Psych · Consultation-liaison psychiatry
Pain psychiatry and somatic symptom disorders
Also known as Somatic symptom disorder · Illness anxiety disorder · Hypochondriasis · Medically unexplained symptoms · Functional somatic syndromes · Chronic pain psychiatry · Bodily distress disorder
Exam-exhaustive fellowship topic on pain psychiatry and somatic symptom disorders for consultation-liaison practice — DSM-5-TR SSD and illness anxiety (vs ICD-11 framing), chronic pain–psych interface, PHQ-15 assessment, CBT and stepped care evidence, cautious SNRI/TCA analgesia, and opioid dual-diagnosis principles. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Pain and multi-system somatic presentations are core consultation-liaison (C-L) work. Fellowship examiners test whether you can (1) use DSM-5-TR / ICD-11 language accurately, (2) avoid dualistic “real vs fake” traps, (3) run a safe assessment (organic red flags, risk, substance use), and (4) deliver evidence-weighted psychological and cautious pharmacological care without defaulting to long-term opioids.[1][6][24]
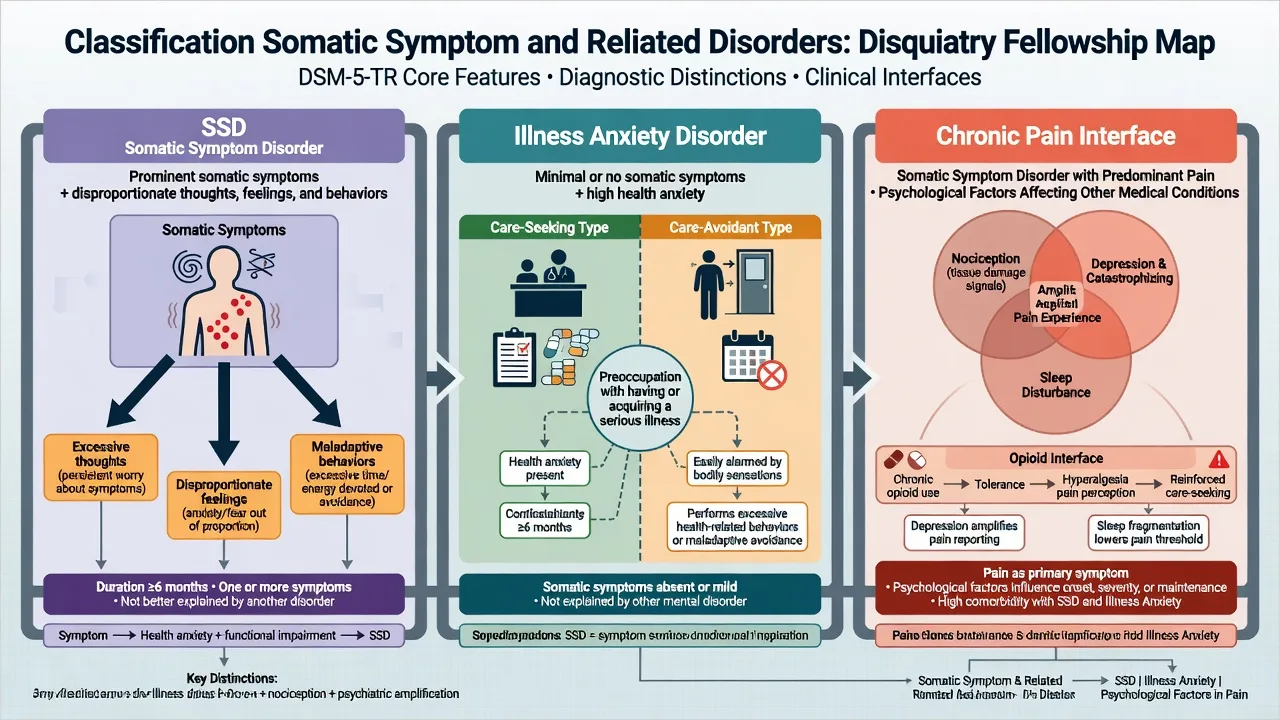
DSM-5-TR SSD requires one or more distressing somatic symptoms that disrupt daily life, plus excessive thoughts, feelings, or behaviours related to the symptoms (e.g. disproportionate health anxiety, high time/energy spent on symptoms, persistent high severity concern), typically for 6 months or more (symptoms may vary). Critically, a concurrent medical diagnosis does not exclude SSD if the cognitive-affective-behavioural B-criteria are met — this is the central DSM-5 reorganisation away from DSM-IV “medically unexplained” logic.[1][2]
Illness anxiety disorder features preoccupation with having or acquiring a serious illness, with somatic symptoms absent or only mild, high health anxiety, and excessive health-related behaviours (care-seeking) or maladaptive avoidance (care-avoidant), usually for at least 6 months. Legacy “hypochondriasis” maps mainly into IAD or SSD with predominant health anxiety, depending on symptom load.[1][3]
ICD-11 uses bodily distress disorder (re-experiencing of distressing bodily symptoms with excessive attention and help-seeking, severity graded) and retains hypochondriasis (health anxiety) framing. Fink’s bodily distress empirical work underpins much European teaching that multi-organ symptom clusters are clinically coherent even when specialist labels (IBS, fibromyalgia, etc.) fragment care.[7][6]
Chronic pain is not automatically SSD. ICD-11 chronic primary pain and disease-related chronic pain exist as pain diagnoses; psychiatry contributes when depression, anxiety, health beliefs, trauma, sleep, substance use, or disability amplify suffering or block rehabilitation. Functional somatic syndromes (e.g. IBS, fibromyalgia) are managed with the same both–and principles Henningsen and colleagues summarised for functional somatic syndromes: positive explanation, limited unfocused investigation, and multimodal care.[6][22]

Classification map (exam discriminators)
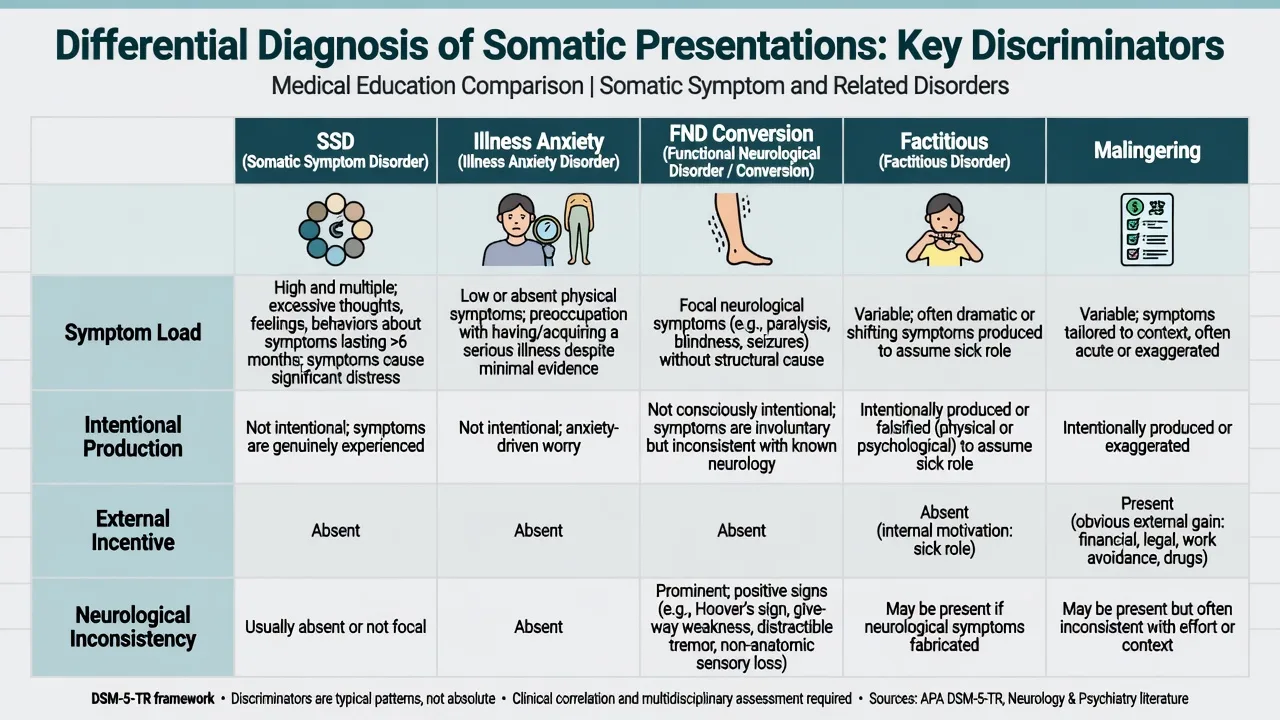
| Construct | Core | Symptom load | Classic trap |
|---|---|---|---|
| SSD | Disproportionate thoughts/feelings/behaviours about symptoms | One or more, often multi-system | Assuming medical disease excludes the diagnosis |
| IAD | Preoccupation with serious illness | Absent or mild | Missing care-avoidant subtype who refuses tests |
| FND / conversion | Voluntary motor/sensory symptoms with incompatibility findings | Neurological pattern | Calling all unexplained neurology “somatisation” |
| Factitious | Intentional symptom production, sick role | Variable | Accusing without evidence |
| Malingering | Intentional production for external incentive | Variable | Using the label as a discharge tool |
Mayou’s critique remains examinable: DSM-5 SSD is broader and can pathologise adaptive illness concern if B-criteria are applied loosely — document impairment and excessiveness, not mere worry about real disease.[3]
Epidemiology and clinical burden
Multiple distressing somatic symptoms are common in primary care and medical clinics; high PHQ-15 scores associate with functional impairment, depression/anxiety comorbidity, and utilisation.[4][5] Depression and musculoskeletal pain co-travel; optimising antidepressant care plus pain self-management improves both domains in primary-care trials (SCAMP).[23] Psychiatric comorbidity is a major missing piece in opioid-era chronic pain systems — the “missing P” in pain management.[24]
Mechanisms — pain, attention, and amplification
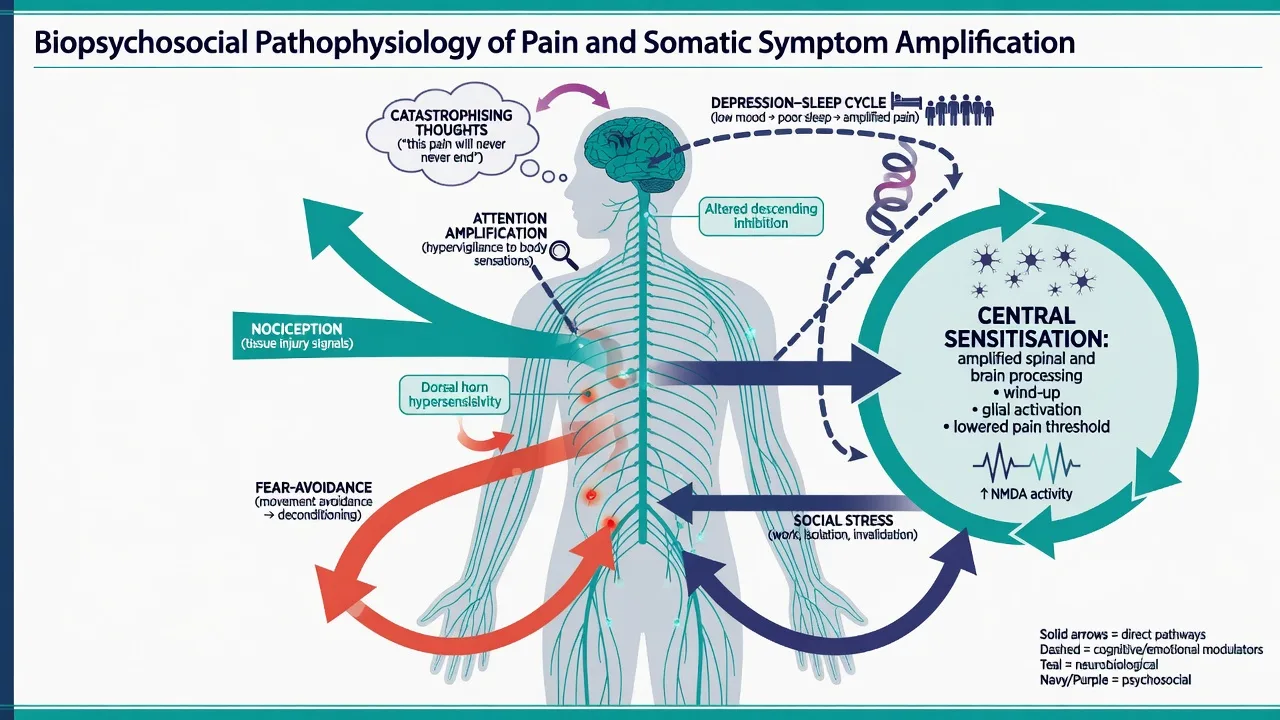
Viva-depth mechanisms without speculative fluff (biopsychosocial amplification, not dualism):[6][11]
- Nociception vs pain vs disability — tissue signals, central processing, and behaviour diverge.[6]
- Attentional amplification and catastrophising — selective attention to bodily signals and catastrophic illness interpretations fuel checking, reassurance-seeking, and avoidance (classic health-anxiety cognitive model underpinning CBT trials).[11][13]
- Fear-avoidance — pain-related fear reduces activity, worsens deconditioning and mood.[6][22]
- Depression–pain monoamine overlap — clinical rationale for SNRI/TCA analgesic trials, not proof of a single lesion.[18][23]
- Iatrogenesis — endless unfocused testing without a positive formulation can reinforce threat beliefs; opioid escalation may worsen outcomes for some chronic non-cancer pain trajectories.[6][20][21]
Clinical presentation (C-L stems)
Typical referrals: “negative” medical admission with persistent multi-system symptoms; chronic back/joint pain with depression and rising opioid doses; post-cancer-scare illness anxiety despite negative work-up; high-utilising primary-care patient with PHQ-15 in the high range; fibromyalgia/IBS with functional collapse; care-avoidant patient refusing colonoscopy despite family history and catastrophic cancer fears.[4][5][24]
MSE focus: affect and anxiety; suicidal ideation; health beliefs (overvalued vs delusional certainty); body checking; substance use; secondary-gain exploration without accusation; capacity only if decisions are contested.[5][24]
Differential diagnosis
Always keep the organic door ajar for red flags or change in pattern (weight loss, night pain, focal neurology, new organ failure signals). Also separate major depression/GAD/panic with somatic prominence, OCD illness obsessions vs IAD, psychotic somatic delusions, FND, and factitious disorder vs malingering (intentionality and incentive type — high threshold language).[1][6]
Assessment
Structure the C-L interview with alliance first (“symptoms are real; the task is to reduce suffering and risk”), symptom and function inventory, PHQ-15 plus depression/anxiety screens, suicide and vulnerability risk, substance/opioid map (dose trajectory, OUD criteria, concurrent sedatives), prior work-ups and what would change management if repeated, and a shared plan with the medical team for re-investigation thresholds and single-clinician coordination where possible.[4][5][6][15][21][24]
Investigations should be hypothesis-driven, not exhaustive. Before TCA/SNRI: consider baseline ECG (age, cardiac risk, drug interactions), metabolic panel as indicated, pregnancy status, and drug–drug interactions (e.g. serotonergic combinations).[17][18]
Acute / emergency issues
Medical red flags, overdose, severe withdrawal, suicidal crisis, and acute abdomen/chest syndromes outrank formulation work. Acute severe pain still deserves humane analgesia; dual diagnosis is not a licence to abandon pain care — it is a licence to use safer multimodal plans and addiction pathways when OUD criteria are met.[21][24]
Definitive management
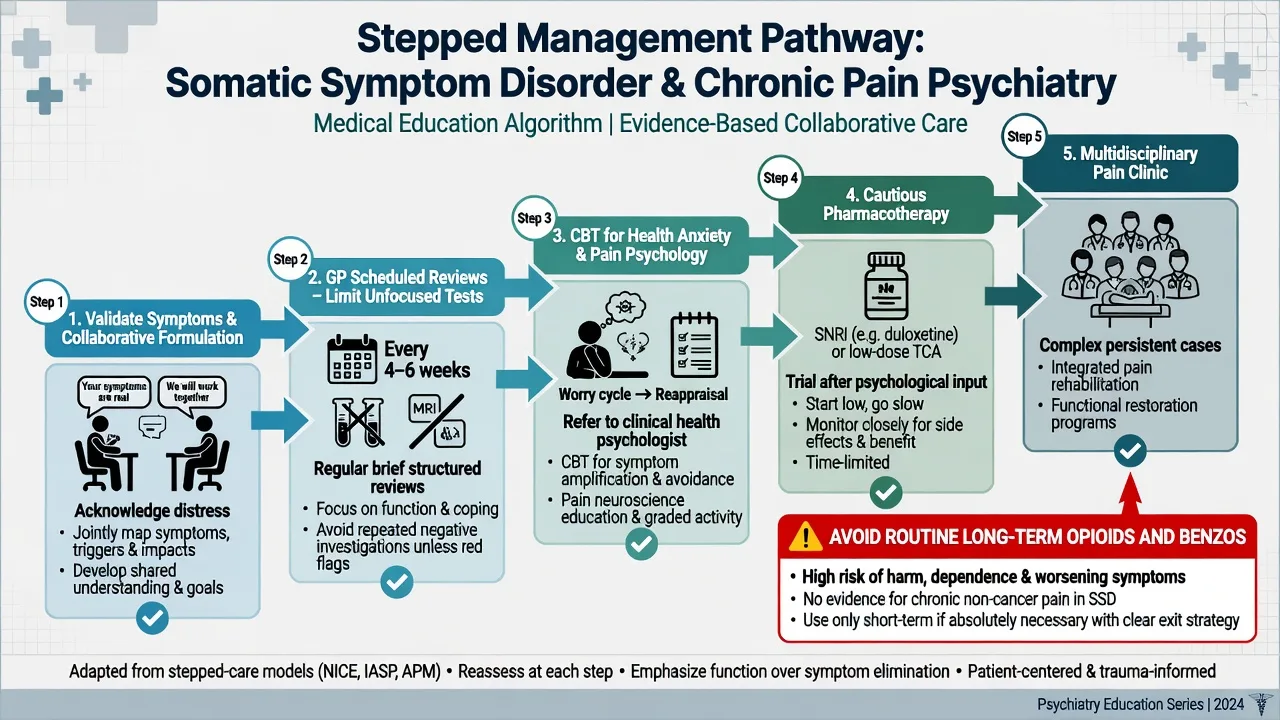
Communication and service model
Henningsen-style principles for functional somatic syndromes: take symptoms seriously; provide a positive, non-dualistic explanation; avoid unnecessary tests and specialist shopping; schedule regular time-limited reviews rather than only crisis visits; set functional goals (walk distance, work return, sleep) rather than total symptom extinction as the only success metric.[6][15]
Psychological therapies
- CBT for hypochondriasis / health anxiety reduces health anxiety versus control (Barsky and Ahern RCT).[11]
- CBT vs paroxetine both outperform waitlist/placebo-type comparators in hypochondriasis; CBT is a durable first-line psychological option (Greeven).[12]
- CHAMP (Tyrer et al.): adapted CBT for health anxiety in medical clinics improved outcomes and was cost-effective in a multicentre RCT — high-yield FRANZCP/MRCPsych citation.[13]
- Fallon et al.: medication and CBT strategies for hypochondriasis in a modern RCT framework — know that combined and monotherapies are studied; do not claim one universal winner without reading the stem.[14]
- Cochrane (van Dessel): non-pharmacological interventions for somatoform disorders / MUPS show modest benefits; CBT-family approaches dominate the evidence base.[8]
- Kleinstäuber meta-analysis: short-term psychotherapy for multiple MUPS has small-to-moderate effects — set realistic expectations.[10]
- Sumathipala: structured CBT adaptable across cultures for MUS versus structured care.[16]
- Chronic pain psychology (Williams Cochrane 2020): psychological therapies (especially CBT) can produce small benefits for pain, disability, and distress; sell function and coping, not miracle cure.[22]
- SCAMP: optimized antidepressant therapy plus pain self-management training improved depression and pain in primary care.[23]
Pharmacotherapy — caution first
Cochrane review of pharmacological interventions for somatoform disorders finds limited, low-certainty signals; do not treat “somatisation” with polypharmacy as if it were an antipsychotic-responsive psychosis.[9]
When medication is used, target comorbid depression/anxiety and selected pain phenotypes (table doses are exam-facing starting spines — confirm local formulary):[9][12][17][18][19]
| Agent | Typical exam-facing use | Practical starting approach | Key cautions |
|---|---|---|---|
| Duloxetine | Diabetic peripheral neuropathic pain, some chronic musculoskeletal/fibromyalgia contexts | Often 30 mg oral daily for 1 week then 60 mg daily (product/local formulary; trial literature centres on 60 mg) | Nausea, sweating, BP, withdrawal, serotonergic interactions; suicide risk discussion in younger patients |
| Amitriptyline | Neuropathic pain (evidence mixed/limited at meta-analytic level — humility required) | Common pain practice 10–25 mg oral at night, titrate slowly (often toward 25–75 mg) as tolerated | Anticholinergic effects, falls, QTc/cardiac risk, overdose lethality |
| SSRI (e.g. sertraline/fluoxetine/paroxetine) | Comorbid depression, anxiety, health anxiety (paroxetine studied in hypochondriasis trials) | Standard antidepressant starts (e.g. sertraline 25–50 mg oral daily) with monitoring | Activation, sexual side effects, interactions; not a universal “anti-somatic” drug |
Goldstein et al. demonstrated duloxetine superiority versus placebo in painful diabetic neuropathy — the classic efficacy signal examiners expect.[19] Lunn Cochrane supports duloxetine for painful neuropathy/fibromyalgia-type indications with realistic effect sizes and adverse-event trade-offs.[18] Moore Cochrane on amitriptyline for neuropathic pain is more cautious than bedside tradition: quality of evidence is limited; still widely used at low night-time doses in pain clinics — state both tradition and evidence humility.[17]
Avoid as default long-term strategy: benzodiazepines for chronic somatic anxiety; high-dose opioids for chronic non-cancer pain without clear functional gain.[20][21]
Opioids and dual diagnosis pointer
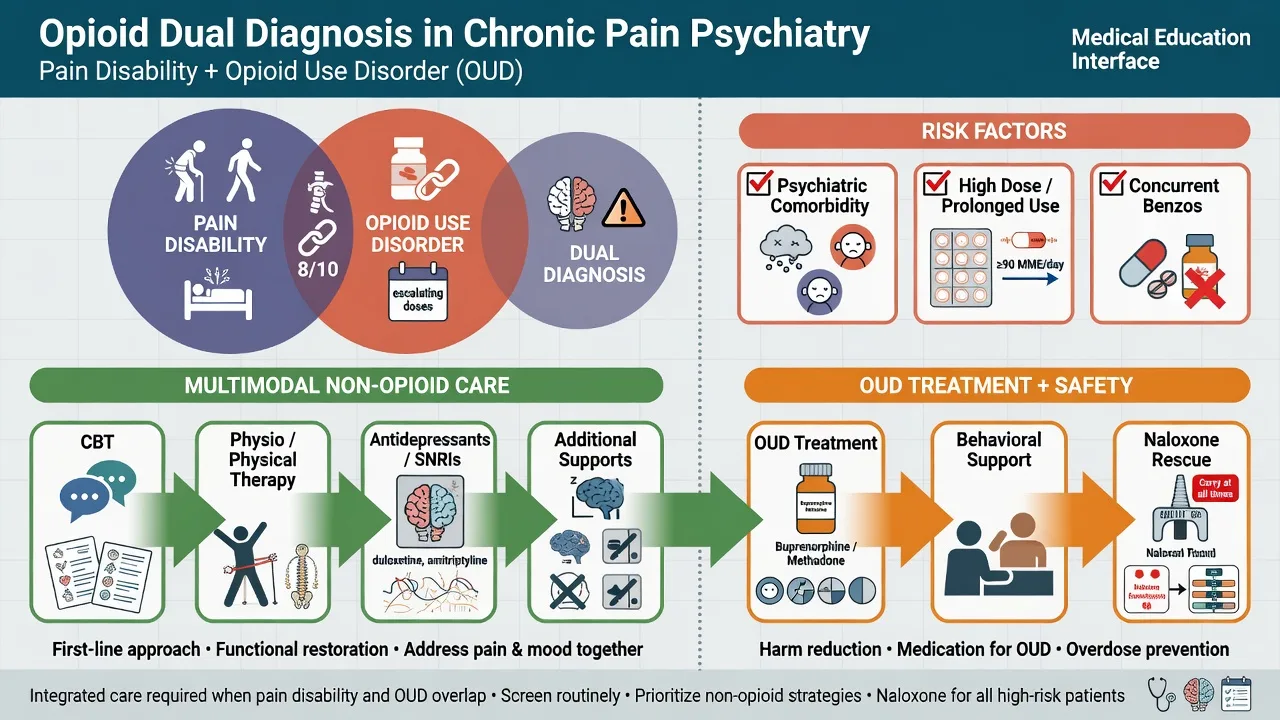
SPACE (Krebs 2018): in chronic back, hip, or knee pain, opioid therapy did not yield superior pain-related function versus optimized non-opioid medication over 12 months, with more adverse medication-related symptoms in the opioid arm — a fellowship pearl against automatic opioid escalation.[20]
CDC 2022 opioid prescribing guidance emphasises maximising non-opioid therapies, careful patient selection, risk mitigation, and avoiding abrupt inappropriate discontinuation myths — use as principles and map to local ANZ guidance rather than memorising US-only dose tables as law.[21]
When opioid use disorder criteria are met (loss of control, craving, continued use despite harm, withdrawal/tolerance in the pathological pattern), manage as dual diagnosis: pain plan + addiction treatment pathway (opioid agonist treatment where indicated, psychosocial care, naloxone, sedative deprescribing). Howe and Sullivan argue psychiatry is the missing pillar of chronic pain systems in the opioid era.[24][21]
Exam dose and monitoring quick card. Duloxetine: 30 mg → 60 mg oral daily is the common trial/clinical titration spine for neuropathic pain; reassess benefit and harms at 2–4 weeks; avoid casual serotonergic stacking.[18][19] Amitriptyline (pain): start low at night (10–25 mg oral), go slow; warn about hangover, dry mouth, urinary retention, falls; cardiac risk stratification in older adults.[17] Opioids: if used at all for chronic non-cancer pain, define functional goals, review frequently, check concurrent benzos, consider urine toxicology/PDMP-type tools where available, plan exit strategy; dual diagnosis changes the pathway.[20][21]
Special populations
Youth: functional symptoms, school avoidance, family reinforcement, developmental formulation, cautious meds. Older adults: multi-morbidity — do not label every symptom cluster as SSD; anticholinergic TCA risk is higher. Pregnancy/lactation: prioritise psychological care; any antidepressant needs individualised obstetric-psychiatry risk discussion. Cultural formulation: idioms of distress may present as bodily complaint; avoid over-pathologising culturally coherent expression while still treating disability and depression.[6][16][17]
Prognosis and disposition
Course is often chronic and fluctuating. Best outcomes track engagement, treated mood/anxiety, reduced iatrogenic harm, and improved function rather than zero symptoms. Disposition is usually shared care: GP continuity, psychology/CBT, psychiatry for complex comorbidity or risk, and multidisciplinary pain services when available.[6][10][22]
Regional notes
ANZ (FRANZCP): Frame care under collaborative C-L and primary-care partnership; use TGA/local formulary for duloxetine and TCA dosing; opioid stewardship aligns with national quality use of medicines principles — CDC 2022 is comparative evidence, not Australian statute. UK (MRCPsych): NICE chronic pain and depression pathways are frequent CASC/MEQ anchors; CHAMP-style health-anxiety CBT in medical settings is high yield. US (ABPN): DSM-5-TR SSD/IAD wording and CDC opioid guidance dominate; document OUD criteria carefully. MD/DNB/NEET-SS: Expect definitions, PHQ-15, CBT principles, and named analgesic antidepressants with cautions.[4][13][21]
Exam pearls
Classic stems
- High-utilising patient with multi-system symptoms and normal work-ups → SSD formulation + CBT + scheduled GP care, not another unfocused scan by default.[8][15]
- Post-negative cancer work-up with body checking → IAD / health anxiety CBT (Barsky, Tyrer).[11][13]
- Chronic OA back pain, depression, rising oxycodone → treat depression, self-management, non-opioid optimisation, SPACE-informed caution, screen OUD.[20][23][24]
Evidence snapshot
Landmark names to deploy: Dimsdale (SSD nosology), Kroenke (PHQ-15; SCAMP), Henningsen (FSS management), Fink (bodily distress), Barsky, Greeven, Tyrer CHAMP, Fallon, van Dessel Cochrane, Kleinstäuber, Williams Cochrane, Lunn duloxetine, Moore amitriptyline, SPACE, CDC 2022, Howe/Sullivan (missing psychiatric services in pain).[1][4][6][11][13][20][22]
References
- [1]Dimsdale JE, Creed F, Escobar J, et al. Somatic symptom disorder: an important change in DSM J Psychosom Res, 2013.PMID 23972410
- [2]Dimsdale JE, Levenson J What's next for somatic symptom disorder? Am J Psychiatry, 2013.PMID 24306336
- [3]Mayou R Is the DSM-5 chapter on somatic symptom disorder any better than DSM-IV somatoform disorder? Br J Psychiatry, 2014.PMID 25029686
- [4]Kroenke K, Spitzer RL, Williams JB The PHQ-15: validity of a new measure for evaluating the severity of somatic symptoms Psychosom Med, 2002.PMID 11914441
- [5]Kroenke K, Spitzer RL, Williams JB, et al. The Patient Health Questionnaire Somatic, Anxiety, and Depressive Symptom Scales: a systematic review Gen Hosp Psychiatry, 2010.PMID 20633738
- [6]Henningsen P, Zipfel S, Herzog W Management of functional somatic syndromes Lancet, 2007.PMID 17368156
- [7]Fink P, Toft T, Hansen MS, et al. Symptoms and syndromes of bodily distress: an exploratory study of 978 internal medical, neurological, and primary care patients Psychosom Med, 2007.PMID 17244846
- [8]van Dessel N, den Boeft M, van der Wouden JC, et al. Non-pharmacological interventions for somatoform disorders and medically unexplained physical symptoms (MUPS) in adults Cochrane Database Syst Rev, 2014.PMID 25362239
- [9]Kleinstäuber M, Witthöft M, Steffanowski A, et al. Pharmacological interventions for somatoform disorders in adults Cochrane Database Syst Rev, 2014.PMID 25379990
- [10]Kleinstäuber M, Witthöft M, Hiller W Efficacy of short-term psychotherapy for multiple medically unexplained physical symptoms: a meta-analysis Clin Psychol Rev, 2011.PMID 20920834
- [11]Barsky AJ, Ahern DK Cognitive behavior therapy for hypochondriasis: a randomized controlled trial JAMA, 2004.PMID 15039413
- [12]Greeven A, van Balkom AJ, Visser S, et al. Cognitive behavior therapy and paroxetine in the treatment of hypochondriasis: a randomized controlled trial Am J Psychiatry, 2007.PMID 17202549
- [13]Tyrer P, Cooper S, Salkovskis P, et al. Clinical and cost-effectiveness of cognitive behaviour therapy for health anxiety in medical patients: a multicentre randomised controlled trial Lancet, 2014.PMID 24139977
- [14]Fallon BA, Ahern DK, Pavlicova M, et al. A Randomized Controlled Trial of Medication and Cognitive-Behavioral Therapy for Hypochondriasis Am J Psychiatry, 2017.PMID 28659038
- [15]Barsky AJ, Ahern DK, Bauer MR, et al. A randomized trial of treatments for high-utilizing somatizing patients J Gen Intern Med, 2013.PMID 23494213
- [16]Sumathipala A, Siribaddana S, Abeysingha MR, et al. Cognitive-behavioural therapy v. structured care for medically unexplained symptoms: randomised controlled trial Br J Psychiatry, 2008.PMID 18700219
- [17]Moore RA, Derry S, Aldington D, et al. Amitriptyline for neuropathic pain in adults Cochrane Database Syst Rev, 2015.PMID 26146793
- [18]Lunn MP, Hughes RA, Wiffen PJ Duloxetine for treating painful neuropathy, chronic pain or fibromyalgia Cochrane Database Syst Rev, 2014.PMID 24385423
- [19]Goldstein DJ, Lu Y, Detke MJ, et al. Duloxetine vs. placebo in patients with painful diabetic neuropathy Pain, 2005.PMID 15927394
- [20]Krebs EE, Gravely A, Nugent S, et al. Effect of Opioid vs Nonopioid Medications on Pain-Related Function in Patients With Chronic Back Pain or Hip or Knee Osteoarthritis Pain: The SPACE Randomized Clinical Trial JAMA, 2018.PMID 29509867
- [21]Dowell D, Ragan KR, Jones CM, et al. CDC Clinical Practice Guideline for Prescribing Opioids for Pain - United States, 2022 MMWR Recomm Rep, 2022.PMID 36327391
- [22]Williams ACC, Fisher E, Hearn L, et al. Psychological therapies for the management of chronic pain (excluding headache) in adults Cochrane Database Syst Rev, 2020.PMID 32794606
- [23]Kroenke K, Bair MJ, Damush TM, et al. Optimized antidepressant therapy and pain self-management in primary care patients with depression and musculoskeletal pain: a randomized controlled trial JAMA, 2009.PMID 19470987
- [24]Howe CQ, Sullivan MD The missing 'P' in pain management: how the current opioid epidemic highlights the need for psychiatric services in chronic pain care Gen Hosp Psychiatry, 2014.PMID 24211157