Psych · Consultation-liaison — transplant and ICU psychiatry
Transplant and ICU psychiatry
Also known as Transplant psychiatry · Psychosocial evaluation for transplant · SIPAT · Post-intensive care syndrome · PICS · ICU PTSD · CAM-ICU psychiatry · Adherence after solid organ transplant
Exam-exhaustive fellowship reference on transplant psychiatry (pre-listing psychosocial evaluation, SIPAT/ISHLT-style domains, adherence, substance risk, immunosuppressant neuropsychiatry) and the ICU psychiatry interface (CAM-ICU/RASS/PADIS delirium pointer, fluctuating capacity, PICS and post-ICU PTSD including family). FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Fellowship examiners treat this as a dual C-L domain: (1) scarce-resource ethics plus chronic disease self-management in transplant, and (2) acute brain failure plus post-critical illness mental health in ICU. The candidate who only recites "psychosocial contraindication" or "give haloperidol for ICU agitation" fails.[1][8][11]
Definition and scope
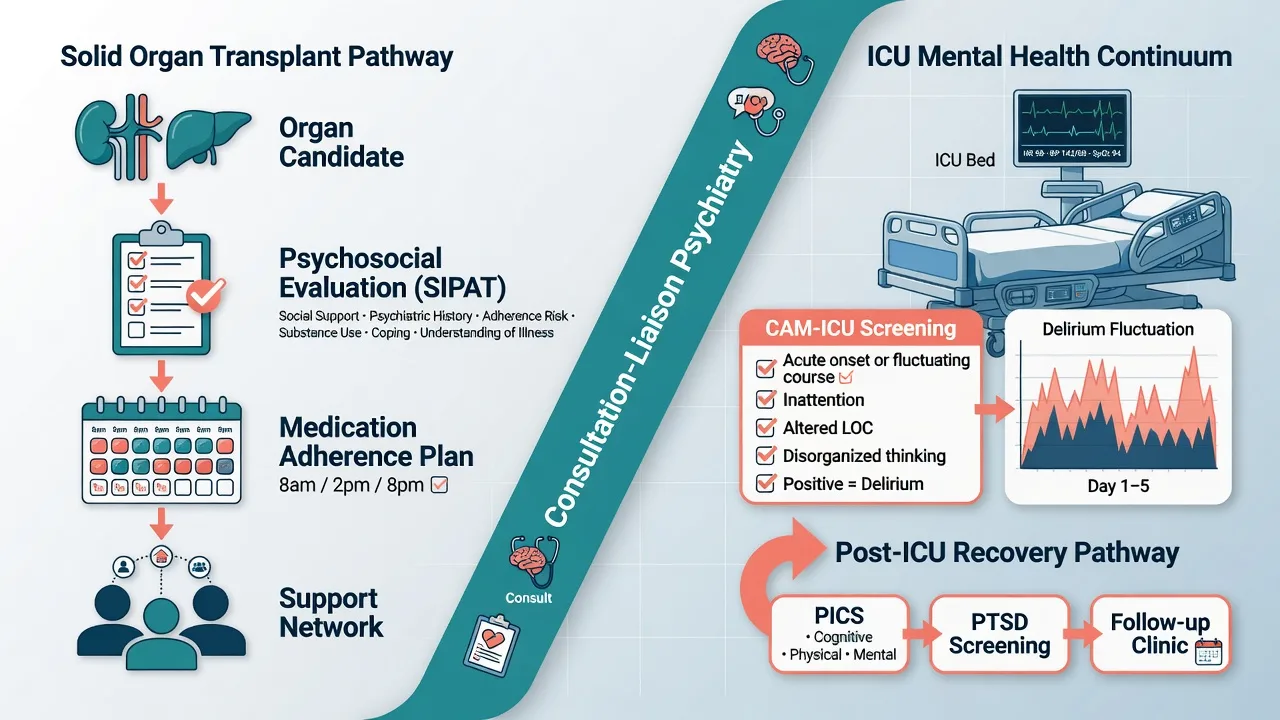
Transplant psychiatry is the psychiatric and psychosocial assessment and care of candidates and recipients of solid organ transplantation (and related advanced therapies such as durable mechanical circulatory support in cardiothoracic programmes). Core tasks: structured pre-listing evaluation, optimisation of modifiable risk, peri-operative liaison, adherence and mood surveillance, substance-use pathways, and neuropsychiatric toxicity of immunosuppression.[1][2][3]
ICU psychiatry in this topic is the interface role: delirium recognition and behavioural safety, capacity for ICU decisions, family distress, and post-ICU psychiatric sequelae — not a full rewrite of the delirium topic.[9][11][15]
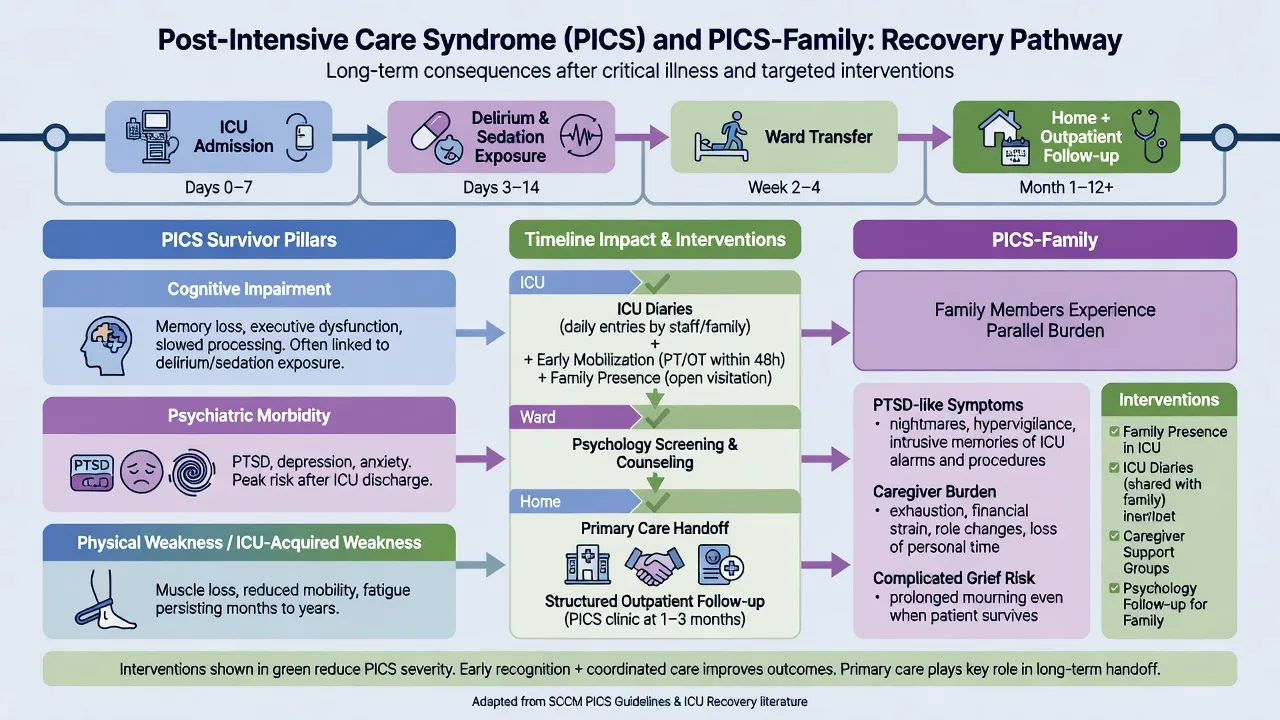
Post-intensive care syndrome (PICS) denotes new or worsening cognitive, psychiatric, and/or physical impairment after critical illness. PICS-Family (PICS-F) captures analogous morbidity in relatives (including PTSD-like symptoms and caregiver burden).[13][14][15]
Pre-transplant psychosocial evaluation
Why evaluate
Psychiatric disorders and poor self-management are associated with adverse medical outcomes after solid organ transplantation; depression and anxiety meta-analytically associate with morbidity and mortality risk after transplant.[6][8] Nonadherence to the medical regimen is common enough to be an examinable outcome pathway, not an anecdote.[5] Evaluation is therefore risk stratification plus optimisation, in the service of graft survival and fair stewardship of organs — not moral judgment.
Multisociety cardiothoracic framework (ISHLT/APM/AST and partners, 2018)
The 2018 recommendations for psychosocial evaluation of adult cardiothoracic transplant candidates and durable MCS candidates standardise domains, process, and team roles.[1][2] Exam use: name that evaluation is multidisciplinary, documented, repeatable when risk changes, and covers psychopathology, substance use, adherence and health behaviours, social support, and cognitive/understanding readiness — adapted by organ programme.
SIPAT (Stanford Integrated Psychosocial Assessment for Transplantation)
SIPAT is a structured clinician-rated tool covering readiness level, social support system, psychopathology and substance use, and lifestyle/effect of substance use, yielding a risk-oriented score profile.[3] Prospective work linked SIPAT risk strata to medical and psychosocial outcomes after transplant.[4]
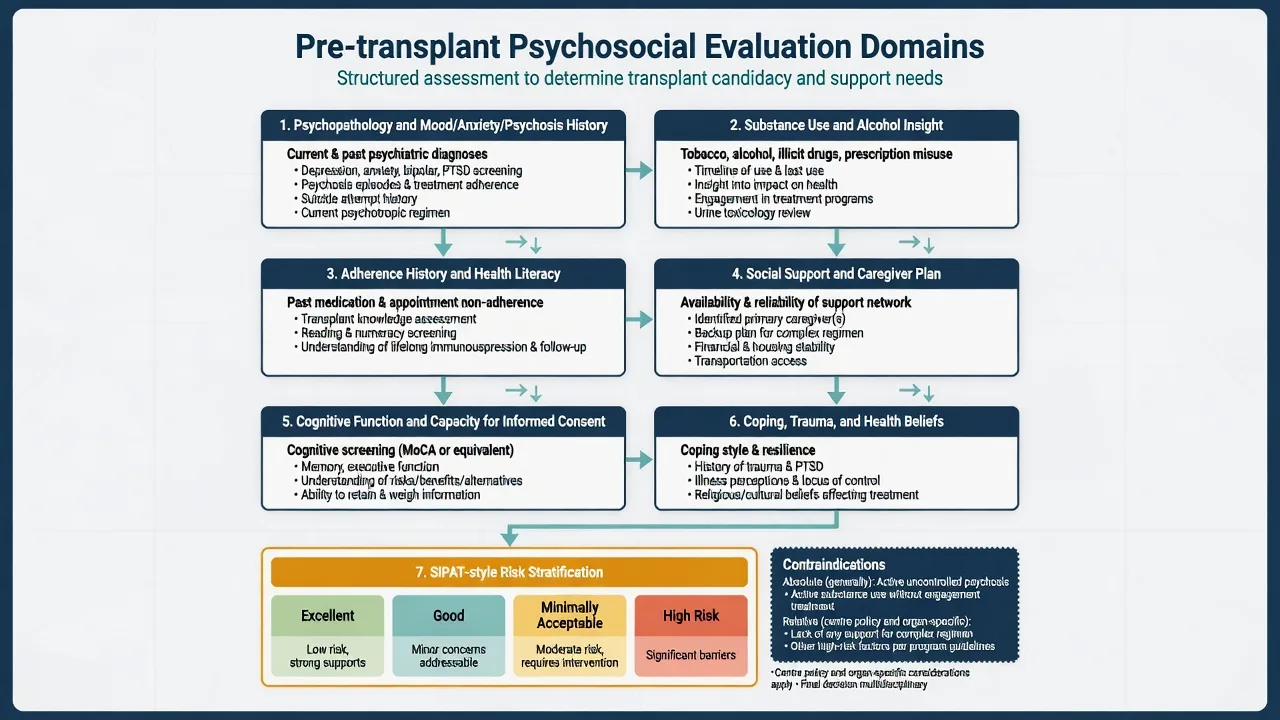
Domain checklist (exam skeleton)
| Domain | Probe | Common examiner traps |
|---|---|---|
| Psychopathology | Lifetime and current mood, anxiety, psychosis, personality, trauma, suicide attempts; treatment engagement | History alone is not automatic exclusion if stable and treated |
| Substance use | Pattern, last use, insight, treatment, collateral, programme requirements | Inventing a universal "six-month rule" as law; centres differ |
| Adherence history | Missed clinics, DNA rates, medication possession, prior graft loss | Assuming future nonadherence from one DNA without context |
| Social support | Named caregiver(s), transport, housing, finances, competing caring roles | Listing without a workable post-op care plan |
| Cognition and capacity | Encephalopathy, dementia, health literacy, teach-back for lifelong immunosuppression | Equating cognitive score alone with capacity verdict |
| Coping and health beliefs | Expectations of transplant, denial, mistrust, cultural formulation | Pathologising culturally framed illness models without exploration |
Absolute vs relative contraindications (principle level)
There is no single global psychiatric statute of absolute contraindications. Programmes commonly treat as high-barrier / often absolute until resolved: active uncontrolled psychosis or mania impairing cooperation; active substance use disorder without engagement when organ risk is high; absence of any feasible support for a complex regimen when the candidate cannot self-manage; persistent intentional nonadherence after optimisation attempts. Relative factors include treated depression, remote substance use with sustained remission and structure, limited but improvable support, and personality disorder with engagement. Always state: centre policy, organ type, and urgency modify thresholds.[1][7][8]
Adherence after transplant
Dew and colleagues' meta-analysis of adult solid organ recipients quantified nonadherence rates across regimen components and identified risk factors that map directly to exam stems (psychopathology, poor social support, substance use, younger age in many series).[5] Depression and anxiety are not "understandable reactions" to be ignored — they are outcome-linked targets.[6]
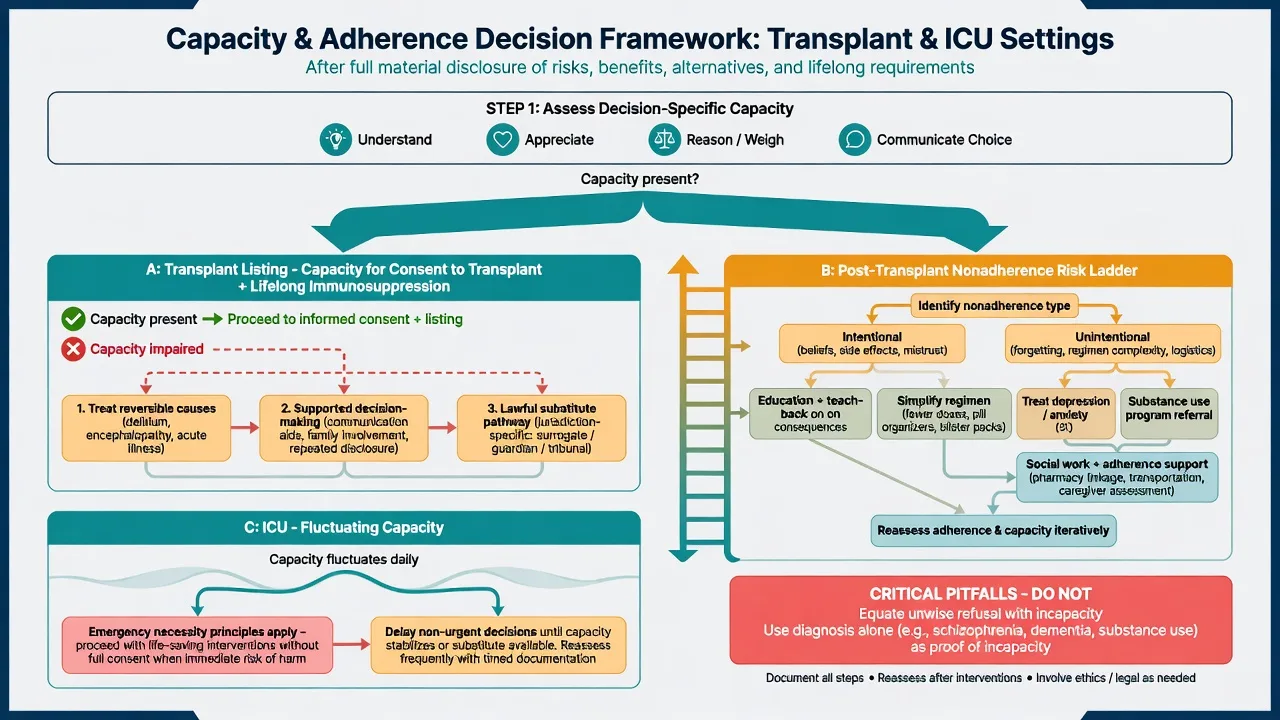
Intentional nonadherence (beliefs, side-effect aversion, distrust) vs unintentional (forgetting, complexity, cognitive impairment, cost, pharmacy access) demand different interventions.[5]
| Strategy | Target |
|---|---|
| Education + teach-back | Knowledge and health literacy gaps |
| Regimen simplification / blister packs / reminders | Unintentional forgetting |
| Treat depression/anxiety; review sedating polypharmacy | Motivation, cognition, energy |
| Motivational interviewing; address side-effect beliefs | Intentional nonadherence |
| Substance treatment programme linkage | Relapse-driven nonadherence |
| Social work / peer support / transport | Structural barriers |
| Closer clinic/pharmacy monitoring after rejection or DNA cluster | High-risk windows |
Substance use and organ-specific notes
Meta-analytic data show meaningful risk of return to substance use after liver and other solid organ transplantation; risk is not uniform and is modified by pre-transplant patterns and support.[7] Alcohol-associated liver disease remains a high-yield stem: assess insight, engagement, social network drinking, prior treatment response, and post-listing monitoring plan. Fixed abstinence durations are programme- and guideline-context dependent — do not invent a universal legal number in viva.[1][7]
Living-donor and dual-candidate family systems need explicit boundary and coercion screening (principle: free, informed, uncoerced donation) without inventing local statute numbers.[1][17]
Immunosuppressant neuropsychiatry
Calcineurin inhibitors (e.g. tacrolimus/ciclosporin class) and other immunosuppressants can cause tremor, headache, insomnia, mood change, psychosis, seizures, and posterior reversible encephalopathy spectrum presentations — coordinate levels, blood pressure, electrolytes, and imaging with the transplant team before a primary psychosis label.[20] High-dose corticosteroids commonly drive insomnia, irritability, mania-like states, and less often frank psychosis; management is medical dose strategy plus short-term psychiatric support, not automatic lifelong antipsychotic commitment.[20]
ICU delirium — psychiatry pointer
Full delirium nosology lives in the dedicated delirium topic. For this interface (RASS then CAM-ICU, PADIS-informed care):[9][10][11]
- Sedation/arousal first — Richmond Agitation-Sedation Scale (RASS) is validated in adult ICU patients.[10]
- CAM-ICU — validated for delirium in mechanically ventilated patients when the patient is sufficiently arousable; features operationalise acute change/fluctuation, inattention, disorganised thinking, and altered consciousness.[9]
- Motor subtype — hypoactive disease is under-recognised and examinable.[9][11]
- PADIS 2018 — multi-society ICU guidelines on pain, agitation/sedation, delirium, immobility, and sleep disruption prioritise prevention bundles and non-pharmacological strategies; routine antipsychotic treatment of delirium is not supported as syndrome-modifying care.[11]
- Long-term cognition — a large cohort (BRAIN-ICU lineage) demonstrated substantial long-term cognitive impairment after critical illness, with delirium as a key associated exposure.[12]
Psychiatry's value-add: behavioural formulation, capacity, family communication, psychotropic review for deliriogenic load, and follow-up for PICS psychiatric domains.[9][11][15]
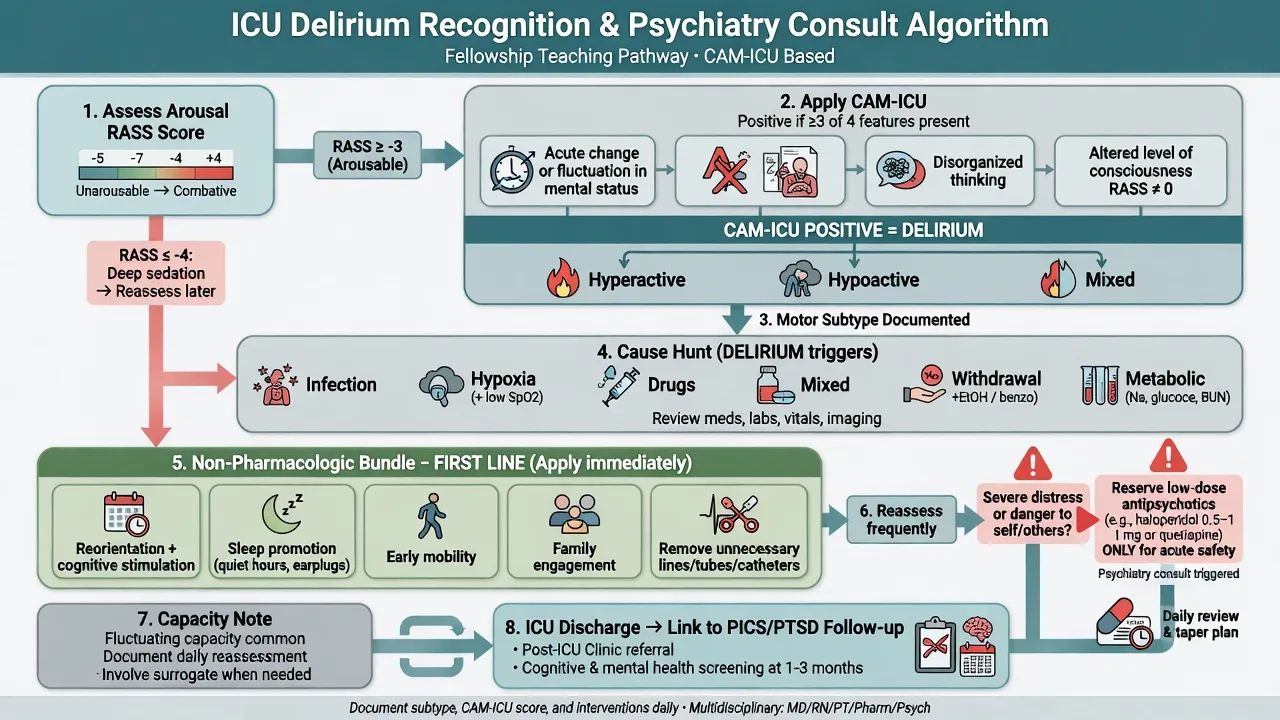
Behavioural emergency ladder (principle)
Protect airway devices and lines; reduce stimulation; reorient; treat pain, hypoxia, hypoglycaemia, withdrawal, constipation, urinary retention; review drug chart. Reserve low-dose short-term antipsychotics only for severe distress or dangerous agitation after medical causes are addressed, with daily review — align with local ICU protocol and PADIS-informed practice.[11] Agent choice must respect QTc, Parkinsonism risk, hepatic/renal failure, and interactions with transplant drugs when relevant.[11][20]
PTSD after ICU and PICS
Systematic reviews and a meta-analysis show PTSD symptoms are common among general ICU survivors; prevalence estimates vary by instrument and timing but are high enough to mandate screening pathways.[13][14] Clinical features: intrusive memories of ICU (often delusional memories of harm), nightmares, avoidance of hospitals/clinics (adherence risk after transplant), hyperarousal, guilt, and depression comorbidity.
PICS bundles cognitive impairment (see long-term cognition data), psychiatric morbidity, and physical disability into a survivorship frame useful for discharge planning.[12][13] PICS-F recognises relatives' PTSD-like symptoms, anxiety, depression, and complicated grief risk.[15]
A randomised trial found ICU diaries reduced new-onset PTSD after critical illness — an examinable non-drug intervention to name alongside early mobilisation, family presence policies, and post-ICU clinics.[16]
Management principles for post-ICU PTSD
- Validate that perceptual ICU experiences were real-to-the-patient even when factually distorted by delirium.
- Screen with trauma-aware questions; offer trauma-focused psychological therapy when PTSD criteria are met and medical stability allows.
- Treat comorbid depression/anxiety; minimise avoidable re-traumatisation in clinics (explain devices, offer control).
- Involve families; screen caregivers.
- For transplant recipients, hospital avoidance is an adherence emergency.[13][14][15][16]
Capacity in transplant and ICU
Capacity is decision-specific and time-specific. The four functional abilities remain: understand relevant information; appreciate the situation and consequences for oneself; reason (use or weigh) options; communicate a choice — after material disclosure.[17][18] Medical inpatients have substantial rates of incapacity when systematically assessed; cognitive impairment and acute illness drive risk.[19]
| Decision | Capacity nuances |
|---|---|
| Listing / transplant consent | Lifelong immunosuppression, rejection risk, infection risk, lifestyle change; teach-back mandatory |
| ICU procedures / ventilation | Often fluctuating; assess at best lucidity; emergency necessity when incapacity + serious harm |
| Research in ICU/transplant | Stricter standards; lawful representative frameworks jurisdiction-specific |
| Discharge against advice post-ICU | Separate decision from prior intubation consent |
Supported decision-making first: quieter environment, simpler language, visual aids, timing off sedation peaks, interpreter, family as support not automatic substitute. Substitute pathways and emergency necessity rules are jurisdiction-specific — do not invent section numbers.[17][19]
Mental health legislation may authorise compulsory psychiatric treatment when statutory criteria are met; it does not automatically authorise solid organ transplantation or all ICU procedures.[17]
Differential diagnosis discriminators
| Presentation | Prefer | Against |
|---|---|---|
| Acute psychosis post-transplant | CNI/steroid toxicity, infection, metabolic, PRES-spectrum | Primary schizophrenia onset at age of transplant without tox work-up |
| Low mood in ICU | Hypoactive delirium, untreated pain, steroids withdrawal, true depression | Assuming depression without attention testing |
| Flashbacks after ICU | PTSD / acute stress | Ongoing delirium if still fluctuating inattention |
| Missed doses | Depression, cognition, cost, beliefs, substance | "Personality" as only explanation |
| Refuses listing | Capable values-based refusal | Incapacity from encephalopathy without teach-back attempt |
Investigations (psychiatry role)
- Cognitive screen when encephalopathy/dementia suspected; neuropsychology for contested complex listing if time allows.
- Alcohol/drug testing as programme protocol, not as a moral test.
- Delirium cause panel owned by ICU/medicine; psychiatry audits deliriogenic medications.
- Immunosuppressant levels and neurology work-up when toxicity suspected.[1][20]
Management summary
Transplant pathway
- Structured evaluation (ISHLT-style domains / SIPAT).
- Optimise depression, psychosis, substance engagement, support, literacy.
- Multidisciplinary listing decision with transparent documentation of residual risk.
- Post-transplant: monitor mood, adherence, substance, toxicity.
- Escalate psychosocial intensity after rejection, DNA clusters, or new psychiatric illness.[1][3][5][6]
ICU pathway
- RASS → CAM-ICU; subtype; causes; non-drug bundle.
- Limited, reviewed psychotropics for danger/distress only.
- Capacity per decision; family communication; PICS-F awareness.
- Survivorship plan: cognition, PTSD/depression screen, rehab, diary where used.[9][10][11][16]
Special populations
- Adolescents/young adults: transition nonadherence risk; peer identity vs regimen.
- Older candidates: frailty, mild cognitive impairment, caregiver dyad capacity.
- Intellectual disability: supported decision-making; optimise supports — not automatic exclusion.
- Cultural and Indigenous contexts: formulation of support networks, trust, and illness meaning in listing discussions.
- Pregnancy after transplant: joint obstetric-transplant-psychiatry planning for psychotropics and risk.
Evidence and guidelines (named anchors)
| Anchor | Exam use |
|---|---|
| ISHLT/APM/AST 2018 psychosocial recommendations | Domain structure for cardiothoracic/MCS evaluation |
| SIPAT (Maldonado) | Structured tool + outcome linkage |
| Dew nonadherence meta-analysis (2007) | Rates/risk factors |
| Dew depression/anxiety meta-analysis (2015) | Psychiatric risk → medical outcomes |
| Dew substance relapse meta-analysis (2008) | Post-transplant substance risk |
| CAM-ICU (Ely); RASS (Sessler) | ICU screening sequence |
| PADIS 2018 (Devlin) | ICU bundle philosophy |
| Pandharipande NEJM 2013 | Long-term cognitive impairment |
| Parker 2015; Davydow 2008 | PTSD after ICU |
| Davidson 2012 | PICS-Family |
| Jones 2010 diary RCT | Non-drug PTSD prevention signal |
| Appelbaum/Grisso; Raymont | Capacity abilities; inpatient incapacity prevalence |
| Wijdicks immunosuppressant neurotoxicity | Differential for post-transplant psychosis |
Region notes
ANZ (FRANZCP primary). C-L psychiatrists contribute to transplant MDTs; mental health acts and guardianship/capacity statutes differ by state/territory — principles only in exam answers. ICU practice aligns with international PADIS-informed bundles adapted locally.[1][11][17]
UK (MRCPsych). Capacity language often maps to MCA-style understand/retain/use-or-weigh/communicate; transplant centres apply national and centre protocols for alcohol-associated liver disease.[17][7]
US (ABPN). Programme-specific UNOS/centre psychosocial criteria; capacity is clinical with state law overlay.[1][17]
India (MD/DNB, NEET-SS). Resource and caregiver structure heavily influence listing practicality; still apply functional capacity and structured evaluation logic.[1][17]
Exam pearls
[3] [6] [9] [11] [13] [15] [17] [20]Bottom line for viva
Be the psychiatrist who can run a structured transplant psychosocial evaluation, separate optimisable from non-modifiable risk, manage adherence as a clinical outcome pathway, speak CAM-ICU/PADIS fluently without over-owning intensive care medicine, assess capacity without outcome bias, and follow survivors and families into PICS and PTSD care.[1][5][9][13][17]
References
- [1]Dew MA, DiMartini AF, Dobbels F, et al. The 2018 ISHLT/APM/AST/ICCAC/STSW Recommendations for the Psychosocial Evaluation of Adult Cardiothoracic Transplant Candidates and Candidates for Long-term Mechanical Circulatory Support Psychosomatics, 2018.PMID 30197247
- [2]Dew MA, DiMartini AF, Dobbels F, et al. The 2018 ISHLT/APM/AST/ICCAC/STSW recommendations for the psychosocial evaluation of adult cardiothoracic transplant candidates and candidates for long-term mechanical circulatory support J Heart Lung Transplant, 2018.PMID 29709440
- [3]Maldonado JR, Dubois HC, David EE, et al. The Stanford Integrated Psychosocial Assessment for Transplantation (SIPAT): a new tool for the psychosocial evaluation of pre-transplant candidates Psychosomatics, 2012.PMID 22424160
- [4]Maldonado JR, Sher Y, Lolak S, et al. The Stanford Integrated Psychosocial Assessment for Transplantation: A Prospective Study of Medical and Psychosocial Outcomes Psychosom Med, 2015.PMID 26517474
- [5]Dew MA, DiMartini AF, De Vito Dabbs A, et al. Rates and risk factors for nonadherence to the medical regimen after adult solid organ transplantation Transplantation, 2007.PMID 17460556
- [6]Dew MA, Rosenberger EM, Myaskovsky L, et al. Depression and Anxiety as Risk Factors for Morbidity and Mortality After Organ Transplantation: A Systematic Review and Meta-Analysis Transplantation, 2015.PMID 26492128
- [7]Dew MA, DiMartini AF, Steel J, et al. Meta-analysis of risk for relapse to substance use after transplantation of the liver or other solid organs Liver Transpl, 2008.PMID 18236389
- [8]Rosenberger EM, Dew MA, Crone C, et al. Psychiatric disorders as risk factors for adverse medical outcomes after solid organ transplantation Curr Opin Organ Transplant, 2012.PMID 22277955
- [9]Ely EW, Inouye SK, Bernard GR, et al. Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU) JAMA, 2001.PMID 11730446
- [10]Sessler CN, Gosnell MS, Grap MJ, et al. The Richmond Agitation-Sedation Scale: validity and reliability in adult intensive care unit patients Am J Respir Crit Care Med, 2002.PMID 12421743
- [11]Devlin JW, Skrobik Y, Gélinas C, et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU Crit Care Med, 2018.PMID 30113379
- [12]Pandharipande PP, Girard TD, Jackson JC, et al. Long-term cognitive impairment after critical illness N Engl J Med, 2013.PMID 24088092
- [13]Parker AM, Sricharoenchai T, Raparla S, et al. Posttraumatic stress disorder in critical illness survivors: a metaanalysis Crit Care Med, 2015.PMID 25654178
- [14]Davydow DS, Gifford JM, Desai SV, et al. Posttraumatic stress disorder in general intensive care unit survivors: a systematic review Gen Hosp Psychiatry, 2008.PMID 18774425
- [15]Davidson JE, Jones C, Bienvenu OJ Family response to critical illness: postintensive care syndrome-family Crit Care Med, 2012.PMID 22080636
- [16]Jones C, Bäckman C, Capuzzo M, et al. Intensive care diaries reduce new onset post traumatic stress disorder following critical illness: a randomised, controlled trial Crit Care, 2010.PMID 20843344
- [17]Appelbaum PS Clinical practice. Assessment of patients' competence to consent to treatment N Engl J Med, 2007.PMID 17978292
- [18]Appelbaum PS, Grisso T Assessing patients' capacities to consent to treatment N Engl J Med, 1988.PMID 3200278
- [19]Raymont V, Bingley W, Buchanan A, et al. Prevalence of mental incapacity in medical inpatients and associated risk factors: cross-sectional study Lancet, 2004.PMID 15488217
- [20]Wijdicks EF Neurotoxicity of immunosuppressive drugs Liver Transpl, 2001.PMID 11699028