Psych · Consultation-liaison psychiatry
HIV psychiatry
Also known as HIV-associated neurocognitive disorders · HAND · AIDS psychiatry · Neuropsychiatry of HIV · Depression in HIV · ART neuropsychiatric effects
Exam-exhaustive fellowship topic on HIV psychiatry for consultation-liaison practice — Frascati HAND spectrum (ANI/MND/HAD), depression and adherence (CBT-AD, measurement-based care), ART neuropsychiatry (efavirenz, INSTIs), psychotropic–antiretroviral interactions with boosters, stigma and suicide risk, and decision-specific capacity. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
HIV psychiatry is the consultation-liaison interface examiners use to test organic cognition, mood–adherence coupling, drug interactions, stigma-informed risk, and capacity. Do not deliver a generic depression lecture. Name Frascati categories, ART culprits, interaction traps, and integrated care models.[1][4][18]
Overview and definition
HIV psychiatry covers psychiatric and neurocognitive morbidity in people living with HIV (PLHIV) from diagnosis through ART optimisation, chronic multimorbidity, ageing, and advanced disease. Psychiatry contributes syndrome diagnosis, risk management, psychopharmacology that respects antiretroviral (ART) kinetics, adherence support, capacity work, and liaison with HIV medicine, pharmacy, psychology, and peer services.[4][5][7]
Classification — HAND and the psychiatric map

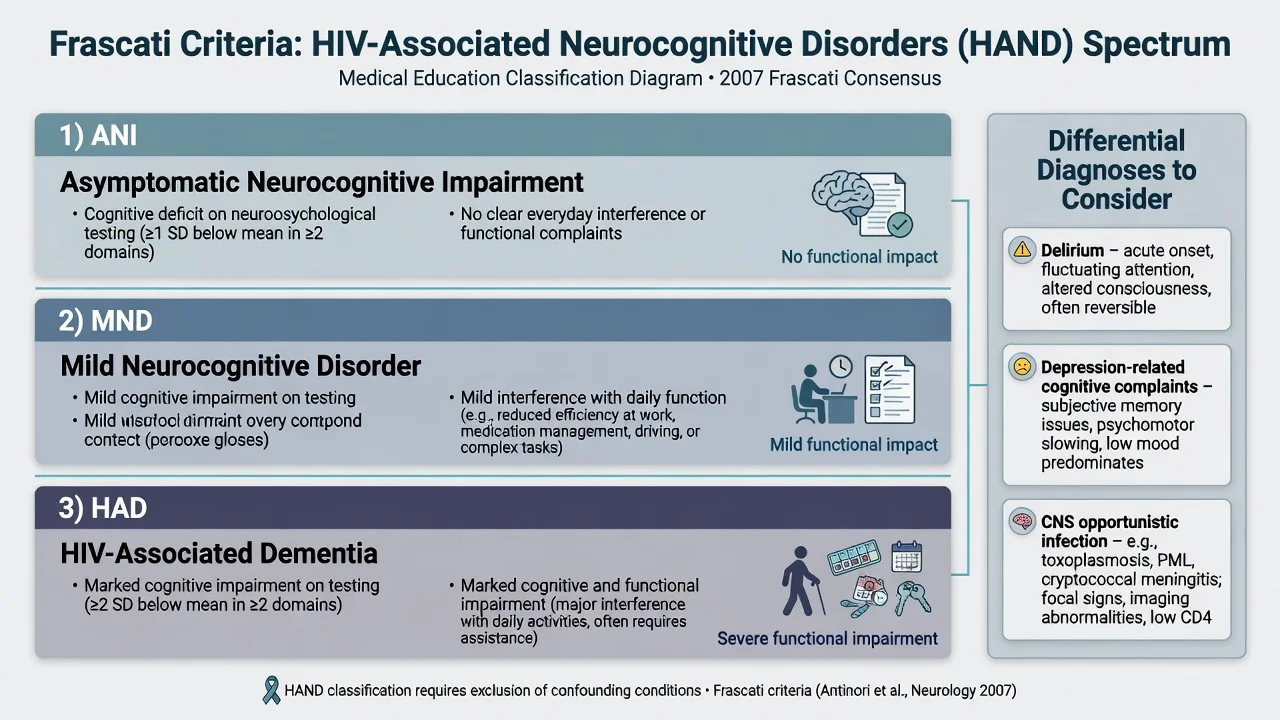
Frascati criteria (Antinori 2007) define HIV-associated neurocognitive disorders (HAND) for research and clinical framing:[1]
| Category | Cognitive performance | Everyday function |
|---|---|---|
| ANI — asymptomatic neurocognitive impairment | Acquired impairment in at least two cognitive domains (typically ≥1 SD below demographically adjusted norms in research batteries) | No clear interference with everyday functioning |
| MND — mild neurocognitive disorder | Impairment in at least two domains (often ≥1 SD) | Mild interference with daily function (work, homemaking, social, adherence complexity) |
| HAD — HIV-associated dementia | Marked impairment (often ≥2 SD in multiple domains) | Marked functional disability |
CHARTER and related work show HAND persists in the potent ART era, usually with milder phenotypes than the pre-cART dementia epidemic; predictors include nadir CD4 and comorbidities.[2][3][4]
Broader psychiatric map in PLHIV: major depression, adjustment disorders, anxiety/PTSD (high trauma burden in many key populations), substance use disorders, primary psychosis/bipolar comorbidity, and ART-induced mood, sleep, anxiety, and psychotic syndromes.[7][15][17]
Epidemiology and risk
Ciesla and Roberts found HIV infection associated with roughly double the risk of depressive disorders versus comparison groups in meta-analysis.[6] Bing and colleagues documented high rates of psychiatric disorders and drug use among HIV-infected adults in the US HCSUS sample.[7] Depression consistently associates with ART nonadherence in pooled data — a CL pearl that converts mood treatment into infectious-disease outcomes language.[8][9]
Suicide risk among PLHIV clusters with depression, substance use, stigma, social isolation, and illness stressors; treat passive and active ideation as high-yield exam content, not afterthoughts.[22][25]
Pathophysiology and mechanisms
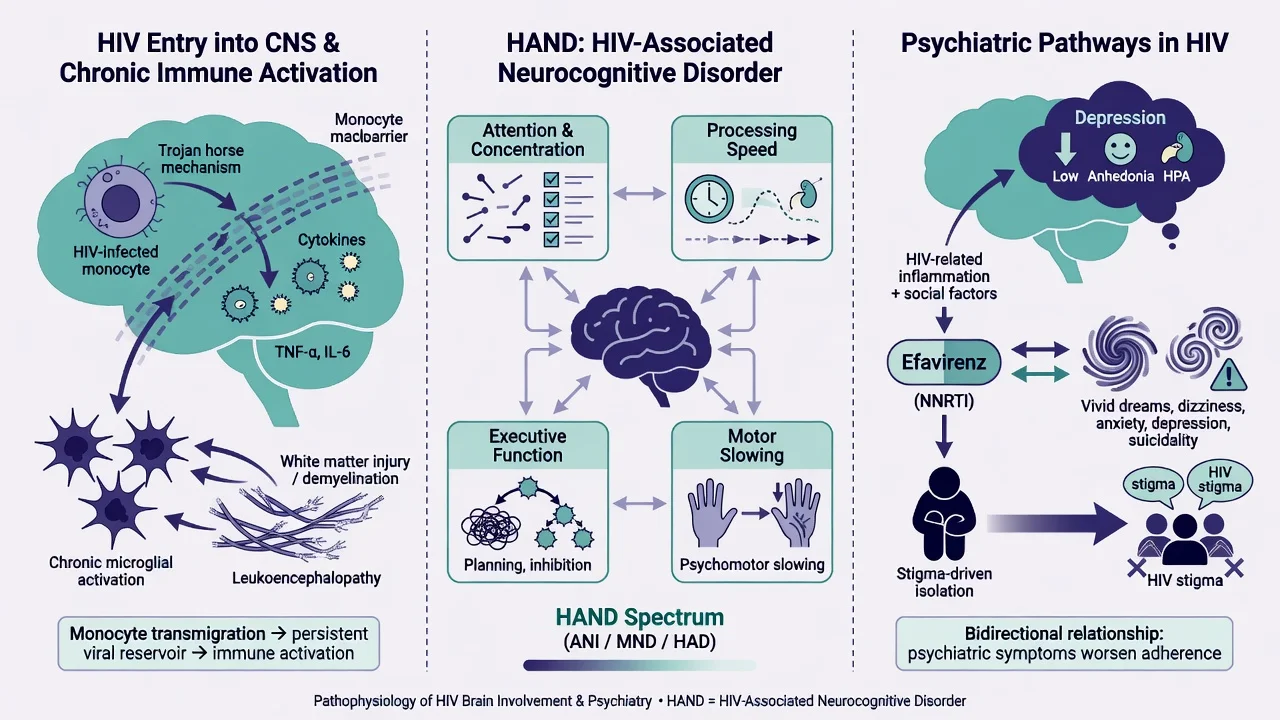
HAND reflects CNS HIV entry, monocyte/macrophage trafficking, chronic immune activation, and network disruption (attention, processing speed, executive function, motor speed) even when plasma virus is suppressed — so-called legacy and compartmental dynamics remain clinically relevant.[4][5]
Efavirenz is the classic ART with psychiatric adverse effects: vivid dreams, insomnia, dizziness, anxiety, depression, and less often psychosis or mania; systematic review summarises the spectrum, and trial pharmacogenetic analyses link suicidality reports with ancestry/metabolism signals — still individualise rather than racialise care.[15][16]
Integrase inhibitors (especially dolutegravir in observational discontinuation series) carry neuropsychiatric signals — insomnia, anxiety, depression — that can drive self-cessation if not elicited.[17]
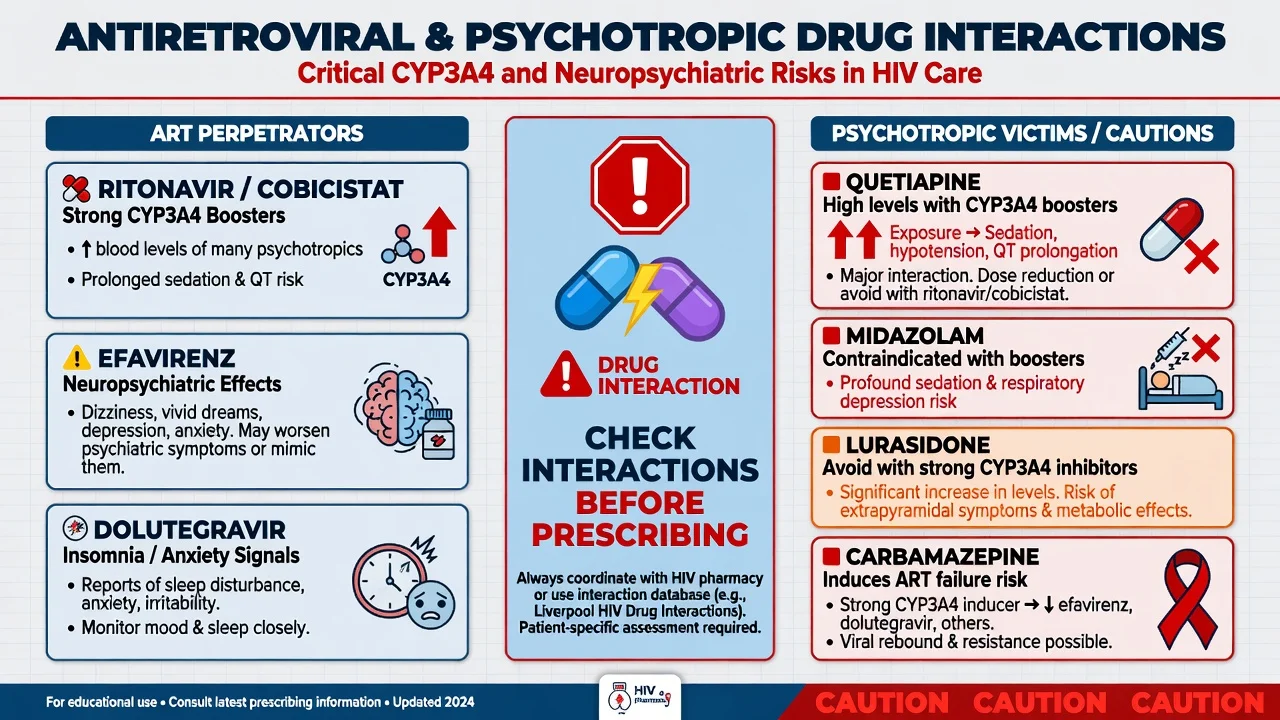
Boosted protease inhibitor or cobicistat regimens strongly inhibit CYP3A4 (and affect transporters), raising levels of many psychotropics; inducers such as carbamazepine can threaten ART efficacy.[18][19]
Stigma is pathogenic: meta-analytic work links HIV-related stigma with poorer mental health, lower social support, and worse care engagement — not merely a sociocultural aside.[21]
Clinical presentation
HAND. Insidious cognitive slowing, forgetfulness for complex tasks, word-finding or multitasking failure, and motor slowing; behavioural apathy or irritability appears more with advanced HAD. Functional questions about bills, work errors, and pill organisation separate ANI from MND/HAD.[1][4]
Depression. Pervasive low mood/anhedonia, cognitive symptoms, guilt, hopelessness, and suicidality lasting weeks. Fatigue and sleep change overlap HIV and depression — weight affective, anhedonic, and suicidality anchors plus collateral functional collapse.[6][20]
ART neuropsychiatry. Nightmares and insomnia within days of efavirenz; acute psychosis/mania stems after initiation are exam favourites. INSTI-related insomnia/anxiety may be subtler but clinically decisive for adherence.[15][17]
Stigma presentation. Concealment, missed clinic, shame language, delayed disclosure, and avoidance of mental health services — ask directly and non-judgementally.[21]
Differential diagnosis — discriminators
- Acquired multi-domain deficit
- Functional interference grades severity
- Often subcortical-frontal pattern
- Exclude OI/delirium first
- May coexist with depression
- Pervasive anhedonia/hopelessness
- ≥2 weeks
- Suicide risk elevated
- Drives nonadherence
- CBT-AD and antidepressants
- Temporal link to efavirenz/INSTI
- Dreams, insomnia, psychosis
- Improves after switch when safe
- Check substances and steroids
- Do not stop ART unsupervised
Always consider delirium, CNS opportunistic infection (toxoplasmosis, cryptococcus, PML, CMV, TB), syphilis, substance intoxication/withdrawal, primary progressive dementias in older adults, and metabolic insults before locking a single label.[4][5]
Assessment
- HIV context: date of diagnosis, nadir and current CD4, viral load, regimen and recent switches, CNS history, adherence pattern.
- Psychiatric history: prior mood/psychosis, self-harm, trauma, substance use.
- MSE: mood, affect, psychosis, attention/processing screens; formal neuropsychology when classifying HAND.
- Risk: suicide (Smith risk-factor review; life stressors in depressed PLHIV), self-neglect, violence, vulnerability.[22][25]
- Stigma and supports: disclosure status, housing, food security, partner violence, peer support.
- Capacity: decision-specific ART consent/refusal, complex financial decisions, research participation — use Appelbaum pillars (understand, appreciate, reason, communicate).[23][24]
- Tools: PHQ-9 for depression tracking; bedside cognitive screens (IHDS/HDS/MoCA) as screens only; full NP testing for Frascati classification.[1][12]
Investigations
Directed work-up for new cognitive, mood, or psychotic change: CD4 and HIV RNA, FBC, electrolytes, glucose, LFTs, B12/folate/TSH as indicated, syphilis and HCV when relevant, substance screen, and MRI (plus LP when OI or alternative CNS disease is plausible). ECG and full interaction check before QT-risky psychotropics on interacting ART.[4][18][20]
Acute management and red flags
For dangerous agitation or psychosis: safety, observation, reverse medical causes, short-term low-dose antipsychotic if required, and urgent discussion of efavirenz (or other culprit) switch with HIV specialists — never abandon ART without a replacement plan.[15][18]
Active suicidality needs environment safety, means restriction, urgent psychiatry, treatment of depression, and jurisdiction-specific legal frameworks when criteria for involuntary care are met.[22][25]
Definitive management
Optimise ART and brain health
Sustained viral suppression and immune recovery are foundational for neurocognitive outcomes; severe HAD is less common on modern ART, though milder HAND persists.[2][3][4] Manage vascular risk, sleep, substance use, and HCV as cognitive co-drivers.[4][5]
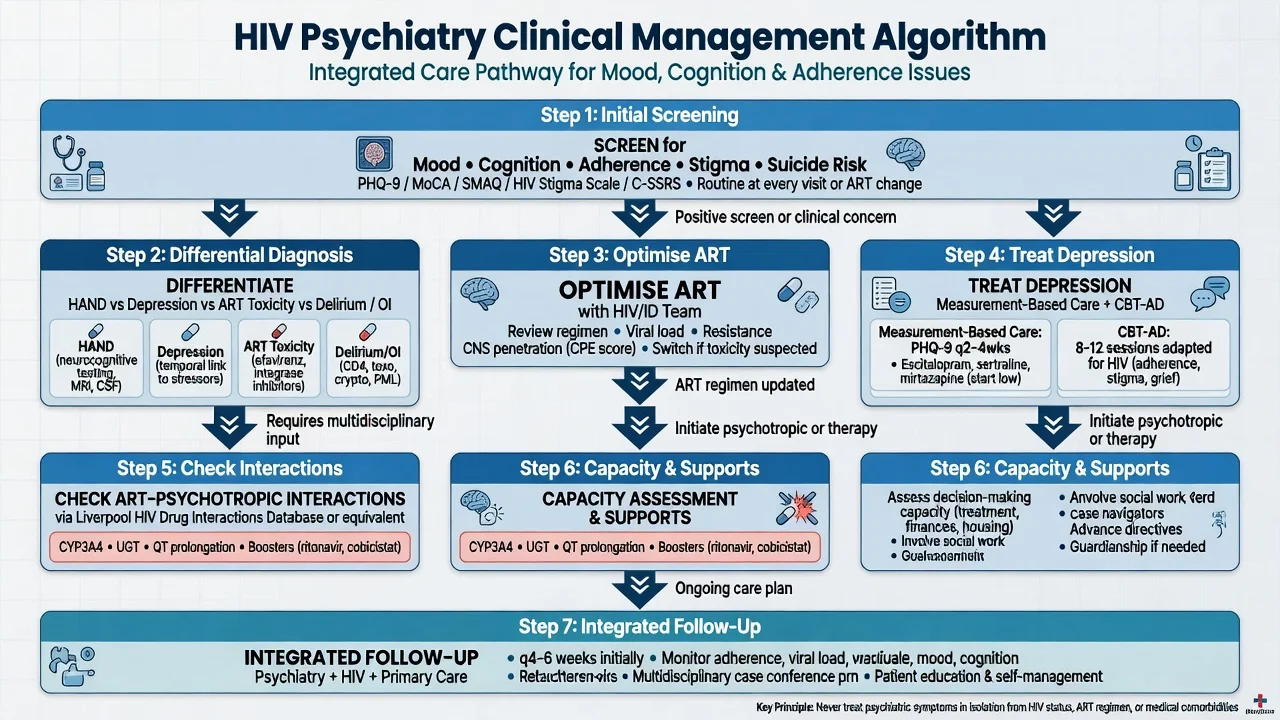
Depression care and adherence
Measurement-based depression care in HIV clinics (SLAM DUNC programme architecture) operationalises systematic screening, algorithm-guided antidepressants, and monitoring.[11][12] In the randomised antidepressant trial embedded in that line of work, depression outcomes improved with structured treatment while HIV biologic outcomes were more nuanced — treat depression for suffering and adherence risk, not as a guaranteed viral-load panacea.[11]
CBT for adherence and depression (CBT-AD) improves depression and adherence behaviours in HIV-infected adults, including adaptations for injection drug users.[13][14]
Historical RCT evidence supports fluoxetine efficacy for depression in HIV/AIDS; modern practice individualises SSRI/SNRI/mirtazapine choice with interaction and side-effect profiles.[10][20]
Practical fellowship dosing anchors (adult, medically stable; start lower if frail/hepatic impairment; verify interactions):[10][18][20]
| Agent | Typical start | Notes in HIV care |
|---|---|---|
| Sertraline | 25–50 mg oral daily; titrate toward 50–150 mg | Often used; check GI overlap and hyponatraemia |
| Escitalopram | 5–10 mg oral daily; usual 10–20 mg | Simpler kinetics; watch QTc at higher doses |
| Mirtazapine | 7.5–15 mg oral at night | Sleep/appetite may help; sedation |
| Fluoxetine | 10–20 mg oral daily | RCT-supported historically; long half-life and CYP interactions |
Monitor response every 1–2 weeks early, adherence, sexual side effects, hyponatraemia, and suicidal ideation after initiation, especially with ongoing life stressors.[20][25]
ART–psychotropic interactions
High-yield rules for viva:[18][19]
- Ritonavir/cobicistat: potent CYP3A4 inhibition — quetiapine, many benzodiazepines (e.g. midazolam, triazolam), lurasidone, and other 3A4 substrates can reach toxic levels; avoid or use drastically reduced doses with pharmacy support.
- Efavirenz: mixed inducer/inhibitor profile plus direct CNS effects — prefer regimen switch for severe psychiatric toxicity rather than stacking sedatives.
- Enzyme-inducing anticonvulsants/mood stabilisers (e.g. carbamazepine): risk of lowering ART levels and virologic failure — avoid where possible.
- Always use an up-to-date interaction checker and HIV pharmacist for complex polypharmacy.[18][19]
Example caution for acute behavioural control on a boosted regimen: prefer agents and doses vetted for interactions; if an antipsychotic is essential for danger, use the lowest effective short-term dose with daily review rather than high standing quetiapine.[18]
HAND-specific care
No single psychotropic reverses HAND. Suppress HIV, treat depression and sleep disorders, reduce alcohol/other drugs, address vascular risk, simplify regimens for cognitive load, and involve occupational therapy/cognitive strategies. Reassess classification after medical optimisation.[4][5]
Stigma-informed care
Name stigma as a clinical target: confidentiality, non-judgemental enquiry, peer navigation, and structural supports improve engagement; meta-analyses link stigma to adverse mental health and care outcomes.[21]
Capacity, stigma, and rights
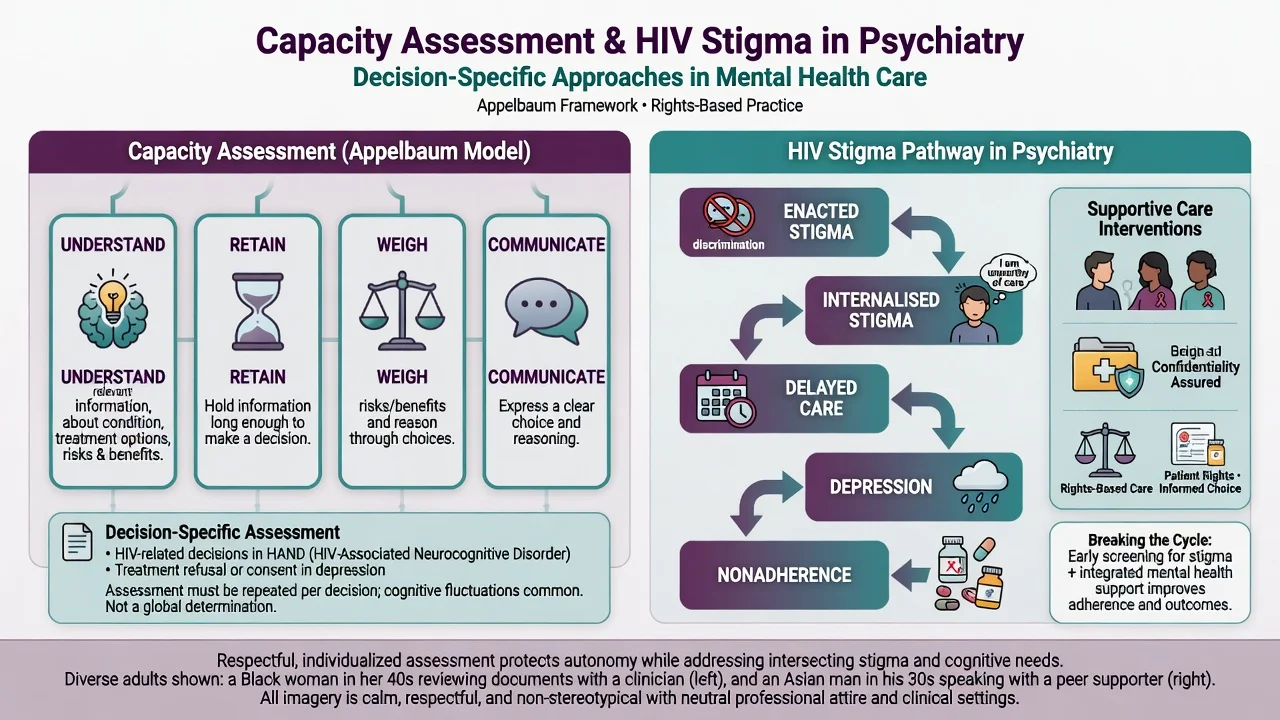
Capacity is decision-specific and time-specific: understand relevant information, appreciate the situation and consequences, reason about options, and communicate a choice.[23] Mild HAND or an HIV diagnosis alone does not equal incapacity. Severe depression with nihilistic distortion, delirium, advanced HAD, or acute ART-related psychosis may impair appreciation and reasoning — document findings, simplify information, use teach-back, treat reversible factors, reassess in a better window, and apply substitute decision-making under local law when needed.[23][24]
Research-consent studies illustrate that capacity can be impaired in serious mental illness and must be tested rather than assumed from diagnosis labels — the clinical lesson transfers to treatment consent in complex HIV care.[24]
Special populations
Ageing PLHIV: HAND plus vascular and Alzheimer pathology; polypharmacy interaction risk.[3][4] PWID: dual-diagnosis integrated care; CBT-AD adaptations exist.[14] Perinatal and adolescent services: depression, disclosure, adherence, developmental transitions. Culturally diverse and Indigenous communities: structural stigma and culturally safe communication.[21]
Evidence and regional notes
ANZ / FRANZCP. CL psychiatry with HIV services; capacity under state/territory legislation; cite Frascati, CHARTER persistence of HAND, efavirenz toxicity, and booster interactions in exams.[1][2][15][18]
UK / MRCPsych. BHIVA-aligned ART frameworks; CASC stations often test new diagnosis counselling, depression, and stigma-sensitive communication.[6][21]
US / ABPN. DHHS ART guidelines influence regimen choice (efavirenz less first-line in many settings); CBT-AD and measurement-based depression care are high yield.[11][13]
MD/DNB / NEET-SS. Expect viva on ANI/MND/HAD, efavirenz psychosis stems, and depression–adherence coupling.[1][8][15]
Landmark names: Antinori/Frascati, Heaton/CHARTER, Clifford, Ciesla, Bing, Gonzalez/Uthman, Rabkin, Pence, Safren CBT-AD, Kenedi/Mollan, Hoffmann INSTI, Goodlet/Thompson interactions, Rueda stigma, Smith suicide, Appelbaum capacity.[1][2][8][13][15][18][21][23]
Prognosis and disposition
Severe dementia has declined with ART, but milder HAND remains clinically important.[2][3] Depression often responds to structured pharmacotherapy and CBT-AD; HIV viral outcomes after depression treatment are less uniformly improved than mood scores — still treat vigorously.[11][13] ART neuropsychiatric effects frequently improve after informed regimen change.[15][17]
Disposition should name HIV clinic follow-up, mental health/CL review, adherence support, crisis contacts, pharmacy interaction review, and stigma-aware social supports.[12][21]
Exam pearls
HIV-CL (bedside scaffold)
Fellowship one-liners: HAND persists on ART; efavirenz dreams/psychosis — switch with HIV team; boosters multiply quetiapine; CBT-AD treats pills and mood together; capacity is decision-specific.[2][13][15][18][23]
References
- [1]Antinori A, Arendt G, Becker JT, et al. Updated research nosology for HIV-associated neurocognitive disorders Neurology, 2007.PMID 17914061
- [2]Heaton RK, Clifford DB, Franklin DR Jr, et al. HIV-associated neurocognitive disorders persist in the era of potent antiretroviral therapy: CHARTER Study Neurology, 2010.PMID 21135382
- [3]Heaton RK, Franklin DR, Ellis RJ, et al. HIV-associated neurocognitive disorders before and during the era of combination antiretroviral therapy: differences in rates, nature, and predictors J Neurovirol, 2011.PMID 21174240
- [4]Clifford DB, Ances BM HIV-associated neurocognitive disorder Lancet Infect Dis, 2013.PMID 24156898
- [5]Letendre S Central nervous system complications in HIV disease: HIV-associated neurocognitive disorder Top Antivir Med, 2011.PMID 22156215
- [6]Ciesla JA, Roberts JE Meta-analysis of the relationship between HIV infection and risk for depressive disorders Am J Psychiatry, 2001.PMID 11329393
- [7]Bing EG, Burnam MA, Longshore D, et al. Psychiatric disorders and drug use among human immunodeficiency virus-infected adults in the United States Arch Gen Psychiatry, 2001.PMID 11483137
- [8]Gonzalez JS, Batchelder AW, Psaros C, et al. Depression and HIV/AIDS treatment nonadherence: a review and meta-analysis J Acquir Immune Defic Syndr, 2011.PMID 21857529
- [9]Uthman OA, Magidson JF, Safren SA, et al. Depression and adherence to antiretroviral therapy in low-, middle- and high-income countries: a systematic review and meta-analysis Curr HIV/AIDS Rep, 2014.PMID 25038748
- [10]Rabkin JG, Wagner GJ, Rabkin R Fluoxetine treatment for depression in patients with HIV and AIDS: a randomized, placebo-controlled trial Am J Psychiatry, 1999.PMID 9892304
- [11]Pence BW, Gaynes BN, Adams JL, et al. The effect of antidepressant treatment on HIV and depression outcomes: results from a randomized trial AIDS, 2015.PMID 26134881
- [12]Pence BW, Gaynes BN, Williams Q, et al. Assessing the effect of Measurement-Based Care depression treatment on HIV medication adherence and health outcomes: rationale and design of the SLAM DUNC Study Contemp Clin Trials, 2012.PMID 22542960
- [13]Safren SA, O'Cleirigh C, Tan JY, et al. A randomized controlled trial of cognitive behavioral therapy for adherence and depression (CBT-AD) in HIV-infected individuals Health Psychol, 2009.PMID 19210012
- [14]Safren SA, O'Cleirigh CM, Bullis JR, et al. Cognitive behavioral therapy for adherence and depression (CBT-AD) in HIV-infected injection drug users: a randomized controlled trial J Consult Clin Psychol, 2012.PMID 22545737
- [15]Kenedi CA, Goforth HW A systematic review of the psychiatric side-effects of efavirenz AIDS Behav, 2011.PMID 21484283
- [16]Mollan KR, Tierney C, Hellwege JN, et al. Race/Ethnicity and the Pharmacogenetics of Reported Suicidality With Efavirenz Among Clinical Trials Participants J Infect Dis, 2017.PMID 28931220
- [17]Hoffmann C, Llibre JM Neuropsychiatric Adverse Events with Dolutegravir and Other Integrase Strand Transfer Inhibitors AIDS Rev, 2019.PMID 30899113
- [18]Goodlet KJ, Zmarlicka MT, Peckham AM Drug-drug interactions and clinical considerations with co-administration of antiretrovirals and psychotropic drugs CNS Spectr, 2019.PMID 30295215
- [19]Thompson A, Silverman B, Dzeng L, et al. Psychotropic medications and HIV Clin Infect Dis, 2006.PMID 16586391
- [20]Watkins CC, Pieper AA, Treisman GJ Safety considerations in drug treatment of depression in HIV-positive patients: an updated review Drug Saf, 2011.PMID 21751824
- [21]Rueda S, Mitra S, Chen S, et al. Examining the associations between HIV-related stigma and health outcomes in people living with HIV/AIDS: a series of meta-analyses BMJ Open, 2016.PMID 27412106
- [22]Smith A, Rages V, Wootton SH, et al. A Systematic Review of Risk Factors for Suicide Among Persons Living with HIV (1996-2020) AIDS Behav, 2022.PMID 35107660
- [23]Appelbaum PS Clinical practice. Assessment of patients' competence to consent to treatment N Engl J Med, 2007.PMID 17978292
- [24]Moser DJ, Schultz SK, Arndt S, et al. Capacity to provide informed consent for participation in schizophrenia and HIV research Am J Psychiatry, 2002.PMID 12091200
- [25]O'Donnell JK, Gaynes BN, Cole SR, et al. Ongoing life stressors and suicidal ideation among HIV-infected adults with depression J Affect Disord, 2016.PMID 26544615