Psych · Consultation-liaison psychiatry
Palliative care psychiatry
Also known as Psychiatry in palliative care · End-of-life psychiatry · Hospice psychiatry · Terminal illness psychiatry · Palliative psychiatry
Exam-exhaustive fellowship topic on palliative care psychiatry for consultation-liaison practice — syndrome map (adjustment, demoralisation, major depression, anxiety, delirium, grief), desire for hastened death, dignity therapy and meaning-centred/CALM psychotherapy, Agar limits on antipsychotics in palliative delirium, antidepressant evidence in palliative care, early palliative care trials (Temel, Zimmermann, Bakitas), capacity and goals-of-care, family distress, and VAD-adjacent assessment. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Palliative care psychiatry is a high-yield medical psychiatry domain. Examiners test whether you can hold concurrent diagnoses (delirium plus depression), name landmark trials (Agar, Temel, Chochinov, Breitbart, Rodin), dose carefully in frail bodies, and navigate desire for hastened death without either moralising or missing treatable drivers.[2][3][6][9]
Overview and definition
Palliative care psychiatry is consultation-liaison psychiatry for people with progressive or life-limiting illness and their families — from concurrent early palliative care through terminal care and into carer bereavement. It is not limited to the last 72 hours. Psychiatry's jobs are syndrome diagnosis, risk (including desire for death), capacity and goals-of-care support, careful psychopharmacology, structured psychotherapy when feasible, and liaison with palliative medicine, nursing, psychology, social work, and spiritual care.[3][4][7]
Early palliative care (Temel; Zimmermann; Bakitas ENABLE II) frames supportive care as concurrent with disease-directed treatment, improving quality of life and mood outcomes rather than signalling abandonment of hope.[3][4][5]
Classification and syndrome map

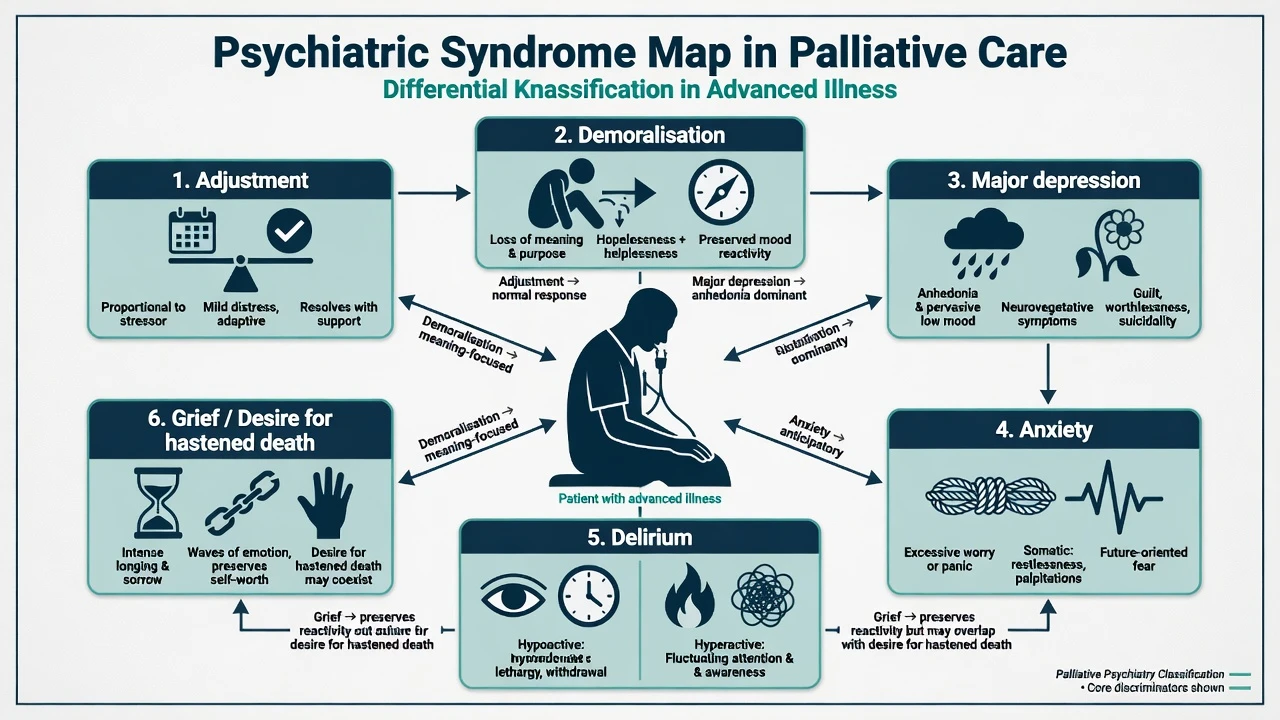
| Syndrome | Core features near end of life | Discriminators |
|---|---|---|
| Adjustment | Emotional/behavioural symptoms tied to prognostic news, functional loss, place-of-care change | Some preserved pleasure windows; tracks stressors; less pervasive anhedonia/guilt than MDD |
| Demoralisation | Pointlessness, trapped feeling, subjective incompetence, loss of meaning | Meaning collapse may dominate over classic melancholic biology; may coexist with MDD |
| Major depression | Pervasive low mood/anhedonia, hopelessness, worthlessness, suicidal ideation for at least 2 weeks | Do not rely only on fatigue/anorexia; weight affective and cognitive anchors |
| Anxiety | Worry, panic about dying, dyspnoea-linked fear, avoidance of discussions | Separate from hypoxia and uncontrolled symptoms; may need both medical and psychological care |
| Delirium | Acute fluctuating inattention and awareness | CAM-positive; often hypoactive; medical precipitants |
| Grief / anticipatory grief | Sadness, yearning, waves of emotion with preserved self-worth | Waves vs pervasive anhedonia; still connected to loved ones and meaning |
| Desire for hastened death (DHD) | Wish that death come sooner; spectrum from passive to active request | Multifactorial — not a single diagnosis; always screen depression and delirium |
DSM-5-TR and ICD-11 both allow mood disorders in medical illness. Examiners care less about coding pedantry and more about not missing delirium, not under-treating MDD, and not pathologising all dying-related sadness.[1][10][13]
Epidemiology and risk
Interview-based meta-analysis shows substantial prevalence of depression, anxiety, and adjustment disorder in palliative-care settings.[1] Desire for death among the terminally ill associates closely with clinical depression and can fluctuate over time.[8] In terminally ill cancer inpatients, depression and hopelessness independently predict desire for hastened death, with smaller contributions from social support and physical function.[9]
Pathophysiology and mechanisms
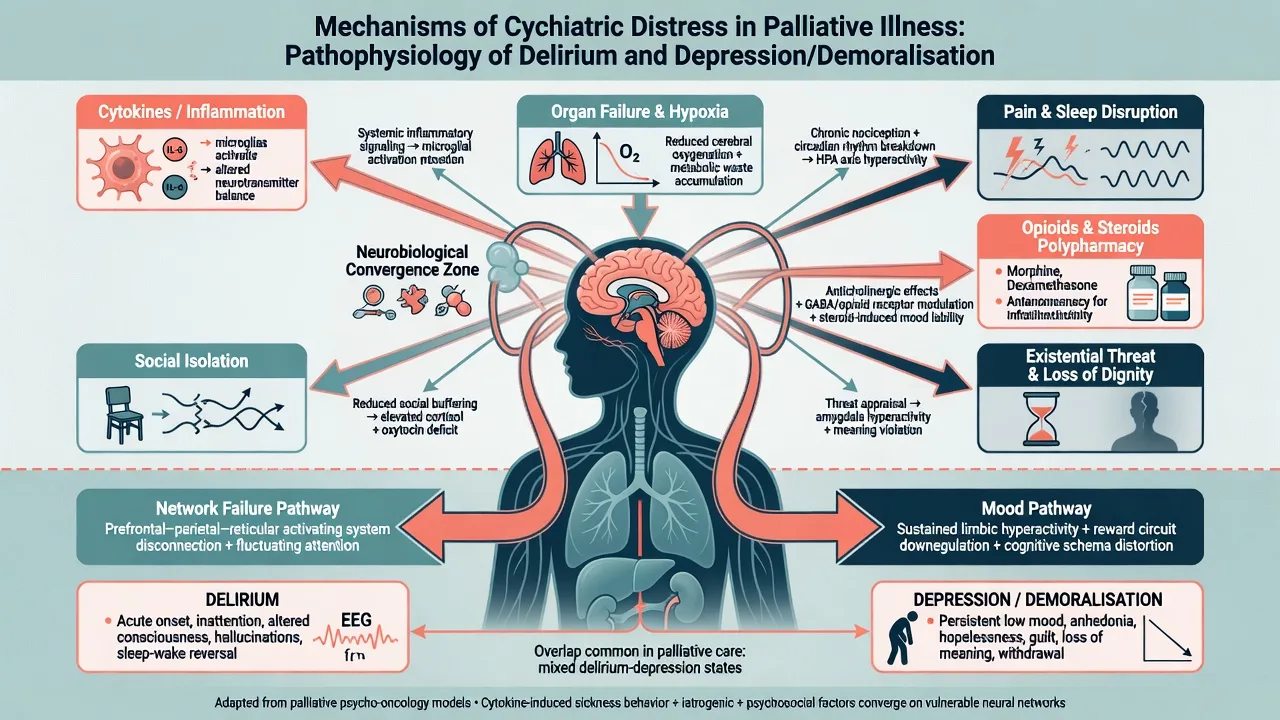
Mechanisms are multifactorial: inflammatory signalling, organ failure, hypoxia, pain, sleep disruption, CNS disease, polypharmacy (opioids, corticosteroids, anticholinergics, benzodiazepines), and existential threat with role and dignity losses.[2][7][10]
Dignity models (Chochinov) organise suffering around illness-related concerns, dignity-conserving repertoire, and social dignity inventory — a practical scaffold for assessment and intervention beyond symptom checklists.[6][7]
Demoralisation conceptualises subjective incompetence and meaning collapse as a distinct but overlapping pathway that guides meaning-centred therapies rather than antidepressants alone.[10][11]
Clinical presentation
Tempo. Link symptoms to illness milestones: new prognostic awareness, transition off disease-modifying therapy, place-of-care change, last weeks, and imminent dying. Carer presentations often peak around transitions and after death.[3][7]
Somatic overlap. Fatigue, anorexia, and sleep change are nearly universal in advanced disease. Lean on pervasive anhedonia, hopelessness, worthlessness out of proportion, guilt, suicidal ideation, and diurnal mood variation, plus collateral functional collapse beyond medical limitation.[12][13]
Demoralisation language. "There is no point," "I am a burden," "I am trapped," with possible retained reactivity to family presence — clinically important for therapy choice.[10][11]
Delirium. Hypoactive forms are mislabelled as depression, "withdrawal," or "natural dying." Test attention; use CAM logic.[2][17]
DHD spectrum. Passive wish to die; intermittent request for hastened death; active suicidal plan; formal voluntary assisted dying (VAD) enquiry where lawful — each needs different risk intensity and documentation.[8][9]
Differential diagnosis — discriminators
- Pervasive anhedonia/hopelessness
- Worthlessness and guilt
- ≥2 weeks
- Active treatment pathway
- May need antidepressant + therapy
- Meaning and coping collapse
- Tied to illness milestones
- Some reactivity possible
- Dignity/meaning therapies fit
- Watch evolution into MDD
- Acute fluctuating inattention
- Altered awareness
- Medical precipitants
- Capacity often impaired
- Fix causes; drugs secondary
Always consider pain, dyspnoea, hypercalcaemia, hyponatraemia, hypoxia, infection, hepatic/renal failure, CNS disease, opioid toxicity, alcohol/benzodiazepine withdrawal, constipation/urinary retention, and steroid effects before locking a purely psychiatric label.[2][13][17]
Assessment
- Illness context: stage, prognosis communication, goals of care, recent changes, place of care.
- Symptom burden: pain, dyspnoea, nausea, sleep, constipation, retention.
- Drugs: opioids, benzodiazepines, corticosteroids, anticholinergics, recent starts/stops.
- Psychiatric history: prior MDD/bipolar/psychosis, self-harm, substance use.
- MSE: affect, anhedonia, hopelessness, psychosis, attention if any confusion.
- Risk: suicide and DHD (passive vs plan/intent/means); carer risk.
- Capacity: decision-specific for treatment limitation, place of care, and VAD-adjacent decisions where lawful.
- Tools: CAM when delirium possible; PHQ-9 for depression severity tracking (limitations with somatic items); dignity-related enquiry; collateral from family and palliative team.[2][8][9][17]
Investigations
Directed and goal-sensitive: vitals, glucose, FBC, U&E, calcium, LFTs, infection work-up when results could change comfort or reversible confusion. Imaging only if management would change. ECG when considering QTc-risk psychotropics. Medication reconciliation is part of the investigation. Avoid investigations that only prolong suffering without altering the plan.[2][13][17]
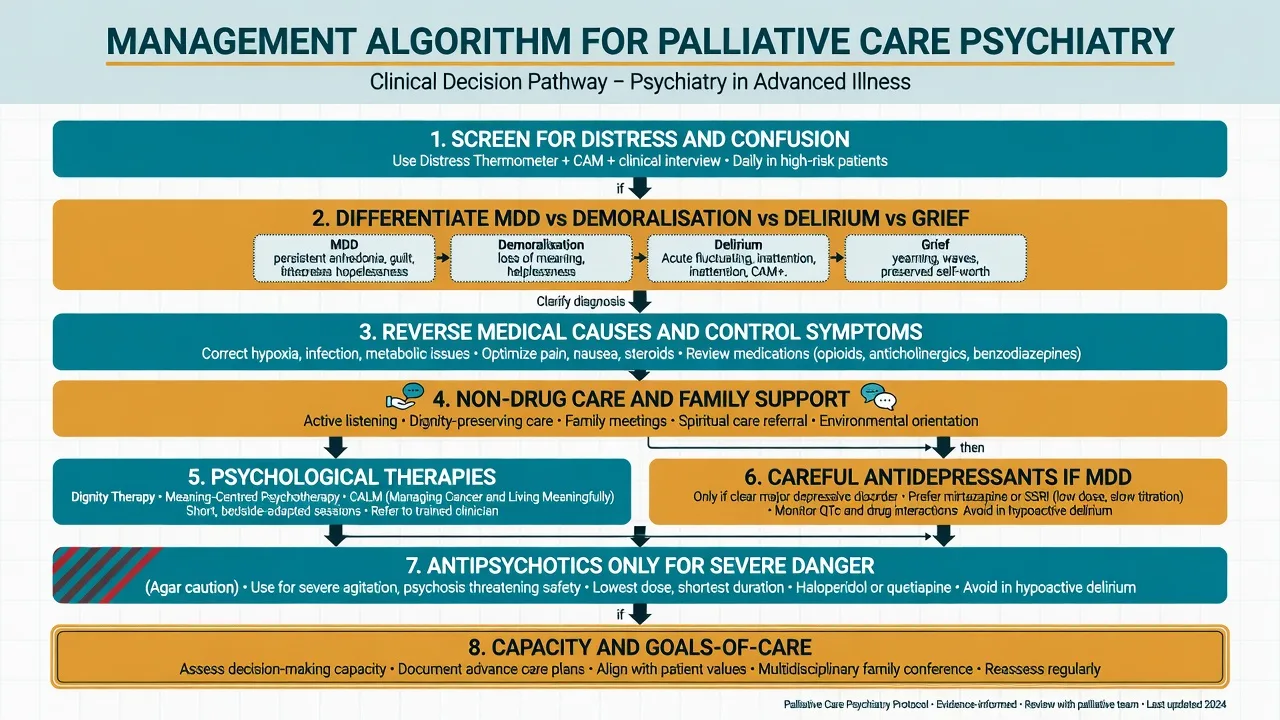
Acute management and red flags
For severe behavioural disturbance with danger (violence, line-pulling, severe distress): environmental safety, 1:1 presence, treat pain and metabolic insults, family presence if calming, and only then consider short-term low-dose antipsychotic with daily review. For alcohol/benzodiazepine withdrawal, use benzodiazepine pathways plus thiamine — not antipsychotic monotherapy.[2][17]
Active suicidality requires safety planning, means restriction, urgent psychiatry, and local mental health law only when criteria are met — statutes are jurisdiction-specific.[8][9]
Definitive management
Partnership with palliative medicine and early integration
Symptom control is psychiatric treatment. Uncontrolled pain, dyspnoea, and insomnia drive mood, delirium risk, and DHD. Early concurrent palliative care improved quality of life and mood in metastatic NSCLC (Temel), with broader advanced-cancer signals from Zimmermann and ENABLE II (Bakitas).[3][4][5]
Psychological therapies (name them)
Dignity therapy is a brief, individualised intervention creating a legacy document; the multicentre RCT found patients reported improved end-of-life experience and dignity-related outcomes versus standard care, even when primary distress endpoints were mixed — examiners expect the name and the model, not a claim of universal mood cure.[6][7]
Meaning-centered psychotherapy (group and individual forms) improves spiritual well-being and meaning in advanced cancer trials.[14][15]
CALM (Managing Cancer and Living Meaningfully) is a brief manualised therapy for advanced cancer that reduces depressive symptoms and prepares for end-of-life in RCT evidence.[16]
Supportive counselling, problem-solving, family meetings, and spiritual care remain foundational. Match therapy intensity to energy, prognosis, and preference.[6][14][16]
Antidepressants
Meta-analysis supports antidepressants for depression in palliative care versus placebo; European palliative cancer depression guidelines endorse structured assessment and treatment rather than therapeutic nihilism.[12][13] Cancer-specific Cochrane synthesis similarly supports antidepressant treatment with usual caveats of trial quality.[18]
Practical fellowship starts (individualise; start low in frail/older adults; check interactions and prognosis window):[12][13][18]
| Agent | Typical start (adult palliative) | Notes |
|---|---|---|
| Sertraline | 25–50 mg oral daily; titrate toward response | Often preferred; watch nausea, hyponatraemia |
| Escitalopram | 5–10 mg oral daily | Simpler kinetics; QTc caution at higher doses |
| Mirtazapine | 7.5–15 mg oral at night | Sleep and appetite may help; sedation |
| Trial window | Reassess 1–2 weeks early | If prognosis is days, prioritise non-drug care and symptom control |
Do not withhold antidepressants solely because illness is advanced if MDD criteria are met and a meaningful trial window exists. Conversely, do not expect full response in the last days of life — goals shift to comfort and presence.[12][13]
Delirium in palliative care
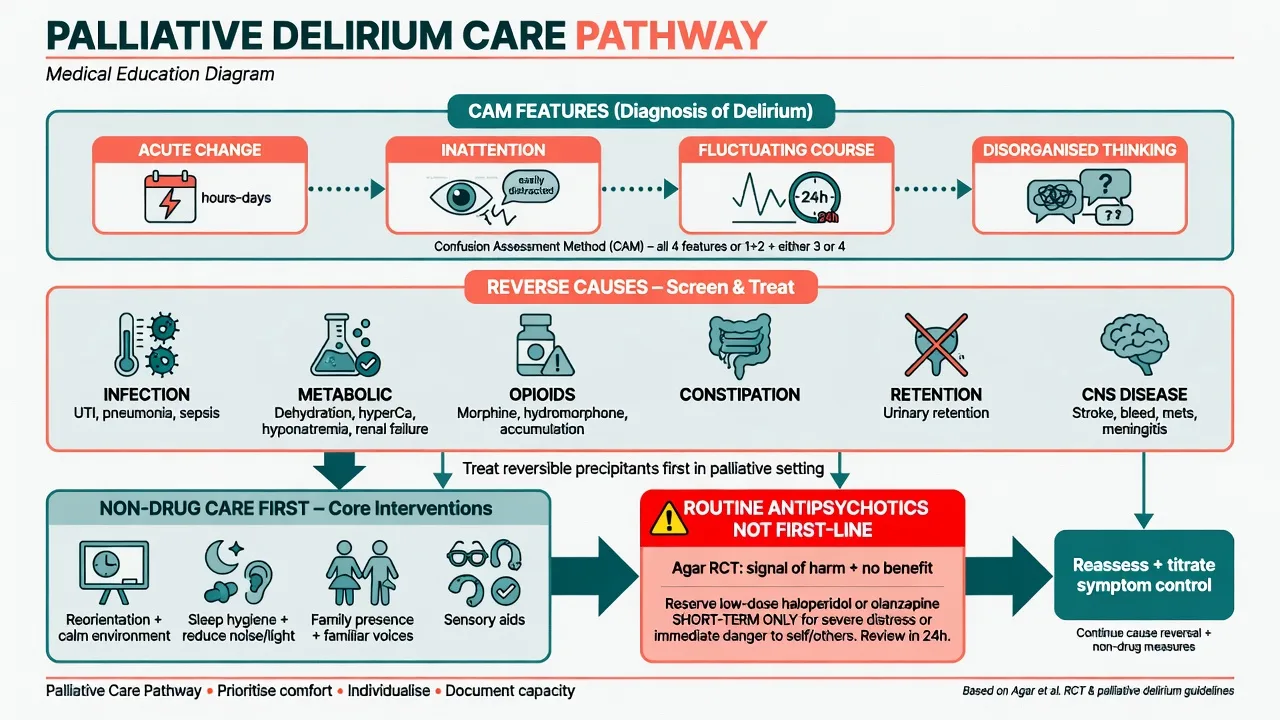
Apply CAM: acute/fluctuating course + inattention + (disorganised thinking or altered consciousness).[17] Reverse infection, metabolic failure, CNS disease, constipation/retention, and deliriogenic drugs when consistent with goals.
Agar 2017: in palliative-care patients with delirium symptoms, risperidone and haloperidol produced worse symptom scores than placebo and more extrapyramidal effects. This kills the "haloperidol QID for terminal confusion" reflex. Reserve antipsychotics for severe distress or danger after non-drug measures, use the lowest effective short-term dose, and reassess daily with goals of care explicit.[2]
Example cautious short-term ranges used in CL practice for severe danger only (not scheduled default; not a substitute for local formulary): haloperidol 0.5–1 mg oral or appropriate parenteral pathway, or olanzapine 2.5–5 mg oral, with ECG/EPS monitoring where feasible, stop early.[2]
Desire for hastened death, capacity, and VAD interface
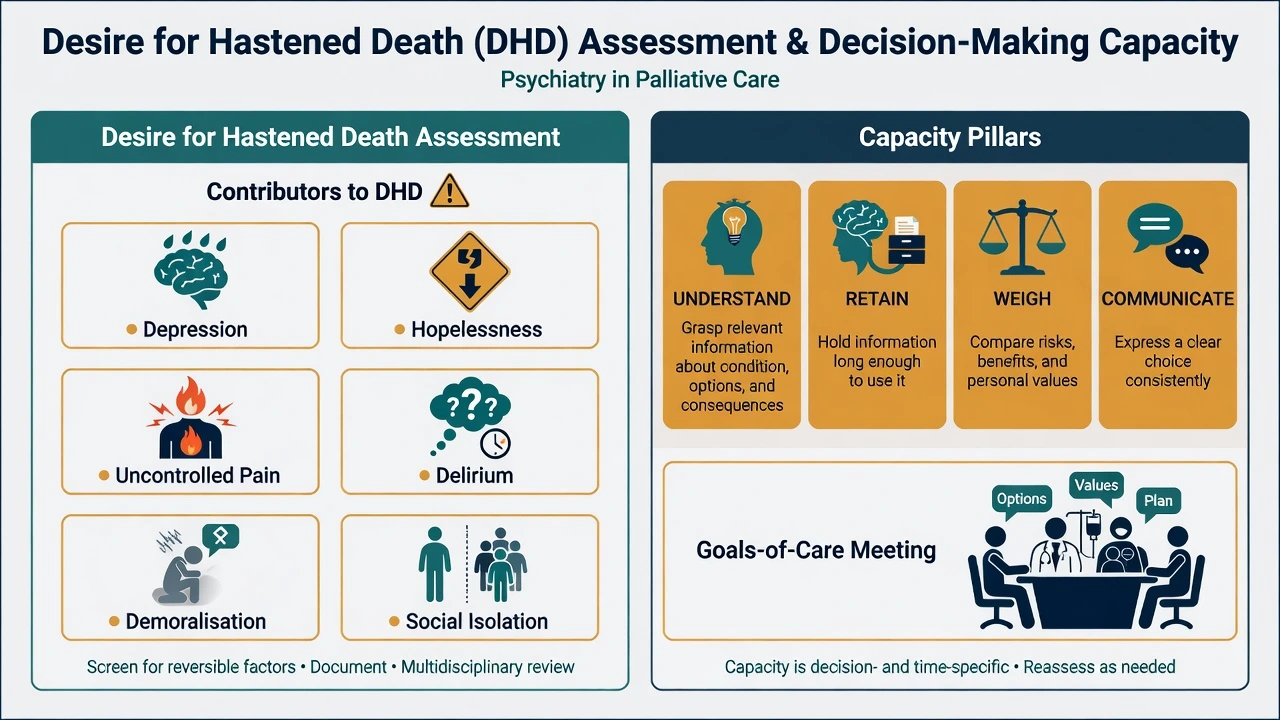
Screen for depression, hopelessness, demoralisation, uncontrolled symptoms, delirium, coercion, and social abandonment before framing DHD as purely autonomy-driven philosophy.[8][9][10] Treat reversible drivers and reassess. Document carefully.
Capacity is decision-specific and time-specific. Delirium and severe depression with nihilistic distortion commonly impair weighing for complex end-of-life decisions — treat, reassess in a lucid window when possible, and use substitute decision-making under local law if incapacitous. Do not invent foreign statute numbers. Where VAD is lawful, psychiatry's role is assessment of capacity, treatable mental illness, coercion, and symptom burden — not moral theatre.[2][8][9][17]
Special populations
Older adults need lower psychotropic starts, delirium vigilance, and sensory optimisation. AYA work emphasises identity, unfinished life tasks, and family systems. Non-cancer trajectories (heart failure, COPD, renal disease, MND/ALS) share DHD and demoralisation themes with longer intermittent crises. Intellectual disability requires supported decision-making and behaviour-as-pain/distress literacy. Cultural and Indigenous care needs interpreters, family-centred decision-making, and spiritual care without ethnocentric capacity shortcuts.[1][7][10]
Evidence and regional notes
ANZ / FRANZCP. CL psychiatry with palliative medicine is core liaison work. Cite Agar humility on antipsychotics, Chochinov dignity model, and demoralisation (Clarke and Kissane). VAD frameworks are jurisdiction-specific (state/territory) — know principles, not invented sections.[2][6][10]
UK / MRCPsych. NICE end-of-life and supportive care themes emphasise holistic needs assessment; CASC stations often test communication about dying, depression in medical illness, and family distress.[12][13]
US / ABPN. Early palliative care trial names (Temel, ENABLE), dignity therapy, and DHD literature are high yield; local assisted-dying laws vary by state.[3][5][6][9]
MD/DNB / NEET-SS. Expect viva on delirium vs depression, demoralisation, antidepressant use when prognosis is limited, and capacity at end of life.[2][10][12][17]
Landmark names to drop cleanly: Mitchell (prevalence), Agar (palliative delirium antipsychotics), Temel / Zimmermann / Bakitas (early palliative care), Chochinov (desire for death; dignity-conserving care; dignity therapy), Breitbart (DHD; meaning-centred psychotherapy), Rodin (CALM), Rayner/Hotopf (antidepressants and guidelines), Clarke and Kissane (demoralisation), Inouye (CAM).[1][2][3][6][8][9][10][12][16][17]
Prognosis and disposition
Depression and demoralisation can improve with integrated care even in advanced disease; early palliative care improves quality of life and mood outcomes in landmark trials.[3][4][5][12] Delirium outcomes track cause reversibility, frailty, and proximity to death — near death, delirium may be irreversible and the goal is comfort and family support.[2][17] Dignity therapy can enrich end-of-life experience even when global distress scores move modestly.[6]
Disposition plans should name joint palliative–psychiatry follow-up, crisis contacts, place-of-care preferences, family education (especially about delirium), spiritual care, and bereavement pathways for carers.[3][6][7]
Exam pearls
PALLIATE (bedside scaffold)
Fellowship viva one-liners: Early palliative care is concurrent, not surrender; Agar undercuts routine neuroleptics in dying patients with delirium; DHD is a signal to treat depression, hopelessness, and symptoms; Dignity therapy and CALM are named interventions, not vague support.[2][3][6][9][16]
References
- [1]Mitchell AJ, Chan M, Bhatti H, et al. Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: a meta-analysis of 94 interview-based studies Lancet Oncol, 2011.PMID 21251875
- [2]Agar MR, Lawlor PG, Quinn S, et al. Efficacy of Oral Risperidone, Haloperidol, or Placebo for Symptoms of Delirium Among Patients in Palliative Care: A Randomized Clinical Trial JAMA Intern Med, 2017.PMID 27918778
- [3]Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer N Engl J Med, 2010.PMID 20818875
- [4]Zimmermann C, Swami N, Krzyzanowska M, et al. Early palliative care for patients with advanced cancer: a cluster-randomised controlled trial Lancet, 2014.PMID 24559581
- [5]Bakitas M, Lyons KD, Hegel MT, et al. Effects of a palliative care intervention on clinical outcomes in patients with advanced cancer: the Project ENABLE II randomized controlled trial JAMA, 2009.PMID 19690306
- [6]Chochinov HM, Kristjanson LJ, Breitbart W, et al. Effect of dignity therapy on distress and end-of-life experience in terminally ill patients: a randomised controlled trial Lancet Oncol, 2011.PMID 21741309
- [7]Chochinov HM Dignity-conserving care--a new model for palliative care: helping the patient feel valued JAMA, 2002.PMID 11980525
- [8]Chochinov HM, Wilson KG, Enns M, et al. Desire for death in the terminally ill Am J Psychiatry, 1995.PMID 7625468
- [9]Breitbart W, Rosenfeld B, Pessin H, et al. Depression, hopelessness, and desire for hastened death in terminally ill patients with cancer JAMA, 2000.PMID 11147988
- [10]Clarke DM, Kissane DW Demoralization: its phenomenology and importance Aust N Z J Psychiatry, 2002.PMID 12406115
- [11]Robinson S, Kissane DW, Brooker J, et al. A systematic review of the demoralization syndrome in individuals with progressive disease and cancer: a decade of research J Pain Symptom Manage, 2015.PMID 25131888
- [12]Rayner L, Price A, Evans A, et al. Antidepressants for the treatment of depression in palliative care: systematic review and meta-analysis Palliat Med, 2011.PMID 20935027
- [13]Rayner L, Price A, Hotopf M, et al. The development of evidence-based European guidelines on the management of depression in palliative cancer care Eur J Cancer, 2011.PMID 21211961
- [14]Breitbart W, Rosenfeld B, Pessin H, et al. Meaning-centered group psychotherapy: an effective intervention for improving psychological well-being in patients with advanced cancer J Clin Oncol, 2015.PMID 25646186
- [15]Breitbart W, Poppito S, Rosenfeld B, et al. Pilot randomized controlled trial of individual meaning-centered psychotherapy for patients with advanced cancer J Clin Oncol, 2012.PMID 22370330
- [16]Rodin G, Lo C, Rydall A, et al. Managing Cancer and Living Meaningfully (CALM): A Randomized Controlled Trial of a Psychological Intervention for Patients With Advanced Cancer J Clin Oncol, 2018.PMID 29958037
- [17]Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the confusion assessment method. A new method for detection of delirium Ann Intern Med, 1990.PMID 2240918
- [18]Ostuzzi G, Matcham F, Dauchy S, et al. Antidepressants for the treatment of depression in people with cancer Cochrane Database Syst Rev, 2018.PMID 29683474