Psych · Consultation-liaison psychiatry
Traumatic brain injury psychiatry
Also known as TBI psychiatry · Neuropsychiatry of head injury · Post-concussion syndrome · Organic personality change after TBI · Post-traumatic psychosis
Exam-exhaustive fellowship topic on traumatic brain injury psychiatry — severity staging, post-concussion symptom complexes, depression and mania after TBI, personality change, delayed psychosis, aggression management (beta-blockers first-line when indicated), capacity, and the rehab multidisciplinary interface. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Examiners reward precise nosology (secondary syndromes, not vague "organic brain syndrome"), medical first-aid for agitation, honest SSRI trial evidence, beta-blocker priority for aggression, and capacity analysis that captures frontal dysexecutive risk.[4][7][12][17]
Definition and severity
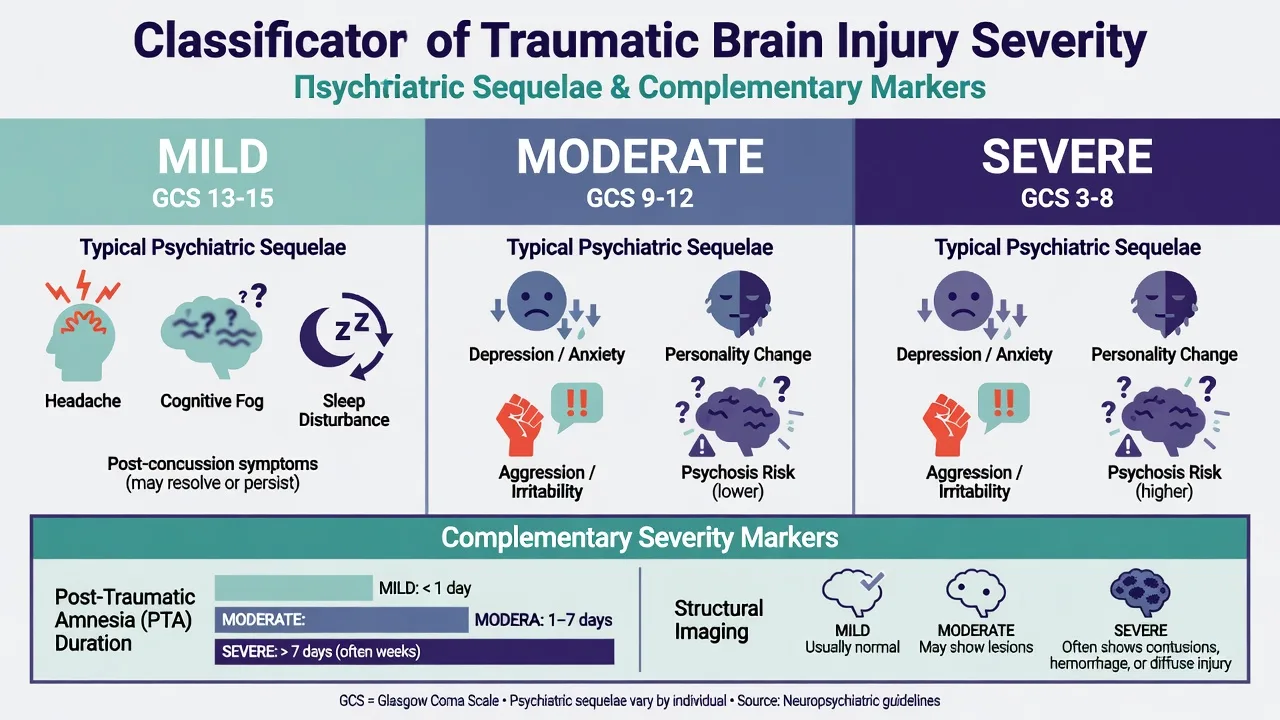
Traumatic brain injury (TBI) is an alteration in brain function, or other evidence of brain pathology, caused by an external force (Menon position statement).[1] Severity is conventionally staged with the Glasgow Coma Scale: mild GCS 13–15, moderate 9–12, severe 3–8, complemented by post-traumatic amnesia (PTA) duration and structural imaging findings.[2][3]
Global care and research still face gaps in prevention, acute pathways, and long-term neuropsychiatric outcomes — the psychiatry interface is not optional decoration after neurosurgery discharge.[3][16]
DSM-5-TR and ICD-11 framing
Use secondary constructs, not invented free-standing codes.[16][17][20]
| Clinical picture | Useful frame |
|---|---|
| Enduring cognitive decline after TBI | Major or mild neurocognitive disorder due to TBI |
| Enduring frontal/behavioural change | Personality change due to another medical condition |
| Mood episode causally linked to TBI | Depressive or bipolar and related disorder due to another medical condition |
| Psychosis causally linked to TBI | Psychotic disorder due to another medical condition |
| Acute fluctuating confusion | Delirium and/or evolving PTA — not "new schizophrenia" |
| Secondary syndrome framing (reviews) | Standard CL neuropsychiatry approach [16][17][20] |
ICD-11 similarly places many presentations as secondary mental or behavioural syndromes associated with diseases classified elsewhere. "Post-concussion syndrome" remains a clinical phrase for a symptom complex after mild TBI; standalone PCS as a crisp DSM entity has been unstable across editions — describe symptoms and treat them rather than arguing nomenclature alone.[16][17][20]
Epidemiology and risk
Psychiatric morbidity after TBI is common and often long-lasting. In a prospective cohort, cumulative major depression approached half of patients in the first year after TBI in Bombardier and colleagues' JAMA study, with strong links to poorer functional outcomes.[5] Deb and colleagues found elevated rates of psychiatric illness at one year after TBI compared with population expectations.[14] Koponen's classic 30-year follow-up demonstrated high lifetime Axis I and II disorder rates after TBI — this is not a short-lived hospital problem only.[13]
Nationwide register data (Orlovska et al.) support head injury as a risk factor for subsequent psychiatric disorders.[15] Contemporary reviews synthesise mood, anxiety, PTSD overlap, aggression, and suicide concern as core mental-health consequences.[16][17]
Risk amplifiers examiners expect: prior psychiatric illness, substance use, greater injury severity, frontal/temporal lesion patterns, poor social support, sleep disruption, pain, and litigation or compensation complexity (especially mild TBI with persistent symptoms).[4][10][18][20]
Mechanisms (viva depth)
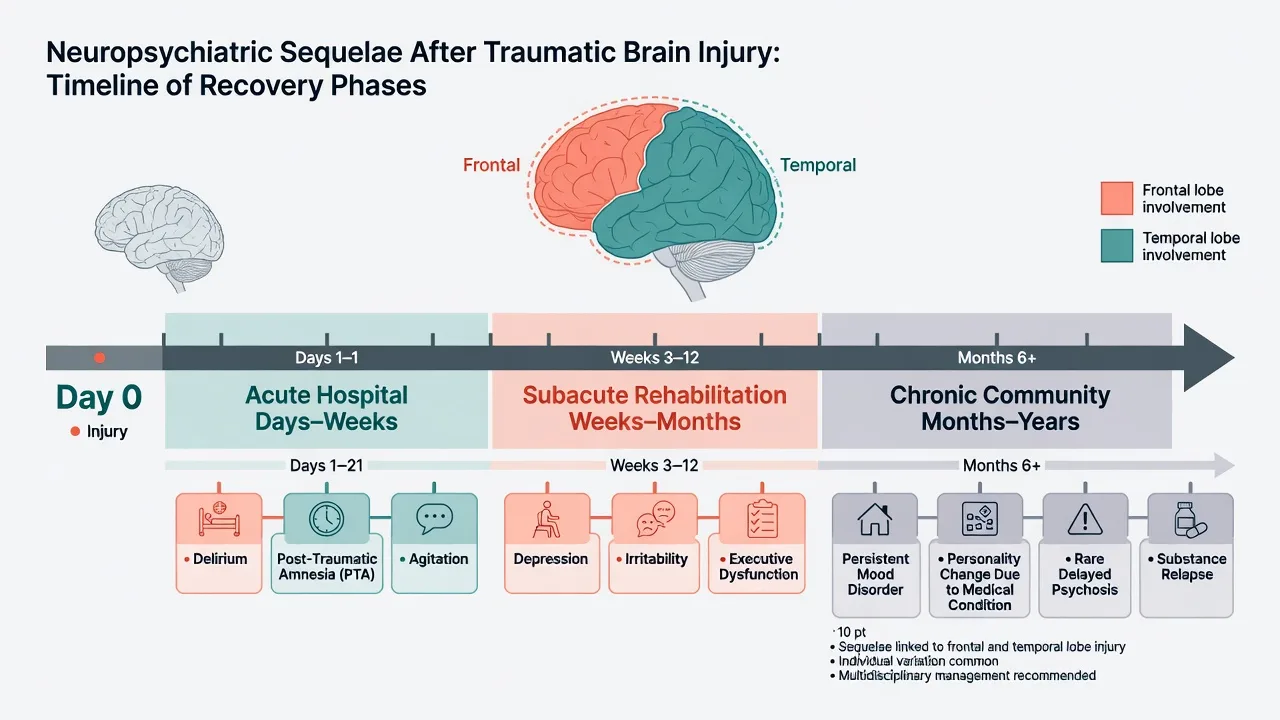
TBI combines focal contusion (orbitofrontal and temporal poles common against the skull base) with diffuse axonal injury and network disconnection. Frontolimbic circuits that regulate affect, social cognition, and impulse control are repeatedly implicated in aggression and personality change.[10][16][20] Neuroinflammation, monoamine disruption, epilepsy risk, and sleep–wake dysregulation further shape mood and behaviour.[16][17]
Psychosis after TBI is often delayed (months to years), may associate with temporal injury and seizures in literature series, and should not be forced into a same-day post-injury onset requirement.[9]
Clinical presentations examiners expect
Acute phase — PTA, confusion, agitation
During PTA and early hospitalisation patients may be confused, confabulatory, emotionally labile, and agitated. This is not personality change due to medical condition yet — document course, treat medical drivers, and avoid permanent labelling in the first days.[11][19][20]
Post-concussion symptom complex (especially after mild TBI)
Somatic (headache, dizziness, phonophobia/photophobia), cognitive (slowed processing, poor concentration), and affective (irritability, anxiety, low mood) clusters are common. Most improve; a minority have prolonged symptoms. Predictors include preinjury mental health, acute stress, and early symptom burden rather than a single imaging finding.[18][16]
Depression
Major depression is among the most frequent and treatable sequelae. Jorge and colleagues characterised post-TBI major depression and its association with executive and psychosocial dysfunction.[4] Distinguish depression from apathy, fatigue, and grief; always assess suicide risk.[5][16]
Secondary mania
Secondary mania after TBI is a classic teaching point (Jorge et al.): elevated/irritable mood, reduced need for sleep, and disinhibition with temporal relationship to injury — frame as bipolar and related disorder due to another medical condition when causal link is clinical.[8]
Personality change
Families describe a person who is "not the same": disinhibition, aggression, affective lability, or apathy. This maps to personality change due to another medical condition, not a late-onset primary personality disorder invented after the crash.[13][17][20]
Psychosis
Delusions and hallucinations with relatively clear sensorium (outside delirium) may appear, often later. Fujii's literature analyses characterise psychotic disorder due to TBI and support a structured organic formulation.[9]
Aggression and disinhibition
Aggression after TBI correlates with frontal injury patterns, depression, and poor social functioning in clinical series (Tateno et al.). It is a leading reason for CL referral on rehab units.[10]
Differential diagnosis
| Presentation | Prefer TBI-related if… | Prefer alternative if… |
|---|---|---|
| Agitation day 2 | PTA, medical triggers, fluctuating attention | Primary mania without injury context |
| Low mood month 2 | Anhedonia, guilt, suicidality post-injury | Pure apathy without depressive cognitions |
| "Personality ruin" | Frontal disinhibition after documented TBI | Pre-existing antisocial pattern unchanged |
| Psychosis year 3 | Temporal injury, seizures, atypical age onset | Classic primary schizophrenia prodrome only |
| Persistent mild-TBI symptoms | Mixed somatic-cognitive-affective cluster | Untreated migraine, sleep apnoea, PTSD alone |
| Discriminators (reviews) | Frontotemporal injury pattern, tempo, collateral | Primary idiopathic syndromes without TBI link [16][17][20] |
Always consider substance use, seizure, endocrine sequelae (post-traumatic hypopituitarism), and concurrent PTSD/adjustment when trauma mechanism was assault or crash.[16][17][20]
Assessment
Structured approach to the CL TBI consult:[17][20]
- Injury dossier — mechanism, LOC, GCS nadir, PTA length, imaging/ops, seizures, current anticonvulsants and other meds.[1][2]
- MSE — attention, executive function, mood, affect regulation, insight, risk to self/others.[20]
- Cognitive screen plus neuropsychology for rehab planning when deficits will drive disposition.[17][20]
- Risk — suicide, violence, vulnerability, absconding, driving, childcare.[16][5]
- Capacity — decision-specific; dysexecutive patients may verbalise options without true weighing of consequences (see capacity topic for legal frameworks — statutes are jurisdiction-specific).[20]
- Outcome frame — GOSE-style global outcome thinking for moderate–severe TBI recovery conversations.[3]
Investigations are directed, not shotgun: review existing neuroimaging; EEG if seizure/NCSE; metabolic panel, thyroid, B12, toxicology as indicated; medication rationalisation; sleep and endocrine review when clinically suggested.[20]
Acute behavioural emergency
Order of operations: ABCDE and neurosurgical stability → identify reversible triggers → environmental de-escalation → least restrictive observation → pharmacotherapy only if needed for safety.[11][19][12] When rapid tranquillisation is unavoidable, use the lowest effective dose of a familiar agent, minimise anticholinergic and heavy benzodiazepine load in non-withdrawal settings, and reassess frequently — TBI brains are sensitive to sedation and EPS.[19][12]
Definitive management by syndrome
Post-concussion care
Education that symptoms are common and usually improve; graded return to cognitive and physical activity; treat migraine-pattern headache, sleep, anxiety, and mood; avoid prolonged total rest and catastrophic narratives. Address compensation stress and workplace re-entry practically.[18][16]
Depression
Psychological therapies adapted to cognitive load plus antidepressants when moderate–severe. Sertraline is the most exam-visible SSRI in TBI trials.[4][6][7]
- Jorge et al. (JAMA Psychiatry 2016): sertraline for prevention of mood disorders after TBI — know that prevention trials exist and interpret effect sizes carefully rather than claiming universal prophylaxis.[6]
- Fann et al. (2017 RCT): sertraline for major depression in the year after TBI — first-line SSRI choice is supported by dedicated trial attention even when results are nuanced.[7]
Practical dosing start (adult, adjust for age/comorbidity): sertraline 25–50 mg oral daily, titrate toward usual antidepressant range (often 50–150 mg) with monitoring for GI effects, hyponatraemia risk in older adults, bleeding risk with antiplatelets, activation/suicidality early in treatment, and seizure threshold concerns. Avoid bupropion when seizure risk is high. Review at 2–4 weeks for response and risk.[6][7][20]
Mania
Treat secondary mania with mood stabilisers and/or atypical antipsychotics as clinically indicated, address sleep, and exclude substance triggers; document organic framing.[8][20]
Psychosis
Lowest effective dose of an atypical antipsychotic, metabolic and EPS monitoring, seizure threshold awareness, and collaboration with neurology if epilepsy coexists. Do not delay organic work-up for "first-episode psychosis pathway only" thinking when history is TBI-laden and atypical.[9][20]
Aggression and behavioural dyscontrol
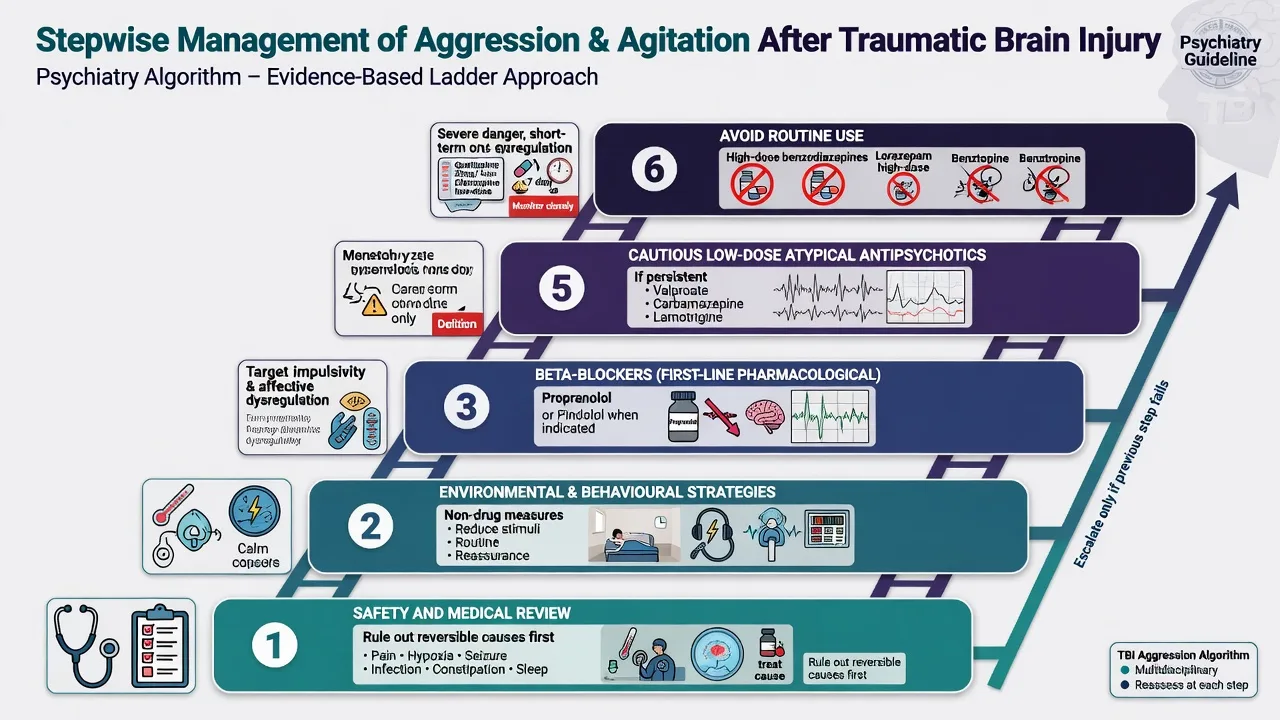
Evidence-informed ladder for post-TBI aggression after medical stabilisation:[12][19]
- Treat medical and environmental drivers; structure the day; reduce overstimulation; consistent behavioural contingencies with rehab psychology.[11][12]
- Beta-blockers — preferred pharmacological class for many post-TBI aggression/agitation scenarios in systematic reviews and French expert recommendations (Plantier/SOFMER), building on older trial work (e.g. Brooke on early agitation treatment; beta-blocker literature including pindolol-class studies in organic aggression).[11][12][19]
- Propranolol example pathway (adult, specialist-supervised): start low (e.g. 20 mg oral two to three times daily or equivalent local protocol), titrate toward response while monitoring BP/HR, bronchospasm risk, depression, sleep, and glucose; withhold if unstable cardiovascular status. Exact targets vary — cite local formulary and cardiology co-management when comorbid heart disease.[12][19]
- Anticonvulsants / mood stabilisers (e.g. valproate, carbamazepine, or other agents per comorbidity and seizure history) when affective instability or epilepsy interface dominates — check bloods, interactions, teratogenicity.[12][19]
- Atypical antipsychotics short-term for severe danger or psychotic aggression (e.g. quetiapine 25–50 mg, olanzapine 2.5–5 mg, or risperidone 0.25–0.5 mg starting bands in sensitive brains — individualise), with QTc/metabolic/EPS monitoring; avoid chronic high-dose "chemical restraint" for personality change.[12][19][20]
- Avoid routine long-term benzodiazepines and anticholinergics for behaviour control.[12][19]
Personality change and apathy
Drugs help associated mood, psychosis, or dangerous aggression more than pure character change. Core treatments are environmental structure, family education, behavioural rehab, vocational adaptation, and sometimes stimulant or dopaminergic strategies for apathy under specialist oversight (evidence thinner — do not invent doses).[17][20]
Substance use
Alcohol and other substances both cause injury and sabotage recovery — integrate dual-diagnosis care early.[16][14]
Capacity, law, and rehab interface
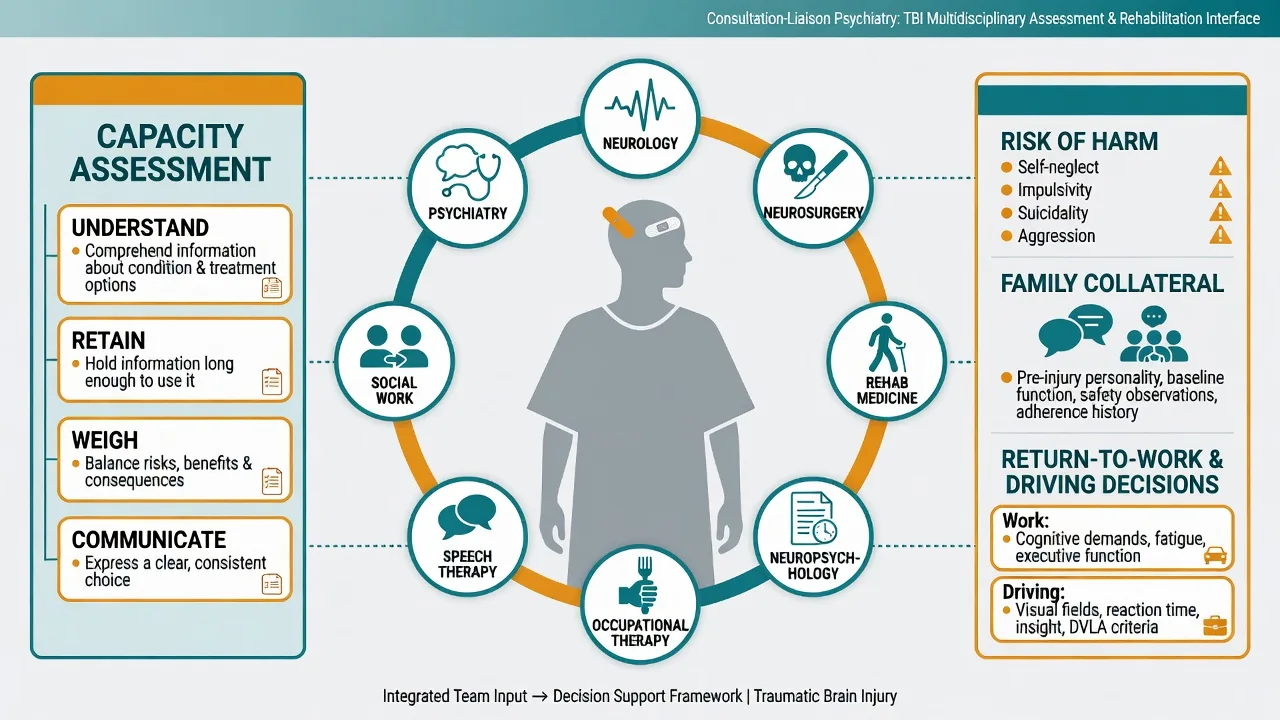
Capacity is decision- and time-specific. A patient oriented to place may still fail to weigh discharge risks after frontal injury. During PTA or delirium, major financial and legal acts are generally inappropriate. Use least-restrictive local mental health, guardianship, and substitute decision-making statutes — do not invent section numbers across jurisdictions.[20][3]
Driving, firearm access, childcare, and workplace safety need explicit risk conversations with the treating team. GOSE and functional goals orient realistic hope without premature permanent pessimism.[3]
Special populations
- Children/adolescents — developmental impact, school re-entry, family system stress.[16]
- Older adults — falls, anticoagulation bleeds, delirium, dementia interaction.[3]
- Forensic interface — disentangle post-TBI personality change from pre-injury antisocial traits when responsibility and risk are examined.[13][17]
- Cultural safety — interpreters, family decision structures, and Indigenous health frameworks in ANZ practice.
Prognosis and disposition
Most people with mild TBI recover substantially; persistent symptoms cluster in those with high early symptom load and psychosocial risk factors.[18] Moderate–severe TBI more often leaves lasting cognitive–behavioural disability; psychiatric disorders may persist for decades.[13][3] Depression treatment and aggression control improve participation in rehab and community reintegration.[5][10]
Disposition: stepwise rehab intensity, community neuropsychiatry follow-up, substance treatment, vocational and family support, and clear crisis plans for suicide or violence risk.[16][20]
Regional notes
ANZ (FRANZCP primary). Practise within local CL–rehab pathways, RANZCP-aligned professionalism, and state/territory capacity and mental health legislation. Coordinate with brain injury rehabilitation services and GP shared care.[3][20]
UK (MRCPsych). NICE head-injury pathways and local neuropsychiatry/rehab networks; CASC rewards plain-language family explanation of personality change and realistic recovery timelines.[3]
US (ABPN). Trauma-centre and rehab continuum; APA neuropsychiatry framing; insurance and medicolegal PCS contexts are frequent exam distractors — keep medicine first.[16][17]
Exam pearls
TBI-PSYCH checklist
Bottom line for fellowship candidates
Own the severity stage, the syndrome map (PCS, depression, mania, personality change, psychosis, aggression), the drug ladder with cited limits, and the capacity–rehab interface. That package answers the majority of FRANZCP, MRCPsych, ABPN, and MD/DNB organic-psychiatry questions on TBI without needing a separate textbook chapter.[3][5][12][16][17]
References
- [1]Menon DK, Schwab K, Wright DW, et al. Position statement: definition of traumatic brain injury Arch Phys Med Rehabil, 2010.PMID 21044706
- [2]Teasdale G, Jennett B Assessment of coma and impaired consciousness. A practical scale Lancet, 1974.PMID 4136544
- [3]Maas AIR, Menon DK, Manley GT, et al. Traumatic brain injury: progress and challenges in prevention, clinical care, and research Lancet Neurol, 2022.PMID 36183712
- [4]Jorge RE, Robinson RG, Moser D, et al. Major depression following traumatic brain injury Arch Gen Psychiatry, 2004.PMID 14706943
- [5]Bombardier CH, Fann JR, Temkin NR, et al. Rates of major depressive disorder and clinical outcomes following traumatic brain injury JAMA, 2010.PMID 20483970
- [6]Jorge RE, Acion L, Burin DI, et al. Sertraline for Preventing Mood Disorders Following Traumatic Brain Injury: A Randomized Clinical Trial JAMA Psychiatry, 2016.PMID 27626622
- [7]Fann JR, Bombardier CH, Temkin N, et al. Sertraline for Major Depression During the Year Following Traumatic Brain Injury: A Randomized Controlled Trial J Head Trauma Rehabil, 2017.PMID 28520672
- [8]Jorge RE, Robinson RG, Starkstein SE, et al. Secondary mania following traumatic brain injury Am J Psychiatry, 1993.PMID 8494069
- [9]Fujii D, Ahmed I Characteristics of psychotic disorder due to traumatic brain injury: an analysis of case studies in the literature J Neuropsychiatry Clin Neurosci, 2002.PMID 11983787
- [10]Tateno A, Jorge RE, Robinson RG Clinical correlates of aggressive behavior after traumatic brain injury J Neuropsychiatry Clin Neurosci, 2003.PMID 12724455
- [11]Brooke MM, Patterson DR, Questad KA, et al. The treatment of agitation during initial hospitalization after traumatic brain injury Arch Phys Med Rehabil, 1992.PMID 1417466
- [12]Plantier D, Luauté J, SOFMER group Drugs for behavior disorders after traumatic brain injury: Systematic review and expert consensus leading to French recommendations for good practice Ann Phys Rehabil Med, 2016.PMID 26797170
- [13]Koponen S, Taiminen T, Portin R, et al. Axis I and II psychiatric disorders after traumatic brain injury: a 30-year follow-up study Am J Psychiatry, 2002.PMID 12153823
- [14]Deb S, Lyons I, Koutzoukis C, et al. Rate of psychiatric illness 1 year after traumatic brain injury Am J Psychiatry, 1999.PMID 10080551
- [15]Orlovska S, Pedersen MS, Benros ME, et al. Head injury as risk factor for psychiatric disorders: a nationwide register-based follow-up study of 113,906 persons with head injury Am J Psychiatry, 2014.PMID 24322397
- [16]Howlett JR, Nelson LD, Stein MB Mental Health Consequences of Traumatic Brain Injury Biol Psychiatry, 2022.PMID 34893317
- [17]Silver JM Neuropsychiatry of Traumatic Brain Injury: A 30-Year Perspective J Neuropsychiatry Clin Neurosci, 2018.PMID 29385931
- [18]Ponsford J, Cameron P, Fitzgerald M, et al. Predictors of postconcussive symptoms 3 months after mild traumatic brain injury Neuropsychology, 2012.PMID 22468823
- [19]Nash RP, Weinberg MS, Laughon SL, et al. Acute Pharmacological Management of Behavioral and Emotional Dysregulation Following a Traumatic Brain Injury: A Systematic Review of the Literature Psychosomatics, 2019.PMID 30665668
- [20]Rao V, Koliatsos V, Ahmed F, et al. Neuropsychiatric disturbances associated with traumatic brain injury: a practical approach to evaluation and management Semin Neurol, 2015.PMID 25714869