Psych · Consultation-liaison psychiatry
Huntington disease psychiatry
Also known as Huntington's disease psychiatry · HD neuropsychiatry · Huntington disease depression · Huntington disease psychosis · Huntington irritability · Huntington suicide risk · Predictive testing Huntington psychiatry · VMAT2 Huntington psychiatry
Exam-exhaustive fellowship topic on the psychiatry of Huntington disease: premanifest and manifest neuropsychiatric syndromes, suicide risk, irritability and apathy, psychosis, expert-consensus psychopharmacology, VMAT2–mood interface, predictive testing ethics, and multidisciplinary CL–neurology care. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Psychiatrists fail this topic when they wait for chorea before recognising HD-related depression, when they miss suicide after predictive testing, when they label apathy as "lazy depression," or when they prescribe tetrabenazine without a depression plan. Examiners reward genetic literacy, stage-aware phenomenology, and VMAT2–mood interface knowledge.[3][8][9][12]
Overview and definition
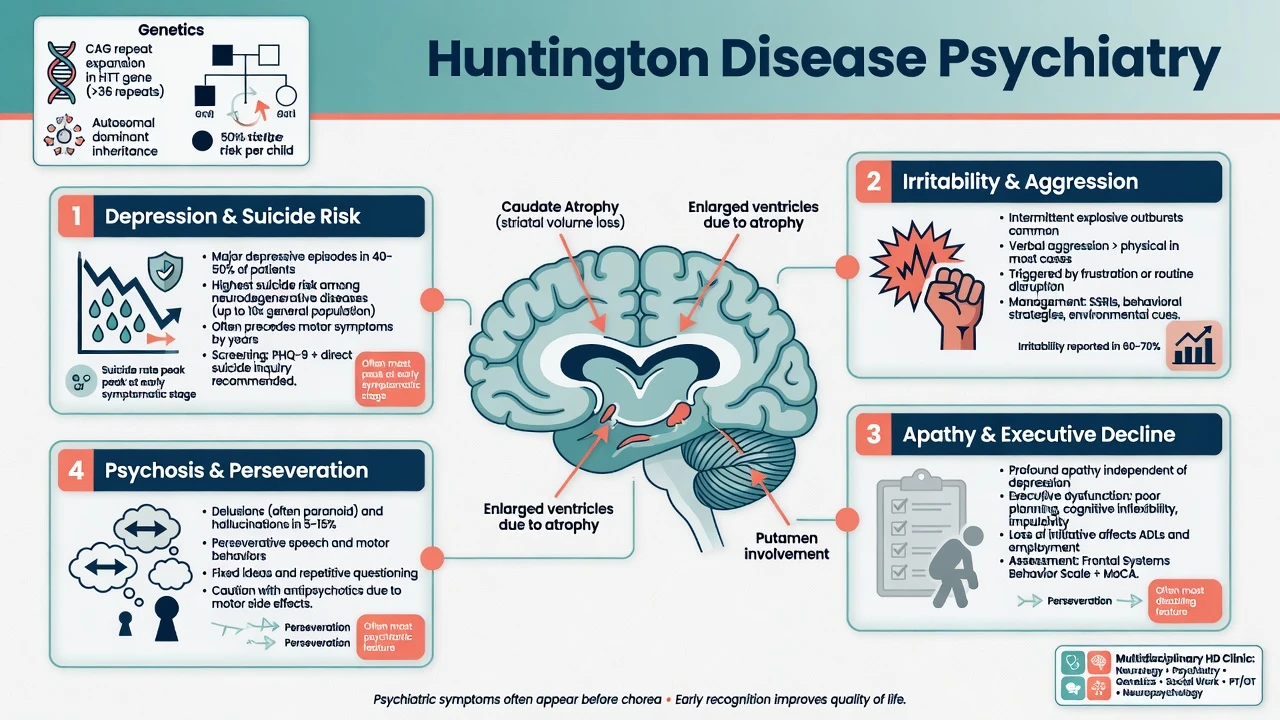
Huntington disease is an autosomal-dominant neurodegenerative disorder caused by a CAG trinucleotide expansion in the HTT gene on chromosome 4, producing mutant huntingtin and progressive striatal and cortical network failure. Motor signs (chorea, later dystonia/rigidity), cognitive decline, and a dense neuropsychiatric phenotype define the clinical syndrome; mean survival after motor onset is typically on the order of 15–20 years, with substantial regional and individual variation.[14][15]
In DSM-5-TR language, psychiatric presentations map to mental disorder due to another medical condition, major neurocognitive disorder due to HD, and related substance/medication-induced differentials. ICD-11 frames HD within diseases of the nervous system with associated behavioural syndromes. The CL task is mechanism-aware management of mood, risk, behaviour, and capacity while preserving function and family systems care.[3][4][14]
Epidemiology and burden
Neuropsychiatric symptoms are the rule, not the exception. In the large European REGISTRY cohort, depression, irritability, and apathy were highly prevalent across disease stages, confirming that behavioural and affective morbidity is a primary driver of disability and care need.[1] Reviews synthesise a heavy burden of mood, behavioural, and psychotic syndromes that often dominate caregiver distress more than chorea alone.[3][4]
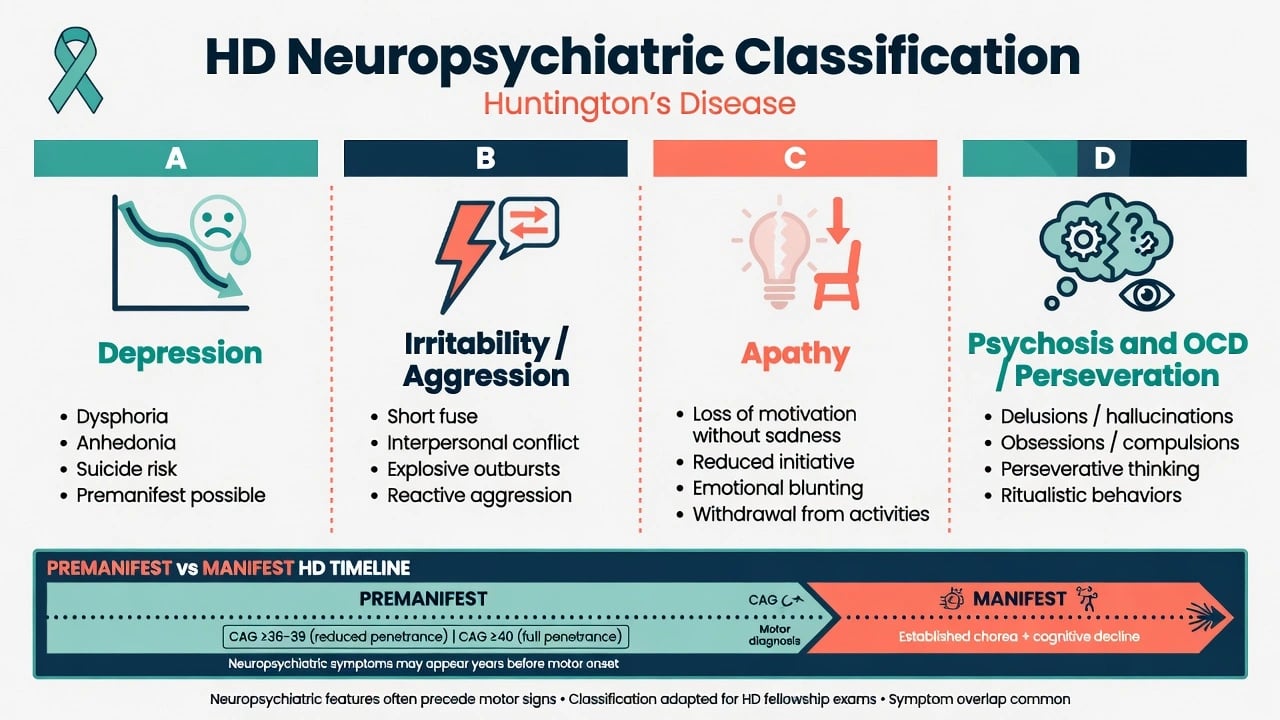
Importantly, psychiatric symptoms frequently appear in the premanifest/prodromal phase, before diagnostic motor onset. PREDICT-HD and related longitudinal work characterise depression and other psychiatric symptoms in gene-expansion carriers years before frank motor diagnosis.[8][9]
Suicide and suicidal ideation are substantially elevated. European data document high rates of suicidal ideation; comorbidity (depression, irritability, substance use, hopelessness) amplifies risk; and prospective global data quantify incidence of attempts and completed suicide in HD populations.[5][6][7]
Classification of key syndromes
Depression
Major depressive episodes include dysphoria, anhedonia, guilt/hopelessness, sleep and appetite change, and suicide risk. Depression occurs in premanifest carriers and across manifest stages; it is not adequately explained as pure demoralisation about genetics or disability.[3][8][9]
Irritability and aggression
Irritability — reduced threshold for anger, short fuse, verbal or physical aggression — is among the most clinically disruptive HD behaviours and a classic exam stem (partner injury, ward conflict, failed residential placement). Structured behavioural tools such as the Problem Behaviours Assessment (PBA) lineage formalise this phenomenology for research and clinics.[2][11]
Apathy
Apathy is loss of motivation and goal-directed behaviour without the same affective pain as depression. It increases with disease progression, devastates function and caregiver load, and is frequently mis-treated with escalating antidepressants alone.[1][4][10]
Psychosis, anxiety, OCD/perseveration
Psychosis is less common than depression/irritability but includes paranoia, delusions, and occasional hallucinations, often mid-stage. Anxiety is frequent. Obsessive-compulsive and perseverative behaviours (repetitive, rigid routines) are recognised HD behavioural phenotypes and differ from primary OCD in flexibility and insight patterns.[3][4][10]
Premanifest versus manifest versus juvenile HD
- Premanifest gene-positive: psychiatric risk + predictive-testing aftermath; subtle executive change.
- Manifest motor HD: full neuropsychiatric spectrum with progressive cognition.
- Juvenile HD (Westphal): akinetic-rigid, behavioural/school decline, different motor face.[14][15]
Pathophysiology (viva depth)
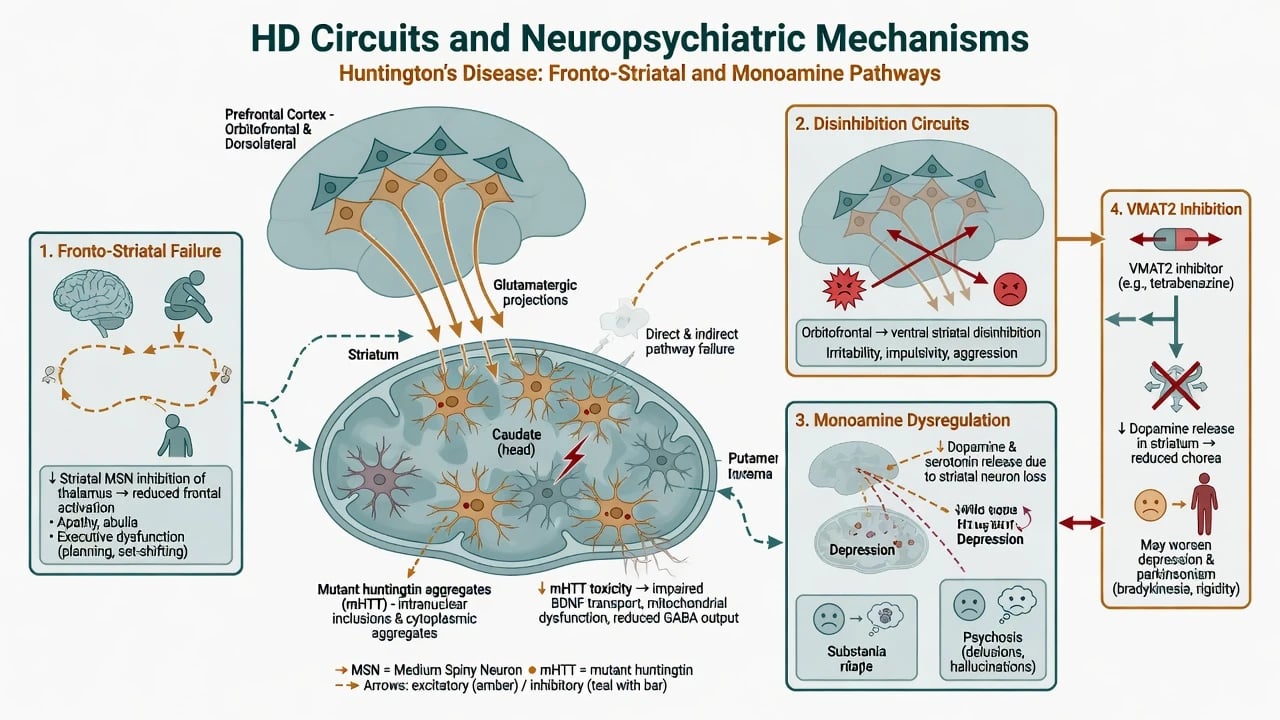
Mutant huntingtin preferentially damages striatal medium-spiny neurons (caudate/putamen) with progressive cortical and network involvement, disrupting fronto-striatal loops that govern motivation, impulse control, affect regulation, and executive function.[14][15] Apathy and dysexecutive decline map to medial and dorsolateral fronto-striatal failure; irritability and disinhibition map to ventral/orbitofrontal circuit disruption; monoaminergic imbalance contributes to depression and psychosis phenotypes.[3][4]
VMAT2 inhibitors reduce packaging of dopamine (and other monoamines) into synaptic vesicles — mechanistically useful for chorea, but they can worsen depression, sedation, and parkinsonism, creating a direct psychiatry–neurology interface every time chorea treatment is escalated.[12][13][16]
Clinical assessment for CL
Structure history around the genetic stage, full neuropsychiatric map, suicide risk, medications (including VMAT2 agents), collateral, and capacity — using tools such as the Problem Behaviours Assessment lineage where available.[2][5][10][16]
- Genetics and disclosure — confirmed expansion? Who knows? Recent predictive testing?
- Stage — premanifest vs motor-manifest; functional independence; swallowing/falls/weight.
- Neuropsychiatric map — depression, irritability, apathy, anxiety, psychosis, perseveration (use PBA-s where available).
- Suicide — ideation, plan, means, past attempts, hopelessness, access to weapons/medication stockpiles.
- Medications — VMAT2 agents, antipsychotics, antidepressants, anticholinergics, benzodiazepines.
- Collateral — partner/carer always; financial risk, aggression, neglect of self-care.
- Capacity — finances, care placement, research, genetic communication to relatives.
- Delirium screen when tempo is acute.[2][5][10][16]
MSE language should capture chorea/motor overlay without missing mood affect, irritability threshold, flat apathy, paranoid content, and executive failures on bedside testing.[2][3][4]
Differential diagnosis
- Primary mood/psychotic/personality disorders coincidental with a family "movement history."
- Other chorea — drug-induced (tardive), Wilson disease, Sydenham, autoimmune/paraneoplastic, thyrotoxicosis — when genetics unconfirmed.
- Delirium and medication toxicity.
- Apathy vs depression vs antipsychotic/VMAT2 sedation.
- Substance use amplifying aggression or mood instability.
- Frontotemporal behavioural phenotypes if pedigree and genetics do not fit.[3][14][15]
Investigations
- Diagnostic genetic testing only within pre- and post-test counselling pathways; psychiatry often supports adjustment and risk after result disclosure.[14][15]
- Never casually test asymptomatic minors for adult-onset HD outside specialist ethical frameworks.
- Imaging may show caudate atrophy in manifest disease (educational correlation, not a stand-alone psychiatric test).
- Baseline metabolic panel, ECG before psychotropics; broader delirium work-up for acute change.
- Medication reconciliation with neurology for VMAT2 and dopamine-blocking load.[10][16]
Acute management
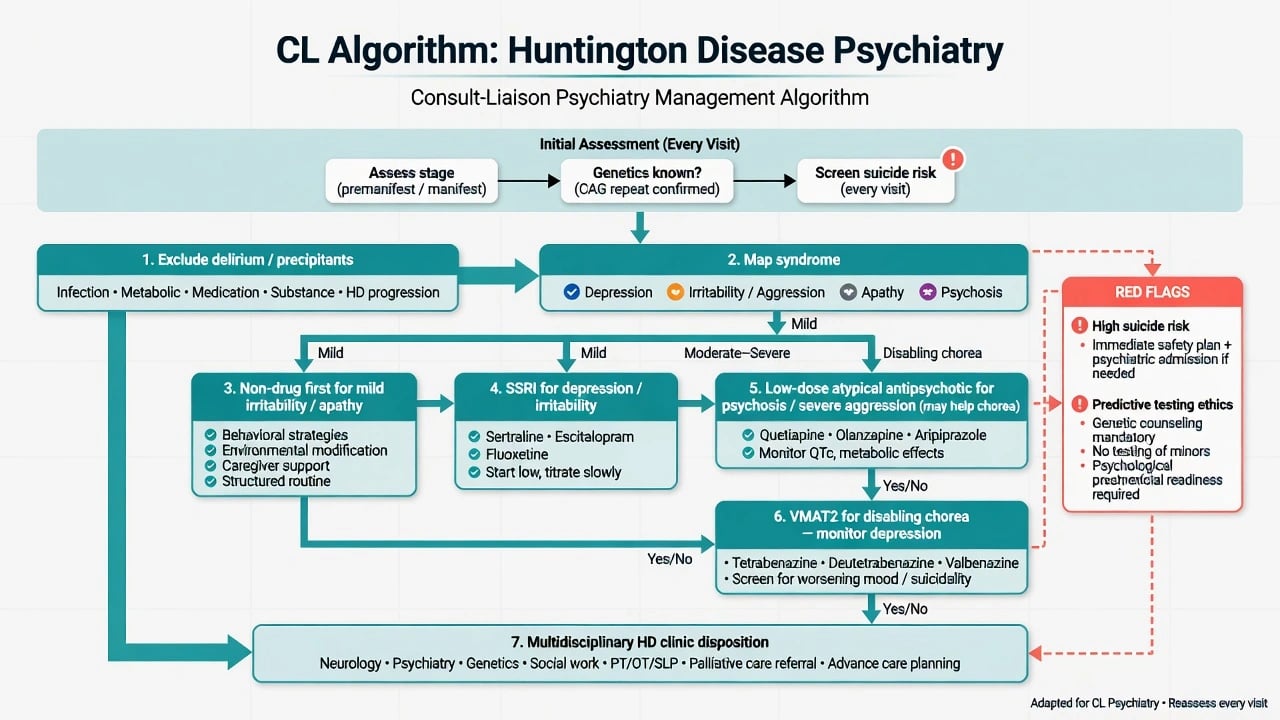
- Safety first — suicide and aggression risk stratification; means restriction; crisis plan; hospital threshold when intent/plan/high lethality or carer safety fails.[5][6][7]
- Exclude delirium/precipitants — infection (including aspiration), dehydration, constipation, pain, medication toxicity.
- Map the dominant syndrome — depression vs irritability vs apathy vs psychosis (they require different first moves).[10][11]
- De-escalation for agitation; short-term environmental measures; avoid reflex high-dose typical antipsychotics without a plan.[10][16]
Definitive management by syndrome
Expert-based consensus guidance (Anderson and colleagues) and irritability algorithms (Groves and colleagues) structure pharmacological choices when non-drug measures fail; evidence quality is often survey/consensus plus clinical experience rather than large head-to-head NPS RCTs — say this honestly in viva.[10][11][16]
Depression
Treat actively. Pragmatic first-line: SSRI (examples used in practice: sertraline 25–50 mg oral daily start, titrate toward 50–100+ mg as tolerated; or citalopram/escitalopram start low — e.g. citalopram 10 mg oral daily, mind QTc and age limits). Monitor activation, hyponatraemia, sexual side effects, and suicidality on initiation, especially in premanifest and early disease.[8][10][16] Offer psychological support, sleep hygiene, and social interventions; involve genetics counselling teams when disclosure distress dominates.
Irritability / aggression
Non-drug first: caregiver education, structure, reduce overstimulation, treat pain/sleep. Pharmacologically, many expert algorithms start with an SSRI; if severe aggression, psychosis, or danger persists, add or switch to a low-dose atypical antipsychotic.[10][11]
Apathy
Limited robust drug evidence. Emphasise environmental activation, structured routines, occupational therapy, and caregiver coaching. Do not escalate multiple antidepressants for pure apathy without dysphoria/suicide features.[1][10]
Psychosis
Use the lowest effective dose of an atypical antipsychotic with monitoring for sedation, falls, metabolic effects, and rigidity. Agents such as olanzapine, risperidone, or quetiapine are used in practice; start low (examples: olanzapine 2.5–5 mg oral at night, or quetiapine 25 mg oral at night, titrate cautiously). Antipsychotic dopamine blockade may also reduce chorea — a dual-benefit pearl — but oversedation and falls remain traps.[10][16]
Chorea agents and the psychiatry interface (high yield)
VMAT2 antichorea agents help motor chorea but require active psychiatric monitoring for depression and parkinsonism.[12][13][16]
| Agent | Landmark evidence | Psychiatry pearl |
|---|---|---|
| Tetrabenazine | TETRA-HD RCT antichorea efficacy | Can worsen depression and parkinsonism; start low, monitor mood/suicide |
| Deutetrabenazine | FIRST-HD RCT | Similar VMAT2 class cautions; often better dosing convenience vs tetrabenazine |
| Valbenazine | Newer VMAT2 option for HD chorea (region-variable access) | Still monitor mood and motor side effects |
Tetrabenazine (TETRA-HD): effective for chorea; classic exam dosing culture is individualised low start (often 12.5 mg oral once or twice daily, titrate slowly) with mandatory depression/parkinsonism surveillance — not a "set and forget" chorea tablet.[12] Deutetrabenazine improved chorea in FIRST-HD with class-related cautions.[13] Always re-check whether new depression began after VMAT2 initiation or dose increase. VMAT2 class mood monitoring applies across agents used for HD chorea.[12][13][16]
Suicide risk — non-negotiable
Assess every clinical contact. Risk is elevated in premanifest carriers and early–mid disease, not only advanced despair. Comorbid depression, irritability, anxiety, substance use, recent genetic disclosure, unemployment, and social isolation raise concern.[5][6][7][8] Document ideation, plan, intent, means, protective factors, and a concrete safety plan. Involve carers when appropriate and lawful; do not invent Mental Health Act section numbers — apply local capacity/risk law principles.
Special populations and genetics ethics
Predictive testing of asymptomatic adults requires protocolised counselling (often multiple sessions), mental health readiness, and follow-up after result. Positive results can unmask or intensify depression and suicidality — plan psychiatry access before testing day.[8][9][14]
Juvenile HD: school failure, rigidity, behavioural change — different motor picture, high family trauma load.[14][15] Pregnancy/reproductive genetics: coordinate specialist genetics; psychiatry supports adjustment and risk. Cultural formulations: hereditary "family curse" narratives need respect without abandoning biomedical risk assessment.
Prognosis and disposition
HD is progressive; psychiatric load shifts (irritability/depression often early–mid; apathy and cognitive failure later), but suicide risk demands ongoing surveillance across stages.[1][6][9] Disposition should default to multidisciplinary HD clinic pathways: neurology, psychiatry/CL, genetics, speech/swallow, physio/OT, social work, and later palliative care. Complete advance care planning while capacity is intact. Support caregivers explicitly — burnout drives placement crises.[4][10][15]
Regional notes
ANZ (FRANZCP): HD services and genetics counselling pathways vary by state; clozapine rarely first-line for HD psychosis — prefer low-dose SGAs and HD clinic liaison. Tetrabenazine access commoner than newer VMAT2 agents in some settings — always teach depression monitoring. Use jurisdiction-specific Mental Health Act principles if capacity lacking (do not invent section numbers). UK (MRCPsych): Specialist HD clinics and CASC communication about genetics, suicide, and carer risk are high yield; NICE-aligned multidisciplinary care culture. US (ABPN): deutetrabenazine and valbenazine more often available for chorea; still teach tetrabenazine depression black-box culture and suicide epidemiology. South Asia (MD/DNB, NEET-SS): diagnostic delay common; family stigma and genetic secrecy complicate disclosure — prioritise collateral, suicide questions, and pragmatic SSRI/low-dose antipsychotic plans with neurology.[10][12][13][15]
Exam pearls
HD-RISK
Summary
Fellowship-level HD psychiatry is a genetic neurodegenerative interface: map depression, irritability, apathy, psychosis, and perseveration by stage; treat suicide risk as disease-core; use expert-consensus psychopharmacology with low-start SSRIs and cautious antipsychotics; and integrate VMAT2 chorea therapy only with active mood monitoring. A candidate who asks about predictive testing aftermath, refuses to conflate apathy with depression, names TETRA-HD/FIRST-HD cautions, and builds a multidisciplinary safety plan has mastered the exam spine of this topic.[1][5][10][12][13]
References
- [1]van Duijn E, Craufurd D, Hubers AA, et al. Neuropsychiatric symptoms in a European Huntington's disease cohort (REGISTRY) J Neurol Neurosurg Psychiatry, 2014.PMID 24828898
- [2]Craufurd D, Thompson JC, Snowden JS Behavioral changes in Huntington Disease Neuropsychiatry Neuropsychol Behav Neurol, 2001.PMID 11725215
- [3]Rosenblatt A Neuropsychiatry of Huntington's disease Dialogues Clin Neurosci, 2007.PMID 17726917
- [4]Paoli RA, Botturi A, Ciammola A, et al. Neuropsychiatric Burden in Huntington's Disease Brain Sci, 2017.PMID 28621715
- [5]Hubers AA, van Duijn E, Roos RA, et al. Suicidal ideation in a European Huntington's disease population J Affect Disord, 2013.PMID 23876196
- [6]van Duijn E, Fernandes AR, Abreu D, et al. Incidence of completed suicide and suicide attempts in a global prospective study of Huntington's disease BMJ Ment Health, 2021.PMID 34462049
- [7]Wetzel HH, Gehl CR, Dellefave-Castillo L, et al. Suicidal ideation in Huntington disease: the role of comorbidity J Neuropsychiatry Clin Neurosci, 2011.PMID 21605914
- [8]Epping EA, Mills JA, Beglinger LJ, et al. Characterization of depression in prodromal Huntington disease in the neurobiological predictors of HD (PREDICT-HD) study J Neuropsychiatry Clin Neurosci, 2013.PMID 23790259
- [9]Epping EA, Kim JI, Craufurd D, et al. Longitudinal Psychiatric Symptoms in Prodromal Huntington's Disease: A Decade of Data Am J Psychiatry, 2016.PMID 26472629
- [10]Anderson KE, van Duijn E, Craufurd D, et al. Clinical Management of Neuropsychiatric Symptoms of Huntington Disease: Expert-Based Consensus Guidelines on Agitation, Anxiety, Apathy, Psychosis and Sleep Disorders J Huntingtons Dis, 2018.PMID 30040737
- [11]Groves M, van Duijn E, Anderson K, et al. An International Survey-based Algorithm for the Pharmacologic Treatment of Irritability in Huntington's Disease PLoS Curr, 2011.PMID 21975525
- [12]Huntington Study Group Tetrabenazine as antichorea therapy in Huntington disease: a randomized controlled trial Neurology, 2006.PMID 16476934
- [13]Huntington Study Group, Frank S, Testa CM, et al. Effect of Deutetrabenazine on Chorea Among Patients With Huntington Disease: A Randomized Clinical Trial JAMA, 2016.PMID 27380342
- [14]Walker FO Huntington's disease Lancet, 2007.PMID 17240289
- [15]McColgan P, Tabrizi SJ Huntington's disease: a clinical review Eur J Neurol, 2018.PMID 28817209
- [16]van Duijn E Medical treatment of behavioral manifestations of Huntington disease Handb Clin Neurol, 2017.PMID 28947111