT
There is no single universal statutory six-month abstinence rule that every exam answer must invent. Programmes vary; structured recovery, insight, monitoring, and support matter.[9][10] Mathurin and colleagues demonstrated that early liver transplantation can be life-saving in carefully selected patients with severe alcoholic hepatitis not responding to medical therapy — an ethics and systems viva, not a rubber stamp.[8]
Psychotropics in cirrhosis and hyperammonaemia
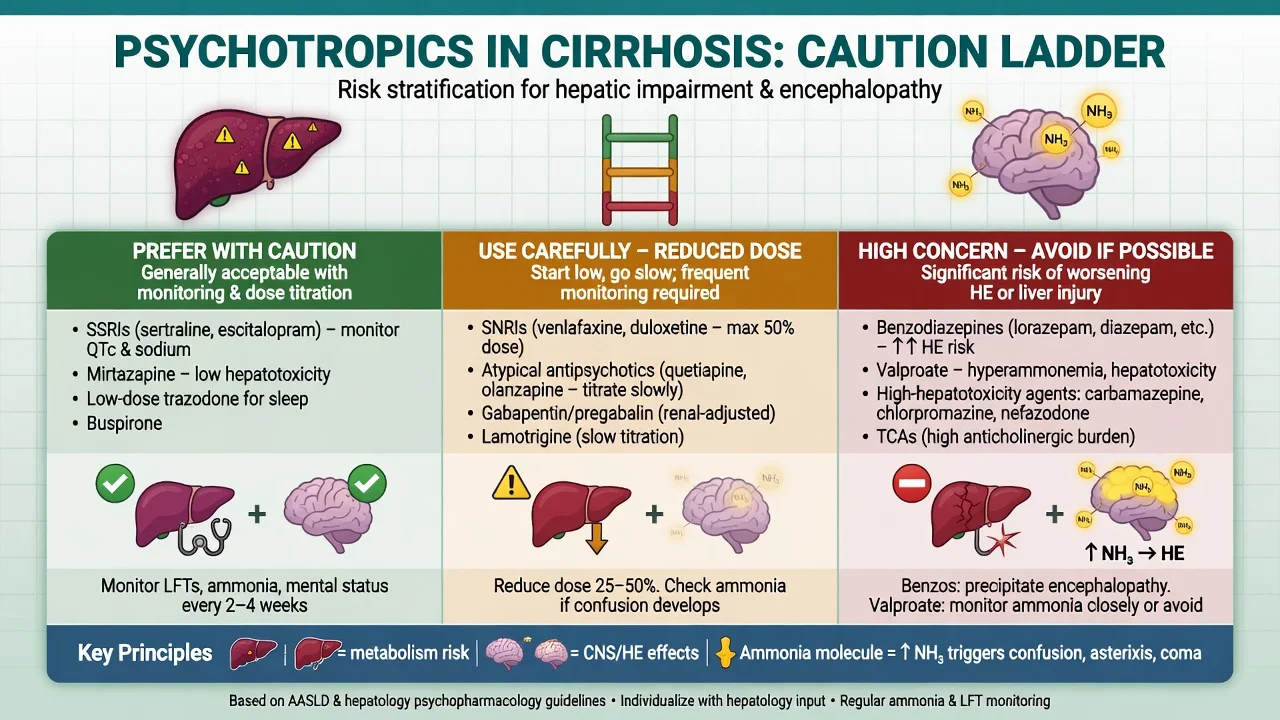
Prescribing in cirrhosis requires reduced first-pass, altered CYP/UGT activity, hypoalbuminaemia (free fraction), and PD sensitivity to sedation. Critical reviews of psychotropics and liver disease plus practical cirrhosis prescribing guides emphasise agent selection, dose reduction, and hepatotoxicity awareness.[15] Benzodiazepines raise HE risk signals in cirrhosis with ascites.[16] Valproate-induced hyperammonaemic encephalopathy is a recognised, potentially reversible toxicity — stop valproate, support airway and ammonia-directed care with medical teams, and do not rechallenge casually.[17] Prefer SSRI/SNRI choices individualised for hepatic impairment, start low and titrate slowly, avoid high hepatotoxicity-risk agents when alternatives exist, and use TDM thinking where relevant (e.g. some TCAs, mood stabilisers) under specialist advice.[15]
Post-transplant neuropsychiatry
Depression treatment and adherence support are outcome interventions, not soft add-ons.[11][12] New psychosis or severe behavioural change: review tacrolimus/ciclosporin levels and steroid dose with the transplant team before a primary schizophrenia label; coordinate level-guided dose strategy and short-term psychotropics chosen for interaction risk.[14]
Subtypes and scenarios
- Type A HE (acute liver failure): transplant emergency; family substitute decisions; psychiatry supports communication and risk, does not delay medical pathway.
- Recurrent type C HE: caregiver burnout, capacity oscillation, listing urgency.
- Covert HE and driving: counsel risk; fitness-to-drive rules are jurisdiction-specific — document clinical concern and local process without inventing statutes.[6]
- Early LT after severe AH: Mathurin selection ethics and relapse planning.[8][9]
- VPA hyperammonaemia in bipolar disorder ± cirrhosis.[17]
- Post-LT CNI toxicity mislabeled as schizophrenia.
Complications and pitfalls
Missing HE; ammonia-only diagnosis; benzo-first sedation; VPA continued through hyperammonaemic coma; psychiatry as permanent gatekeeper; equating any alcohol history with lifelong exclusion; ignoring Dew-level depression and nonadherence outcome data; inventing MHA section numbers or universal abstinence durations.[2][10][12][16][17]
Prognosis and disposition
Each overt HE episode worsens prognosis and should trigger precipitant control, secondary prevention, and transplant-evaluation thinking when appropriate.[2][7] Psychiatric morbidity and nonadherence predict poorer transplant outcomes — treat as modifiable risk.[11][12] Step down follow-up intensity by HE recurrence, substance risk, depression severity, and adherence scaffolding.
Special populations
Older candidates (cognitive frailty, capacity); adolescent transition and adherence; pregnancy after LT (psychotropic–immunosuppression coordination principles); cultural formulation in alcohol and support planning; intellectual disability with supported decision-making rather than automatic exclusion; acute liver failure families under extreme time pressure.[14][18]
Evidence and guidelines
ANZ / FRANZCP C-L practice: Apply AASLD/EASL HE pillars with local hepatology protocols; structured psychosocial evaluation using SIPAT-like domains; RANZCP-aligned ethical MDT listing without invented national abstinence statutes.[2][13][14]
UK / MRCPsych: NICE-era liver and alcohol pathways interface with local transplant centre protocols; CASC communication on capacity and alcohol recovery.[2][18]
US / ABPN: AASLD HE guidance and centre policy frameworks; SIPAT is widely used in US programmes for structured psychosocial risk.[2][13]
India / MD-DNB / NEET-SS: High burden of alcohol-associated disease in many centres; viva emphasis on West Haven staging, lactulose/rifaximin principles, and psychotropic hepatic cautions.[1][4][15]
Landmark anchors: Ferenci working party; AASLD/EASL 2014 HE guidance; Bajaj covert/overt and driving literature; ISHEN unresolved questions; Bass rifaximin RCT; Mathurin early LT; DiMartini alcohol/substance in LT; Dew nonadherence, depression/anxiety, and substance-relapse meta-analyses; SIPAT and ISHLT-style psychosocial recommendations; Telles-Correia psychotropics–liver; Grønbæk benzos–HE; Segura-Bruna VPA hyperammonaemia; Appelbaum capacity.[1][2][4][5][8][10][13][16][17][18]
Exam pearls
- HE is clinical; ammonia is supportive only.
- Covert HE is the quiet exam trap.
- Lactulose cornerstone; rifaximin for recurrent HE (Bass).
- Stop benzos early in cirrhotic agitation.
- SIPAT organises risk; MDT lists.
- No universal six-month abstinence statute — Mathurin early LT is the counter-example viva.
- Depression and nonadherence after transplant are medical outcome risks (Dew).
- VPA + hyperammonaemia + encephalopathy = stop VPA.
- CNI/steroid toxicity before new schizophrenia post-LT.
- Capacity is decision-specific and often returns as HE clears.[4][8][12][13][17][18]
References
- [1]Ferenci P, Lockwood A, Mullen K, et al. Hepatic encephalopathy--definition, nomenclature, diagnosis, and quantification: final report of the working party at the 11th World Congresses of Gastroenterology, Vienna, 1998 Hepatology, 2002.PMID 11870389
- [2]Vilstrup H, Amodio P, Bajaj J, et al. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver Hepatology, 2014.PMID 25042402
- [3]American Association for the Study of Liver Diseases; European Association for the Study of the Liver Hepatic encephalopathy in chronic liver disease: 2014 practice guideline by the European Association for the Study of the Liver and the American Association for the Study of Liver Diseases J Hepatol, 2014.PMID 25015420
- [4]Bass NM, Mullen KD, Sanyal A, et al. Rifaximin treatment in hepatic encephalopathy N Engl J Med, 2010.PMID 20335583
- [5]Patidar KR, Bajaj JS Covert and Overt Hepatic Encephalopathy: Diagnosis and Management Clin Gastroenterol Hepatol, 2015.PMID 26164219
- [6]Shaw J, Bajaj JS Covert Hepatic Encephalopathy: Can My Patient Drive? J Clin Gastroenterol, 2017.PMID 28027071
- [7]Bajaj JS, Lauridsen M, Tapper EB, et al. Important Unresolved Questions in the Management of Hepatic Encephalopathy: An ISHEN Consensus Am J Gastroenterol, 2020.PMID 32618647
- [8]Mathurin P, Moreno C, Samuel D, et al. Early liver transplantation for severe alcoholic hepatitis N Engl J Med, 2011.PMID 22070476
- [9]DiMartini A, Crone C, Dew MA Alcohol and substance use in liver transplant patients Clin Liver Dis, 2011.PMID 22032526
- [10]Dew MA, DiMartini AF, Steel J, et al. Meta-analysis of risk for relapse to substance use after transplantation of the liver or other solid organs Liver Transpl, 2008.PMID 18236389
- [11]Dew MA, DiMartini AF, De Vito Dabbs A, et al. Rates and risk factors for nonadherence to the medical regimen after adult solid organ transplantation Transplantation, 2007.PMID 17460556
- [12]Dew MA, Rosenberger EM, Myaskovsky L, et al. Depression and Anxiety as Risk Factors for Morbidity and Mortality After Organ Transplantation: A Systematic Review and Meta-Analysis Transplantation, 2015.PMID 26492128
- [13]Maldonado JR, Dubois HC, David EE, et al. The Stanford Integrated Psychosocial Assessment for Transplantation (SIPAT): a new tool for the psychosocial evaluation of pre-transplant candidates Psychosomatics, 2012.PMID 22424160
- [14]Dew MA, DiMartini AF, Dobbels F, et al. The 2018 ISHLT/APM/AST/ICCAC/STSW Recommendations for the Psychosocial Evaluation of Adult Cardiothoracic Transplant Candidates and Candidates for Long-term Mechanical Circulatory Support Psychosomatics, 2018.PMID 30197247
- [15]Telles-Correia D, Barbosa A, Cortez-Pinto H, et al. Psychotropic drugs and liver disease: A critical review of pharmacokinetics and liver toxicity World J Gastrointest Pharmacol Ther, 2017.PMID 28217372
- [16]Grønbæk L, Watson H, Vilstrup H, et al. Benzodiazepines and risk for hepatic encephalopathy in patients with cirrhosis and ascites United European Gastroenterol J, 2018.PMID 29774154
- [17]Segura-Bruna N, Rodriguez-Campello A, Puente V, et al. Valproate-induced hyperammonemic encephalopathy Acta Neurol Scand, 2006.PMID 16774619
- [18]Appelbaum PS Clinical practice. Assessment of patients' competence to consent to treatment N Engl J Med, 2007.PMID 17978292