Psych · Consultation-liaison psychiatry
Stroke and post-stroke psychiatry
Also known as Post-stroke depression · PSD · Poststroke depression · Stroke neuropsychiatry · Vascular depression after stroke · Post-stroke apathy
Exam-exhaustive fellowship topic on stroke and post-stroke psychiatry — post-stroke depression epidemiology and natural history, treatment and prevention evidence, lesion-location myths, apathy and psychosis, capacity, and the multidisciplinary rehab interface. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Examiners reward precise secondary nosology, honest trial literacy (prevention vs treatment vs motor recovery), myth correction on lesion location, and capacity reasoning that does not equate aphasia with incapacity.[1][6][7][9]
Definition and classification
Post-stroke depression (PSD) is a major or minor depressive syndrome temporally and clinically linked to ischaemic or haemorrhagic stroke. When the stroke is judged to be the aetiological context, DSM-5-TR framing is depressive disorder due to another medical condition; ICD-11 places analogous presentations among secondary mental or behavioural syndromes associated with diseases of the nervous system classified elsewhere.[1][7]
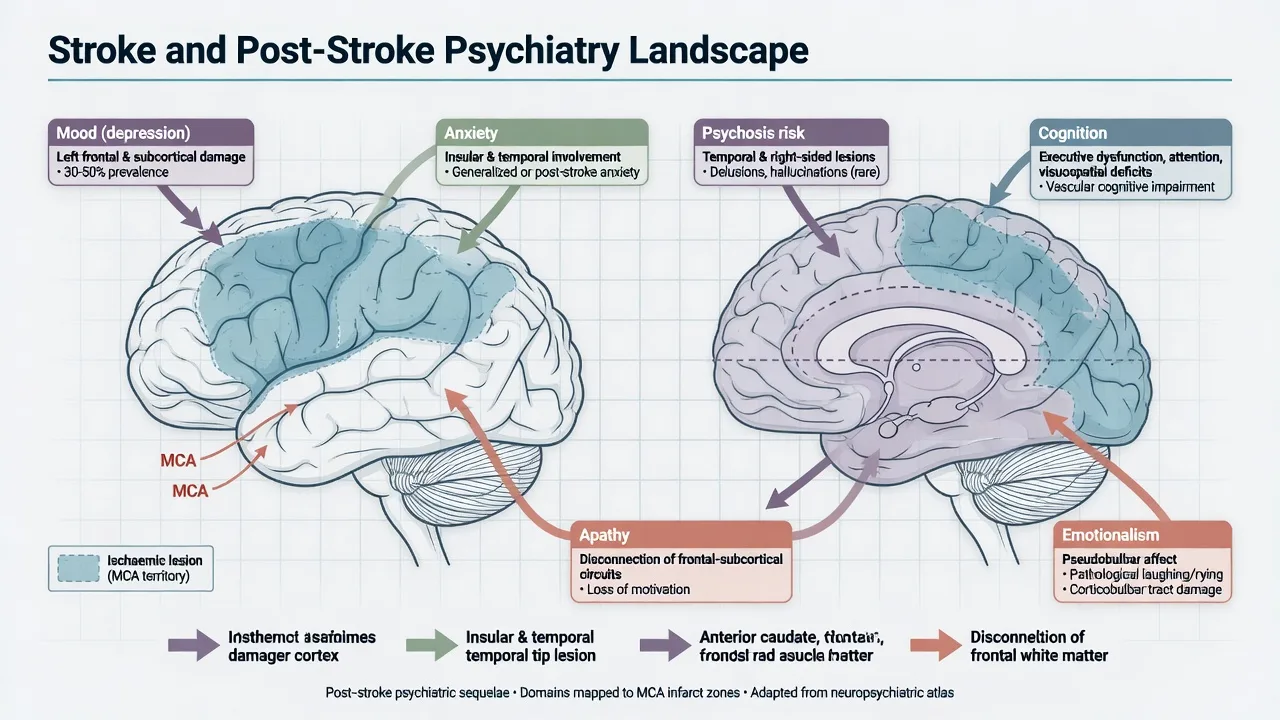
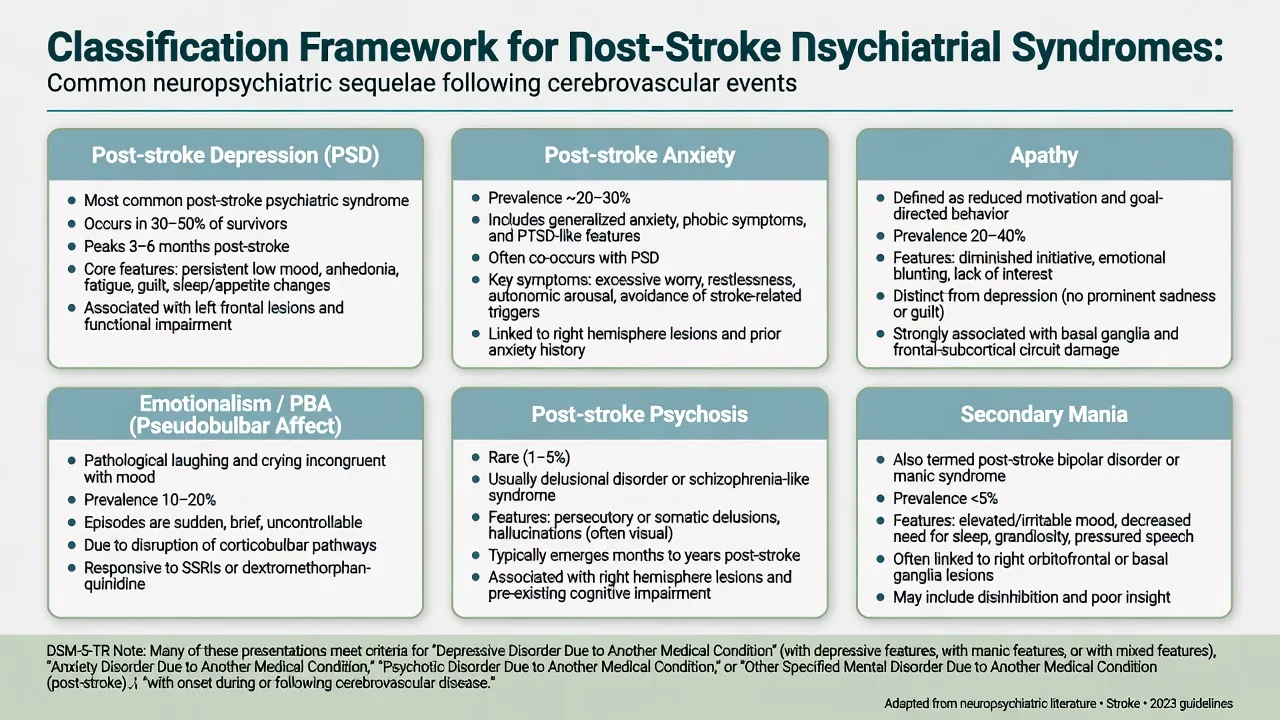
PSD is one node in a broader post-stroke psychiatric map: anxiety, apathy, emotionalism (including pseudobulbar affect patterns), uncommon post-stroke psychosis, and rare secondary mania.[1][5][17] Time course spans early hospital weeks through subacute rehab months and late community recurrence — there is no single mandatory onset day.[4][7]
| Clinical picture | Useful frame |
|---|---|
| Major depressive syndrome after stroke | Depressive disorder due to another medical condition (stroke) when causal link is clinical |
| Persistent low engagement without sadness | Apathy (may coexist with or without PSD) |
| Pathological crying/laughing out of proportion to mood | Emotionalism / PBA-spectrum — not automatic major depression |
| Delusions/hallucinations after stroke | Psychotic disorder due to another medical condition (rare; systematic review evidence) |
| Elevated/irritable mood with reduced sleep post-stroke | Secondary mania due to medical condition (teaching rarity) |
| Fluctuating attention days 1–5 | Delirium until proven otherwise — not PSD alone [1][7][17] |
Epidemiology and risk
Pooled observational data place PSD among the most common neuropsychiatric complications of stroke. Hackett and Pickles (Part I) estimated that about one-third of stroke survivors experience depression at any time after stroke — the order-of-magnitude figure examiners expect (~31% class of estimate depending on timing and method).[2] Mitchell and colleagues' meta-analysis of post-stroke mood disorders reinforces high rates of depression and anxiety and maps predictors across studies.[5] Paolucci's epidemiology review emphasises clinical burden and historically incomplete treatment pathways.[18]
Ayerbe and colleagues synthesised natural history: depression is common across the first year and beyond, with signals for poorer functional outcome and adverse prognosis when untreated or persistent.[4] Kutlubaev and Hackett (Part II) summarise predictors (greater disability, prior depression, cognitive impairment, limited social support) and the impact of depression on stroke outcome, including reduced rehab participation.[3]
Risk amplifiers examiners list: prior depression, stroke severity/disability, cognitive impairment, social isolation, pain, communication barriers, and limited social support — more reliable than any single cortical address.[3][4][5]
Mechanisms and the location myth
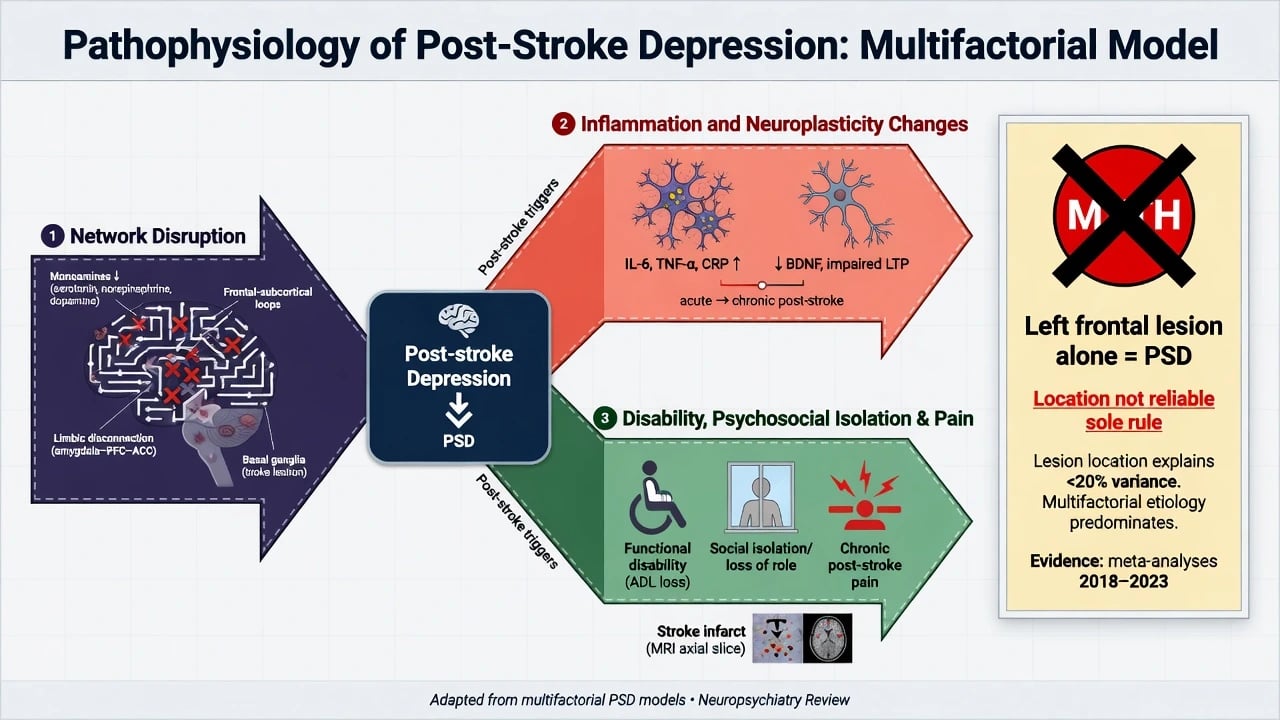
PSD is multifactorial: disruption of monoaminergic projections and frontolimbic networks, inflammatory and plasticity changes after infarction or haemorrhage, plus the psychological load of disability, role loss, and isolation.[7][8] Robinson and Jorge's modern review integrates biological and psychosocial strands without reducing PSD to one Brodmann area.[7]
Classic teaching associated left frontal and left basal-ganglia lesions with higher PSD risk. That association does not survive as a reliable standalone rule. Carson and colleagues' systematic review concluded that lesion location was not a consistent determinant of depression after stroke once methodological limits were accounted for.[6] Fellowship answers may mention the historical left-frontal story and then correct it with Carson and contemporary network framing.[6][7][8]
Clinical presentations examiners expect
Post-stroke depression
Low mood, anhedonia, guilt, hopelessness, sleep and appetite change, and suicidality may be present. Overlap with stroke-related fatigue, sleep disruption, and motor slowing means examiners reward attention to psychological depressive cognitions, diurnal mood, and loss of interest in previously valued rehab goals.[1][7] Aphasia, neglect, and anosognosia hide symptoms — collateral from family and therapists is essential.[1]
Anxiety and adjustment
Post-stroke anxiety and adjustment disorders are common companions in mood meta-analyses; fear of recurrence and health anxiety are clinically frequent on stroke units.[5]
Apathy
Apathy is reduced motivation and goal-directed behaviour that may occur without pervasive sadness. Collapsing apathy into depression leads to wrong expectations of SSRI response alone; structure, stimulation, and dopaminergic strategies (specialist) may be considered while still treating comorbid PSD when present.[1][7]
Emotionalism
Disproportionate crying or laughing can reflect emotionalism/pseudobulbar patterns. It can coexist with depression but is not synonymous with major depressive episode — clarify with mood, anhedonia, and functional history.[1]
Post-stroke psychosis
Uncommon. Stangeland and colleagues' systematic review characterises phenomenology and associations (including laterality patterns in series). Frame as psychotic disorder due to another medical condition after excluding delirium, seizure, and medication toxicity.[17]
Differential diagnosis
| Presentation | Prefer post-stroke psychiatric syndrome if… | Prefer alternative if… |
|---|---|---|
| Low mood week 3 | Anhedonia, guilt, SI, reduced therapy engagement | Pure grief without depressive syndrome |
| Non-engagement | Depressive cognitions or clear apathy pattern | Pain, untreated infection, medication sedation |
| Crying spells | Emotionalism features without full MDD | Severe PSD with pervasive hopelessness |
| New psychosis | Clear sensorium, stroke context, no drugs | Delirium, NCSE, substance, encephalitis |
| Irritability | Mood episode or frontal behavioural change | Hypoxia, retention, constipation, sleep debt |
| Discriminators | Tempo after stroke, collateral, therapy logs | Primary idiopathic syndrome only, no vascular link [1][7][17] |
Always keep delirium, recurrent stroke, seizure, endocrine/metabolic disturbance, and medication effects on the list in hospitalised patients.[1]
Assessment
Structured CL stroke psychiatry consult:[1][7]
- Stroke dossier — infarct vs haemorrhage, territory, severity/disability, aphasia/neglect/dysphagia, secondary prevention drugs (antiplatelet, anticoagulant, antihypertensive, statin).
- MSE adapted for communication limits; observe affect during therapy tasks.
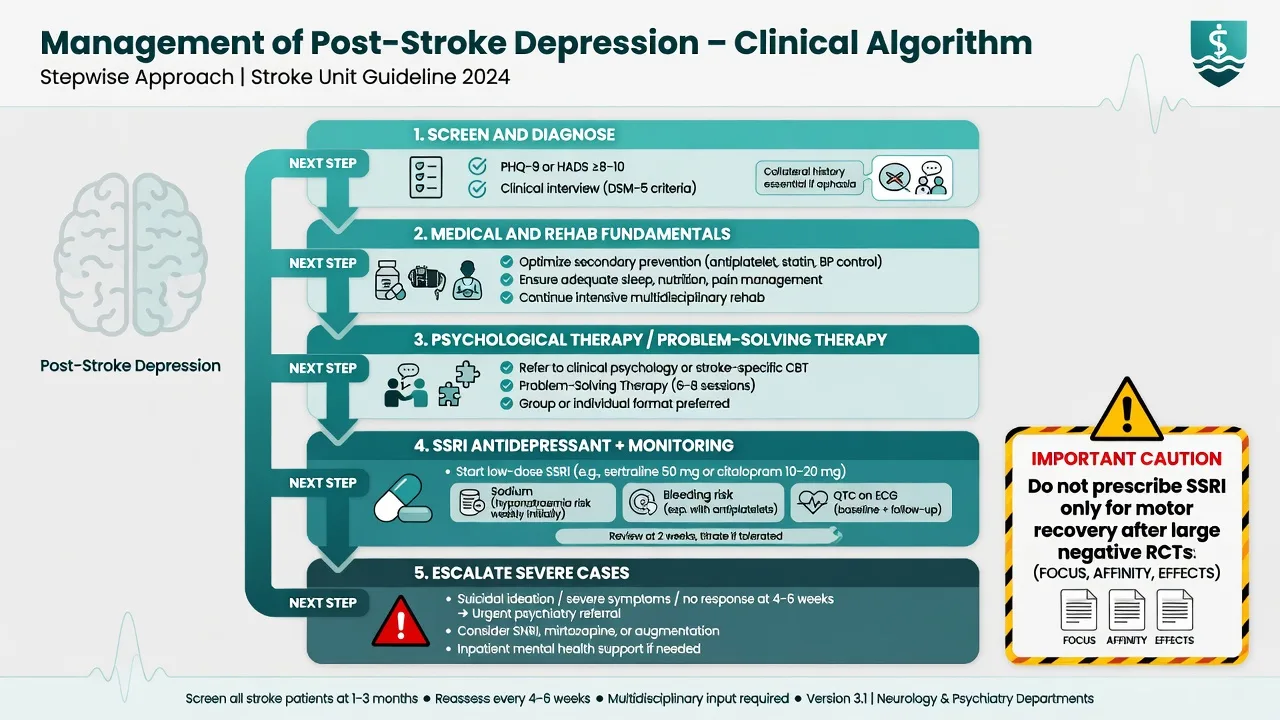
- Screening — PHQ-2/9, HADS, or similar when language allows; structured interview remains the reference standard when feasible.[1]
- Risk — suicide, self-neglect, falls, aggression, vulnerable discharge.
- Capacity — decision-specific (PEG, residential care, finances, research consent); aphasia impairs expression more than always impairing understanding — test with supported communication.[1]
- Cognition — screen and refer neuropsychology when deficits will drive goals.
Investigations are directed: review existing imaging; metabolic panel, TSH, B12, glucose, infection markers for new behavioural change; ECG and bleeding-risk context before SSRI; EEG if seizure/NCSE suspected.[1][7]
Acute safety and medical first aid
Order of operations: neurological stability and stroke pathway issues → reverse medical triggers → environmental support → least-restrictive observation for suicide/self-neglect → pharmacotherapy only as needed for safety or syndrome treatment.[1] Avoid sedative loads that erase therapy participation.
Definitive management
Multimodal foundation (all patients)
AHA/ASA scientific statement framing: recognise PSD as common and outcome-relevant; screen; treat with integrated medical, rehabilitative, psychological, and pharmacological care rather than nihilism about "understandable sadness."[1] Optimise secondary prevention adherence, sleep, pain, continence, and social support — depression care fails if the person cannot participate in rehab at all.[1][3]
Psychological therapies
Problem-solving therapy has randomised prevention evidence alongside escitalopram in non-depressed stroke patients.[9] Adapted CBT and supportive/behavioural activation approaches are used clinically with cognitive and aphasia modifications. Cochrane treatment evidence supports psychological interventions among available modalities with the usual quality caveats of stroke psychiatry trials.[11]
Antidepressant treatment
SSRIs are the most widely used pharmacological class for PSD. The 2023 Cochrane review (Allida et al.) evaluates pharmacological, psychological, non-invasive brain stimulation, and combination interventions for treating depression after stroke — know that treatment options exist and that evidence quality is mixed, not that "nothing works."[11] Robinson and Jorge summarise clinical antidepressant practice in PSD.[7]
Practical adult starting bands (individualise for age, renal/hepatic function, interactions) drawn from PSD treatment practice reviews and trial-adjacent SSRI use:[7][11]
- Escitalopram 5–10 mg oral daily (often 5 mg in older adults), titrate toward usual antidepressant range as tolerated; monitor QTc, sodium, falls, sexual side effects, and bleeding risk with antiplatelets/anticoagulants.[7][9][11]
- Sertraline 25–50 mg oral daily, titrate (often 50–150 mg range as tolerated); same class monitoring emphasis on GI effects, hyponatraemia, and bleeding.[7][11]
Review response and suicide risk within 1–2 weeks initially in hospital/rehab settings; allow full trial length before declaring failure unless intolerability or risk forces change.[1][11]
Prevention of PSD
Robinson and colleagues (JAMA 2008) showed that escitalopram or problem-solving therapy reduced the incidence of depression versus placebo in non-depressed patients after stroke — a high-yield prevention RCT.[9] Mikami et al. later reported increased first-episode PSD after discontinuation of escitalopram, supporting thoughtful duration planning rather than abrupt stop without review.[10] Cochrane prevention reviews (Allida 2020) provide a broader, more cautious synthesis — fellowship answers should not claim universal prophylaxis for every stroke survivor as mandatory standard of care, but should know the Robinson trial exists and is examinable.[12][9]
Fluoxetine and motor recovery — trial literacy
FLAME (Chollet et al.) reported a motor-recovery signal with fluoxetine after ischaemic stroke in a smaller efficacy trial, which fuelled enthusiasm for routine SSRI use for hemiparesis.[13] Large pragmatic trials FOCUS, AFFINITY, and EFFECTS subsequently tested fluoxetine for functional outcomes after acute stroke and did not support routine use for functional recovery.[14][15][16] Exam pearl: treat PSD on psychiatric grounds; do not prescribe fluoxetine solely to 'help the arm' after these neutral large trials.[14][15][16]
Psychosis and severe illness
Low-dose atypical antipsychotics for short periods when psychosis or dangerous agitation is present, with metabolic, EPS, QTc, and falls monitoring; collaborate with neurology.[17] For severe, psychotic, or treatment-refractory PSD, specialist consideration of ECT may be appropriate with individualised stroke and anaesthetic risk counselling (local pathways).[1][7]
Capacity, law, and rehab interface
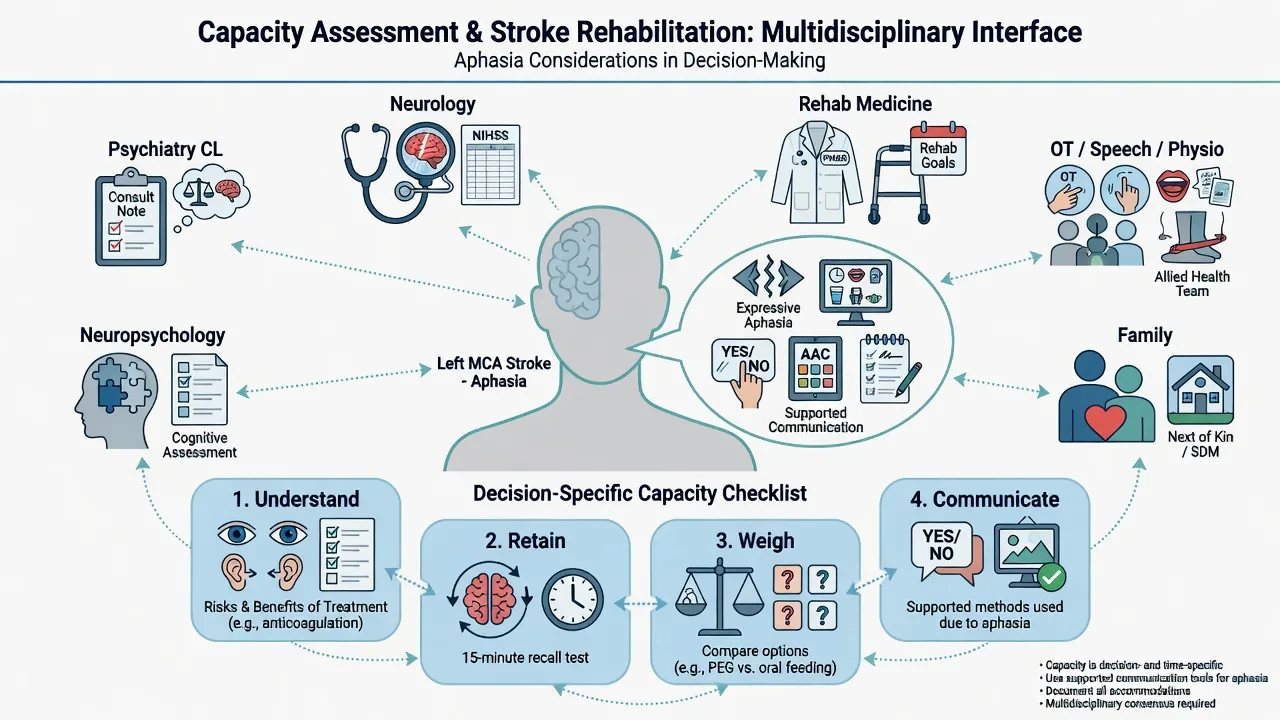
Capacity is decision- and time-specific. Aphasia complicates demonstration of understanding and communication but does not automatically abolish capacity — use supported decision-making, speech-language pathology strategies, and written/pictorial aids.[1] Depression can bias risk–benefit weighing (hopelessness → refusal of rehab or life-prolonging care); document whether depressive distortion is operating and whether treatment might restore capacity.[1][7]
Use least-restrictive local mental health, guardianship, and substitute decision-making law — do not invent section numbers across jurisdictions. Driving, firearm access, finances, and discharge destination need explicit team discussions timed to recovery.[1]
Special populations
- Severe aphasia — observational diagnosis, collateral, adapted tools.[1]
- Older adults — hyponatraemia, falls, polypharmacy, delirium overlap; start low, go slow on SSRIs.[7][11]
- Young stroke — identity, vocation, parenting, adherence to secondary prevention under mood load.[1]
- Haemorrhagic stroke — same PSD principles; blood-pressure and antithrombotic context for drug safety.[1]
- Cultural safety — interpreters, family decision structures, Indigenous health frameworks in ANZ practice.
Prognosis and disposition
PSD may remit with time and treatment, yet recurrence and chronicity are common enough that follow-up planning matters.[4] Untreated depression predicts poorer functional trajectories and higher care burden.[3][4] Disposition: stepwise rehab intensity, community CL/GP shared care, mood and suicide safety netting, and support for secondary prevention adherence.[1][18]
Regional notes
ANZ (FRANZCP primary). Practise within local acute stroke and rehabilitation pathways, RANZCP-aligned CL standards, and state/territory capacity legislation. Coordinate with stroke units, rehab medicine, and GP shared care for PSD follow-up.[1]
UK (MRCPsych). NICE stroke rehabilitation interfaces and local neuropsychiatry/CL links; CASC rewards plain-language explanation of PSD and realistic recovery without location myths.[1][6]
US (ABPN). AHA/ASA Towfighi statement is the high-visibility English-language scientific statement; trauma/stroke-centre and IRF continuum contexts appear in items.[1]
Exam pearls
STROKE-MD checklist
Bottom line for fellowship candidates
Own the epidemiology (~1 in 3), the syndrome map (PSD, anxiety, apathy, emotionalism, rare psychosis), the location myth correction, the prevention and treatment trial names, the fluoxetine motor-recovery arc (FLAME → large neutral RCTs), and the aphasia-aware capacity–rehab interface. That package answers the majority of FRANZCP, MRCPsych, ABPN, and MD/DNB questions on stroke psychiatry without a separate textbook chapter.[1][2][6][9][14]
References
- [1]Towfighi A, Ovbiagele B, El Husseini N, Hackett ML, et al. Poststroke Depression: A Scientific Statement for Healthcare Professionals From the American Heart Association/American Stroke Association Stroke, 2017.PMID 27932603
- [2]Hackett ML, Pickles K Part I: frequency of depression after stroke: an updated systematic review and meta-analysis of observational studies Int J Stroke, 2014.PMID 25117911
- [3]Kutlubaev MA, Hackett ML Part II: predictors of depression after stroke and impact of depression on stroke outcome: an updated systematic review of observational studies Int J Stroke, 2014.PMID 25156411
- [4]Ayerbe L, Ayis S, Wolfe CD, Rudd AG Natural history, predictors and outcomes of depression after stroke: systematic review and meta-analysis Br J Psychiatry, 2013.PMID 23284148
- [5]Mitchell AJ, Sheth B, Gill J, Yadegarfar M, et al. Prevalence and predictors of post-stroke mood disorders: A meta-analysis and meta-regression of depression, anxiety and adjustment disorder Gen Hosp Psychiatry, 2017.PMID 28807138
- [6]Carson AJ, MacHale S, Allen K, Lawrie SM, et al. Depression after stroke and lesion location: a systematic review Lancet, 2000.PMID 10963248
- [7]Robinson RG, Jorge RE Post-Stroke Depression: A Review Am J Psychiatry, 2016.PMID 26684921
- [8]Villa RF, Ferrari F, Moretti A Post-stroke depression: Mechanisms and pharmacological treatment Pharmacol Ther, 2018.PMID 29128343
- [9]Robinson RG, Jorge RE, Moser DJ, Acion L, et al. Escitalopram and problem-solving therapy for prevention of poststroke depression: a randomized controlled trial JAMA, 2008.PMID 18505948
- [10]Mikami K, Jorge RE, Moser DJ, Arndt S, et al. Increased frequency of first-episode poststroke depression after discontinuation of escitalopram Stroke, 2011.PMID 21868736
- [11]Allida SM, Hsieh CF, Cox KL, Patel K, et al. Pharmacological, non-invasive brain stimulation and psychological interventions, and their combination, for treating depression after stroke Cochrane Database Syst Rev, 2023.PMID 37417452
- [12]Allida S, Cox KL, Hsieh CF, House A, et al. Pharmacological, psychological and non-invasive brain stimulation interventions for preventing depression after stroke Cochrane Database Syst Rev, 2020.PMID 32390167
- [13]Chollet F, Tardy J, Albucher JF, Thalamas C, et al. Fluoxetine for motor recovery after acute ischaemic stroke (FLAME): a randomised placebo-controlled trial Lancet Neurol, 2011.PMID 21216670
- [14]FOCUS Trial Collaboration Effects of fluoxetine on functional outcomes after acute stroke (FOCUS): a pragmatic, double-blind, randomised, controlled trial Lancet, 2019.PMID 30528472
- [15]AFFINITY Trial Collaboration Safety and efficacy of fluoxetine on functional outcome after acute stroke (AFFINITY): a randomised, double-blind, placebo-controlled trial Lancet Neurol, 2020.PMID 32702334
- [16]EFFECTS Trial Collaboration Safety and efficacy of fluoxetine on functional recovery after acute stroke (EFFECTS): a randomised, double-blind, placebo-controlled trial Lancet Neurol, 2020.PMID 32702335
- [17]Stangeland H, Orgeta V, Bell V Poststroke psychosis: a systematic review J Neurol Neurosurg Psychiatry, 2018.PMID 29332009
- [18]Paolucci S Epidemiology and treatment of post-stroke depression Neuropsychiatr Dis Treat, 2008.PMID 18728805