Psych · Consultation-liaison psychiatry
Multiple sclerosis psychiatry
Also known as MS depression · Multiple sclerosis neuropsychiatry · Pseudobulbar affect MS · MS cognitive impairment psychiatry · Suicide multiple sclerosis · MS psychiatric comorbidity · Interferon depression MS
Exam-exhaustive fellowship topic on the psychiatry of multiple sclerosis: depression and suicide risk, anxiety, pseudobulbar affect, cognitive impairment, steroid and DMT interfaces, AAN psychiatric guidance, and joint CL–neurology management. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Psychiatrists fail this topic when they leave MS depression untreated as "understandable," mislabel PBA as bipolar mood lability, stop a disease-modifying therapy (DMT) unilaterally for mild dysphoria, or miss suicide risk after a new disability milestone. Examiners reward structured screening, suicide literacy, PBA pharmacology (dextromethorphan/quinidine where available), and joint neurology plans.[3][10][12]
Overview and definition
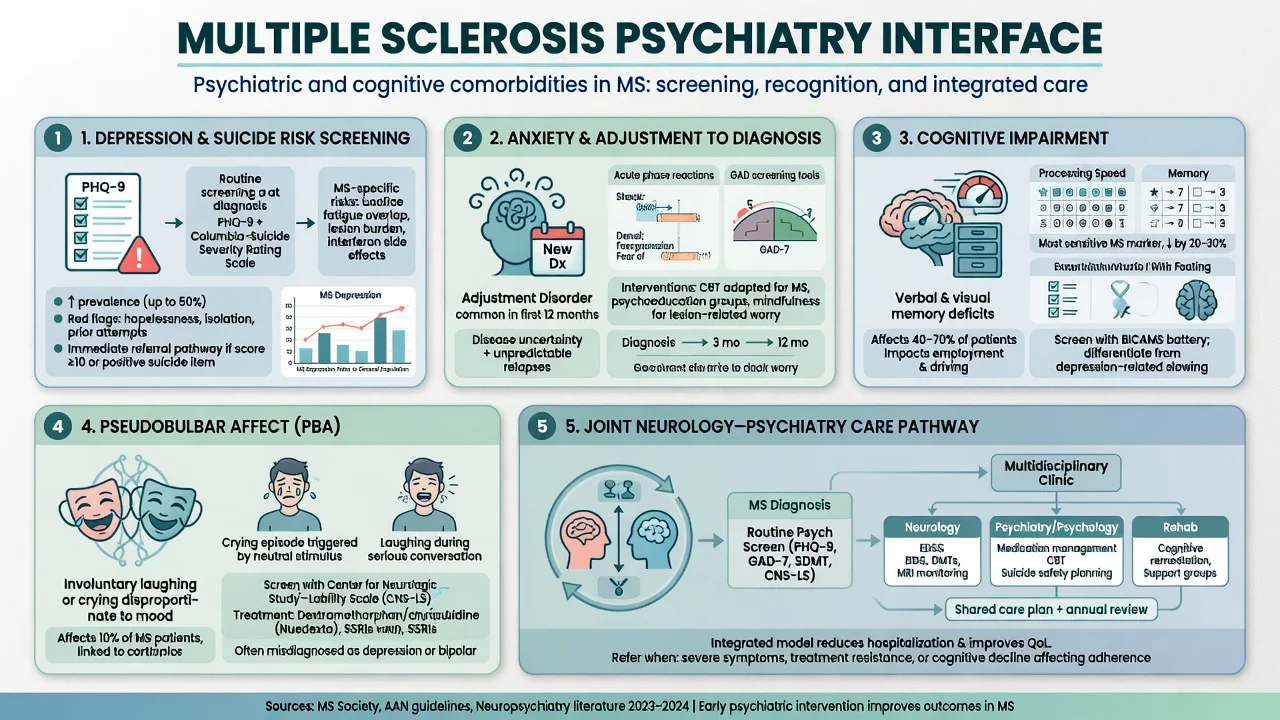
MS psychiatry covers the neuropsychiatric syndromes of CNS demyelinating disease: major depression and demoralisation, anxiety spectrum disorders, PBA (involuntary emotional expression), cognitive impairment with employment impact, bipolar and psychotic presentations (including corticosteroid-induced), substance and sleep comorbidity, and the psychopharmacology of agents that interact with fatigue, spasticity drugs, and DMTs. In DSM-5-TR language many presentations map to mental disorder due to another medical condition or medication-induced disorders; the clinical task is mechanism-aware management without sacrificing disease control or safety.[3][4][15]
Epidemiology
Depression and anxiety are highly prevalent in MS. A systematic review and meta-analysis by Boeschoten and colleagues pooled a large literature and confirmed substantially elevated rates versus general population benchmarks, with heterogeneity by instrument, sampling frame, and diagnostic threshold — examiners should quote "common and clinically important," not a single false-precise percentage from memory.[2] Community and clinic data show depressive symptoms track illness severity and disability burden, though depression is not simply a linear function of EDSS alone.[6]
The Goldman Consensus framed depression in MS as under-recognised and undertreated, calling for systematic clinical attention rather than passive acceptance of low mood as inevitable.[1] Suicide risk is elevated relative to the general population; Feinstein and colleagues synthesise mechanisms spanning depression, social isolation, substance use, and disease milestones, while Kalb and co-authors emphasise red flags and ethical risk management.[9][10]
Cognitive impairment affects a large minority to majority of people with MS depending on battery and cut-points; Rao's classic series established frequency, patterns (notably processing speed and memory), and predictors still taught in fellowship exams.[13] Psychiatric comorbidity is associated with greater disability progression risk in population analyses — another reason mood is not a "soft" add-on to motor care.[16]
Classification of key syndromes
Depression and demoralisation
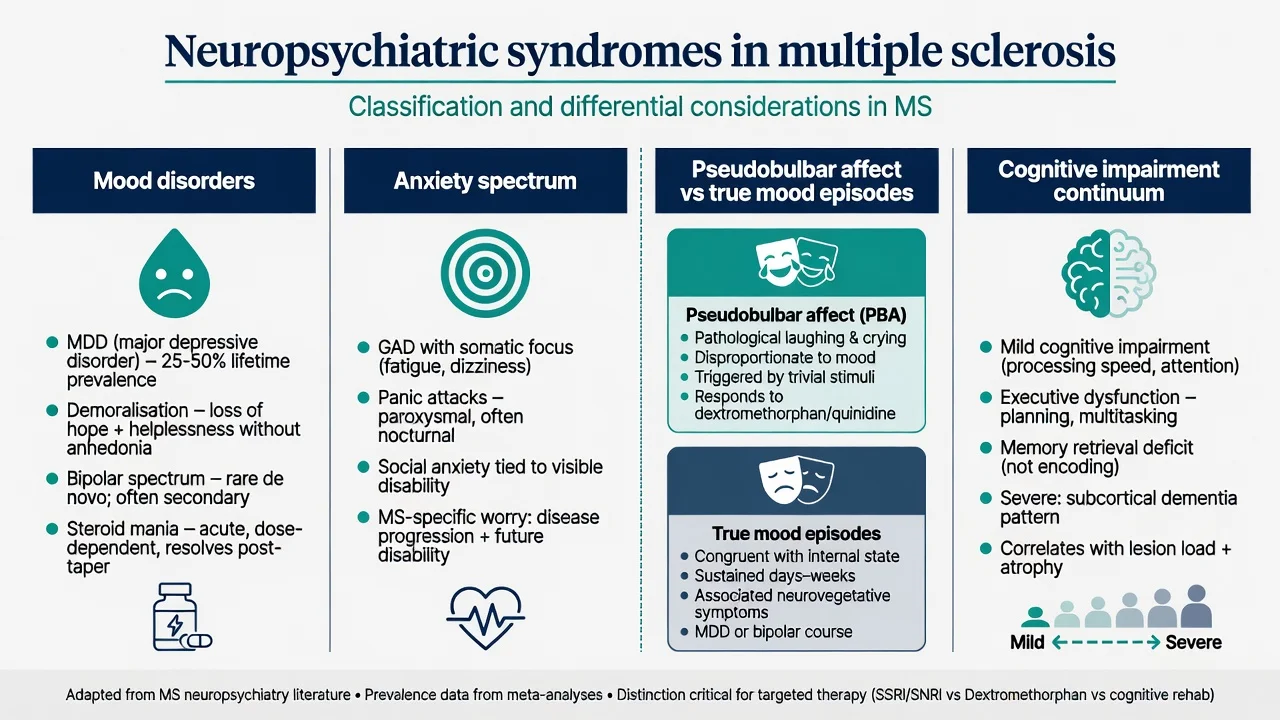
Major depression includes persistent dysphoria, anhedonia, guilt, worthlessness, and suicidality with functional impact. Demoralisation/adjustment after diagnosis or progression may be reactive without full major depressive episode criteria — still needs support, but treatment intensity differs. Somatic overlap with MS (fatigue, sleep disruption, concentration difficulty, pain) forces careful history of mood-congruent cognitive content, diurnal variation, and loss of interest beyond disability limits.[1][4][5]
Pseudobulbar affect
PBA is brief, involuntary laughing or crying that is exaggerated or incongruent relative to subjective mood, often socially disabling. It is a network/disconnection syndrome (corticobulbar and related pathways), not proof of mania or histrionic personality. Quantitative MRI work in MS links PBA to specific lesion patterns; treatment targets the expression disorder, not only "mood."[11][12]
Cognitive impairment
MS cognitive impairment classically emphasises processing speed, episodic memory, and executive function more than dense cortical aphasia syndromes. Employment and social role loss follow cognitive change even when motor disability is moderate — a high-yield viva point from Rao's programme of work.[13]
Steroid and secondary affective/psychotic states
High-dose corticosteroids for relapse can produce insomnia, euphoria, irritability, mania, or frank psychosis. Distinguish from primary bipolar disorder and from delirium due to infection or metabolic derangement. Onset is typically temporally linked to the pulse or high-dose taper window.[3][15]
Pathophysiology (viva depth)
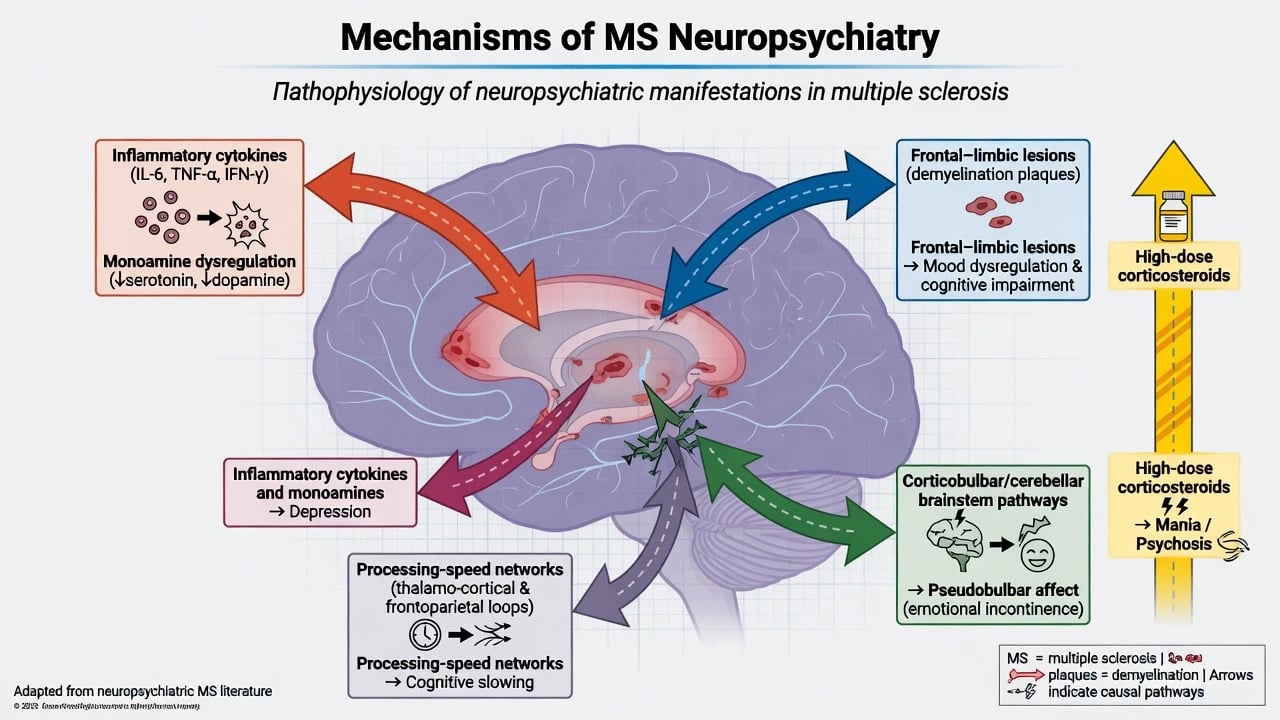
MS depression reflects a mix of inflammatory/cytokine signalling, monoaminergic disruption, lesion burden in mood-relevant white-matter tracts and cortical–subcortical circuits, and psychosocial load of unpredictable disability.[4][5] PBA maps to disinhibition of emotional expression networks rather than primary mood generation — Ghaffar and colleagues' quantitative MRI study supports anatomical correlates in MS populations.[11] Cognitive slowing tracks distributed network integrity and lesion load affecting information processing speed.[13] Steroid mania/psychosis is a dose- and vulnerability-related neuropsychiatric toxicity. Historical concern that interferon-beta "causes depression" is more nuanced in modern practice: population and treatment-association data (e.g. antidepressant use patterns with interferon versus glatiramer) inform risk communication without automatic DMT cessation for mild mood change.[14]
Clinical assessment for CL
Structure history around: MS phenotype (RRMS, SPMS, PPMS), recent relapses, disability milestones, full DMT and symptomatic list (baclofen, gabapentinoids, anticholinergics for bladder, opioids, cannabinoids, amantadine/modafinil for fatigue), recent steroid pulses, sleep, pain, bladder/bowel, sexual function, employment, caregiving, substance use, prior psychiatric history, and suicide risk with explicit ideation/plan/intent questions.[3][10][15]
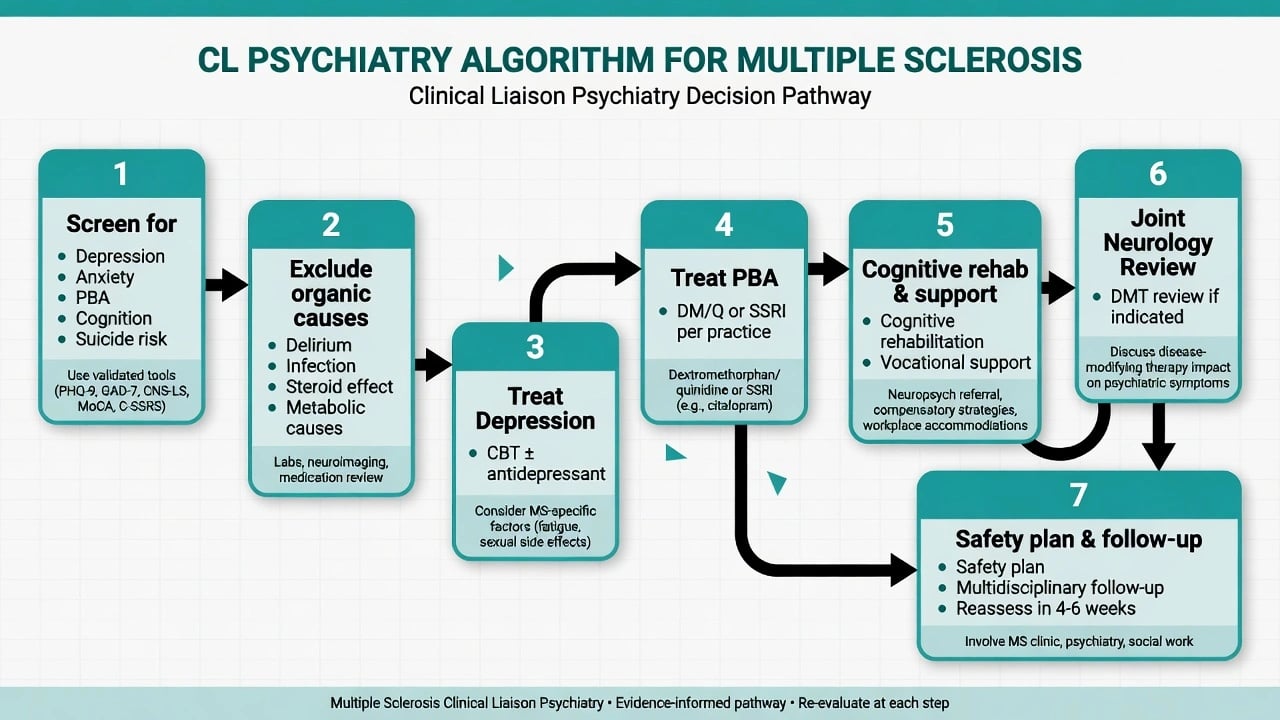
Screen mood with clinical interview as gold standard; PHQ-9/HADS can support serial monitoring but neurological symptom contamination is recognised — interpret scores clinically.[3] Ask specifically for PBA: sudden brief crying/laughing out of proportion to mood, difficulty stopping, social embarrassment.[11] Cognitive screens (e.g. Symbol Digit Modalities Test culture / formal neuropsychology when work capacity is contested) matter when complaints or functional decline appear.[13] Collateral from partners is often essential for PBA, cognition, and suicide risk minimisation.
Differential diagnosis
- MS fatigue versus depression versus medical contributors (hypothyroidism, anaemia, sleep apnoea, nocturia, sedating polypharmacy).
- PBA versus depressive crying, bipolar affect, frontal disinhibition, or seizures with affective automatisms (rare).
- Delirium (infection, metabolic, post-operative) versus new psychosis.
- Steroid-induced mood/psychosis versus primary bipolar disorder.
- Depression-related cognitive complaints versus objective MS cognitive impairment.
- Functional neurological symptoms can co-occur with MS — dual formulation may be needed, not either/or dogma.[3][4][15]
Investigations
Do not re-image the brain for every mood fluctuation. Reassess neurologically and investigate when there is new focal deficit suggesting relapse, fever/delirium features, atypical first-onset psychosis, or unexplained cognitive collapse. Baseline labs as indicated (TSH, B12, metabolic panel, infection screen); ECG and metabolic monitoring before selected psychotropics; formal neuropsychology for diagnostic clarity, rehabilitation planning, or medicolegal/vocational questions.[3][13]
Acute management
Suicide and crisis
Treat active suicidal ideation with standard crisis pathways, safety planning, and admission thresholds identical in principle to other high-risk depression — MS diagnosis is never a reason to withhold care. Identify red flags: severe depression, prior attempts, social isolation, substance use, progressive disability without hope, and access to means.[9][10]
Steroid-associated mania/psychosis
Coordinate urgently with neurology on steroid cessation/taper, rule out infection/delirium, use environmental measures, and short-term antipsychotic or mood-stabilising strategies as clinically indicated while motor and medical status are protected.[3][15]
Definitive management of depression
The Goldman Consensus and subsequent reviews make active treatment of MS depression a clinical priority, not optional soft care.[1][4][5] The AAN 2014 evidence-based guideline (Minden and colleagues) recommends assessment and management of psychiatric disorders in MS; it also notes limited high-quality comparative efficacy data for many specific interventions — fellowship answers should be honest about evidence gaps while still treating.[3]
Psychological therapies
Cognitive-behavioural therapy, including telephone-administered programmes evaluated by Mohr and colleagues, is a cornerstone option, particularly when mobility, fatigue, or rural access limit clinic attendance. Adapt pace for fatigue, cognitive load, and realistic activity scheduling. Address health anxiety around MRI/relapse cycles and injection or infusion procedures when relevant.[3][8]
Antidepressant pharmacotherapy
SSRIs and SNRIs are widely used in MS clinic practice. An RCT of paroxetine in persons with MS and major depressive disorder (Ehde and colleagues) informs exam-level discussion of pharmacotherapy feasibility and response patterns in this population.[7]
Practical exam dosing example (adult, after interaction and medical review): start paroxetine 10 mg oral once daily, titrate cautiously (e.g. toward 20 mg oral daily as tolerated under review), monitoring sexual dysfunction, hyponatraemia (especially older adults), bleeding risk with NSAIDs/anticoagulants, activation, and suicidality early in treatment. Alternative SSRIs (e.g. sertraline) are often chosen in practice for interaction profiles — individualise with local formulary and neurology input. Avoid overselling superiority of one agent where head-to-head MS-specific evidence is thin.[3][7]
Do not combine carelessly with MAOIs; review tramadol and other serotonergic agents for toxicity risk. Treat comorbid pain, sleep, and spasticity in parallel — untreated pain sabotages antidepressant response.[3][7][15]
Pseudobulbar affect management
Educate patients and families that PBA is a neurological expression disorder. Where available, dextromethorphan plus low-dose quinidine reduced PBA episodes in a randomised trial across neurological populations including relevant MS cohorts in the development programme; Pioro and colleagues reported efficacy of dextromethorphan with ultra-low-dose quinidine.[12]
Practical exam dosing (where licensed/accessible; adult PBA): dextromethorphan 20 mg / quinidine 10 mg oral, typically starting once daily then increasing to twice daily as per product guidance, with attention to QT prolongation, CYP2D6 interactions, serotonin syndrome risk with other serotonergic drugs, and falls/sedation. Access and subsidy are region-dependent. SSRIs are often used pragmatically for PBA when DM/Q is unavailable — acknowledge practice versus pivotal DM/Q trial evidence.[11][12]
Cognition, fatigue, and function
Cognitive rehabilitation strategies, vocational adjustment, fatigue pacing, and treating depression/sleep disorders are synergistic. Rao's work underpins the message that cognitive change predicts employment and social role loss — disposition plans should include practical supports, not only a prescription.[13] Fatigue management (energy conservation, treatable medical contributors, selected wake-promoting strategies with neurology) runs parallel to antidepressant care; do not promise that treating depression alone abolishes MS fatigue.[15]
DMT interface and interferon controversy
Discuss mood changes in the context of disease activity, disability, steroids, and life events — not only the DMT label. Observational work on antidepressant use alongside interferon versus glatiramer informs pharmacoepidemiologic thinking without mandating automatic interferon cessation for every low mood episode.[14] Any DMT change for psychiatric reasons should be a joint neurology–psychiatry decision weighing relapse risk versus psychiatric severity.[3][14]
Special populations
Young adults with new MS diagnosis: high identity disruption, educational/occupational stakes, and peer comparison — early mood screening. Pregnancy and postpartum: coordinate antidepressant and DMT safety with MS and perinatal psychiatry expertise. Progressive MS: higher disability, social isolation, and suicide vigilance. Cultural formulations of involuntary crying or laughing may be spiritualised — still assess PBA and suicide risk while respecting explanatory models. Rural/ANZ access: telephone CBT is exam-relevant for equity.[8][10][15]
Prognosis and disposition
Treated depression improves quality of life and engagement with MS care; untreated psychiatric comorbidity associates with worse disability trajectories in population data.[16] Disposition should specify MS clinic follow-up, mental health or CL review intensity for high-risk depression/PBA/psychosis, caregiver education, crisis contacts, and vocational/cognitive supports. Driving and occupational decisions follow local legal standards after cognitive or psychiatric risk changes — do not invent rules.[3][10]
Regional notes
ANZ (FRANZCP): Emphasise suicide risk assessment, collaborative MS clinic care, and telephone/telehealth CBT access for disability and distance. Dextromethorphan/quinidine availability and funding may be limited — know SSRI pragmatism for PBA and when to seek specialist pharmacy advice. Use jurisdiction-specific Mental Health Act principles if capacity lacking (do not invent section numbers). UK (MRCPsych): NICE MS pathway emphasises coordinated multidisciplinary care; CASC communication about depression, PBA, and DMT concerns is high yield. US (ABPN): AAN 2014 psychiatric guideline is core; DM/Q (Nuedexta) more familiar for PBA. South Asia (MD/DNB, NEET-SS): High family involvement in care; steroid mania after pulses for optic neuritis is a classic stem; ensure antidepressant access and suicide safety planning in resource-variable settings.[3][8][12]
Exam pearls
MS-MOOD
Summary
Fellowship-level MS psychiatry is a systems interface: depression is common, under-treated, and suicide-relevant (Goldman; Boeschoten; Feinstein/Kalb); PBA is a treatable expression disorder distinct from mood episodes (Ghaffar anatomy; Pioro DM/Q); cognition and fatigue demand structured assessment (Rao); and DMT or steroid decisions are joint with neurology (AAN Minden guideline; Patten treatment-context data). A candidate who screens for suicide, names telephone CBT and antidepressant practicality, separates PBA from bipolar disorder, and refuses unilateral DMT cessation has mastered the exam spine of this topic.[1][2][3][8][12][13]
References
- [1]Goldman Consensus Group The Goldman Consensus statement on depression in multiple sclerosis Mult Scler, 2005.PMID 15957516
- [2]Boeschoten RE, Braamse AMJ, Beekman ATF, et al. Prevalence of depression and anxiety in Multiple Sclerosis: A systematic review and meta-analysis J Neurol Sci, 2017.PMID 28017241
- [3]Minden SL, Feinstein A, Kalb RC, et al. Evidence-based guideline: assessment and management of psychiatric disorders in individuals with MS: report of the Guideline Development Subcommittee of the American Academy of Neurology Neurology, 2014.PMID 24376275
- [4]Feinstein A Multiple sclerosis and depression Mult Scler, 2011.PMID 22058085
- [5]Feinstein A, Magalhaes S, Richard JF, Audet B, Moore C The link between multiple sclerosis and depression Nat Rev Neurol, 2014.PMID 25112509
- [6]Chwastiak L, Ehde DM, Gibbons LE, et al. Depressive symptoms and severity of illness in multiple sclerosis: epidemiologic study of a large community sample Am J Psychiatry, 2002.PMID 12411220
- [7]Ehde DM, Kraft GH, Chwastiak L, et al. Efficacy of paroxetine in treating major depressive disorder in persons with multiple sclerosis Gen Hosp Psychiatry, 2008.PMID 18164939
- [8]Mohr DC, Hart SL, Julian L, et al. Telephone-administered psychotherapy for depression Arch Gen Psychiatry, 2005.PMID 16143732
- [9]Feinstein A, Pavisian B Multiple sclerosis and suicide Mult Scler, 2017.PMID 28327056
- [10]Kalb R, Feinstein A, Rohrig A, Sankary L, Willis A Depression and Suicidality in Multiple Sclerosis: Red Flags, Management Strategies, and Ethical Considerations Curr Neurol Neurosci Rep, 2019.PMID 31463644
- [11]Ghaffar O, Chamelian L, Feinstein A Neuroanatomy of pseudobulbar affect: a quantitative MRI study in multiple sclerosis J Neurol, 2008.PMID 18297331
- [12]Pioro EP, Brooks BR, Cummings J, et al. Dextromethorphan plus ultra low-dose quinidine reduces pseudobulbar affect Ann Neurol, 2010.PMID 20839238
- [13]Rao SM, Leo GJ, Bernardin L, Unverzagt F Cognitive dysfunction in multiple sclerosis. I. Frequency, patterns, and prediction Neurology, 1991.PMID 2027484
- [14]Patten SB, Williams JV, Metz LM Anti-depressant use in association with interferon and glatiramer acetate treatment in multiple sclerosis Mult Scler, 2008.PMID 17986504
- [15]Chwastiak LA, Ehde DM Psychiatric issues in multiple sclerosis Psychiatr Clin North Am, 2007.PMID 17938046
- [16]McKay KA, Tremlett H, Fisk JD, et al. Psychiatric comorbidity is associated with disability progression in multiple sclerosis Neurology, 2018.PMID 29523642