Psych · Consultation-liaison psychiatry
Perinatal psychiatry in the general hospital
Also known as Obstetric psychiatry liaison · Maternity ward psychiatry · Perinatal consultation-liaison psychiatry · Hospital perinatal mental health · Puerperal psychiatry on the ward
Exam-exhaustive fellowship topic on perinatal psychiatry as general-hospital consultation-liaison work — maternity-ward presentations, postpartum psychosis emergency pathway, medical mimics, EPDS screening limits, mother-infant risk, capacity for obstetric decisions, pregnancy and lactation prescribing, lithium peri-delivery, ECT, mother-baby unit disposition, and multi-board guideline framing. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
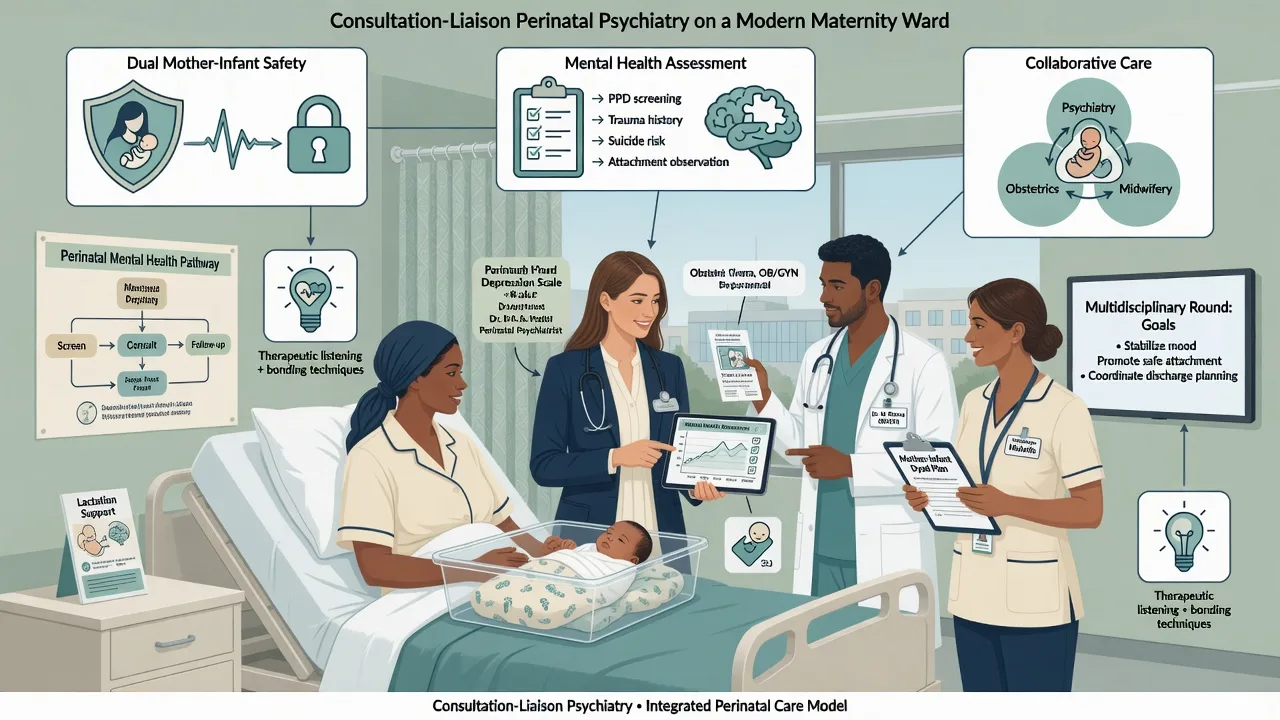
Perinatal mental health is examinable as hospital liaison, not only community PMAD clinics. On maternity and obstetric high-dependency units, the registrar must hold concurrent medical differentials, same-day psychosis pathways, infant safeguarding, and reproductive psychopharmacology while coordinating midwifery, obstetrics, neonatology, and social work.[7][8][18]
Overview and definition
Perinatal psychiatry in the general hospital is consultation-liaison psychiatry for people who are pregnant, in labour, or within the postnatal year (service windows vary) while admitted under obstetric or medical teams. Core tasks are syndrome diagnosis, dual-risk assessment (mother and infant), medical exclusion of organic confusion, capacity for obstetric and psychiatric decisions, careful psychopharmacology, emergency containment of postpartum psychosis, and disposition planning including mother-baby units where available.[5][7][16][18]
DSM-5-TR uses the mood episode specifier with peripartum onset when onset is during pregnancy or within four weeks after delivery. Many maternity pathways still use a broader postnatal year for service access — state which frame you are using in exam answers.[3][7]
Classification and hospital syndrome map
| Syndrome | Typical ward tempo | Discriminators for CL |
|---|---|---|
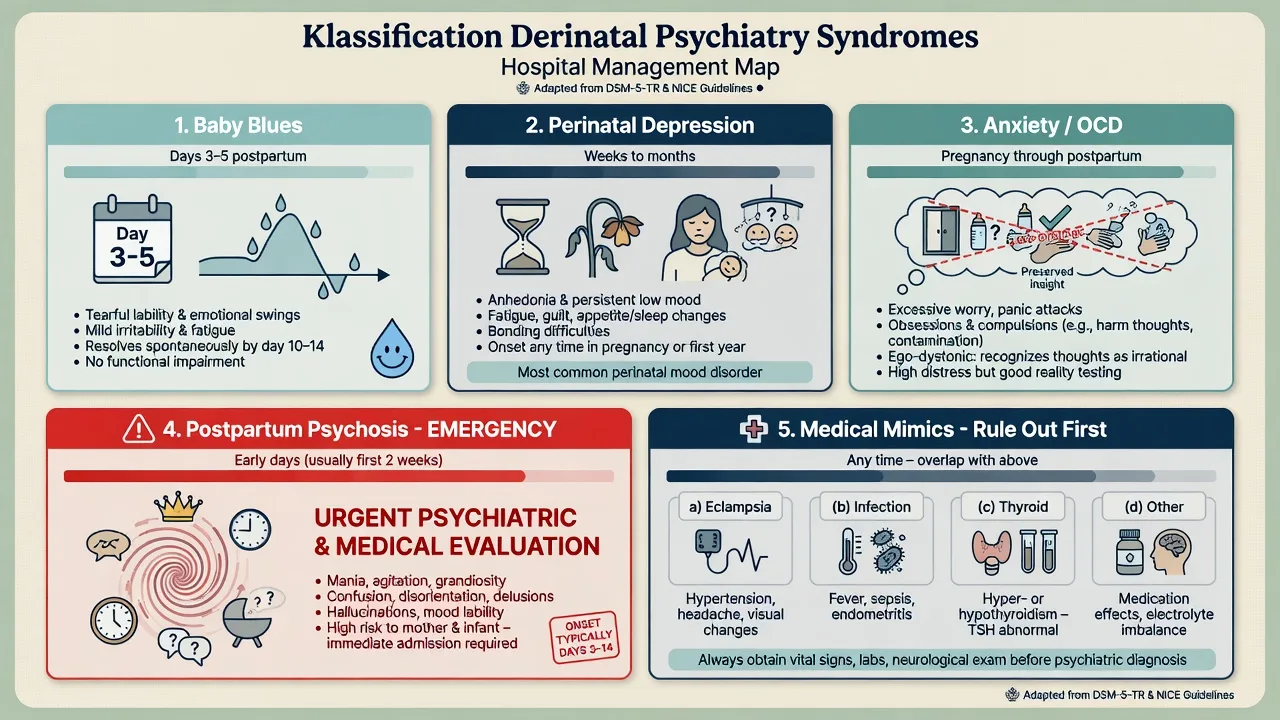
| Baby blues | Days 3–5 peak | Tearfulness, lability; function largely preserved; self-limiting |
| Perinatal depression | Antenatal or weeks–months postnatal | Pervasive anhedonia, guilt, hopelessness, impaired care |
| Anxiety / panic / tokophobia | Any trimester or after traumatic birth | Avoidance of care, panic, fear of birth/CS without psychosis |
| Perinatal OCD | Pregnancy or postnatal | Ego-dystonic infant-harm images; insight preserved; checking |
| Postpartum psychosis | Usually first 2 weeks, often days 1–7 | Rapid mania/mixed/psychosis, confusion, poor sleep without fatigue |
| Organic / medical | Linked to fever, BP, steroids, toxins | Fluctuating inattention, focal neurology, systemic signs |
Postpartum psychosis (PPP) is a clinical emergency syndrome, not a single DSM-5-TR code. It spans mania, mixed states, depressive psychosis, and sometimes atypical confusional presentations, often on a bipolar diathesis background.[5][8]
Epidemiology and risk
Interview and systematic reviews show clinically important rates of perinatal depression and non-psychotic disorders across pregnancy and the postnatal year.[1][7] Population registers demonstrate a sharp rise in first psychiatric contacts and admissions after childbirth, particularly in the first postpartum month.[10] Women with bipolar disorder or prior postpartum psychosis carry high postpartum relapse risk — examiners expect this as a planning, not surprise, problem.[6][8] Untreated perinatal mental disorders affect fetal and child developmental outcomes as well as maternal morbidity and mortality framing.[9][18]
Pathophysiology and mechanisms
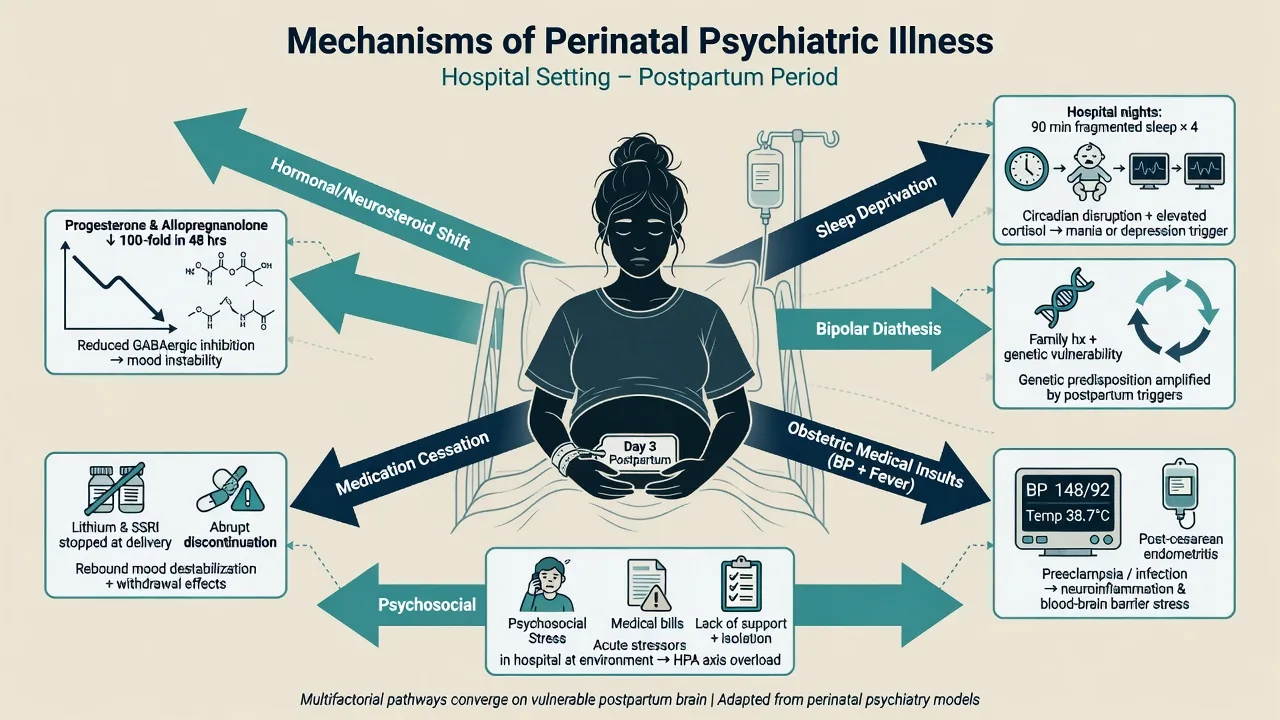
Mechanisms relevant to hospital work are multifactorial: abrupt hormonal and neurosteroid change, severe sleep deprivation, immune activation, blood loss and metabolic stress, obstetric complications, and psychotropic disruption when medicines are stopped at conception without a plan.[5][7][8]
Bipolar genetic vulnerability concentrates risk for early puerperal mania and psychosis; prior PPP is the strongest single historical predictor for recurrence without prophylaxis planning.[4][6][8]
Medical pathways on the ward include eclampsia and PRES, sepsis, thyroid storm or postpartum thyroiditis, hyponatraemia, anaesthetic or opioid effects, corticosteroid neuropsychiatry, and substance intoxication or withdrawal — each can mimic or co-occur with primary psychiatric illness.[5][12]
Clinical presentation in hospital
Antenatal admissions. Hyperemesis-linked despair, severe depression with poor oral intake, panic and tokophobia interfering with monitoring, substance withdrawal, and capacity disputes about induction or caesarean are classic CL triggers.[7][18]
Early puerperium red pattern. Rapid onset of insomnia without tiredness, elation or irritable mania, perplexity, delusions (often related to the infant or birth), hallucinations, and disorganised care of the baby — this is PPP until proven otherwise.[5][8][12]
OCD vs psychosis language. "I keep seeing myself dropping the baby and I know it is not me" with distress and checking is usually ego-dystonic OCD. "The baby is possessed and must be saved by sacrifice" with conviction and action risk is psychosis.[5][7]
Bonding and care capacity. Observe mother-infant interaction; inability to feed, soothe, or keep the infant safe may reflect depression, psychosis, exhaustion, pain, NICU separation, or medical illness — document behaviourally.[9][16]
Differential diagnosis — discriminators
Postpartum psychosis
- Rapid early puerperal onset
- Mania, mixed, or depressive psychosis
- Ego-syntonic delusions about infant
- Emergency dual-risk pathway
Perinatal MDD / anxiety
- Weeks of pervasive low mood/anhedonia
- Guilt, hopelessness, panic
- No full manic package
- Stepped therapy ± antidepressant
Perinatal OCD
- Ego-dystonic infant-harm images
- Insight usually preserved
- Checking and avoidance
- Not treated as PPP
Organic / medical
- Fever, BP, neurology, toxins
- Fluctuating inattention
- Steroids/sepsis/eclampsia
- Fix medical drivers first
Always hold eclampsia/PRES, infection, metabolic failure, thyroid disease, substance effects, and medication toxicity in the differential of puerperal confusion before locking a purely functional psychiatric label.[5][12]
Assessment on the maternity ward
- Obstetric context: gestation or postpartum day, delivery mode, complications, pain, blood loss, NICU status, breastfeeding goals.
- Drugs: psychotropics stopped or continued, steroids, opioids, antiemetics, substances.
- Psychiatric history: bipolar, prior PPP, depression, psychosis, self-harm, IPV, social supports.
- MSE: mood, sleep, psychosis content, attention, bonding behaviour.
- Dual risk: maternal suicide and self-harm; infant harm ideation, intent, psychosis; neglect risk; partner risk.
- Screening: EPDS is a validated depression screen, not a psychosis or suicide complete assessment — use clinically, not as discharge stamp.[2][7]
- Capacity: decision-specific for caesarean, induction, psychotropics, discharge with infant.
- Collateral: partner, midwifery, obstetric team, child-protection services when indicated.[5][7][8][18]
Investigations
Directed and time-critical when confusion or new psychosis appears: vital signs and blood pressure, glucose, FBC, U&E, LFTs, TFT, infection work-up, urine toxicology when indicated, and neurological examination for eclampsia/PRES features. ECG and baseline metabolic panel before psychotropics with QTc or metabolic risk. Lithium levels around delivery when the mother is on lithium. Imaging or EEG only if neurological red flags or results will change management — do not delay secure psychiatric care for PPP while waiting for non-urgent tests.[5][12][14]
Acute management and red flags
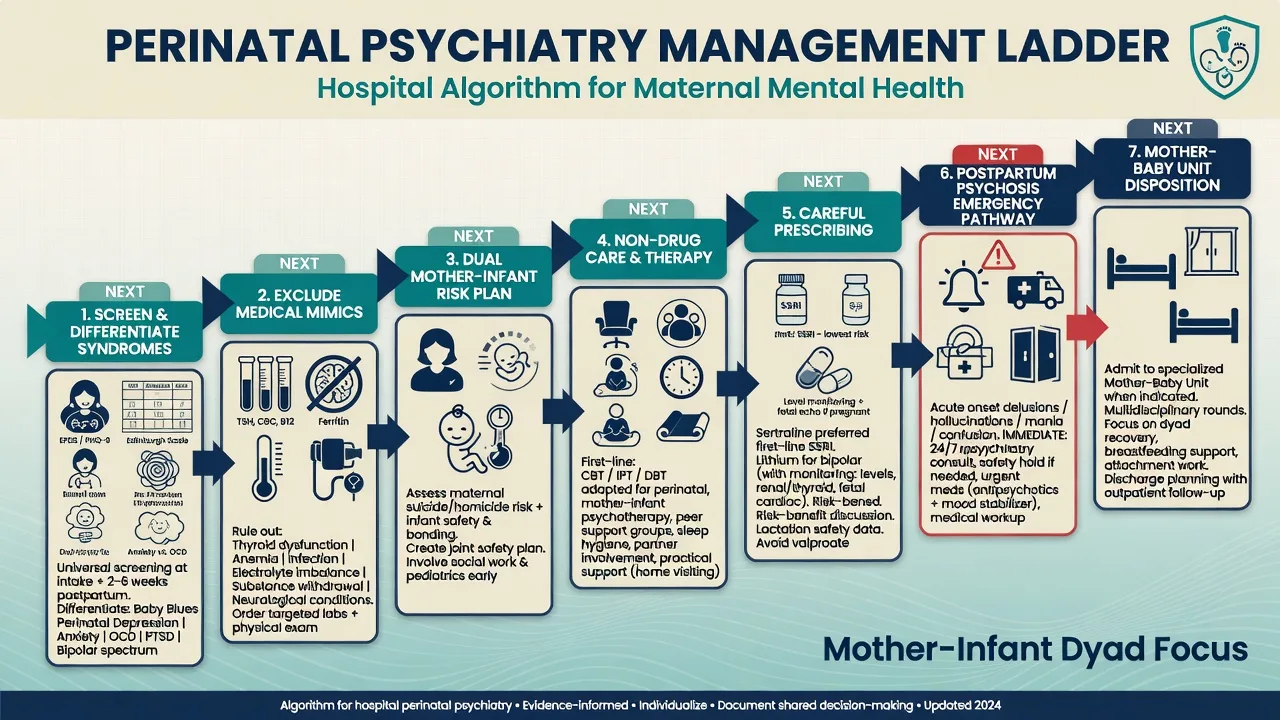
PPP emergency sequence (hospital): stabilise ABC and obstetric issues → exclude organic drivers → one-to-one nursing with infant safety plan (supervised contact if needed) → restore sleep → start antipsychotic and/or lithium pathway per severity and prior response → short-term benzodiazepine for severe insomnia/agitation when obstetric and neonatal teams agree → consider ECT early for life-threatening depression, catatonia, or refractory psychosis → use local mental health law only when criteria are met (statutes are jurisdiction-specific).[4][5][12][13]
For severe maternal suicidality without psychosis: observation intensity, means restriction, treat depression aggressively, involve supports, and do not normalise as "hormones."[7][18]
Definitive management
Non-psychotic perinatal depression and anxiety
Psychological therapies (CBT-informed care, interpersonal psychotherapy approaches, behavioural activation, partner-inclusive work) are first-line for mild-moderate illness and continue alongside medicines for moderate-severe illness when feasible in hospital or after discharge.[7][18] Optimise sleep, pain, anaemia, and social supports with the obstetric team — these are psychiatric interventions on the ward.[7][9]
Antidepressants in pregnancy and lactation
Risk-benefit counselling must include untreated depression risks (maternal suicide, poor antenatal care, substance use, bonding failure, child developmental impact) as well as medication signals.[9][11][18] Large meta-analytic data on early-pregnancy SSRI exposure and malformations show small absolute risks that require nuanced counselling rather than reflexive cessation of all antidepressants.[17] Maternal antidepressant use and pregnancy outcomes should be discussed with obstetric partners without alarmist or dismissive extremes.[11]
Practical fellowship start often used postpartum when an SSRI is indicated and lactation is desired: sertraline 50 mg oral daily, titrate toward response typically in the 50–150 mg daily range, monitor nausea, activation, hyponatraemia risk, and early suicide risk; reassess within 1–2 weeks. Sertraline features prominently in pooled lactation analyses showing relatively low infant serum levels among common antidepressants — still individualise and observe the infant.[15][11][3]
Do not stop an effective antidepressant at a positive pregnancy test without a documented plan; relapse of severe depression can exceed medication risk for many patients.[3][11][18]
Lithium, bipolar prophylaxis, and peri-delivery care
Prior bipolar disorder or PPP is a planning problem antenatally. Preventive strategies including lithium prophylaxis for high-risk women reduce postpartum mania/psychosis in specialised cohorts — individualise with obstetrics and document the peripartum plan early.[4][6][8]
Patorno et al. (NEJM 2017): lithium exposure in pregnancy was associated with an increased risk of cardiac malformations, with a small absolute risk increase that still requires structured counselling and shared decision-making rather than reflexive lifelong bans or casual prescribing.[14] Around labour and delivery, coordinate dose holding or adjustment, frequent levels, hydration, and neonatal monitoring because of fluid shifts and neonatal lithium exposure — this is classic general-hospital CL work with neonatology.[14][8]
Valproate is a major teratogen; avoid in pregnancy-capable patients except exceptional circumstances with documented safeguards and contraception planning — examiners treat casual valproate use as a fail.[3][8]
Antipsychotics and sleep in PPP
Treatment of postpartum psychosis and mania uses antipsychotics, lithium, and aggressive sleep restoration; Bergink and colleagues outline structured inpatient pathways and expect prompt response monitoring.[12][5] Choose agents with obstetric and neonatal awareness (metabolic, sedation, EPS, QTc); start low in medically frail mothers and titrate to effect with daily review. Example cautious acute ranges used in adult CL practice for severe agitation (individualise; check local formulary and lactation goals): olanzapine 5–10 mg oral or haloperidol 0.5–2 mg oral short-term with monitoring, combined with a sleep plan — not as monotherapy for untreated medical delirium.[12][5]
ECT in the perinatal hospital setting
ECT remains highly effective for severe depressive disorders and is a core option for life-threatening perinatal depression, catatonia, or refractory PPP when speed of response and oral intake matter; the UK ECT Review Group meta-analysis anchors efficacy in depressive illness broadly.[13][12][3] Coordinate obstetric anaesthesia, fetal or neonatal monitoring as relevant, left lateral tilt in late pregnancy, and aspiration risk. Do not reserve ECT only as last-resort folklore when the mother is not eating, is catatonic, or is severely suicidal.[13][5]
Mother-baby units and disposition
Australian public mother-baby units share common clinical functions with regional variation in models; when available, MBUs allow joint admission and intensive parenting support while treating maternal illness.[16] If no MBU bed exists, plan psychiatric admission with supervised infant access, or intensive home perinatal mental health follow-up only when dual-risk allows. Write a clear overnight and weekend contingency with midwifery and child-protection partners when needed.[16][18]
Special populations and scenarios
Adolescent mothers need developmentally adapted consent processes and safeguarding literacy. Stillbirth and neonatal death require grief-informed care without missing comorbid MDD. NICU separation drives panic, guilt, and bonding disruption — schedule contact and psychological support. Substance use in pregnancy is concurrent CL and addiction work with neonatal abstinence planning. Cultural and Indigenous care requires interpreters, family-inclusive decision-making, and avoidance of ethnocentric capacity shortcuts.[7][9][18]
Evidence and regional notes
ANZ / FRANZCP. Perinatal CL and MBU pathways are high-yield. Cite RANZCP mood guidelines for prescribing principles, Bergink for PPP, Galbally for Australian MBUs, and jurisdiction-specific mental health and child-protection statutes without inventing section numbers.[3][5][16]
UK / MRCPsych. NICE antenatal and postnatal mental health themes emphasise identification, stepped care, and specialist perinatal teams; CASC stations often test explaining PPP, medication in breastfeeding, and dual-risk plans.[7][18]
US / ABPN. Reproductive psychopharmacology items commonly test lithium cardiac risk framing (Patorno), antidepressant counselling (Yonkers/Gao), and emergency PPP recognition (Jones/Bergink).[11][14][17][8]
MD/DNB / NEET-SS. Expect viva on blues vs depression vs PPP, EPDS limits, sertraline in lactation, lithium peri-delivery, and ECT indications.[2][5][15][13]
Landmark names to drop cleanly: Gavin (prevalence), Cox (EPDS), Munk-Olsen (register admission risk), Lancet 2014 series (Howard, Jones, Stein), Bergink (prevention, treatment, PPP review), Wesseloo (relapse meta-analysis), Patorno (lithium cardiac malformations), Yonkers / Gao (antidepressants in pregnancy), Weissman (lactation levels), UK ECT Review Group, Galbally (ANZ MBUs), Malhi/RANZCP mood guidelines.[1][2][3][4][5][6][7][8][10][14][16]
Prognosis and disposition
PPP often responds well to prompt biological treatment, but bipolar recurrence risk remains high across future postpartum periods without a written plan.[4][6][12] Non-psychotic perinatal depression is treatable; untreated illness harms mothers and children.[7][9][18] Disposition should name setting (MBU, psychiatric unit, maternity ward with 1:1, home intensive), infant contact rules, psychotropic plan, sleep strategy, crisis contacts, and early outpatient perinatal review — highest intensity in the first two postpartum weeks for high-risk bipolar/PPP histories.[5][16][6]
Exam pearls
MATERNITY (ward scaffold)
Fellowship viva one-liners: PPP is a same-day dual-risk emergency; EPDS screens depression, not psychosis; sertraline is often preferred when breastfeeding if an SSRI is needed; lithium needs peri-delivery logistics, not slogans; OCD images are ego-dystonic — psychosis is not.[2][5][14][15]
References
- [1]Gavin NI, Gaynes BN, Lohr KN, Meltzer-Brody S, Gartlehner G, Swinson T Perinatal depression: a systematic review of prevalence and incidence Obstet Gynecol, 2005.PMID 16260528
- [2]Cox JL, Holden JM, Sagovsky R Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale Br J Psychiatry, 1987.PMID 3651732
- [3]Malhi GS, Bell E, Bassett D, Boyce P, Bryant R, Hazell P, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [4]Bergink V, Bouvy PF, Vervoort JS, Koorengevel KM, Steegers EA, Kushner SA Prevention of postpartum psychosis and mania in women at high risk Am J Psychiatry, 2012.PMID 22407083
- [5]Bergink V, Rasgon N, Wisner KL Postpartum Psychosis: Madness, Mania, and Melancholia in Motherhood Am J Psychiatry, 2016.PMID 27609245
- [6]Wesseloo R, Kamperman AM, Munk-Olsen T, Pop VJ, Kushner SA, Bergink V Risk of Postpartum Relapse in Bipolar Disorder and Postpartum Psychosis: A Systematic Review and Meta-Analysis Am J Psychiatry, 2016.PMID 26514657
- [7]Howard LM, Molyneaux E, Dennis CL, Rochat T, Stein A, Milgrom J Non-psychotic mental disorders in the perinatal period Lancet, 2014.PMID 25455248
- [8]Jones I, Chandra PS, Dazzan P, Howard LM Bipolar disorder, affective psychosis, and schizophrenia in pregnancy and the post-partum period Lancet, 2014.PMID 25455249
- [9]Stein A, Pearson RM, Goodman SH, Rapa E, Rahman A, McCallum M, et al. Effects of perinatal mental disorders on the fetus and child Lancet, 2014.PMID 25455250
- [10]Munk-Olsen T, Laursen TM, Pedersen CB, Mors O, Mortensen PB New parents and mental disorders: a population-based register study JAMA, 2006.PMID 17148723
- [11]Yonkers KA, Forray A, Smith MV Maternal Antidepressant Use and Pregnancy Outcomes JAMA, 2017.PMID 28810017
- [12]Bergink V, Burgerhout KM, Koorengevel KM, Kamperman AM, Hoogendijk WJ, Lambregtse-van den Berg MP, et al. Treatment of psychosis and mania in the postpartum period Am J Psychiatry, 2015.PMID 25640930
- [13]UK ECT Review Group Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis Lancet, 2003.PMID 12642045
- [14]Patorno E, Huybrechts KF, Hernandez-Diaz S Lithium Use in Pregnancy and the Risk of Cardiac Malformations N Engl J Med, 2017.PMID 28854098
- [15]Weissman AM, Levy BT, Hartz AJ, Bentler S, Donohue M, Ellingrod VL, et al. Pooled analysis of antidepressant levels in lactating mothers, breast milk, and nursing infants Am J Psychiatry, 2004.PMID 15169695
- [16]Galbally M, Sved-Williams A, Kristianopulos D, Mercuri K, Brown P, Buist A Comparison of public mother-baby psychiatric units in Australia: similarities, strengths and recommendations Australas Psychiatry, 2019.PMID 30407072
- [17]Gao SY, Wu QJ, Sun C, Zhang TN, Shen ZQ, Liu CX, et al. Selective serotonin reuptake inhibitor use during early pregnancy and congenital malformations: a systematic review and meta-analysis of cohort studies of more than 9 million births BMC Med, 2018.PMID 30415641
- [18]Howard LM, Khalifeh H Perinatal mental health: a review of progress and challenges World Psychiatry, 2020.PMID 32931106