Psych · Consultation-liaison psychiatry
SLE and autoimmune neuropsychiatry
Also known as Neuropsychiatric SLE · NPSLE · Lupus psychosis · Lupus cerebritis · CNS lupus · Anti-ribosomal P · Autoimmune neuropsychiatry · SLE neuropsychiatric syndromes
Exam-exhaustive fellowship topic on neuropsychiatric systemic lupus erythematosus and related autoimmune neuropsychiatry — ACR 19 syndromes, attribution, inflammatory versus thrombotic mechanisms, anti-ribosomal P and anti-NR2 signals, EULAR-aligned treatment branches, steroid psychosis, and CL psychopharmacology. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Psychiatrists fail this topic when every mood change in lupus is labelled "cerebritis," when infection is missed before cyclophosphamide, or when steroid mania is treated as primary bipolar disorder without a shared steroid plan. Examiners reward attribution discipline, mechanism branching, and honest limits of autoantibodies.[5][6][14]
Overview and definition
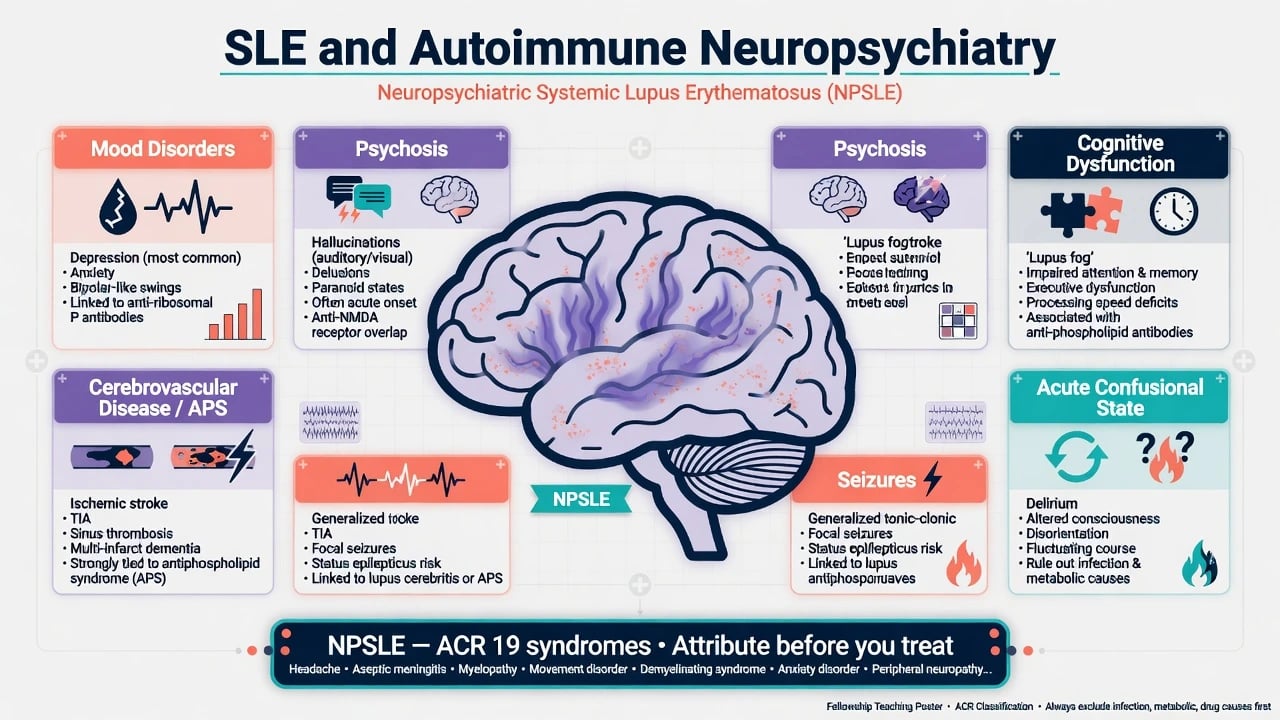
Systemic lupus erythematosus (SLE) is a multi-system autoimmune disease. Neuropsychiatric SLE (NPSLE) denotes neurologic and psychiatric syndromes linked to SLE after rigorous exclusion of alternative explanations. The 1999 ACR nomenclature provides case definitions for 19 syndromes (12 central, 7 peripheral) to standardise reporting — it does not automatically prove lupus causality for every listed event.[1][3]
DSM-5-TR / ICD-11 framing uses mental disorder due to another medical condition (or medication-induced) when SLE (or its treatment) is judged causal. Classification of SLE itself uses frameworks such as SLICC 2012 and EULAR/ACR 2019 criteria; those diagnose SLE, not the specific NP syndrome.[13]
Related autoimmune neuropsychiatry for the viva includes antiphospholipid syndrome (APS) cerebrovascular disease, primary autoimmune encephalitis, Sjögren CNS disease, and demyelinating mimics — each with different antibody logic and treatment ownership.[6][14]
Classification — ACR 19 syndromes
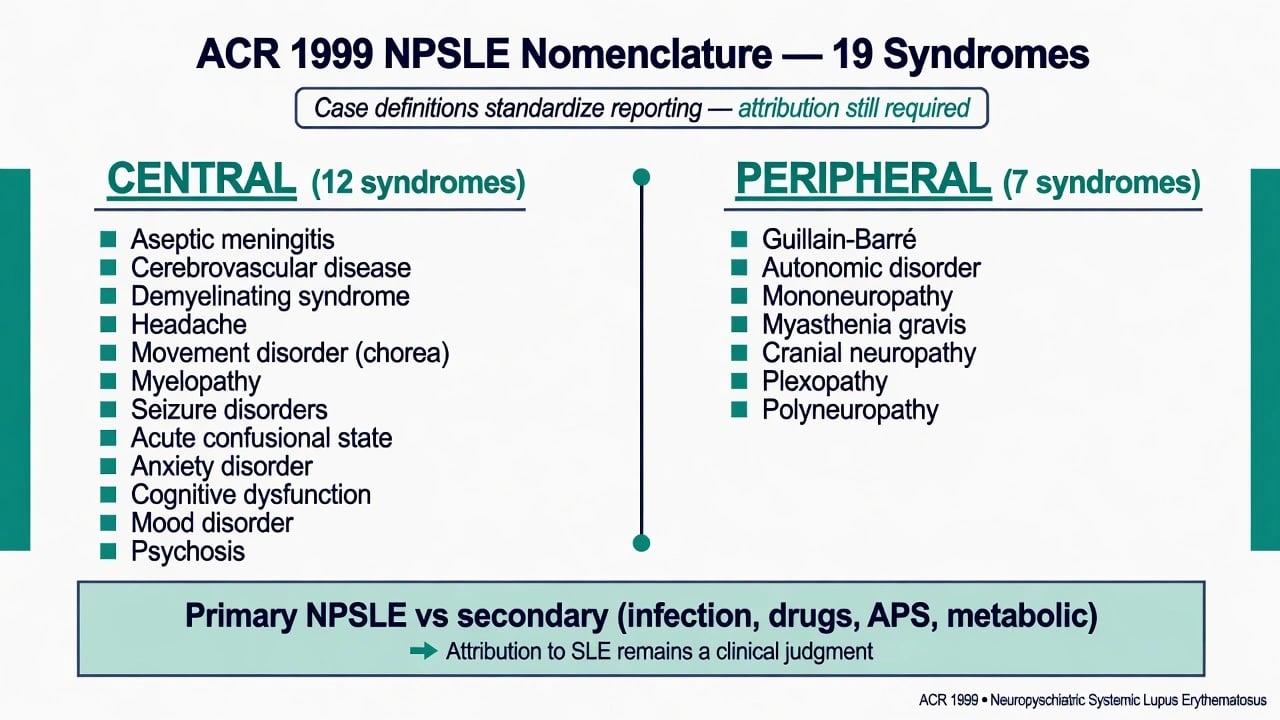
Central (exam core for psychiatry): acute confusional state, anxiety disorder, cognitive dysfunction, mood disorder, psychosis, plus headache, seizure disorders, cerebrovascular disease, aseptic meningitis, demyelinating syndrome, movement disorder (chorea), myelopathy.[1]
Peripheral: Guillain-Barré, autonomic disorder, mononeuropathy, myasthenia gravis, cranial neuropathy, plexopathy, polyneuropathy.[1]
Ainiala and colleagues showed that applying ACR case definitions without attribution filters yields very high NP prevalence, driven by common non-specific events (especially headache and mild cognitive complaints). Validity improves when mild or poorly attributed events are excluded — a classic exam pearl.[2][3]
Epidemiology and risk
Population and clinic estimates of NPSLE vary widely because of case-definition stringency. Unterman and colleagues' meta-analysis synthesises heterogeneous prevalence of the ACR syndromes across studies; headache, mood disorder, and cognitive dysfunction dominate crude tallies, while psychosis and ACS are less frequent but high-stakes.[4]
The international SLICC inception cohort (Hanly and colleagues) prospectively tracked NP events, attribution, and impact on health-related quality of life — many events are multifactorial or not primarily SLE-attributed, yet still impair function.[9] A dedicated inception analysis of mood disorders found they are common in SLE and often not solely explained by active CNS lupus; psychiatry still owns risk and treatment.[10]
Risk amplifiers: high global SLE activity, prior NP events, aPL positivity (especially for stroke/TIA phenotype), childhood-onset disease in some series, and glucocorticoid exposure for iatrogenic affective/psychotic states.[9][5][14]
Pathophysiology (viva depth)
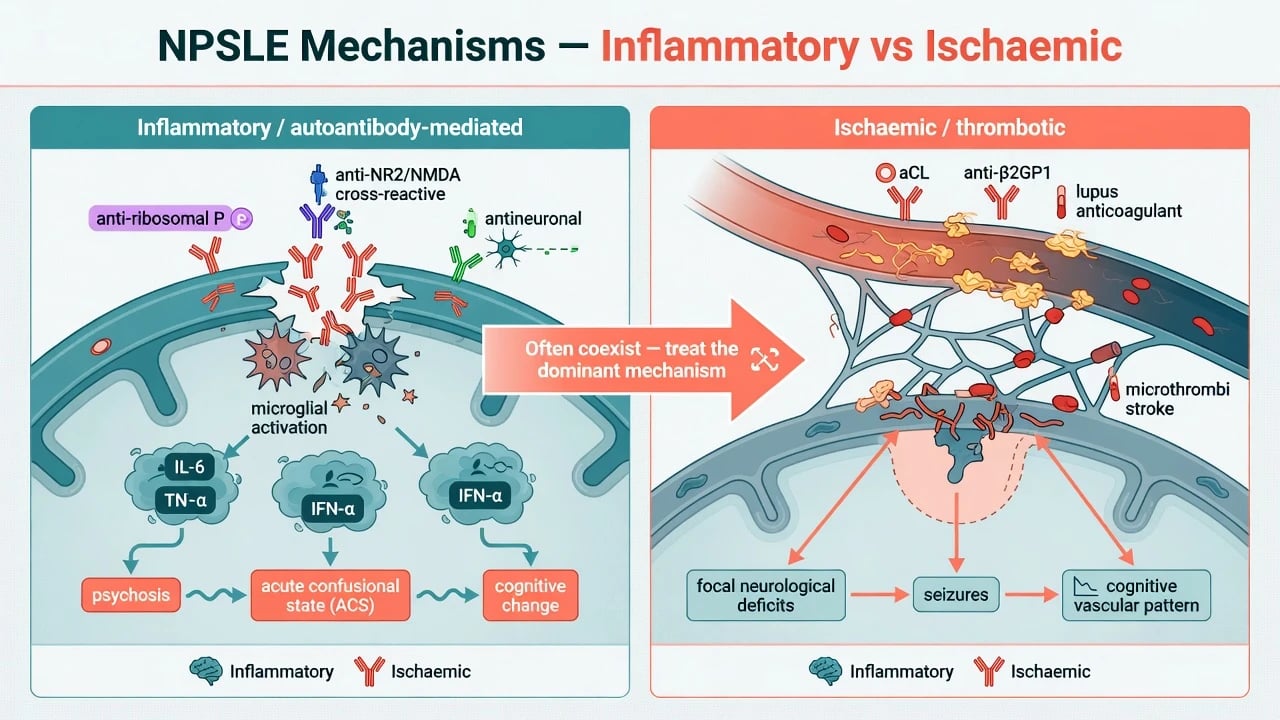
Two interlocking mechanisms dominate teaching models for fellowship-level NPSLE care.[6][14]
-
Inflammatory / autoantibody-mediated. Blood-brain barrier disruption allows autoantibodies and cytokines to injure neuronal networks. Anti-ribosomal P antibodies have been associated with lupus psychosis and diffuse NPSLE phenotypes in classic serologic studies (Isshi and Hirohata) — supportive, not pathognomonic.[7] A subset of lupus anti-DNA antibodies cross-reacts with the NR2 subunit of the NMDA receptor (DeGiorgio and colleagues), linking adaptive immunity to glutamatergic dysfunction and cognitive/behavioural change in experimental and translational models.[8]
-
Ischaemic / thrombotic. Antiphospholipid antibodies (lupus anticoagulant, anticardiolipin, anti-β2-glycoprotein I) promote endothelial injury and arterial/venous events, producing focal deficits, seizures, and vascular cognitive patterns. Steroids alone will not fix pure thrombotic disease.[5][6]
Mechanisms often coexist. The clinical task is to decide which driver is dominant for the current event because that choice sets the drug class.[6][14]
Clinical presentation (MSE language)
Mood disorder. Persistent dysphoria, anhedonia, guilt, insomnia, and suicidality may track SLE activity, demoralisation from chronic illness, steroid effects, or primary mood diathesis. Inception data show mood events are frequent and clinically important even when not fully "CNS lupus."[10]
Psychosis. New delusions or hallucinations with preserved or fluctuating alertness; often subacute in the setting of active SLE. Historical teaching links anti-ribosomal P, but serology never replaces full organic work-up.[7][1]
Acute confusional state (ACS). Lupus-related delirium: inattention, disorientation, fluctuating arousal — infection and metabolic causes first, always.[1][5]
Cognitive dysfunction. Attention, processing speed, memory, and executive complaints ranging from "lupus fog" to multi-domain impairment; vascular contribution when aPL/stroke history is present.[4][9]
Hard neurologic anchors. Seizures, chorea, myelopathy, stroke/TIA, aseptic meningitis — pull neurology in early.[1][5]
Steroid toxicity. Insomnia, euphoria, irritability, mania, or psychosis temporally linked to high-dose pulses or rapid escalations — a CL classic after nephritis treatment.[6][11]
Differential diagnosis
| Presentation | Prefer SLE-attributed when... | Prefer alternative when... |
|---|---|---|
| Psychosis | Active SLE, multi-system flare, anti-P supportive, infection excluded | Isolated chronic psychosis, substance use, primary FEP without SLE activity |
| ACS / delirium | Active SLE after infection ruled out | Fever, opportunistic infection, metabolic, Wernicke, drug toxicity |
| Mood episode | Temporal link to flare or steroids; multi-system activity | Long primary bipolar history offline from SLE activity |
| Focal deficit | aPL positive, MRI vascular territory | Purely inflammatory MRI patterns without aPL still need both tracks considered |
| New AE-like course | SLE context possible | Pure anti-NMDAR multistage encephalitis without SLE — different pathway |
Use the table as an attribution scaffold, not a checklist substitute for full history and work-up.[5][6]
Always include infection on immunosuppression, primary autoimmune encephalitis, MS/NMO spectrum, and functional neurological symptoms that can co-occur with SLE.[5][6][14]
Assessment for CL
Structure the consult: SLE phenotype and current activity (rash, arthritis, nephritis, cytopenias), full drug list with steroid dose and recent pulses, infection risk and prophylaxis, aPL and thrombosis history, prior NP events, substance use, sleep, pain, and suicide risk with plan/intent questions.[9][10]
MSE examples: fluctuating attention in ACS; mood-congruent psychotic content in severe depression; manic speech after methylprednisolone; perseveration and slowed processing in cognitive syndromes. Complete a focused neurologic screen. Assess capacity for investigation and treatment; document least-restrictive legal pathway under local law when consent is impaired — do not invent foreign statute numbers.[5][14]
Investigations
- SLE activity package: anti-dsDNA, C3/C4, blood count, creatinine, urinalysis, inflammatory markers (remember CRP may stay modest in pure SLE while infection raises it).[11][12]
- aPL panel: lupus anticoagulant, aCL IgG/IgM, anti-β2GP1.[5][6]
- Anti-ribosomal P when diffuse psychiatric phenotypes are under discussion — interpret with clinical syndrome.[7]
- MRI brain (± spine for myelopathy); EEG for seizure/ACS; LP when infection, inflammatory CNS disease, or AE differential requires CSF (cells, protein, culture/PCR, consider neuronal Abs if AE is live).[5][6]
- Do not overcall every non-specific white-matter change as active cerebritis.[14]
Acute management
- Stabilise ABCDE, treat seizures, activate stroke pathway if indicated.
- Delirium bundle and infection screen before escalating immunosuppression.
- Joint rheumatology ± neurology ownership for disease-modifying decisions.
- Short-term symptomatic psychotropics for safety while attribution proceeds.[5][6]
Definitive management (mechanism branch)
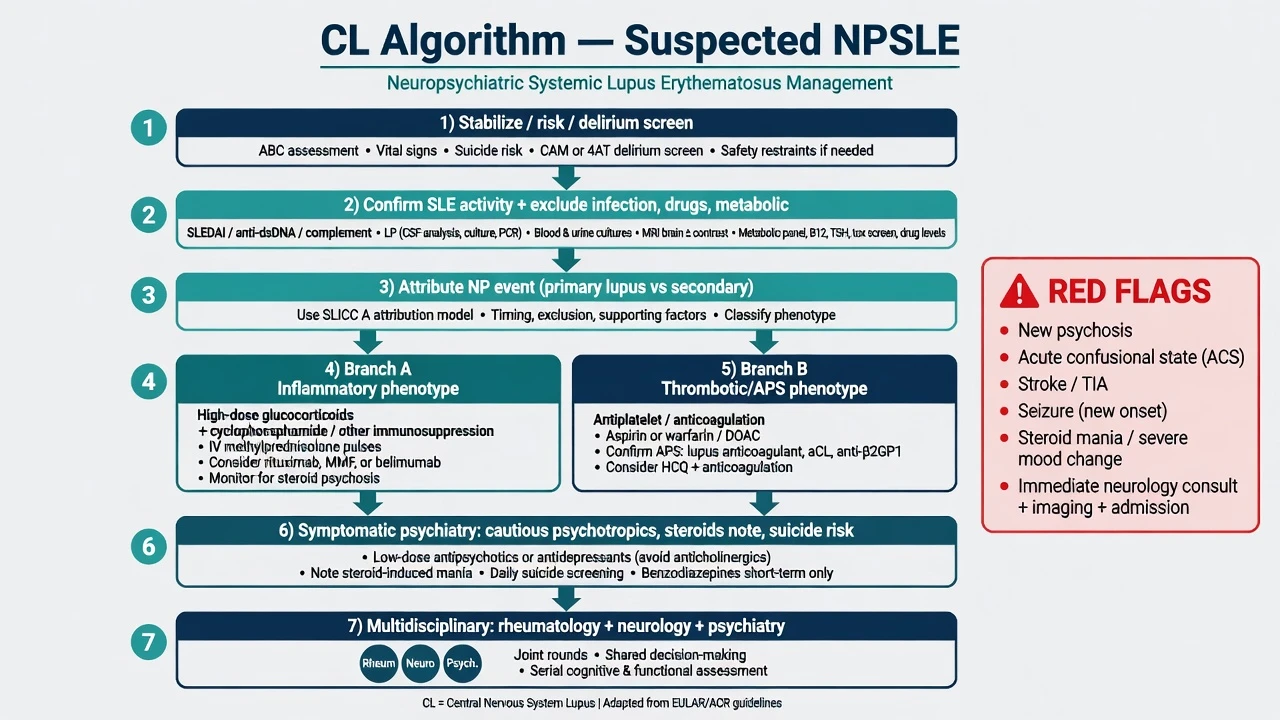
EULAR recommendations for NPSLE (Bertsias task force) and subsequent general SLE updates (Fanouriakis 2019 and 2023) structure care around symptom severity, inflammatory versus APS/thrombotic mechanisms, and glucocorticoid-sparing immunosuppression where appropriate.[5][11][12]
Inflammatory severe CNS events (psychosis, ACS, inflammatory myelopathy, etc.)
Cornerstone teaching: high-dose glucocorticoids plus immunosuppression, classically intravenous cyclophosphamide for severe inflammatory NP disease, with alternatives (mycophenolate, azathioprine maintenance, rituximab, IVIG, plasma exchange) in refractory or contraindicated settings under specialist protocols.[5][6]
Exam-level steroid example (adult, specialist protocol only): methylprednisolone 500–1000 mg IV daily for 3 days (local protocol and infection screen first), then oral prednisolone taper co-managed with rheumatology, monitoring glucose, blood pressure, infection, mood, and insomnia.[5][6][11] Exact cytotoxic dosing belongs to rheumatology protocols — quote principles, not freestyle chemo recipes in the viva.
Thrombotic / APS phenotype
Antiplatelet or anticoagulation (often warfarin with target INR per APS phenotype and local protocol) plus risk-factor control; do not treat pure thrombotic stroke as if it were only cerebritis.[5][6][12]
Symptomatic psychiatry
- Depression: SSRI first-line in medically complex adults after interaction review. Example: sertraline 50 mg oral once daily, titrate toward 100–150 mg oral daily as tolerated under review; monitor hyponatraemia, sexual dysfunction, bleeding risk with anticoagulants/NSAIDs, activation, and suicidality early.[10][6]
- Psychosis: lowest effective second-generation antipsychotic (e.g. olanzapine 2.5–5 mg oral at night, cautious titration) with metabolic and QTc monitoring; prefer less anticholinergic burden in delirium-prone patients.[6][14]
- Agitation/ACS bridge: short-term benzodiazepines with fall and respiratory caution; fix the cause.
- Steroid mania: coordinate dose reduction or switch strategy with rheumatology if disease control allows; add mood-stabilising or antipsychotic cover short-term.[6][11]
Subtypes and scenarios
- Psychosis as first SLE presentation — look for multi-system clues, serology, and ACR syndrome framing.[1][7]
- ACS with high disease activity — treat as emergency organic mental state.[1][5]
- aPL stroke with secondary depression — vascular plus psychosocial care.[9]
- Post-pulse steroid mania after lupus nephritis — iatrogenic pathway.[6]
- Chronic cognitive complaints in quiescent SLE — rehab, sleep, mood, vascular risk, neuropsychology; avoid endless steroids.[14]
Complications and pitfalls
Missing opportunistic infection; calling every headache primary NPSLE; giving only antipsychotics for inflammatory psychosis; ignoring APS; over-reading MRI white-matter dots; under-treating suicide risk in "understandable" lupus depression; polypharmacy EPS/QTc harm.[3][5][14]
Prognosis and disposition
SLICC data show many NP events improve, some recur, and quality of life tracks NP status. Mood disorders need longitudinal psychiatry even when not labelled primary NPSLE. Predictors of worse course include high activity, APS, delayed care, and incomplete rehabilitation.[9][10][14] Step down to shared rheumatology–CL follow-up with clear relapse triggers (new psychosis, ACS, focal neurology).
Special populations
Pregnancy/lactation: coordinate obstetrics, rheumatology, and psychiatry; aPL obstetric risk is high-stakes; many cytotoxics and some psychotropics are restricted — use pregnancy-safe ladders from specialist guidance rather than freestyle dosing.[11][12] Paediatric SLE may carry substantial NP burden — family communication and developmental framing matter. Older adults bring vascular and polypharmacy complexity. Cultural formulation never cancels organic red flags.
Evidence and regional deltas
| Source | Role in exams |
|---|---|
| ACR 1999 nomenclature | Lists 19 syndromes and case definitions |
| EULAR NPSLE 2010 (Bertsias) | Mechanism-based NP management |
| EULAR SLE 2019 / 2023 (Fanouriakis) | Overall SLE GC/immunosuppression updates |
| EULAR/ACR 2019 classification (Aringer) | Diagnosing SLE, not NP syndromes |
| Magro-Checa / Govoni–Hanly | Practical management synthesis and unmet needs |
| Isshi; DeGiorgio; Hanly SLICC | Antibody and cohort pearls |
These sources form the core exam evidence map for attribution, classification, and mechanism-based therapy.[1][2][5][6][11][12][13][14]
ANZ / RANZCP: CL service model with rheumatology co-management; local MHA principles for capacity; no single RANZCP NPSLE guideline — lean on EULAR/ACR evidence and hospital protocols.[5][12]
UK / MRCPsych / NICE-context: NICE SLE guidance sits at system level; CASC expects plain-language attribution and infection safety.[2][3]
US / ABPN / APA: ACR classification fluency; APS antithrombotic standards; malpractice-sensitive infection exclusion.[1][13]
India / MD-DNB / NEET-SS: High viva weight on ACR 19 list, anti-P, steroid psychosis, and cyclophosphamide principles.[1][4][5]
Exam pearls
- 19 syndromes ≠ automatic lupus cause.
- Attribute, then branch inflammatory vs thrombotic.
- Anti-ribosomal P supports psychosis talks — does not replace LP/infection logic.
- NR2 cross-reactive Abs are mechanism viva gold (DeGiorgio).
- Headache is common and often non-specific.
- Steroid mania is a differential, not a reason to abandon necessary immunosuppression without a joint plan.
- Normal MRI does not exclude diffuse NPSLE.
- Never invent Mental Health Act section numbers across jurisdictions.[1][5][7][8][3]
References
- [1]ACR Ad Hoc Committee on Neuropsychiatric Lupus Nomenclature The American College of Rheumatology nomenclature and case definitions for neuropsychiatric lupus syndromes Arthritis Rheum, 1999.PMID 10211873
- [2]Ainiala H, Loukkola J, Peltola J, et al. The prevalence of neuropsychiatric syndromes in systemic lupus erythematosus Neurology, 2001.PMID 11502919
- [3]Ainiala H, Hietaharju A, Loukkola J, et al. Validity of the new American College of Rheumatology criteria for neuropsychiatric lupus syndromes: a population-based evaluation Arthritis Rheum, 2001.PMID 11642640
- [4]Unterman A, Nolte JE, Boaz M, et al. Neuropsychiatric syndromes in systemic lupus erythematosus: a meta-analysis Semin Arthritis Rheum, 2011.PMID 20965549
- [5]Bertsias GK, Ioannidis JP, Aringer M, et al. EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs Ann Rheum Dis, 2010.PMID 20724309
- [6]Magro-Checa C, Zirkzee EJ, Huizinga TW, Steup-Beekman GM Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives Drugs, 2016.PMID 26809245
- [7]Isshi K, Hirohata S Association of anti-ribosomal P protein antibodies with neuropsychiatric systemic lupus erythematosus Arthritis Rheum, 1996.PMID 8814059
- [8]DeGiorgio LA, Konstantinov KN, Lee SC, et al. A subset of lupus anti-DNA antibodies cross-reacts with the NR2 glutamate receptor in systemic lupus erythematosus Nat Med, 2001.PMID 11689882
- [9]Hanly JG, Urowitz MB, Su L, et al. Prospective analysis of neuropsychiatric events in an international disease inception cohort of patients with systemic lupus erythematosus Ann Rheum Dis, 2010.PMID 19359262
- [10]Hanly JG, Su L, Urowitz MB, et al. Mood Disorders in Systemic Lupus Erythematosus: Results From an International Inception Cohort Study Arthritis Rheumatol, 2015.PMID 25778456
- [11]Fanouriakis A, Kostopoulou M, Alunno A, et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus Ann Rheum Dis, 2019.PMID 30926722
- [12]Fanouriakis A, Kostopoulou M, Andersen J, et al. EULAR recommendations for the management of systemic lupus erythematosus: 2023 update Ann Rheum Dis, 2024.PMID 37827694
- [13]Aringer M, Costenbader K, Daikh D, et al. 2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus Arthritis Rheumatol, 2019.PMID 31385462
- [14]Govoni M, Hanly JG The management of neuropsychiatric lupus in the 21st century: still so many unmet needs? Rheumatology (Oxford), 2020.PMID 33280014