Psych · Emergency psychiatry — absconding and missing patients
Absconding and missing patients
Also known as AWOL · Absent without leave · Unauthorised absence · Missing psychiatric patient · Failure to return from leave · Absconsion · Psychiatric elopement · Leave without permission
Fellowship-depth atlas on absconding, AWOL, and missing psychiatric patients — definitions and pathways; epidemiology and suicide link (NCISH); risk factors and motives; immediate search and police thresholds; multi-element prevention and Safewards; leave decision-making; forensic absconsion; post-return care; special populations; CASC communication. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definitions
Absconding is the unauthorised departure of a psychiatric patient from care, or failure to return from authorised leave at the agreed time. Operational definitions vary: some studies count only detained patients who leave the ward, others the hospital boundary, and some include late returns from leave. That definitional scatter is why published rates range widely and cannot be compared raw.[1][4]
Examiners expect clean legal-clinical language distinguishing detained AWOL, failure to return, voluntary AMA, forensic absconsion, and police missing-person pathways.[1][12]
- Detained / involuntary patient abscond (AWOL): leaves without lawful permission or breaches leave conditions under mental health legislation (jurisdiction-specific).[1]
- Failure to return: was on authorised leave (escorted or unescorted) and does not return by the agreed time.[1][4]
- Voluntary / informal patient leaving against medical advice (AMA): not "AWOL" in the statutory sense, but still a clinical emergency if suicide or vulnerability risk is high.[1][9]
- Absconsion / escape (forensic-secure): unauthorised absence from secure or restricted settings, often with justice co-governance.[12][14]
- Missing person (police definition): may be activated in parallel when location is unknown and risk criteria are met — health AWOL policy and police missing-person policy are related, not identical.[1][9]
In the Safewards model, absconding is a conflict behaviour (alongside aggression, self-harm, substance use, and medication refusal). Staff responses (observation upgrades, door locking, leave restriction, specialling) are containment. Conflict and containment feed each other; reducing flashpoints reduces absconds without relying only on security hardware.[10][11]
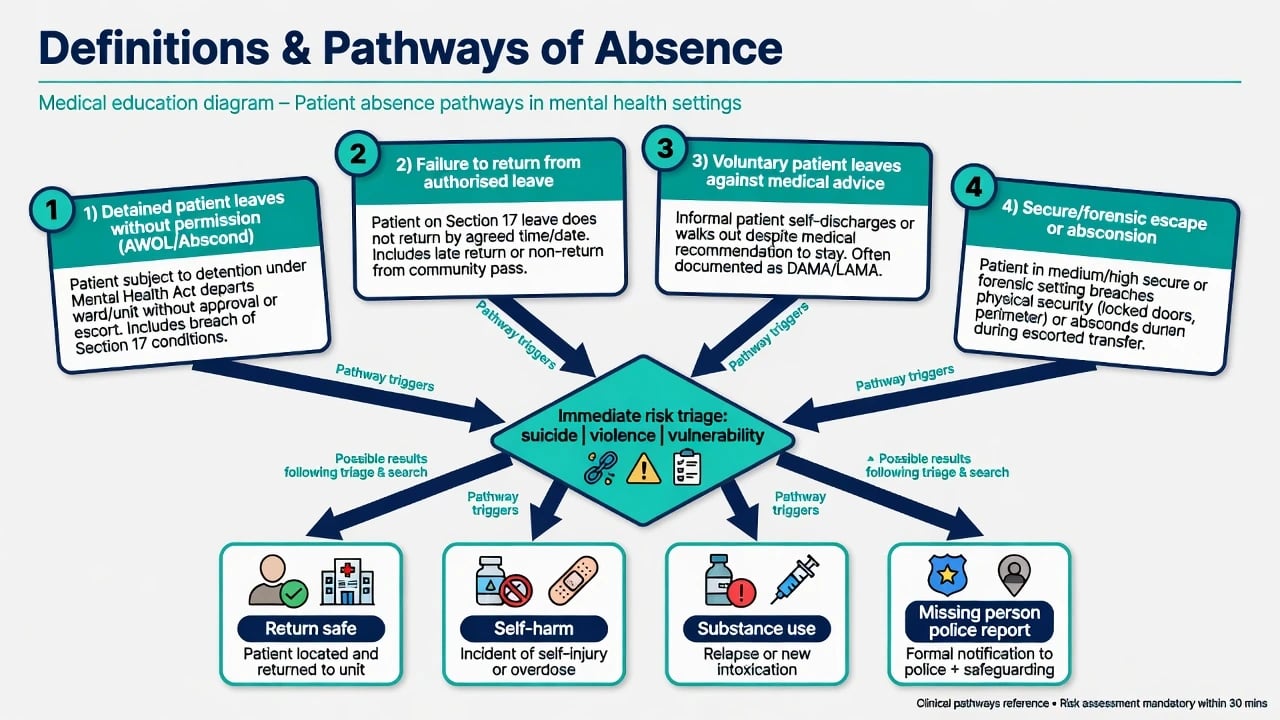
Classification — pathways of absence
| Pathway | Core feature | Immediate priority |
|---|---|---|
| Detained AWOL | Leaves ward/grounds without permission | Legal status + search + risk triage |
| Failure to return | Breach of leave return time | Phone/family first; escalate if high risk |
| Voluntary AMA | Capacity and residual risk | Safety plan or legal pathway if risk high |
| Forensic absconsion | Security/leave breach | Dual clinical–justice notification |
| Pathway framing follows standard absconding literature: legal status, leave breach, voluntary AMA risk, and forensic absconsion each still require immediate suicide/violence/vulnerability triage.[1][12][9] |
How patients leave is often mundane: walking out an unlocked door, following visitors, leaving via garden or fire exit, or simply not returning from a cigarette break or community leave. Timing clusters around staffing transitions, visiting hours, and early admission days in many series.[4][8]
Epidemiology and risk
Literature reviews report highly variable rates (commonly cited from a few percent to well above 10–20% of admissions depending on definition and setting). Australian acute-ward series repeatedly show overrepresentation of younger males, involuntary status, prior absconding, and episodes concentrated early in the admission, with a non-trivial minority of repeat absconders.[1][6][7][8]
Why fellowship candidates must take this seriously: National Confidential Inquiry work on inpatient suicide shows that a large majority of inpatient suicides occur off the ward, and absconding-related suicides have a distinct profile — more often younger, unemployed, and homeless compared with other inpatient suicides. Absconding is also linked to self-harm, substance use, missed medication, treatment disruption, and harm to others in classic outcome studies.[9][3]
Forensic rates and motives differ from general adult wards; case-control and prospective forensic work shows that simple checklists have limited ability to predict the next absconsion at the individual level, reinforcing formulation-based leave management rather than actuarial false comfort.[12][14]
Mechanisms and motives — person × illness × environment × system
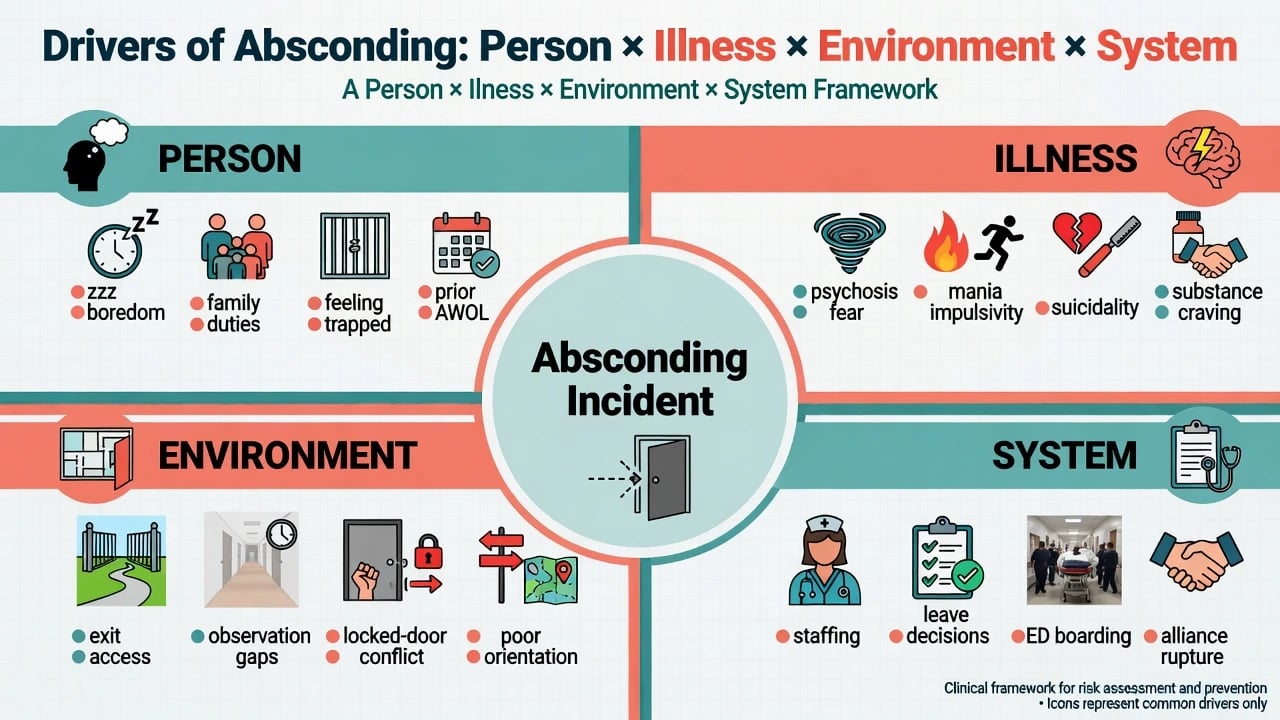
Illness drivers
Active psychosis (especially persecutory fear or command phenomena), mania with impulsivity and irritability, severe depression or mixed states with intent to leave in order to die, substance craving or withdrawal, and cognitive impairment or delirium with exit-seeking. These are dynamic and treatable — they belong in today's plan.[2][6]
Person and social motives
Classic qualitative work finds boredom, feeling trapped, home and family responsibilities, disagreement with detention or medication, fear of other patients, poor alliance, and wanting cigarettes or substances. Ignoring motives produces security-only responses that fail.[2]
Environment and system
Observation gaps, exit design, locked-door regimes (which can reduce some exits while increasing enclosure-related conflict), poor orientation to the ward, ED boarding, staffing skill-mix, and inconsistent leave practices. Door locking is not a complete solution and has acceptability trade-offs for patients, staff, and visitors.[4][10]
Clinical presentation and warning signs
Pre-abscond signals include packing belongings, outdoor clothing at odd times, hovering near exits, repeated failed leave requests, sudden calm after agitation, arranging pickup by phone, and irritability when boundaries are enforced. None is pathognomonic; clusters plus known risk factors raise the index of suspicion.[4][2]
Scenarios examiners use: empty bed at 15-minute observations; late return from unescorted leave; ED mental-health bay empty before assessment finished; community crisis patient not at agreed visit with phone off; forensic patient late from community leave.[4][8][12]
Differential — get the legal frame right
Do not conflate authorised leave with communication failure, purposeful abscond with delirium wandering, voluntary AMA with statutory AWOL, or open-ward walk-out with secure-unit escape. Do not lead with "malingering" or "attention-seeking." Assess risk, legal status, and capacity first; secondary-gain hypotheses come last and rarely change the need for a search plan.[1]
- Statutory unauthorised absence
- Recall/return powers apply
- Police liaison often required
- Document legal section
- Leave was authorised
- Breach of return time
- Phone and family first
- Escalate by residual risk
- Not statutory AWOL
- Capacity and residual risk
- Safety plan or re-detain
- Never passive high-risk discharge
Legal-status discriminators guide return powers and police thresholds but never remove the duty to triage suicide, violence, and vulnerability risk.[1][9]
Assessment
On admission and before leave
Formulate abscond risk alongside suicide, violence, and vulnerability risk. Key elements: prior AWOL, legal status, insight and agreement with detention, substance use, family conflict or domestic drivers to leave, housing/homelessness, destination likelihood, and cultural safety of the ward. Before any leave, reassess MSE, purpose of leave, escort level, destination, return time, contacts, and contingency if late. Forensic services benefit from structured decision-making tools around leave privileges; A-B design work has linked structured processes to fewer absconsions.[6][13]
When a patient is missing
Build a minute-by-minute timeline: last seen (time, place, clothing, companions), money/phone/keys, likely destinations, risk content from last MSE, legal status, and dependents at home. Collateral from family and co-patients often locates the person faster than random search.[3][4][9]
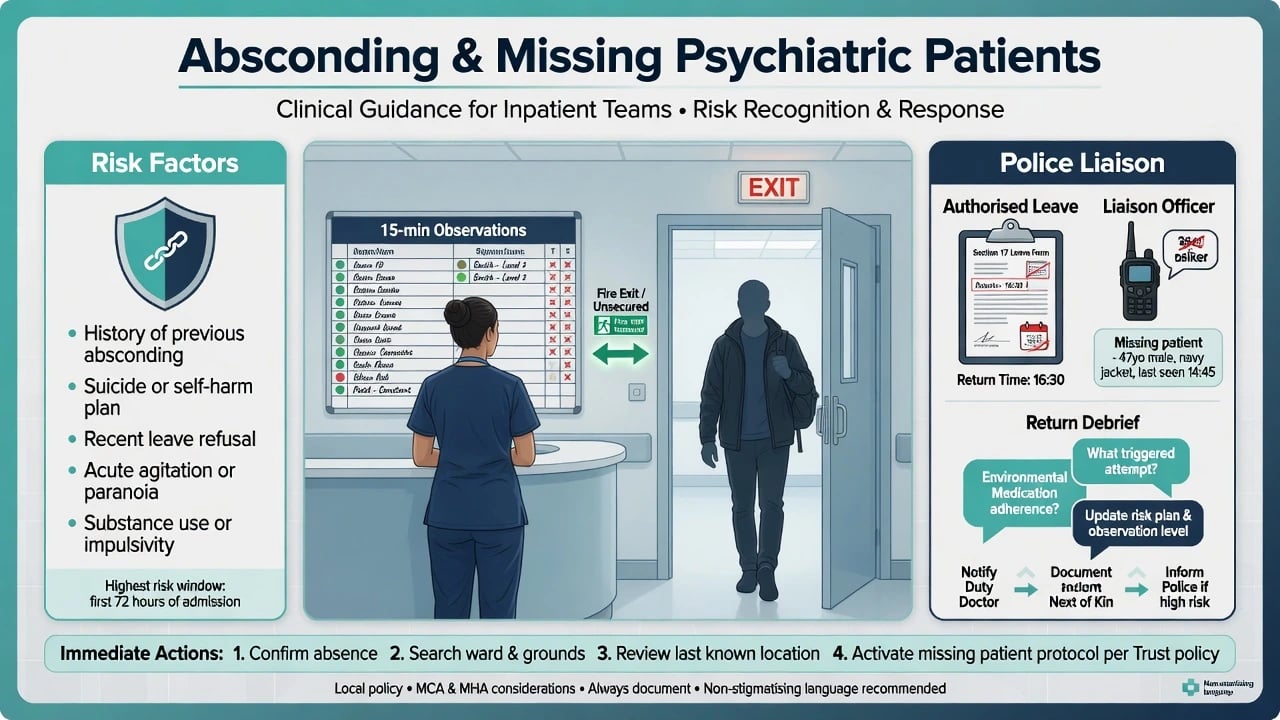
Immediate management (resuscitation phase)
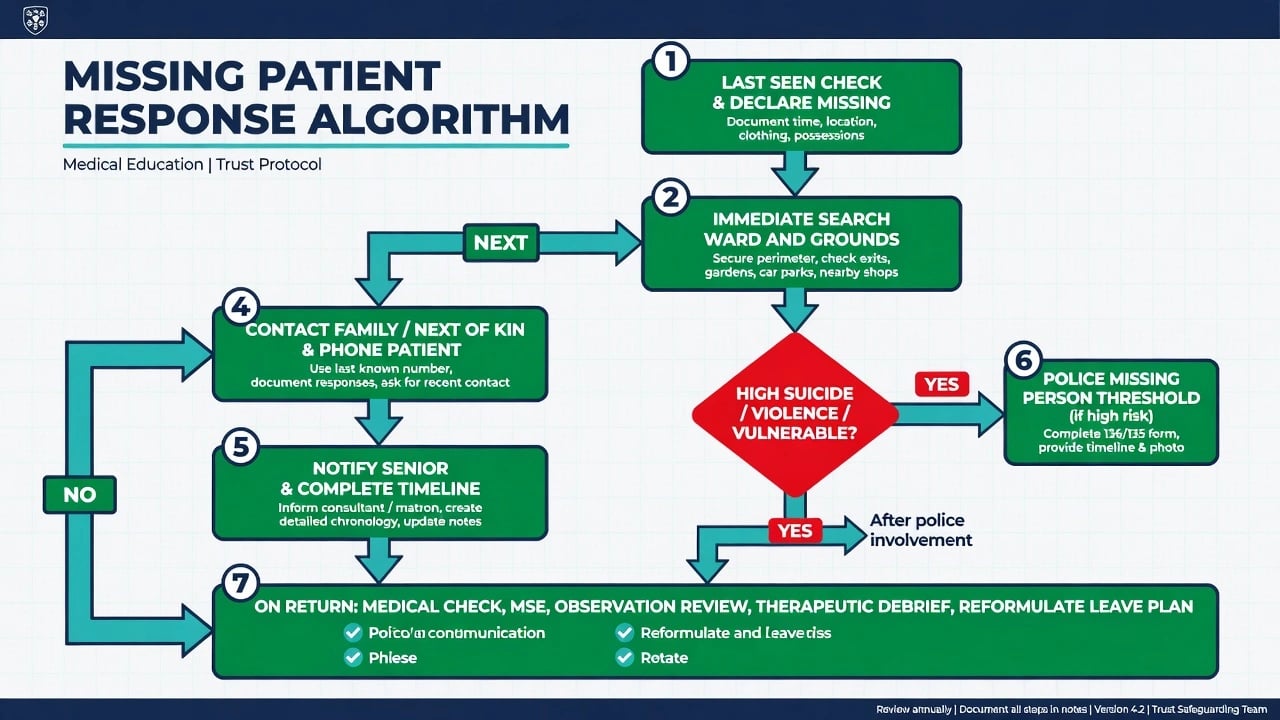
- Declare missing per local policy; document last-seen details.
- Search ward, bathrooms, gardens, car parks, nearby exits; review door/CCTV logs if available.
- Risk-stratify: high if active suicide/homicide concern, recent attempt, severe psychosis with vulnerability, child/older adult/frail, extreme weather, forensic dual status, or known lethal means access.
- Contact patient phone and next of kin; ask where they are and whether they will return.
- Notify nurse-in-charge, duty doctor, and consultant/on-call senior as policy requires; complete incident timeline.
- Police: use local missing-person / AWOL notification pathways promptly for high-risk cases — do not wait hours because "they usually come back."
- Media only via authorised organisational channels when public-protection criteria are met. Immediate response is driven by off-ward harm risk (including suicide) and outcome data linking absconding to self-harm and treatment disruption; high-risk cases warrant prompt multi-agency escalation.[9][3]
Least-restrictive principle still applies once found: de-escalate, negotiate return, use lawful restraint only for imminent harm. Punitive "strip privileges forever" responses without formulation increase future conflict.[10]
Definitive management and prevention
Multi-element nursing intervention (Bowers)
A real-world multi-element package (including identification of high-risk patients, targeted nursing time, careful delivery of bad news, multidisciplinary review after incidents, and structured post-return work) produced a substantial reduction in absconding rates in practice settings — the fellowship "name the intervention components" pearl.[5]
Safewards
The Safewards cluster RCT reduced conflict and containment rates on acute wards. Because absconding sits in the conflict domain, culture interventions that reduce flashpoints (clear mutual expectations, soft words, discharge messages, calm down methods, and related interventions) are part of abscond prevention, not soft add-ons.[10][11]
Leave redesign
Clear purpose, graded leave, documented return times, escort decisions linked to risk, contingency contacts, and structured forensic leave decision tools. Address boredom and family contact needs within policy rather than forcing patients into covert exits.[13][2]
Treat the illness
Optimise psychosis, mania, depression, substance withdrawal, and akathisia. Review whether detention remains necessary. Alliance repair after conflict reduces motives to flee.[2][6]
Post-return care
Medical check (injury, intoxication, overdose, exposure), full MSE with suicide and violence re-assessment, observation-level review, legal-status review, means restriction if needed, substance plan, and a non-humiliating debrief: what triggered leaving, what would help next time, what the team will change. Update the risk formulation and leave plan in the notes the same shift.[3][9]
Special populations
- Child/adolescent: bolting, peer facilitation, care-system trauma; child-protection if risk outside.
- Older adult: delirium and dementia exit-seeking; falls, exposure, traffic injury; not always "purposeful abscond."
- Perinatal: dyad safety and child-protection interface if mother leaves with or without infant concerns.
- Intellectual disability / autism: elopement under sensory or communication stress; plain-language plans.
- Indigenous and culturally diverse: culturally unsafe wards as a driver; involve family and cultural supports early.
- Homeless: harder to locate; appears in NCISH abscond-suicide profiles — escalate search and outreach.[9][6]
- Forensic: dual reporting; structured leave review after any absconsion.[12][13][14]
Regional practice notes
Always label the jurisdiction before quoting statutory powers in an exam answer; absconding and AWOL powers are statute- and policy-specific across ANZ, UK, US, and Indian systems.[1][9]
Complications and pitfalls
Under-reporting of brief absconds; delayed police for high-risk cases; false reassurance from "usual behaviour"; pure security responses that ignore boredom and alliance; incomplete leave documentation that fails coronial scrutiny; missing dependents or child-protection issues; assuming voluntary status removes the duty to act on high suicide risk.[1][9][3]
Prognosis and disposition
Most episodes are short and without serious harm, but the risk distribution has a lethal tail. Repeat absconders need formulation-driven plans (often including activity programmes, family mediation, substance treatment, and graded leave), not only higher locks. After return, disposition ranges from increased observation and PICU step-up through revised leave, to — when detention criteria are no longer met and community safety is achievable — negotiated discharge with intensive follow-up. Forensic leave is commonly stepped down pending formal review.[3][7][13]
Evidence and exam pearls
Landmark lines to name: Bowers literature review and motive/outcome series; Bowers multi-element reduction intervention; Australian profiles (Mosel, Muir-Cochrane, Gerace); Hunt/NCISH abscond suicide survey; Safewards model and RCT; Wilkie forensic motives; Simpson structured leave decision-making; Cullen prospective forensic absconsion study.[1][5][9][11][13]
Summary
Absconding is a preventable conflict event with rare but catastrophic outcomes. Formulate risk, act fast when someone is missing, prevent with multi-element relational and leave-system redesign (Safewards included), and treat return as a clinical reassessment — not a punishment ceremony.[5][11][9]
References
- [1]Bowers L, Jarrett M, Clark N Absconding: a literature review J Psychiatr Ment Health Nurs, 1998.PMID 10067481
- [2]Bowers L, Jarrett M, Clark N, et al. Absconding: why patients leave J Psychiatr Ment Health Nurs, 1999.PMID 10633672
- [3]Bowers L, Jarrett M, Clark N, et al. Absconding: outcome and risk J Psychiatr Ment Health Nurs, 1999.PMID 10633674
- [4]Bowers L, Jarrett M, Clark N, et al. Absconding: how and when patients leave the ward J Psychiatr Ment Health Nurs, 1999.PMID 10633673
- [5]Bowers L, Simpson A, Alexander J Real world application of an intervention to reduce absconding J Psychiatr Ment Health Nurs, 2005.PMID 16164511
- [6]Muir-Cochrane E, Mosel K, Gerace A, et al. The profile of absconding psychiatric inpatients in Australia J Clin Nurs, 2011.PMID 21320199
- [7]Gerace A, Oster C, Mosel K, et al. Five-year review of absconding in three acute psychiatric inpatient wards in Australia Int J Ment Health Nurs, 2015.PMID 25444670
- [8]Mosel KA, Gerace A, Muir-Cochrane E Retrospective analysis of absconding behaviour by acute care consumers in one psychiatric hospital campus in Australia Int J Ment Health Nurs, 2010.PMID 20550641
- [9]Hunt IM, Windfuhr K, Swinson N, et al. Suicide amongst psychiatric in-patients who abscond from the ward: a national clinical survey BMC Psychiatry, 2010.PMID 20128891
- [10]Bowers L Safewards: a new model of conflict and containment on psychiatric wards J Psychiatr Ment Health Nurs, 2014.PMID 24548312
- [11]Bowers L, James K, Quirk A, et al. Reducing conflict and containment rates on acute psychiatric wards: The Safewards cluster randomised controlled trial Int J Nurs Stud, 2015.PMID 26166187
- [12]Wilkie T, Penney SR, Fernane S, Simpson AI Characteristics and motivations of absconders from forensic mental health services: a case-control study BMC Psychiatry, 2014.PMID 24669758
- [13]Simpson AI, Penney SR, Fernane S, Wilkie T The impact of structured decision making on absconding by forensic psychiatric patients: results from an A-B design study BMC Psychiatry, 2015.PMID 25935745
- [14]Cullen AE, Jewell A, Tully J, et al. A Prospective Cohort Study of Absconsion Incidents in Forensic Psychiatric Settings: Can We Identify Those at High-Risk? PLoS One, 2015.PMID 26401653