Psych · Consultation-liaison psychiatry
Renal and dialysis psychiatry
Also known as Dialysis psychiatry · CKD depression · ESRD mental health · Uraemic encephalopathy psychiatry · Haemodialysis anxiety · Renal consultation-liaison
Exam-exhaustive fellowship topic on renal and dialysis psychiatry for consultation-liaison practice — depression and anxiety in CKD/ESRD, CAST and ASCEND evidence, uraemic encephalopathy and cognitive impairment, psychotropic dosing and lithium–kidney interface, non-adherence, capacity and dialysis withdrawal, and shared nephrology–psychiatry care. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Examiners use renal stems to test organic differentials, landmark depression trials (CAST/ASCEND), renal psychopharmacology, and capacity at end of dialysis life. A candidate who only recites primary MDD criteria will fail when the stem is uraemic delirium, fluid non-adherence, lithium in falling eGFR, or a request to stop haemodialysis.[5][6][11][13]
Overview and definition
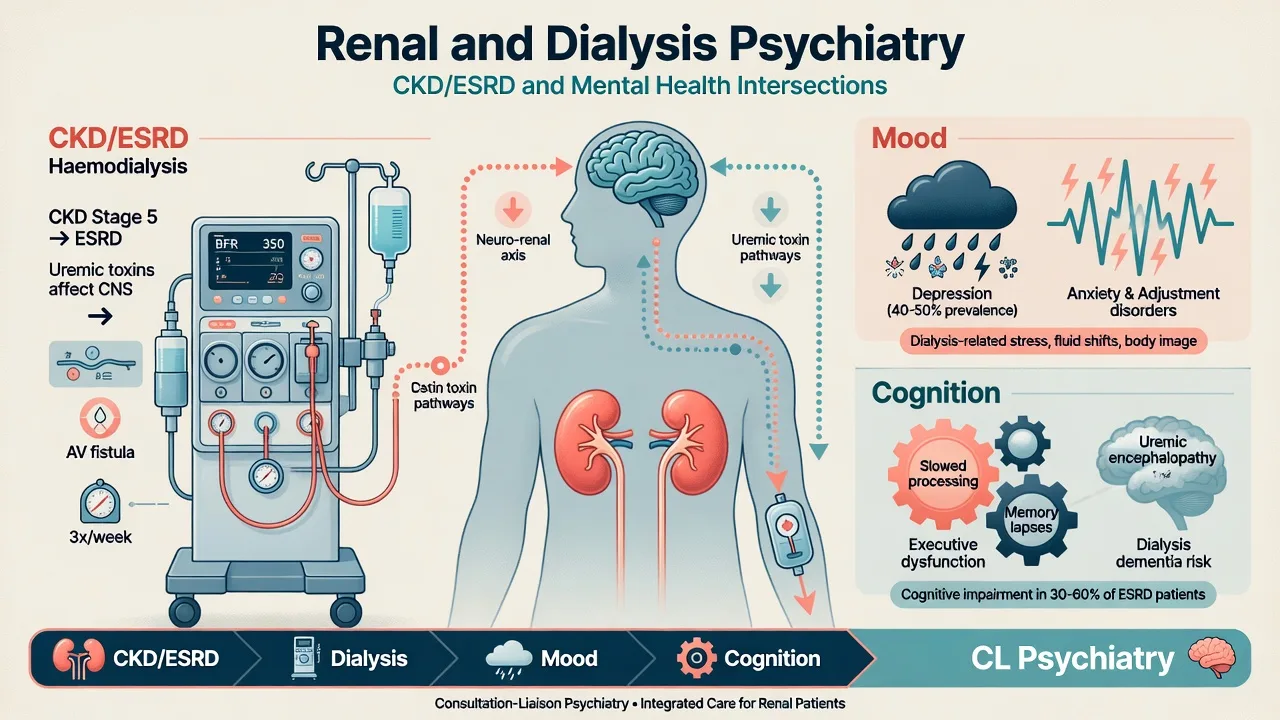
Renal and dialysis psychiatry is the consultation-liaison discipline covering psychiatric syndromes in chronic kidney disease (CKD), end-stage kidney disease (ESKD/ESRD), maintenance dialysis (haemodialysis and peritoneal dialysis), and interfaces with transplant and conservative kidney care. Coding may use depressive or anxiety disorder due to another medical condition, delirium, or primary psychiatric comorbidity; viva credit goes to mechanism, risk, renal-safe prescribing, and shared decision-making, not nosological pedantry alone.[4][9]
Core axes for fellowship exams are: high-prevalence depression and anxiety with mortality and adherence links; cognitive impairment across CKD stages; uraemic encephalopathy and dialysis-related confusional states; psychotropic pharmacokinetics in low eGFR and dialysis; non-adherence as a biopsychosocial problem; and dialysis withholding or withdrawal with rigorous capacity assessment.[1][2][10][11][12]
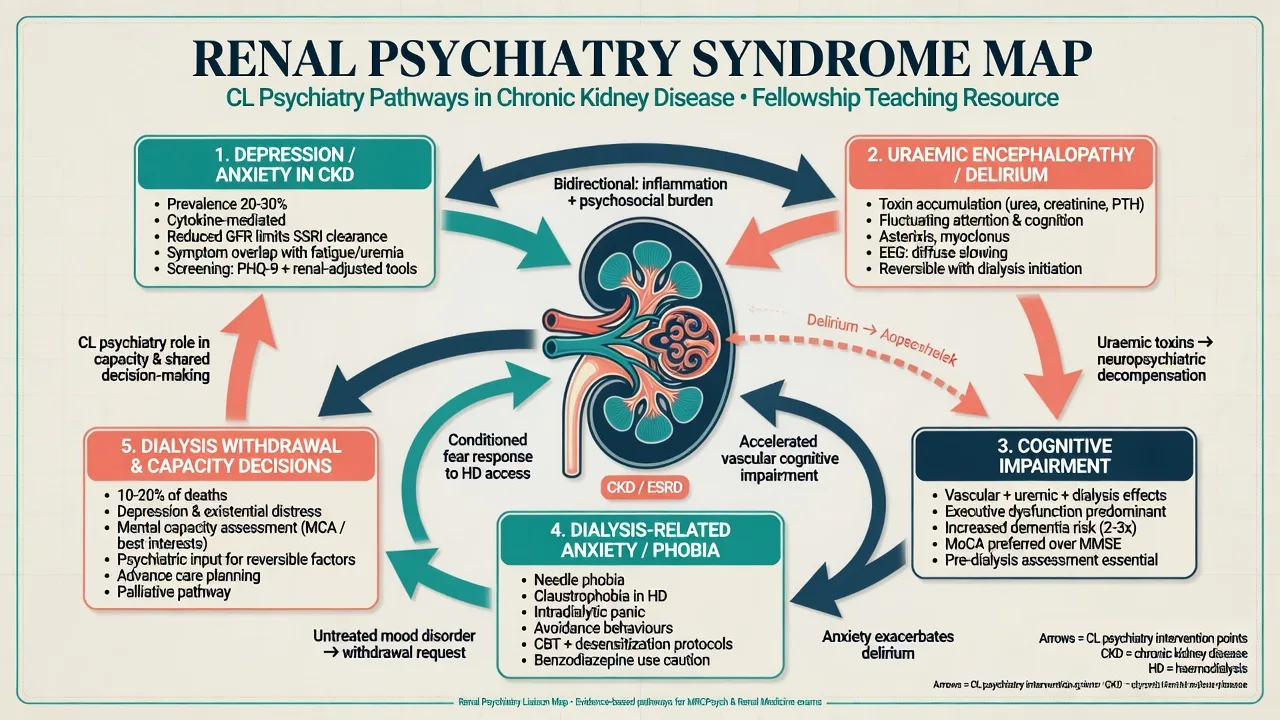
Classification and syndrome map
| Axis | Typical psychiatric pattern | Key medical anchors |
|---|---|---|
| CKD/ESRD depression | Anhedonia, guilt, hopelessness, suicidality beyond uraemic fatigue | High symptom burden; underdiagnosis common |
| Anxiety on dialysis | Panic, needle/machine phobia, GAD, death anxiety | Access procedures, alarms, intradialytic events |
| Uraemic encephalopathy | Fluctuating confusion, irritability, rare psychosis | Severe azotaemia; asterixis, myoclonus, seizures |
| Cognitive impairment | Executive dysfunction, slowed processing | Advanced CKD/HD; vascular and metabolic drivers |
| Dialysis refusal/withdrawal | Values-based refusal or impaired decision-making | Capacity, depression/delirium screen, palliative plan |
DSM-5-TR / ICD-11 allow medical and primary psychiatric coding. Discriminators that matter: tempo with metabolic change, dialysis adequacy and timing, physical and laboratory confirmation, and response when uraemia or depression is treated.[4][9]
Epidemiology and risk
Palmer and colleagues summarised a high point prevalence of depressive symptoms across CKD, with rates depending on whether self-report scales or diagnostic interviews are used — exam candidates must not equate a high PHQ-9 rate with interview-confirmed MDD.[1] Depression associates with increased risk of death in people with CKD in meta-analysed cohort data.[2] In non-dialysis CKD clinics, major depressive episode is common enough that routine screening is justified in practical treatment frameworks.[3][4]
On maintenance haemodialysis, urban samples show substantial current depressive disorder and frequent anxiety comorbidity; depressive affect contributes to low medication adherence.[7][8] Anxiety specifically is common yet overlooked in HD populations.[10] Cognitive impairment is frequent in CKD and worsens with more advanced disease.[12]
Risk amplifiers: prior psychiatric illness, social isolation, unemployment, pain and symptom burden, catheter vascular access, inadequate dialysis, fluid/diet restriction stress, and structural barriers to care.[4][8][9]
Pathophysiology and mechanisms
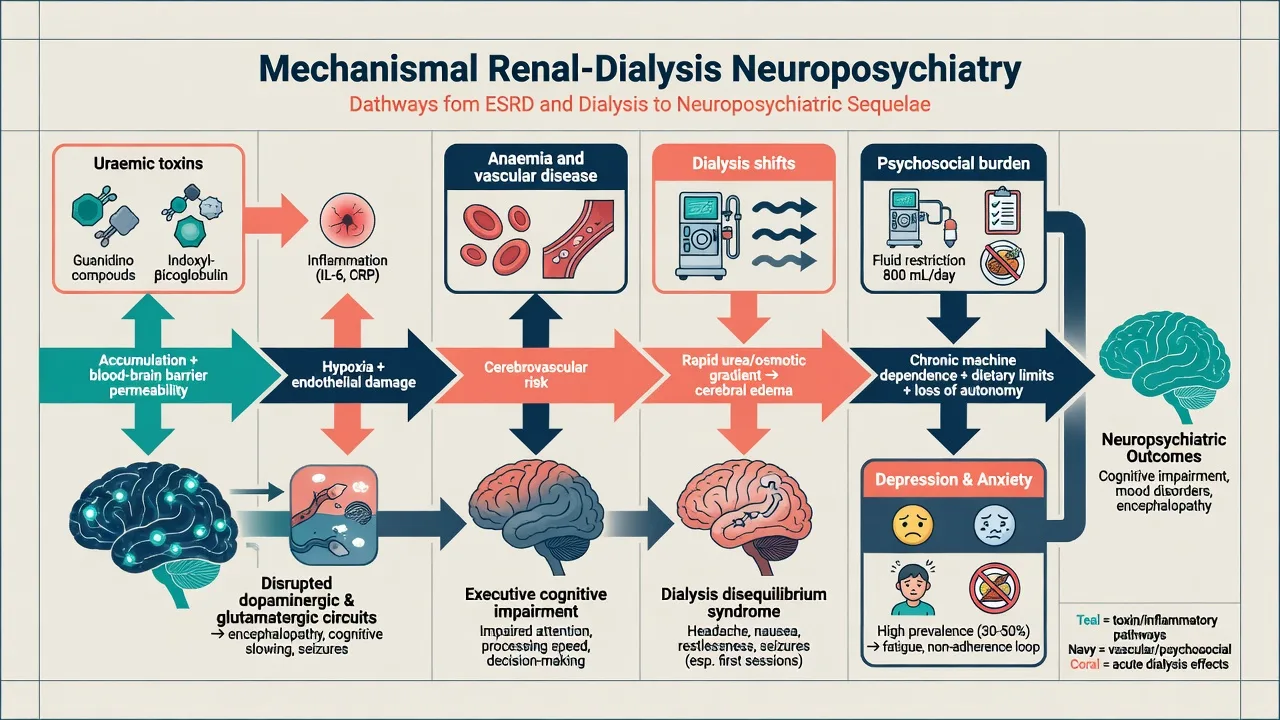
Biological. Retained uraemic solutes, chronic inflammation, anaemia, secondary hyperparathyroidism, and high vascular disease burden alter cerebral function and mood circuitry. Severe azotaemia produces uraemic encephalopathy, a toxic-metabolic delirium spectrum that can include neuromuscular irritability and seizures and that improves when adequate renal replacement is restored.[4][12]
Dialysis-specific. Rapid osmotic shifts can produce dialysis disequilibrium (headache, restlessness, rare seizures/delirium), especially early high-efficiency sessions. Intradialytic hypotension and silent cerebrovascular disease contribute to the executive cognitive phenotype emphasised in CKD cognition literature.[12]
Psychosocial. Machine dependence, body-image change (fistula, catheter, scars), loss of work role, dietary and fluid restriction, sexual dysfunction, and death anxiety maintain depression and anxiety independently of eGFR numbers alone.[7][9][10]
Pharmacokinetic. Reduced GFR slows clearance of renally excreted parent drugs and metabolites; uraemia alters protein binding; dialysis removes some small water-soluble agents (notably lithium), creating timing traps for levels and dosing.[13][14][15]
Clinical presentation
Depression in CKD and dialysis
Expect low mood, anhedonia, guilt, worthlessness, suicidal ideation, and impaired concentration. Do not dismiss these as "normal on dialysis." Overlap with uraemic fatigue, anorexia, and sleep disturbance is real — use psychological symptoms (anhedonia, excessive guilt, suicidal planning) and functional trajectory to diagnose major depression.[4][9]
Anxiety
Needle phobia, machine alarm panic, anticipatory dread of sessions, generalised worry, and PTSD-like responses after intradialytic crises are high-yield CL presentations. Anxiety is treatable and not a "personality problem."[7][10]
Cognitive change
Executive dysfunction, slowed processing, and attention deficits are common and under-detected; they impair consent, adherence, and safety at home on PD.[12]
Uraemic encephalopathy and behavioural emergencies
Fluctuating inattention, irritability, sleep–wake reversal, and agitation; severe cases progress toward stupor, seizures, or rare psychotic features. On the dialysis unit, line-pulling and leaving mid-session create medical emergencies requiring access protection and de-escalation.[4]
Differential diagnosis — discriminators
- High symptom burden context
- Anhedonia/guilt/suicidality beyond fatigue
- Adherence and QoL impact
- Responds to multimodal CL care
- CAST/ASCEND evidence base
- Acute fluctuating inattention
- Asterixis, myoclonus, severe azotaemia
- Infection/electrolyte/drug toxicity co-causes
- Improves with RRT optimisation
- Not primary schizophrenia
- Understands options and consequences
- Consistent values over time
- Depression/delirium treated or excluded
- Palliative plan available
- Not equated with suicide automatically
Also hold: primary bipolar/psychotic illness, substance withdrawal, stroke, hypothyroidism, B12 deficiency, hypercalcaemia, hyponatraemia, infection, and psychotropic toxicity (lithium, gabapentinoids).[13][15]
Assessment
- Renal context: CKD stage, eGFR, modality (HD/PD), residual urine output, adequacy, access type, transplant listing or conservative pathway.
- Symptom burden: pain, pruritus, insomnia, restless legs, sexual function, intradialytic symptoms.
- MSE: mood valence, anxiety, psychosis, attention (delirium screen), insight.
- Risk: suicide, access self-harm, deliberate missed dialysis as passive self-harm, aggression around access.
- Capacity: decision-specific for starting, continuing, or stopping dialysis; reassess when delirium or severe depression is treated.[4][11]
- Collateral from dialysis nurses, nephrology, and family — unit staff often know non-adherence patterns first.
Investigations
Routine package. Urea and electrolytes, eGFR, bicarbonate, calcium/phosphate/PTH, haemoglobin and iron studies, glucose, B12/folate, thyroid function, infection markers as indicated.[4]
Neuro work-up. Image or EEG when focal signs, first seizures without clear uraemic explanation, atypical progressive cognitive decline, or encephalitis differential — not automatically for every fluctuating uraemic confusion that clears with dialysis.[12]
Drug safety. Lithium trough timed to dialysis schedule; review renally cleared psychotropics; ECG before QT-prolonging agents given electrolyte flux risk.[13][15]
Acute management and red flags
Agitation mid-dialysis. Protect fistula/catheter first; reduce stimulation; use the lowest effective short-term antipsychotic if behavioural risk is high (example cautious adult starting range used in medical illness: haloperidol 0.5–1 mg oral or IM, or olanzapine 2.5–5 mg oral, with EPS/QTc monitoring and early stop when the driver is fixed).[13]
Lithium toxicity. Stop lithium; serial levels; volume support if depleted; involve nephrology/toxicology; extracorporeal treatment per EXTRIP recommendations when severity criteria are met.[15][16]
Suicide and access risk. Joint observation plan; remove immediate means where possible; legal status under local mental health law if criteria met. Depression in CKD associates with adverse outcomes including mortality risk, so treat active suicidal ideation as a shared medical–psychiatric emergency rather than unit discipline alone.[2][4]
Definitive management
Depression — multimodal, not nihilistic
Practical frameworks emphasise screening, diagnosis, and combined medical, psychological, and social care rather than therapeutic despair.[4][9]
CAST (non-dialysis CKD MDD). Sertraline was not superior to placebo for depressive symptoms in patients with CKD without dialysis dependence. This does not mean depression is untreatable — it means do not oversell SSRI monotherapy, integrate psychosocial care, and individualise after shared decision-making.[5]
ASCEND (maintenance HD). Both cognitive behavioural therapy and sertraline improved depression; the trial informs comparative real-world options on dialysis, including engagement strategies for treatment acceptance.[6]
Example cautious antidepressant starts after medical review (individualise; local formulary; watch hyponatraemia, bleeding risk, QTc): sertraline 25–50 mg oral daily titrating slowly, commonly preferred in renal teaching because of favourable clinical experience and ERBP-oriented reviews of antidepressant use in advanced CKD — still monitor closely.[13][14]
Anxiety
CBT and exposure for needle/machine phobia; dialysis-unit behavioural plans; short-term low-dose anxiolysis only if essential, preferring agents with less active-metabolite accumulation and avoiding reflexive long-acting benzodiazepines in frail or cognitively impaired patients.[10]
Psychotropics and the kidney
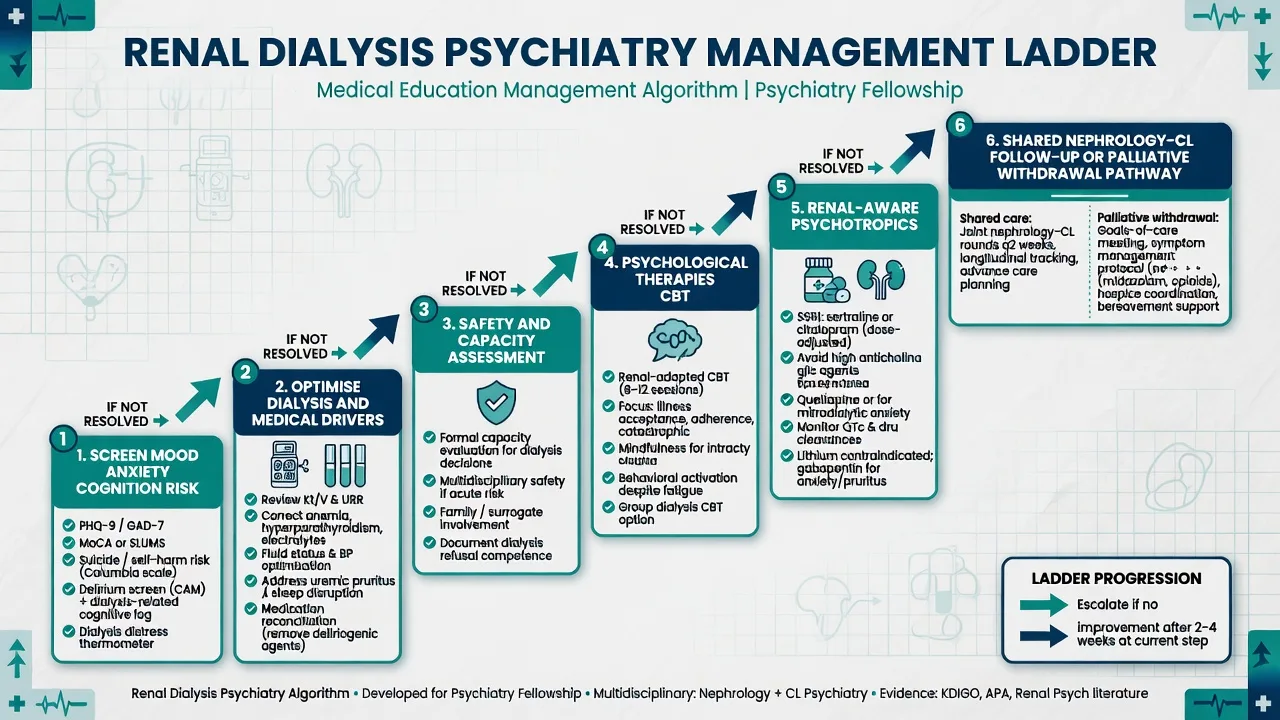
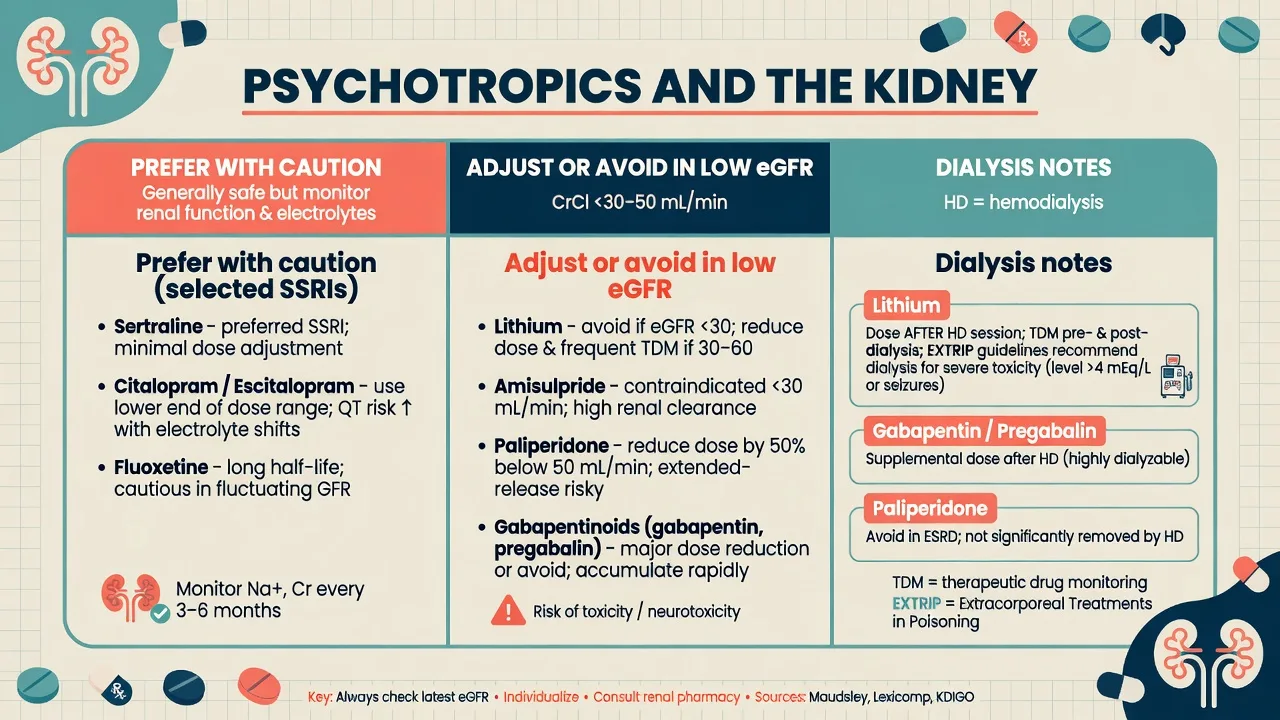
- Prefer agents with better-studied or more favourable renal profiles when possible; start low, titrate slow.[13][14]
- Adjust or avoid high renal-dependence agents: lithium, amisulpride, paliperidone, gabapentin, pregabalin — dose to CrCl/eGFR or choose alternatives.[13]
- Lithium: shared nephrology decision when eGFR falls; levels, thyroid/renal monitoring; dose after dialysis if continued on HD; remember chronic kidney risk signals from systematic review literature without abandoning lithium's bipolar efficacy lightly.[15]
- Toxicity pathway: EXTRIP guides extracorporeal treatment for severe lithium poisoning.[16]
Non-adherence
Treat depression and cognitive barriers; use motivational interviewing; involve social work for transport, cost, and housing; coordinate fluid/diet education with the dialysis team rather than purely blaming the patient.[8]
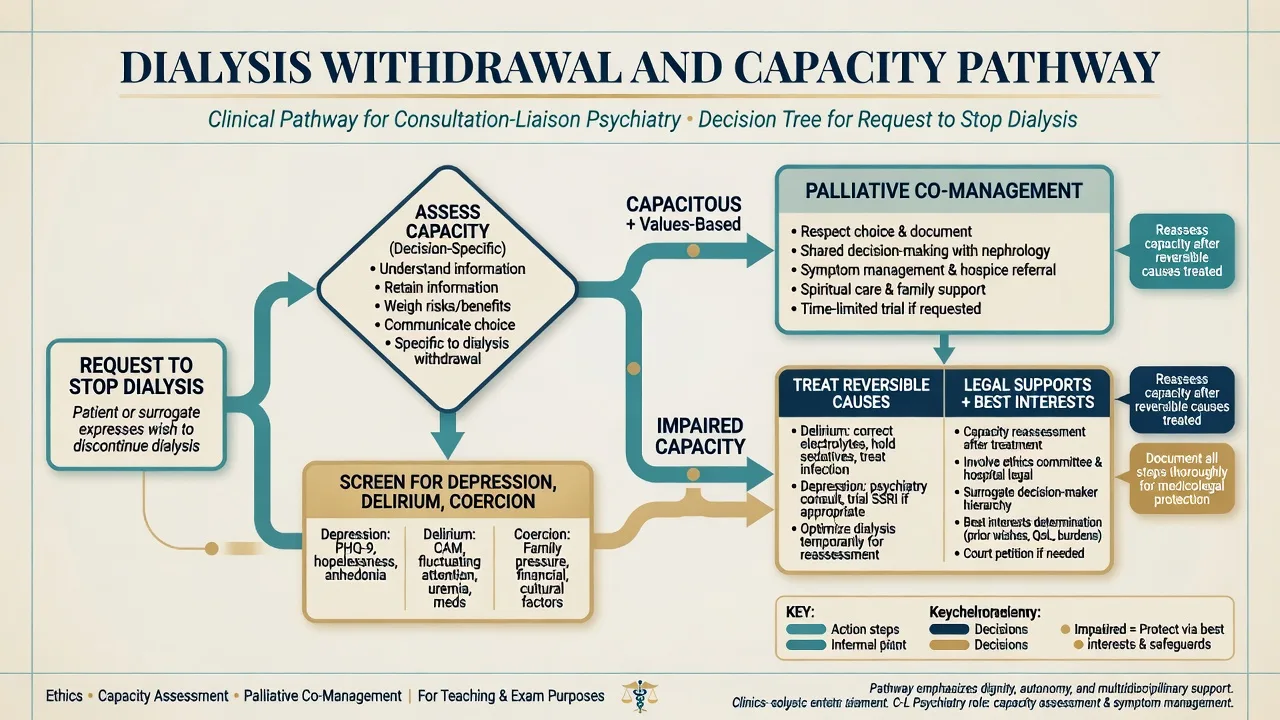
Dialysis withdrawal and capacity
Stopping dialysis can be an ethically appropriate option when burdens outweigh benefits; practical frameworks stress symptom control, family communication, and palliative co-management after a careful process.[11] CL psychiatry tasks:
- Assess decision-specific capacity (understand, appreciate, reason, communicate).
- Screen and treat depression, delirium, coercion, and inadequate information.
- If capacitous and values-consistent: support nephrology–palliative pathway; document.
- If impaired: treat reversible causes; use local guardianship/mental health law; avoid simplistic equivalence of withdrawal with suicide, while still taking suicidal intent seriously when present.[11]
Special populations
Older adults: frailty, polypharmacy, delirium risk, and conservative kidney management pathways — lower psychotropic starts.[12][13] Young adults: adherence, identity, body image, fertility, and transition from paediatric services. PD at home: cognitive and mood fitness for self-care. Indigenous and culturally diverse patients: interpreter use, family decision models, and equity of transplant/dialysis access. Pre-transplant: psychiatric assessment interfaces with adherence prediction humility and support planning.
Evidence and regional notes
ANZ / FRANZCP. Viva expects CAST/ASCEND name recognition, uraemic delirium priorities, lithium–CKD traps, and capacity for dialysis withdrawal. Pair with local mental health and guardianship law and ANZSN/KDIGO-informed nephrology practice.[5][6][11]
UK / MRCPsych. Paper and CASC stems often hide depression on dialysis or capacity to refuse RRT; NICE depression and CKD pathways still require medical differentials.[4][11]
US / ABPN. CAST (JAMA) and ASCEND (Ann Intern Med) are blueprint-friendly; EXTRIP lithium and ERBP antidepressant reviews support prescribing items.[5][6][14][16]
MD/DNB / NEET-SS. Expect classic lists: depression prevalence in ESRD, uraemic encephalopathy features, psychotropics in renal failure, and dialysis discontinuation ethics.[1][9][13]
Landmark names: Palmer (prevalence and mortality meta-analyses); Hedayati (MDE prevalence, practical treatment, CAST); Mehrotra/Cukor (ASCEND); Cukor (HD depression/anxiety, adherence); Kimmel (ESRD depression teaching); Cohen (withdrawal; anxiety on HD); Kurella (cognition); Baghdady/Nagler (renal psychotropics/antidepressants); McKnight and EXTRIP (lithium harm and extracorporeal treatment).[1][2][5][6][11][15][16]
Prognosis and disposition
Depression associates with higher mortality risk and poorer adherence; treating mood and anxiety aims at quality of life, engagement, and possibly intermediate outcomes even where survival trial data remain incomplete.[2][8] Cognitive burden may progress with advancing CKD and dialysis exposure for some patients — plan supports rather than surprise failures of self-care.[12]
Disposition: shared nephrology–CL follow-up; dialysis unit communication of risk and adherence plans; transplant pathway mental health support when listed; early palliative care when goals shift toward withdrawal or conservative care.[4][11]
Exam pearls
References
- [1]Palmer S, Vecchio M, Craig JC, et al. Prevalence of depression in chronic kidney disease: systematic review and meta-analysis of observational studies Kidney Int, 2013.PMID 23486521
- [2]Palmer SC, Vecchio M, Craig JC, et al. Association between depression and death in people with CKD: a meta-analysis of cohort studies Am J Kidney Dis, 2013.PMID 23623139
- [3]Hedayati SS, Minhajuddin AT, Toto RD, et al. Prevalence of major depressive episode in CKD Am J Kidney Dis, 2009.PMID 19493599
- [4]Hedayati SS, Yalamanchili V, Finkelstein FO A practical approach to the treatment of depression in patients with chronic kidney disease and end-stage renal disease Kidney Int, 2012.PMID 22012131
- [5]Hedayati SS, Gregg LP, Carmody T, et al. Effect of Sertraline on Depressive Symptoms in Patients With Chronic Kidney Disease Without Dialysis Dependence: The CAST Randomized Clinical Trial JAMA, 2017.PMID 29101402
- [6]Mehrotra R, Cukor D, Unruh M, et al. Comparative Efficacy of Therapies for Treatment of Depression for Patients Undergoing Maintenance Hemodialysis: A Randomized Clinical Trial Ann Intern Med, 2019.PMID 30802897
- [7]Cukor D, Coplan J, Brown C, et al. Depression and anxiety in urban hemodialysis patients Clin J Am Soc Nephrol, 2007.PMID 17699455
- [8]Cukor D, Rosenthal DS, Jindal RM, et al. Depression is an important contributor to low medication adherence in hemodialyzed patients and transplant recipients. Kidney Int, 2009.PMID 19242502
- [9]Kimmel PL Depression in patients with chronic renal disease: what we know and what we need to know J Psychosom Res, 2002.PMID 12377308
- [10]Cohen SD, Cukor D, Kimmel PL Anxiety in Patients Treated with Hemodialysis Clin J Am Soc Nephrol, 2016.PMID 27660303
- [11]Cohen LM, Germain MJ, Poppel DM Practical considerations in dialysis withdrawal: "to have that option is a blessing" JAMA, 2003.PMID 12709469
- [12]Kurella M, Chertow GM, Luan J, et al. Cognitive impairment in chronic kidney disease J Am Geriatr Soc, 2004.PMID 15507063
- [13]Baghdady NT, Banik S, Swartz SA, et al. Psychotropic drugs and renal failure: translating the evidence for clinical practice Adv Ther, 2009.PMID 19444657
- [14]Nagler EV, Webster AC, Vanholder R, et al. Antidepressants for depression in stage 3-5 chronic kidney disease: a systematic review of pharmacokinetics, efficacy and safety with recommendations by European Renal Best Practice (ERBP) Nephrol Dial Transplant, 2012.PMID 22859791
- [15]McKnight RF, Adida M, Budge K, et al. Lithium toxicity profile: a systematic review and meta-analysis Lancet, 2012.PMID 22265699
- [16]Decker BS, Goldfarb DS, Dargan PI, et al. Extracorporeal Treatment for Lithium Poisoning: Systematic Review and Recommendations from the EXTRIP Workgroup Clin J Am Soc Nephrol, 2015.PMID 25583292