Psych · Consultation-liaison psychiatry
Mild cognitive impairment
Also known as MCI · Mild neurocognitive disorder · Mild NCD · Cognitive impairment no dementia · Amnestic MCI
Exam-exhaustive fellowship topic on mild cognitive impairment and mild neurocognitive disorder — Petersen/Winblad criteria, DSM-5-TR mild NCD, amnestic vs non-amnestic subtypes, conversion risk and reversion, MoCA vs MMSE, work-up for reversible causes, differential from ageing/depression/major NCD/delirium, lifestyle and risk-factor care (Lancet Commission, FINGER), and why cholinesterase inhibitors are not routine for MCI (AAN, Cochrane, Petersen 2005, InDDEx). FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
MCI sits at the CL/old-age interface where examiners test nosology, functional independence, conversion literacy, depression/delirium traps, and pharmacology restraint. The candidate who starts donepezil "to stop Alzheimer disease" without evidence fails; the candidate who formulates subtype, risk, reversible factors, and a monitoring plan passes.[9][10][15]
Overview and definition
Clinical MCI (Petersen criteria lineage) classically requires: a cognitive concern (patient, informant, or clinician); objective impairment relative to age and education; largely preserved general cognition; essentially normal functional activities; and absence of dementia.[1][2][27]
The International Working Group (Winblad 2004) framed MCI as a heterogeneous syndrome rather than a single disease, endorsing amnestic versus non-amnestic and single- versus multi-domain stratification.[3]
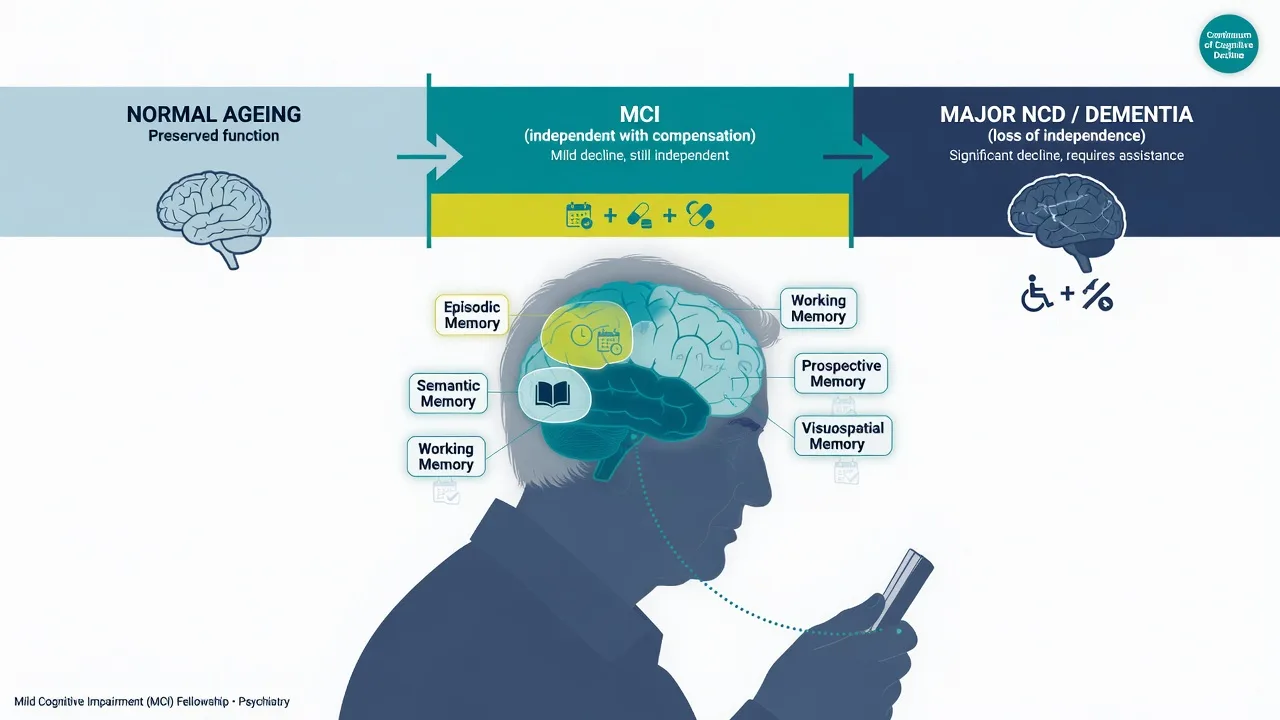
In DSM-5-TR, the parallel construct is mild neurocognitive disorder (mild NCD): modest decline from a previous level of performance in one or more cognitive domains (complex attention, executive function, learning and memory, language, perceptual-motor, or social cognition); the deficits do not interfere with independence in everyday activities (though greater effort, compensatory strategies, or accommodation may be required); not exclusively in the context of delirium; and not better explained by another mental disorder.[8]
ICD-11 likewise recognises mild neurocognitive disorder as modest cognitive decline with preserved independence. Fellowship answers should be bilingual: MCI for clinical/research language still ubiquitous in memory clinics; mild NCD when speaking pure DSM; and always name the independence hinge that separates mild from major NCD.[8][9]
Classification and subtypes
| Subtype | Core profile | Exam relevance |
|---|---|---|
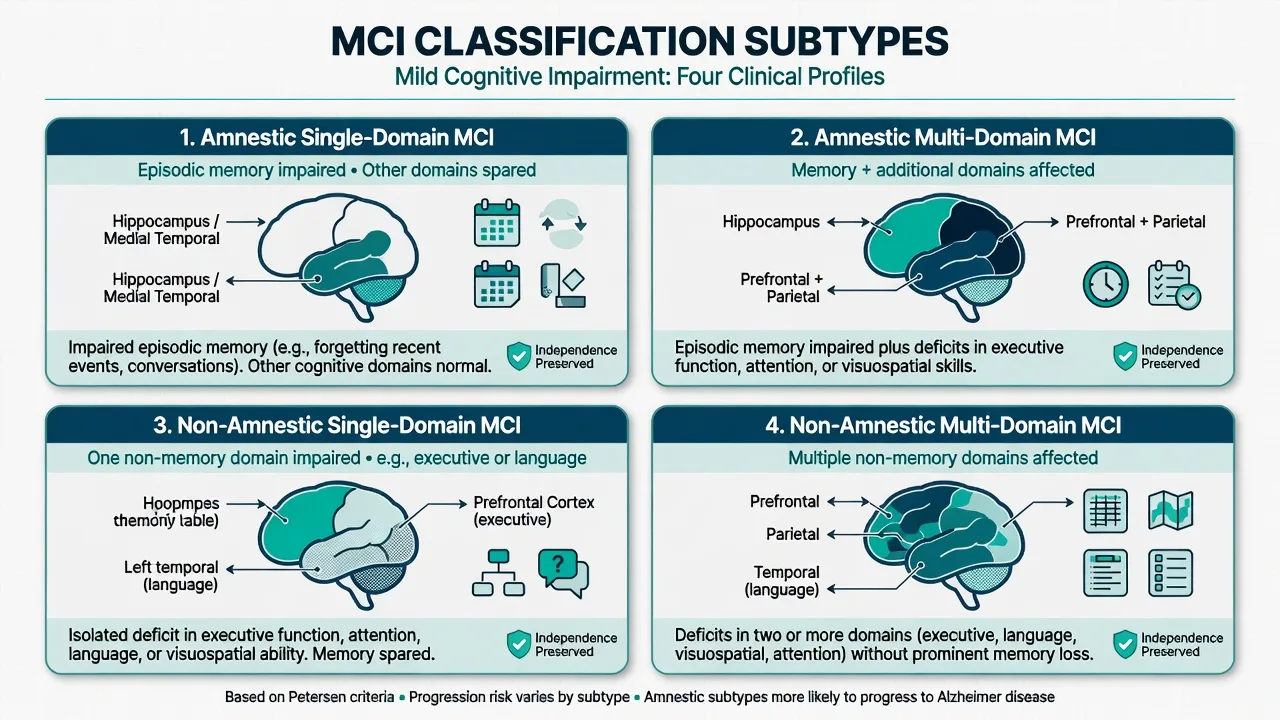
| Amnestic single-domain | Episodic memory impaired; other domains relatively spared | Classic AD-risk phenotype in many series |
| Amnestic multi-domain | Memory plus ≥1 other domain | Higher conversion risk than single-domain in many cohorts |
| Non-amnestic single-domain | Executive, language, or visuospatial alone | Consider vascular, FTD spectrum, other non-AD pathways |
| Non-amnestic multi-domain | Multiple non-memory domains | Heterogeneous; careful aetiological work-up |
MCI due to Alzheimer disease (NIA-AA)
Albert 2011 NIA-AA criteria define MCI due to AD clinically (cognitive concern, objective impairment, preserved independence, not demented) and allow research use of biomarkers to increase certainty of underlying AD pathophysiology. This sits between preclinical AD (Sperling) and dementia due to AD (McKhann).[5][6][7]
The NIA-AA Research Framework (Jack 2018) emphasises a biological (ATN) definition of AD for research — fellowship viva awareness, not a community mandatory panel in every MCI case.[26]
Mild behavioural impairment
Mild behavioural impairment (MBI) criteria (Ismail et al.) capture late-life persistent neuropsychiatric symptoms (apathy, affective dysregulation, impulse dyscontrol, social inappropriateness, abnormal perception/thought content) as possible early manifestations of neurodegeneration, including when frank MCI criteria are borderline.[28]
Epidemiology and conversion risk
Prevalence of MCI rises with age and depends on definition and setting (community versus specialty clinic).[9][10][11]
Conversion to dementia is the classic exam statistic. Mitchell and Shiri-Feshki's meta-analysis of robust inception cohorts showed elevated progression rates that vary by sample (clinic samples higher than community) and definition; annualised rates historically quoted near about 10% per year in many clinic series are useful order-of-magnitude figures, but candidates must also state that many remain stable and some revert to normal cognition.[11][9]
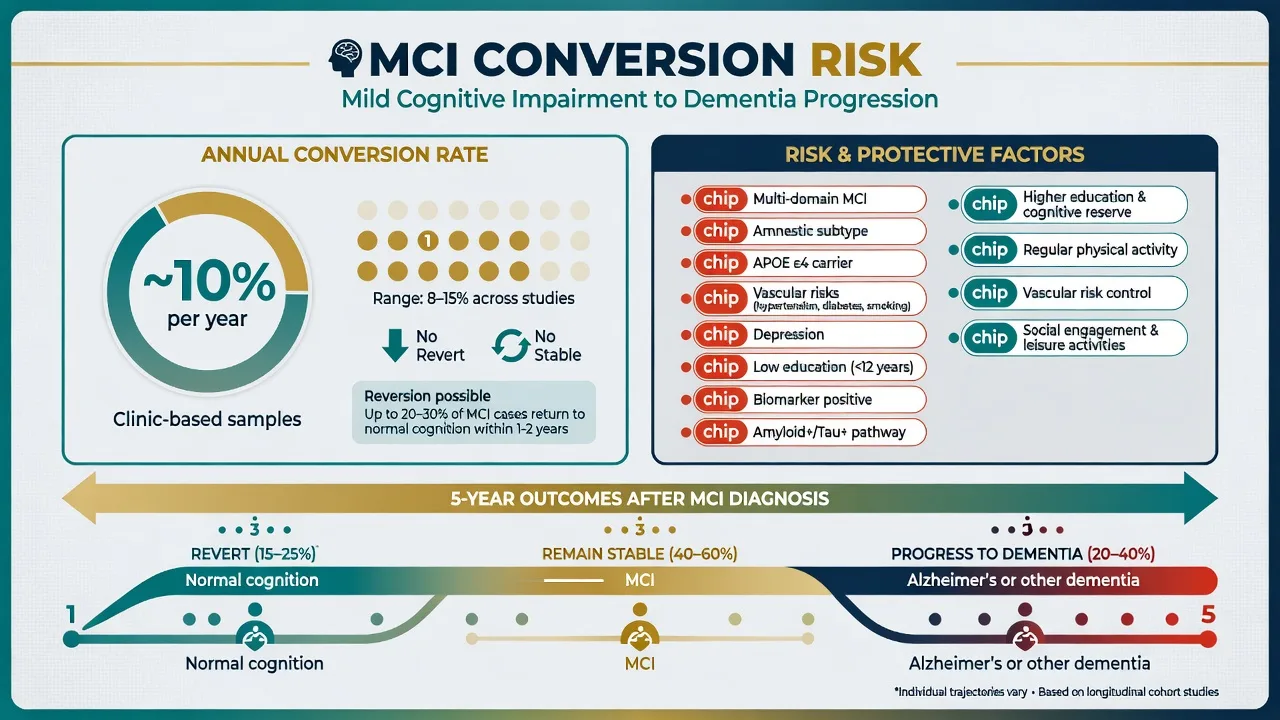
Modifiable predictors of progression from MCI to dementia (Cooper meta-analysis) include diabetes, and signals for other vascular and lifestyle factors — reinforcing risk-factor management even when disease-modifying drugs are not indicated.[12]
APOE ε4, family history, and AD biomarker positivity increase likelihood of underlying AD pathology and conversion risk but do not replace clinical diagnosis or functional assessment.[5][9]
Pathophysiology (exam-depth)
MCI is a clinical syndrome with multiple substrates: early Alzheimer pathology, cerebrovascular disease, mixed pathology, Lewy body disease prodrome, frontotemporal spectrum, medical/toxic-metabolic contributors, and psychiatric comorbidity.[3][4][9]
The AD continuum model (preclinical → MCI due to AD → dementia due to AD) is the research backbone; vascular and mixed pathology dominate real-world older adults.[5][7][20]
Cholinergic basal forebrain degeneration is relevant to dementia pharmacotherapy, but trial evidence does not support using AChEIs to delay conversion from MCI to dementia as routine practice.[15][16][17]
Clinical presentation
Typical referral: progressive memory or executive complaints over months to years; patient or family notice missed appointments, repeated questions, or word-finding; person still cooks, drives with caution, manages bills with lists or partner oversight.[1][9]
MSE focus: orientation often near-normal; free recall weak with variable cueing benefit; executive errors on clock/trail tasks; language usually conversationally intact early in amnestic MCI; mood (depression/anxiety/apathy); insight partial; no delirium-level inattention.[9][13]
Neuropsychiatric symptoms (depression, anxiety, irritability, apathy) are common and prognostically relevant — treat them, and consider MBI framing when behavioural change leads.[23][28]
Differential diagnosis
| Entity | Discriminators |
|---|---|
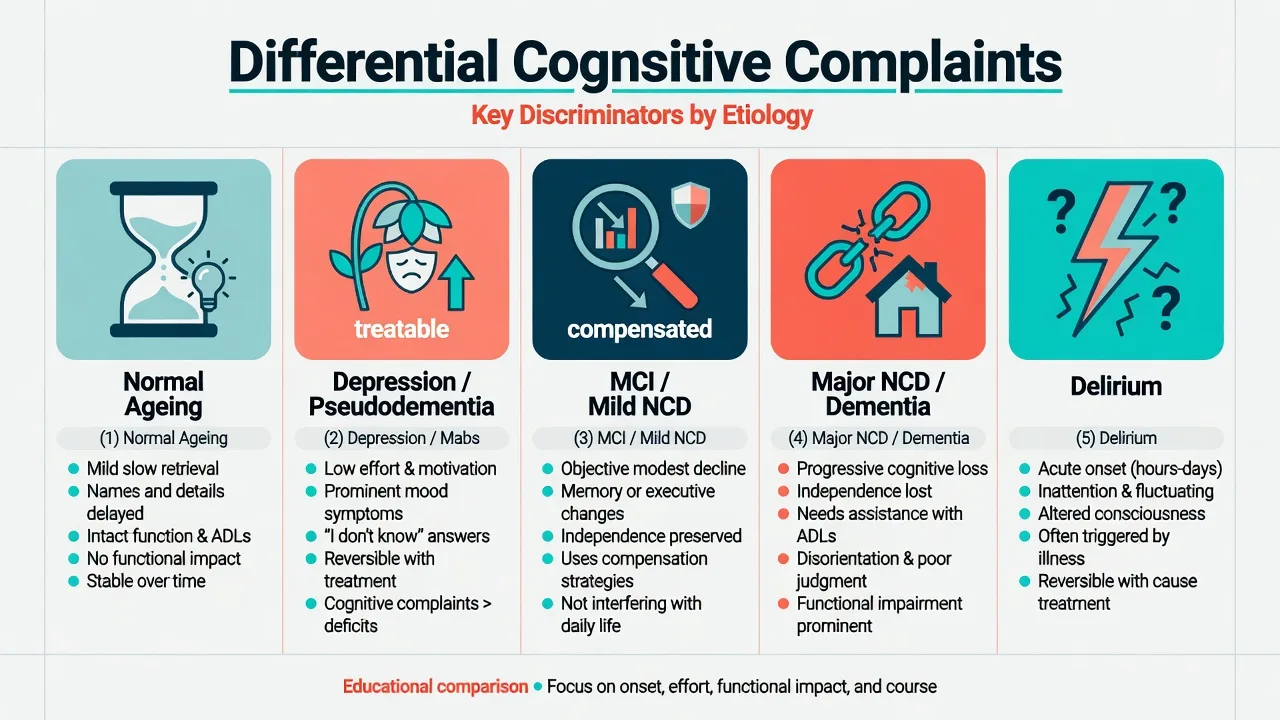
| Normal ageing | Mild retrieval slowing; function intact; stable trajectory |
| Depression-related cognitive impairment | Low effort, pervasive mood/anhedonia, "I don't know" responses; treat mood and reassess cognition |
| MCI / mild NCD | Objective modest decline; independence preserved with compensation |
| Major NCD / dementia | Independence interfered with |
| Delirium | Acute onset, inattention, fluctuation — not an MCI diagnosis setting |
Also exclude: medications (anticholinergics, benzodiazepines, opioids), alcohol, OSA, B12/thyroid/metabolic disease, sensory impairment, and in atypical/rapid cases infection, autoimmune encephalitis, structural lesions, and prion disease pathways.[9][10]
Assessment
- History with collateral — onset, tempo, domains, function (IADLs: finances, medications, shopping, cooking, transport), mood, sleep (including dream enactment), vascular risks, alcohol, medications.[9][10]
- MSE as above plus risk (driving, fire, finance, self-neglect, carer stress).[9]
- Cognitive screens — MoCA is more sensitive than MMSE for mild deficits; neither replaces formal neuropsychology when diagnosis is uncertain or stakes are high (medico-legal, atypical profile). Education, language, and culture affect cut-offs.[13][14]
- Functional assessment is the mild-versus-major discriminator — interview plus informant report of real-world independence.[8][9]
- Capacity is decision-specific (Appelbaum: understand, appreciate, reason, communicate a choice). Many people with MCI retain capacity for treatment and placement decisions; reassess for complex financial instruments or high-risk driving.[25]
Investigations
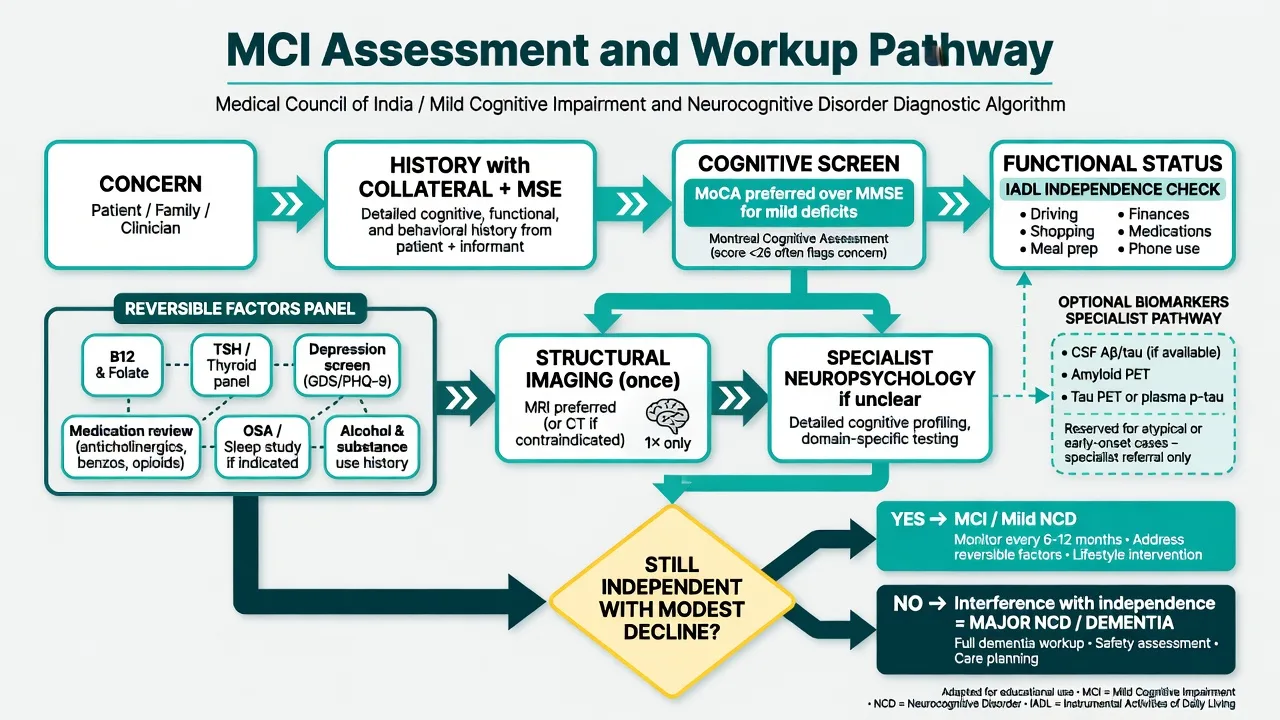
Baseline bloods: FBC, electrolytes/renal, glucose/HbA1c, B12, folate, TSH, calcium; consider HIV/syphilis if risk factors or atypical features.[9][10]
Structural imaging once (MRI preferred where available; CT acceptable) to exclude mass lesion, significant vascular burden, and support subtype thinking — discuss patterns educationally; do not invent a "patient scan".[9][10]
Specialist biomarkers (CSF Aβ/tau, PET, emerging plasma assays) belong in memory clinic/research pathways with region-dependent access — not universal primary-care MCI panels.[5][26]
Management
Acute / safety
There is no "MCI rapid tranquilisation" pathway. Acute cognitive change is a delirium work-up. Address immediate safety: driving advice if indicated, financial vulnerability, fire risk, and carer support.[9][10]
Definitive care (what actually helps)
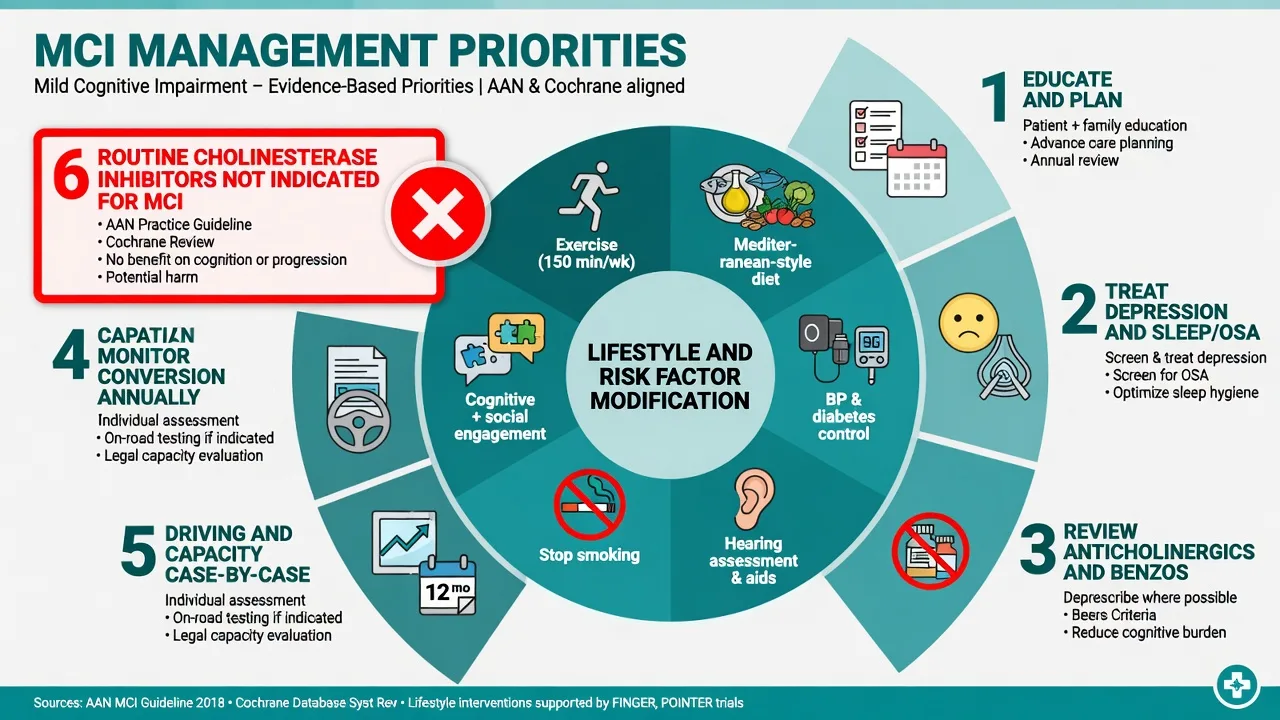
Education and planning. Explain heterogeneity (progress / stable / revert), the independence threshold for dementia, and value of early legal/financial planning while capacity is clear.[9][10][11]
Lifestyle and risk-factor modification. Align with Lancet Commission dementia prevention pillars (education, hearing, hypertension, obesity, smoking, depression, physical inactivity, social isolation, diabetes, alcohol, TBI, air pollution, among others) and FINGER multidomain trial evidence that diet, exercise, cognitive training, and vascular risk monitoring can benefit cognition in at-risk older adults.[20][21][22]
Treat comorbidity: late-life depression and anxiety; sleep disorders including OSA; sensory impairment (hearing aids); vascular risk optimisation.[12][23][24]
Deprescribe where safe: anticholinergics, long-term benzodiazepines, and other cognitive toxins.[9][10]
Cholinesterase inhibitors and related drugs — limits in MCI
This is a high-yield exam trap — conversion-prevention pharmacotherapy is not supported as routine care for pure MCI.[10][17]
- Petersen 2005 (NEJM): donepezil produced a modest reduction in progression rate at 12 months that was not sustained at 36 months; vitamin E was not effective; donepezil caused more adverse events (including GI and muscle cramps).[15]
- InDDEx (Feldman 2007): rivastigmine did not significantly delay diagnosis of Alzheimer disease from MCI and increased withdrawals for side effects.[16]
- Cochrane (Russ and Morling 2012) and commentary: little evidence of benefit; not recommended for MCI; adverse effects including GI and possible increased mortality signal in some pooled data warrant caution.[17][19]
- Tricco 2013 meta-analysis: cognitive enhancers show limited efficacy signals with important safety concerns in MCI populations.[18]
- AAN 2018 practice guideline update on MCI: clinicians may choose not to offer cholinesterase inhibitors; if offered, discuss lack of evidence for meaningful long-term benefit and risk of side effects; emphasise exercise and cognitive/lifestyle counselling.[10]
Practical exam line: for pure MCI/mild NCD without a concurrent dementia (major NCD) indication, do not start donepezil, rivastigmine, or galantamine as routine conversion prevention. Memantine is not an MCI conversion drug. If the person actually meets major NCD/AD criteria, manage under dementia pathways instead.[10][15][17]
Psychological and social care
Supportive counselling, carer education, cognitive strategies (external aids), and referral to memory services or community aged-care supports as needed. CBT elements may help anxiety/depression co-travelers.[9][23]
Special populations and scenarios
- Young-onset MCI: expanded differential and earlier specialist referral.[9]
- Post-delirium hospital consult: wait for recovery before diagnosing MCI; serial testing.[9]
- Intellectual disability / low baseline literacy: track change from baseline, not absolute screen cut-offs.[8]
- CALD / Indigenous peoples: culturally safe assessment; interpreter use; avoid over-pathologising language/education effects.[9]
- Comorbid SMI: separate medication effects, negative symptoms, and true neurocognitive decline from progressive MCI/major NCD trajectories.[9]
Prognosis and disposition
Counsel three possible trajectories: progression to major NCD, stability, or reversion. Review typically every 6–12 months sooner if change is reported. Reclassify when independence is lost. Document driving advice and safety planning. Link to dementia services if conversion occurs.[10][11][9]
Regional notes
ANZ (FRANZCP). Use mild NCD/MCI language fluently; memory clinic pathways vary by jurisdiction; cholinesterase inhibitors are licensed/indicated for dementia, not as routine conversion prevention in pure MCI. Driving fitness is clinician judgement plus local transport authority rules. Guardianship statutes are state/territory-specific — state principles (least restriction, decision-specificity) without inventing section numbers.[10][9][25]
UK (MRCPsych). Dementia pathways emphasise prevention and post-diagnostic support; do not invent UK-specific drug licences for MCI conversion. CASC: explain MCI without terror or false reassurance.[10][20]
US (ABPN). AAN MCI guideline is a core citation; billing/coding and biomarker access differ by system.[10][26]
India (MD/DNB, NEET-SS). High burden of vascular risk factors and mixed pathology; family collateral and medication review (including OTC anticholinergics) are critical; access to formal neuropsychology and biomarkers is uneven.[9][12][20]
Exam pearls
MCI CARE
References
- [1]Petersen RC, Smith GE, Waring SC, et al. Mild cognitive impairment: clinical characterization and outcome Arch Neurol, 1999.PMID 10190820
- [2]Petersen RC, Doody R, Kurz A, et al. Current concepts in mild cognitive impairment Arch Neurol, 2001.PMID 11735772
- [3]Winblad B, Palmer K, Kivipelto M, et al. Mild cognitive impairment--beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment J Intern Med, 2004.PMID 15324367
- [4]Gauthier S, Reisberg B, Zaudig M, et al. Mild cognitive impairment Lancet, 2006.PMID 16631882
- [5]Albert MS, DeKosky ST, Dickson D, et al. The diagnosis of mild cognitive impairment due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease Alzheimers Dement, 2011.PMID 21514249
- [6]McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease Alzheimers Dement, 2011.PMID 21514250
- [7]Sperling RA, Aisen PS, Beckett LA, et al. Toward defining the preclinical stages of Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease Alzheimers Dement, 2011.PMID 21514248
- [8]Sachdev PS, Blacker D, Blazer DG, et al. Classifying neurocognitive disorders: the DSM-5 approach Nat Rev Neurol, 2014.PMID 25266297
- [9]Langa KM, Levine DA The diagnosis and management of mild cognitive impairment: a clinical review JAMA, 2014.PMID 25514304
- [10]Petersen RC, Lopez O, Armstrong MJ, et al. Practice guideline update summary: Mild cognitive impairment [RETIRED]: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology Neurology, 2018.PMID 29282327
- [11]Mitchell AJ, Shiri-Feshki M Rate of progression of mild cognitive impairment to dementia--meta-analysis of 41 robust inception cohort studies Acta Psychiatr Scand, 2009.PMID 19236314
- [12]Cooper C, Sommerlad A, Lyketsos CG, et al. Modifiable predictors of dementia in mild cognitive impairment: a systematic review and meta-analysis Am J Psychiatry, 2015.PMID 25698435
- [13]Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment J Am Geriatr Soc, 2005.PMID 15817019
- [14]Folstein MF, Folstein SE, McHugh PR "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician J Psychiatr Res, 1975.PMID 1202204
- [15]Petersen RC, Thomas RG, Grundman M, et al. Vitamin E and donepezil for the treatment of mild cognitive impairment N Engl J Med, 2005.PMID 15829527
- [16]Feldman HH, Ferris S, Winblad B, et al. Effect of rivastigmine on delay to diagnosis of Alzheimer's disease from mild cognitive impairment: the InDDEx study Lancet Neurol, 2007.PMID 17509485
- [17]Russ TC, Morling JR Cholinesterase inhibitors for mild cognitive impairment Cochrane Database Syst Rev, 2012.PMID 22972133
- [18]Tricco AC, Soobiah C, Berliner S, et al. Efficacy and safety of cognitive enhancers for patients with mild cognitive impairment: a systematic review and meta-analysis CMAJ, 2013.PMID 24043661
- [19]Russ TC Cholinesterase inhibitors should not be prescribed for mild cognitive impairment Evid Based Med, 2014.PMID 24482151
- [20]Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission Lancet, 2020.PMID 32738937
- [21]Livingston G, Sommerlad A, Orgeta V, et al. Dementia prevention, intervention, and care Lancet, 2017.PMID 28735855
- [22]Ngandu T, Lehtisalo J, Solomon A, et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a randomised controlled trial Lancet, 2015.PMID 25771249
- [23]Butters MA, Young JB, Lopez O, et al. Pathways linking late-life depression to persistent cognitive impairment and dementia Dialogues Clin Neurosci, 2008.PMID 18979948
- [24]Taylor WD, Aizenstein HJ, Alexopoulos GS The vascular depression hypothesis: mechanisms linking vascular disease with depression Mol Psychiatry, 2013.PMID 23439482
- [25]Appelbaum PS, Grisso T Assessing patients' capacities to consent to treatment N Engl J Med, 1988.PMID 3200278
- [26]Jack CR Jr, Bennett DA, Blennow K, et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer's disease Alzheimers Dement, 2018.PMID 29653606
- [27]Petersen RC Mild Cognitive Impairment Continuum (Minneap Minn), 2016.PMID 27042901
- [28]Ismail Z, Smith EE, Geda Y, et al. Neuropsychiatric symptoms as early manifestations of emergent dementia: Provisional diagnostic criteria for mild behavioral impairment Alzheimers Dement, 2016.PMID 26096665