Psych · Emergency psychiatry
Acute agitation and rapid tranquillisation
Also known as Rapid tranquillisation · Rapid tranquilization · Acute agitation · Behavioural emergency · Severe behavioural disturbance · Chemical restraint · Emergency sedation psychiatry
Exam-exhaustive fellowship topic on acute agitation and rapid tranquillisation — de-escalation first, capacity and least-restrictive legal principles, oral-then-IM ladders with named doses (lorazepam, midazolam, promethazine, haloperidol, olanzapine, aripiprazole, droperidol), never IM olanzapine plus parenteral benzodiazepine, post-RT monitoring, TREC and Project BETA evidence, BAP/NAPICU principles, special populations. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Acute agitation is a time-critical behavioural emergency, not a diagnosis. Rapid tranquillisation (RT) is the time-limited pharmacological calm that allows assessment and definitive treatment when verbal and environmental measures fail. This topic goes deeper than the psychiatric-emergencies hub: full oral and IM ladders with doses, TREC and ANZ ED evidence, monitoring, documentation, and special-population traps that examiners love.[1][7]
Overview and definition
Acute agitation is a state of motor restlessness, emotional arousal, and heightened responsiveness that may progress to aggression or violence. Aggression is behaviour intended to harm or intimidate. Violence is the physical act causing or likely to cause injury. Rapid tranquillisation is the emergency use of medication — preferably oral, then parenteral — to calm severe agitation so that assessment and treatment can proceed safely. RT is not long-term chemical restraint and is not a substitute for diagnosis or for treating the cause.[1][3][18]
DSM-5-TR and ICD-11 do not define a single “agitation disorder.” You manage a syndrome while identifying psychosis, mania, delirium, intoxication, withdrawal, pain, or medical mimic as the driver.[4][18]
Classification — severity drives the ladder
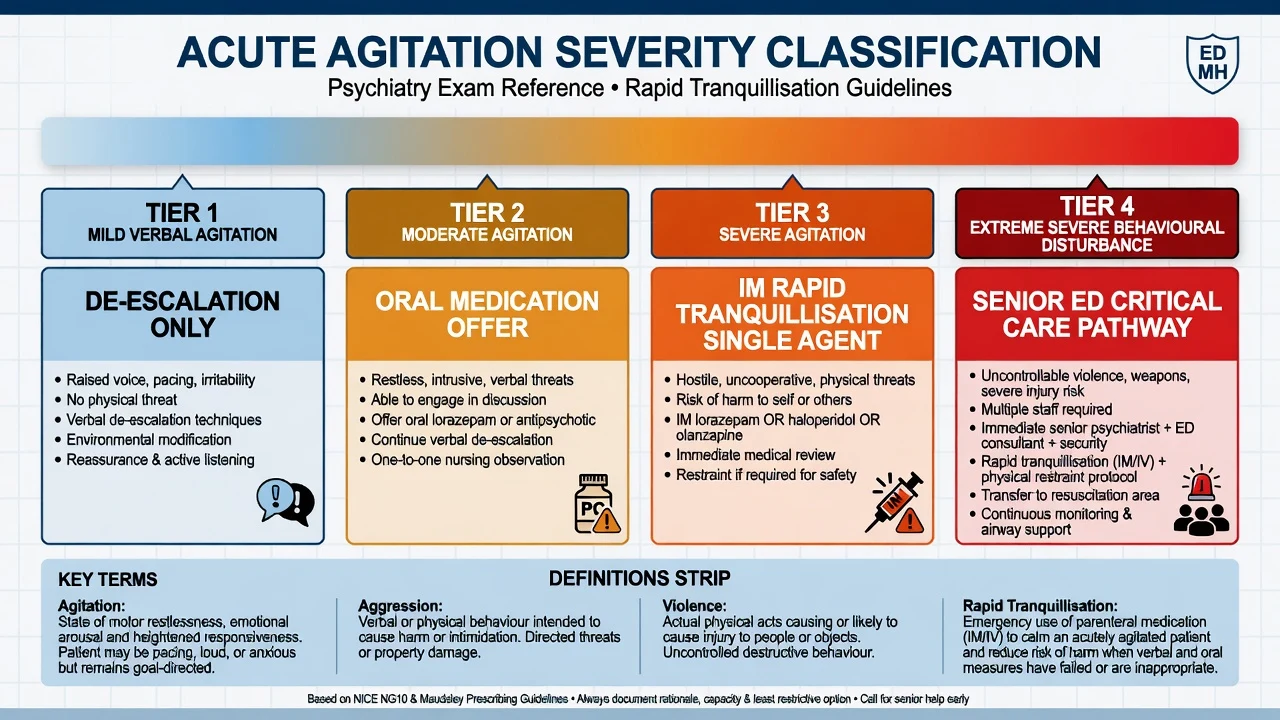
| Tier | Clinical cues | Default response |
|---|---|---|
| 1 Mild | Raised voice, pacing, no physical threat | Environment + verbal de-escalation |
| 2 Moderate | Restless, intrusive, able to engage | Continue de-escalation; offer oral RT |
| 3 Severe | Hostile, uncooperative, imminent risk | IM RT single agent if oral refused/unsafe |
| 4 Extreme SBD | Continuous extreme agitation, hyperthermia risk, weapons, collapse risk | Senior ED/ICU pathway, airway-ready sedation |
Operational threshold for IM RT: severe agitation, oral refused or impossible, de-escalation failed or unsafe to continue alone, and imminent risk of harm that cannot be contained by other means. Document indication, alternatives considered, capacity, and legal basis.[1][17]
Epidemiology and risk context
Agitation is common in ED and acute psychiatry; serious violence is less common but concentrates where prior violence, intoxication, paranoia with threat content, command hallucinations to harm, and chaotic environments coexist.[1][18] Staff injury, prolonged restraint, and oversedation are preventable system harms. Extreme severe behavioural disturbance (SBD) carries medical mortality risk from hyperthermia, acidosis, rhabdomyolysis, and cardiorespiratory collapse — treat as a medical resuscitation problem, not “just a psych sedation.”[4][8]
Pathophysiology — final common pathway
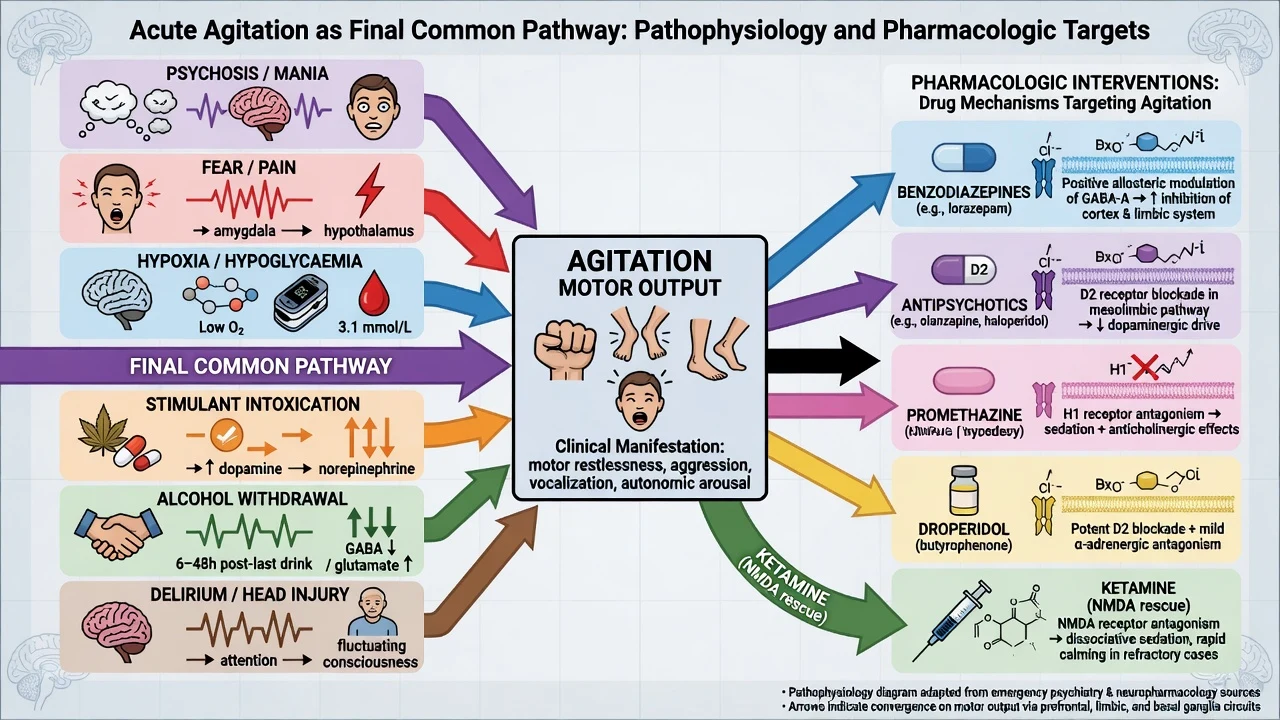
Psychosis, mania, fear, pain, hypoxia, hypoglycaemia, stimulant intoxication, alcohol or sedative withdrawal, and delirium all converge on the same motor-behavioural output. Pharmacological RT targets that output while you treat the driver.[3][4]
- Benzodiazepines — positive allosteric modulators at GABA-A; anxiolysis and sedation; preferred when anxiety, withdrawal, or undifferentiated fear dominates.[1][3]
- Antipsychotics (D2 antagonism) — reduce psychotic drive and can calm agitation; trade-offs include EPS, akathisia, and QTc effects for some agents.[3][11]
- Promethazine — sedating H1 antagonist; combined with haloperidol in TREC to improve early calm and reduce dystonia versus haloperidol alone.[5][12]
- Droperidol — butyrophenone used extensively in Australian ED SBD protocols; PK and safety series support IM use with monitoring.[7][8][9]
- Ketamine — NMDA antagonism for rescue of difficult-to-sedate SBD under ED/critical-care governance with airway readiness.[10]
Clinical presentation
Scene and interview safety
Before phenomenology: clear exit routes for you and the patient, remove potential weapons, adequate staffing, one primary communicator, calm voice, offer seating and water, avoid cornering. If violence is imminent, withdraw and escalate security per local protocol — heroism is not a competency.[2][17]
Phenomenology of escalating agitation
Look for pacing, clenched fists, invasion of personal space, loud speech, throwing objects, threat content, and rising autonomic signs. Distinguish instrumental purposeful aggression from disorganised agitation (delirium, excited catatonia, stimulant toxicity). Document verbatim threats and command hallucinations.[18]
Extreme SBD features
Continuous extreme agitation, incoherent speech, apparent pain tolerance, hyperthermia risk, and sudden collapse risk define the operational emergency. Prefer descriptive language (severe behavioural disturbance) over contested forensic labels, and manage the physiology first.[4][8]
Differential diagnosis — medical mimics first
Never miss list with discriminators:[4][13]
- Delirium — inattention, fluctuation, medical signs
- Hypoglycaemia / hypoxia / hypercarbia — observations and glucose
- Head injury / intracranial event — trauma, focal neurology
- Encephalitis (including autoimmune) — new psychosis with seizure, dysautonomia, movement
- Sepsis / meningitis — fever, source, meningism
- Alcohol or benzodiazepine withdrawal — tremor, diaphoresis, seizures
- Stimulant intoxication — mydriasis, tachycardia, paranoia, hyperthermia
- Serotonin toxicity / NMS / anticholinergic toxicity — tempo, clonus versus lead-pipe rigidity
- Akathisia — inner restlessness after antipsychotics; wrong response is more D2 blockade
- Primary psychosis or mania — after the above are considered
Medical evaluation of the agitated patient is history- and examination-driven, not a fixed pan-lab ritual for every low-risk presentation. AAEP Project BETA and medical-clearance task force guidance emphasise targeted testing with documented rationale.[4][13][14]
Clinical and bedside assessment
- ABCDE + capillary glucose + SpO2 + temperature
- Scene safety and team roles
- Focused history: onset tempo, substances, medications, trauma, medical disease
- Emergency MSE: suicidality, homicidality, command content, insight, attention
- Dynamic violence risk factors and protective factors
- Capacity for the specific decision (accept oral meds, remain for assessment)
- Legal status and least-restrictive options
- Collateral when available
Agitation scales (for example PANSS-EC, OAS, RASS in monitored settings) structure observation; they do not replace clinical judgment or safe disposition thinking.[1][18]
Investigations
| Priority | Test | Why |
|---|---|---|
| Immediate | Vitals + glucose | Hypoglycaemia and instability kill first |
| Before or ASAP with antipsychotics | ECG (QTc), pregnancy test if relevant | Cardiac safety of RT agents |
| Restraint / extreme exertion | CK, U&E, FBC | Rhabdomyolysis, renal injury |
| Overdose context | Paracetamol, salicylate ± others | Concurrent self-poisoning |
| Organic red flags | Imaging, LP, EEG, infection/autoimmune panel | Do not delay life-saving care for low-yield tests |
| Substance | UDS with known limitations | Negative screen does not exclude |
Do not delay necessary RT for a urine drug screen. Do not label “functional” in the presence of fever and fluctuating attention without a medical work-up plan.[4][13]
Management — resuscitation sequence
Non-pharmacological first
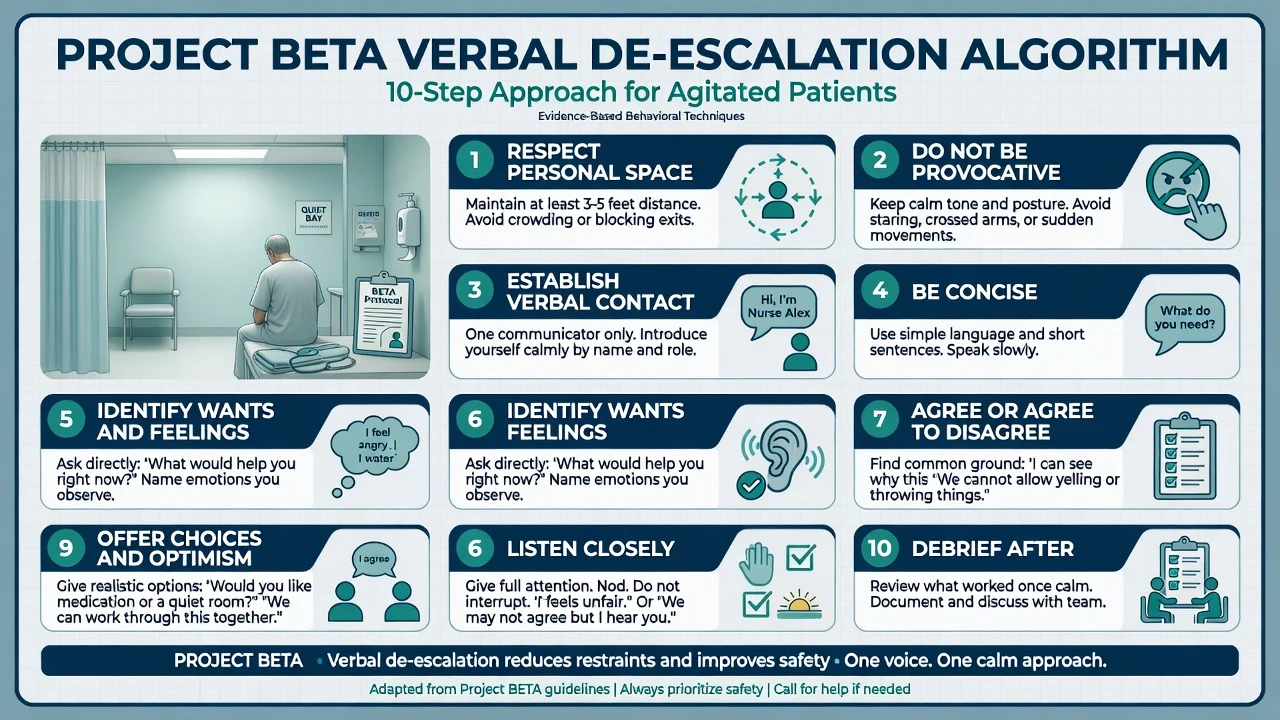
Project BETA verbal de-escalation principles examiners expect you to name in spirit if not verbatim: respect personal space; do not be provocative; establish verbal contact with one communicator; be concise; identify wants and feelings; listen; agree or agree to disagree; set clear limits; offer choices and optimism; debrief after.[2] Quiet bay, reduce audience, remove triggers, and offer oral medication as partnership rather than as punishment.[1][2]
Physical restraint and seclusion are last-line, time-limited, staffed by trained teams, never prolonged prone, released as soon as pharmacological calm allows. Evidence comparing restraint versus seclusion is limited; minimisation is the ethical default.[16][17]
The RT ladder with named doses
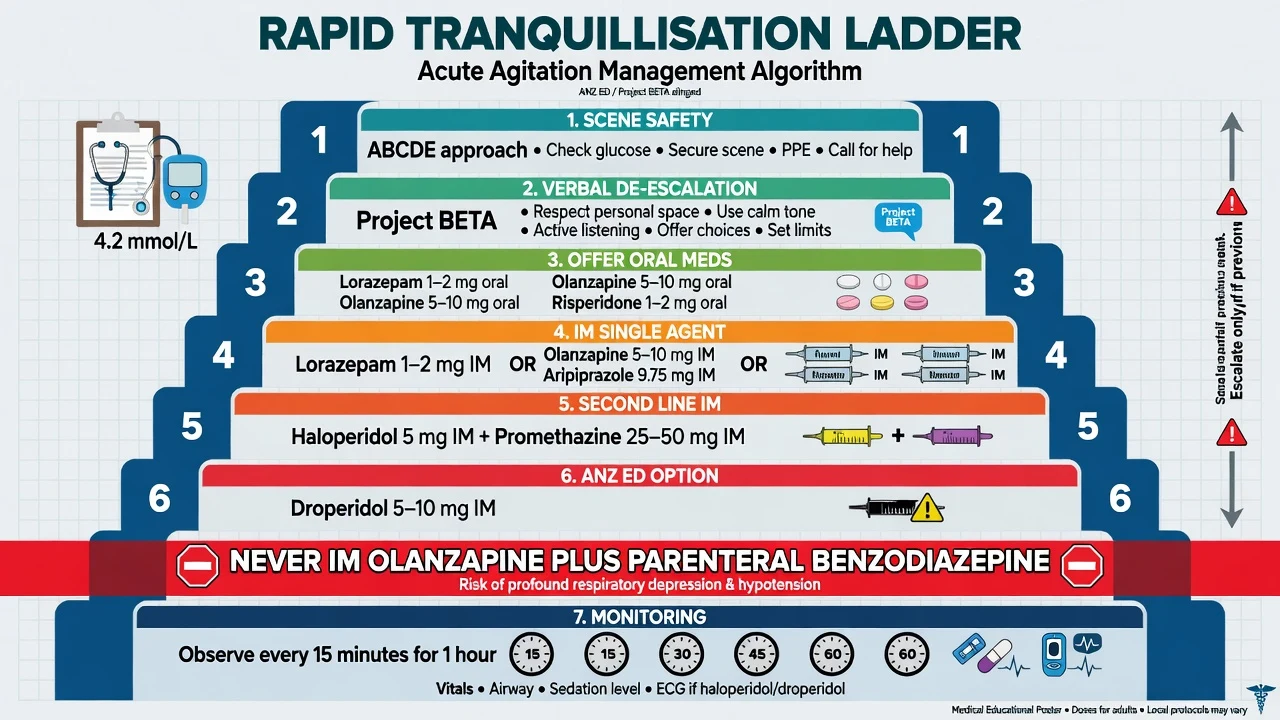
Principles (BAP/NAPICU-aligned, Project BETA-compatible):[1][3]
- Safety and de-escalation first.
- Treat reversible causes (pain, hypoxia, hypoglycaemia, fear, withdrawal).
- Offer oral medication if safe.
- If IM required, prefer a single agent.
- Monitor airway and vital signs after sedation.
- Endpoint is calm and rousable, not unconscious.
- Document capacity, legal basis, agent, dose, and review time.[1][15]
Named oral options (adult typical starting ranges)
Use local formulary and product information; reduce doses in older adults and medically frail patients.[1][3]
| Agent | Typical oral dose | Notes |
|---|---|---|
| Lorazepam | 1–2 mg | Anxiolysis/sedation; useful when psychosis is not the sole driver |
| Olanzapine | 5–10 mg (orodispersible if available) | Antipsychotic + sedation |
| Risperidone | 1–2 mg | Antipsychotic option |
| Promethazine | 25–50 mg | Sedating antihistamine in some protocols |
| Aripiprazole | 10–15 mg | Less sedating; metabolic/QTc profile may favour |
Named IM options — UK consensus style (psychiatric settings)
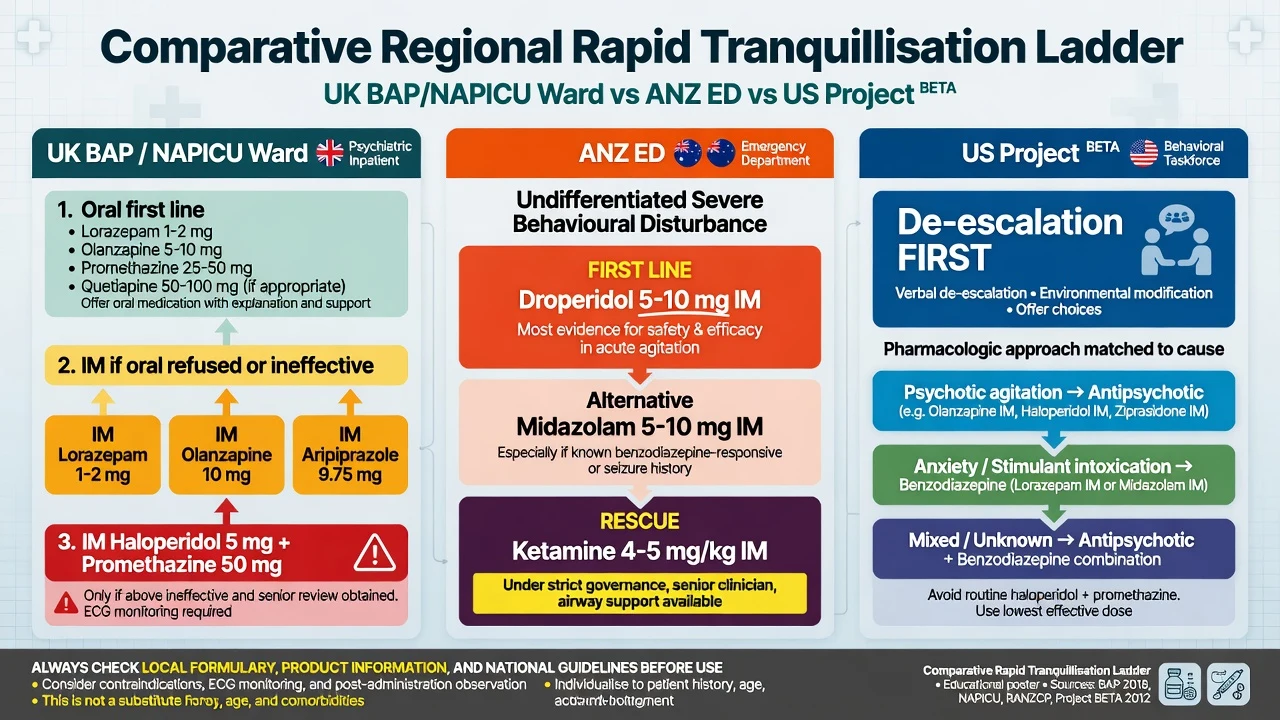
First-line single-agent IM options in BAP/NAPICU-style frameworks include:[1]
- IM lorazepam 1–2 mg
- IM olanzapine 5–10 mg (not with parenteral benzodiazepine)
- IM aripiprazole commonly 9.75 mg (licensed range often cited around 5.25–15 mg depending on product)
Second-line / TREC-backed combination:
IM haloperidol 5 mg + IM promethazine 25–50 mg was superior to haloperidol alone for rapid tranquillisation in pragmatic Brazilian TREC work — promethazine reduces acute dystonia risk and improves early calm. Cochrane synthesis supports the combination for psychosis-induced aggression.[5][12]
Obtain ECG as soon as practicable when using butyrophenones, especially with cardiac risk, electrolyte abnormality, or high cumulative dose. Prefer avoiding IM haloperidol if QTc is already prolonged.[1][11]
ANZ ED / undifferentiated SBD options
Australian ED programmes have extensive experience with IM droperidol 5–10 mg for violence and acute behavioural disturbance. The DORM RCT compared IM droperidol with midazolam; subsequent safety series and population PK analyses support droperidol with monitoring.[7][8][9]
- IM midazolam 5–10 mg — rapid onset; more airway/oversedation vigilance and sometimes more redosing than droperidol in comparative work.[7]
- Ketamine rescue for difficult-to-sedate SBD in ED (for example protocols studied around 4–5 mg/kg IM under specialist governance) — not default ward first-line; airway-ready environment only.[10]
These are service- and region-specific. Do not claim droperidol is universal first-line on every psychiatry ward worldwide.[1][7]
Cause-matched agent choice (exam pearl)
| Likely driver | Prefer | Avoid / caution |
|---|---|---|
| Primary psychosis / mania | Antipsychotic oral or IM; H+P if needed | High-dose benzo alone if florid psychosis untreated |
| Anxiety / panic / undifferentiated fear | Lorazepam oral/IM | Unnecessary high-potency D2 blockade |
| Alcohol / sedative withdrawal | Benzodiazepines | Antipsychotic alone (does not treat withdrawal) |
| Stimulant SBD (ANZ ED) | Droperidol ± midazolam per protocol | Unmonitored polypharmacy |
| Delirium | Treat cause; lowest effective sedation | High anticholinergic load in elderly |
| Parkinson / DLB | Low-dose benzo carefully; specialist advice | High-potency typical antipsychotics |
Post-sedation monitoring
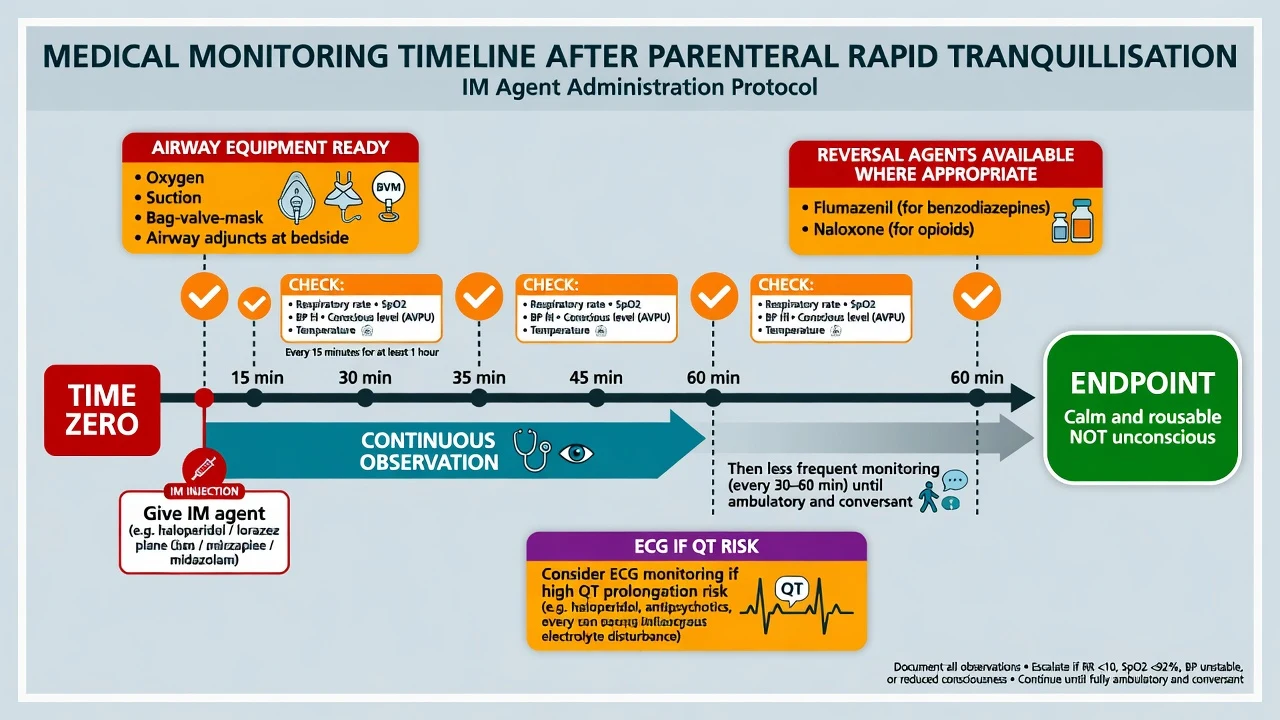
Practical standard after parenteral RT:[1]
- Continuous observation until ambulatory and conversant
- Respiratory rate, SpO2, BP, HR, conscious level, temperature every 15 minutes for at least 1 hour, then as clinically indicated
- Oxygen, suction, bag-valve-mask, and airway-skilled staff available
- ECG if QT risk agents or cardiac risk
- Document recovery and any need for further doses
Flumazenil is not a routine RT adjunct; reverse only with extreme caution if used at all (seizure risk in chronic benzodiazepine users). Naloxone only if opioids are implicated.[1][3]
Acute dystonia
Painful muscle spasm (oculogyric crisis, torticollis, laryngospasm risk) after antipsychotics is an emergency. Treat with an anticholinergic — for example benztropine 1–2 mg IM/IV or procyclidine 5–10 mg IM depending on local availability — and review the antipsychotic plan.[1][11]
Management — after the calm: definitive care and documentation
Once behaviourally safer: (1) complete medical and psychiatric assessment that RT made possible; (2) treat the underlying driver (psychosis pathway, mania pathway, detox, delirium work-up); (3) plan observation level and disposition; (4) debrief patient and staff after restrictive practices; (5) write a contemporaneous note covering risks, de-escalation attempts, capacity findings, legal basis, agent/dose/route/time, monitoring, response, complications, and review plan.[1][15][17]
Specific scenarios
Primary psychotic agitation. Offer oral antipsychotic if accepted; IM single-agent antipsychotic or H+P if needed; avoid IM olanzapine + parenteral BZD; start definitive antipsychotic plan once safe.[1][5]
Acute mania. Same ladder; high energy and poor insight often require admission; lithium/valproate decisions are not RT — they are definitive mood stabilisation after medical checks.[1]
Stimulant intoxication. Medical observation for hyperthermia and arrhythmia; ANZ ED droperidol/midazolam evidence is highly examinable; avoid unmonitored stacked sedatives.[7][8]
Withdrawal. Benzodiazepines treat the pathophysiology; antipsychotics alone can worsen the picture.[3]
Inpatient ward vs ED. Ward RT often follows BAP/NAPICU oral-then-single-IM logic; ED SBD often follows droperidol-led local protocols. State which setting you are in.[1][7]
Complications and pitfalls
- Respiratory depression from polypharmacy, especially IM olanzapine + parenteral BZD
- Oversedation to unconsciousness with aspiration
- QTc prolongation / torsades risk context with high-dose butyrophenones
- Acute dystonia and akathisia misread as agitation
- Positional asphyxia, rhabdomyolysis, VTE, psychological trauma from restraint
- Missed medical mimic labelled “behavioural”
- Inventing Mental Health Act section numbers across jurisdictions
Prognosis and disposition
| Destination | When |
|---|---|
| Medical ED / ICU | Unstable vitals, severe SBD physiology, deep sedation needing airway support |
| Psychiatric inpatient (voluntary) | High residual risk, accepts admission |
| Involuntary pathway | Serious risk + statutory criteria; least-restrictive rationale documented |
| ED observation | Evolving intoxication, awaiting collateral, short-term safety |
| Discharge with plan | Risk reduced, supports present, follow-up timed, documentation complete |
Handover after an RT event must include agent, dose, time, response, observations, residual risk, and outstanding investigations.[1]
Special populations
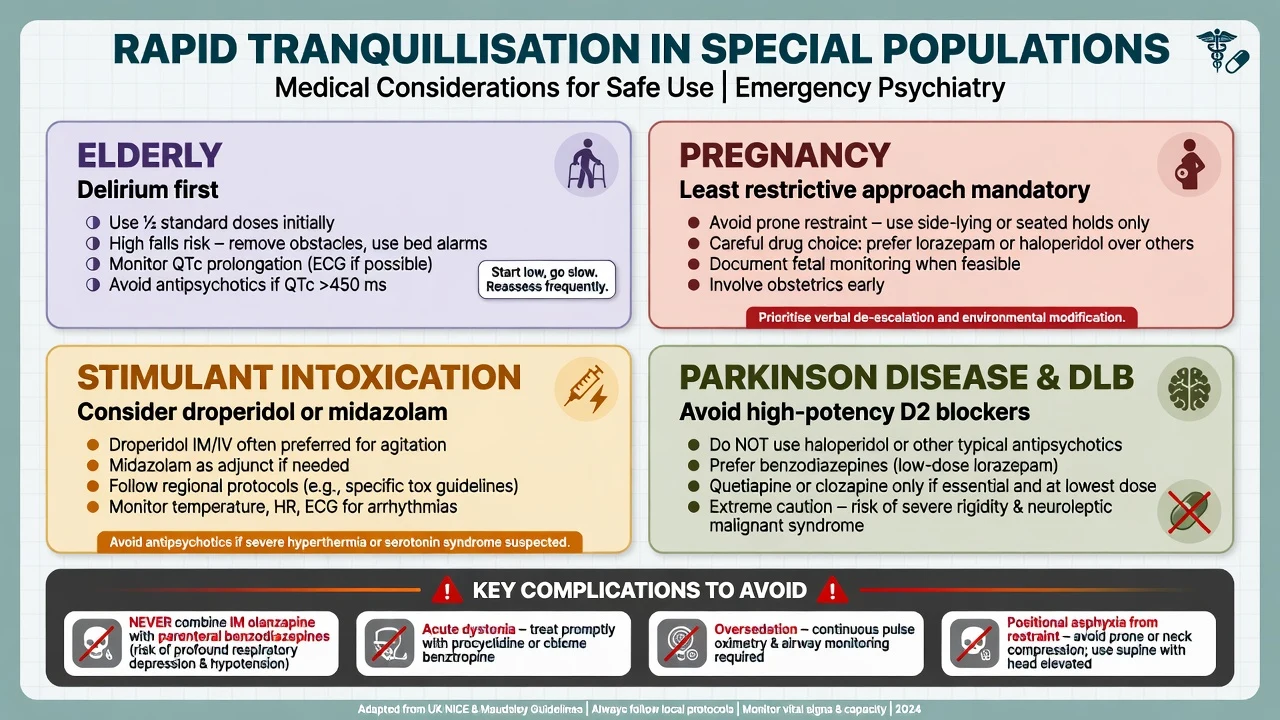
Older adults. Delirium until proven otherwise. Start at approximately half usual adult RT doses; high fall and QTc risk; avoid polypharmacy sedation.[1][13]
Pregnancy. Avoid prone restraint; prefer least-restrictive measures; involve obstetrics early; agent choice balances maternal safety, fetal considerations, and product information — do not invent “safe list” dogma without local specialist advice.[1]
Children and adolescents. Consent/assent, family systems, lower weight-based dosing, minimise restraint trauma; involve CAMHS pathways.[1]
Intellectual disability / autism. Sensory overload and pain may drive behaviour; environmental modification first; beware mislabelling distress as “non-compliance.”[1]
Parkinson disease / DLB. Avoid high-potency typical antipsychotics; low-dose benzodiazepine carefully if essential; specialist advice for any antipsychotic use.[1][3]
Capacity, law and least-restrictive care
Capacity (functional test shared across common-law systems): can the person understand, retain, use/weigh, and communicate a decision? Capacity is decision-specific and time-specific. Psychosis does not automatically erase capacity for every decision; detention under a Mental Health Act does not automatically equal incapacity for every decision.[15]
Least-restrictive principle. Prefer voluntary care, oral medication, and environmental measures when safe. Involuntary treatment and restrictive practices require serious risk (or statutory criteria), documented failure or unsuitability of less restrictive options, and scheduled review. Do not invent section numbers for Australia, New Zealand, England, or the United States — name the principle and apply the local statute with senior advice.[1][15][17]
Evidence, guidelines and regional differences
Landmark evidence you must name: BAP/NAPICU 2018 (de-escalation and RT with combination ban); Project BETA (verbal de-escalation and psychopharmacology); TREC Brazil Huf 2007 (H+P superior to H alone); TREC India Raveendran 2007 (olanzapine versus H+P pathways); Cochrane reviews of haloperidol and H+P; DORM Isbister 2010 plus Calver 2015 and Foo 2016 (droperidol); Isbister 2016 (ketamine rescue for difficult-to-sedate SBD).[1][2][3][5][6][7][8][9][10][11][12]
Exam pearls
SAFE-RT
- Oral first, single IM agent, never IM olanzapine + parenteral BZD.
- Endpoint is calm and rousable, not unconscious.
- H+P beats H alone for early tranquillisation with less dystonia (TREC/Cochrane).
- Droperidol is ANZ ED culture, not universal ward first-line.
- Ketamine is rescue under governance, not default registrar first choice on a general ward.
- Akathisia is not “more psychosis.”
- Capacity is decision-specific; statutes are jurisdiction-specific.
References
- [1]Patel MX, Sethi FN, Barnes TR, et al. Joint BAP NAPICU evidence-based consensus guidelines for the clinical management of acute disturbance: De-escalation and rapid tranquillisation J Psychopharmacol, 2018.PMID 29882463
- [2]Richmond JS, Berlin JS, Fishkind AB, et al. Verbal De-escalation of the Agitated Patient: Consensus Statement of the American Association for Emergency Psychiatry Project BETA De-escalation Workgroup West J Emerg Med, 2012.PMID 22461917
- [3]Wilson MP, Pepper D, Currier GW, et al. The psychopharmacology of agitation: consensus statement of the american association for emergency psychiatry project Beta psychopharmacology workgroup West J Emerg Med, 2012.PMID 22461918
- [4]Nordstrom K, Zun LS, Wilson MP, et al. Medical evaluation and triage of the agitated patient: consensus statement of the american association for emergency psychiatry project BETA medical evaluation workgroup West J Emerg Med, 2012.PMID 22461915
- [5]Huf G, Coutinho ES, Adams CE, et al. Rapid tranquillisation in psychiatric emergency settings in Brazil: pragmatic randomised controlled trial of intramuscular haloperidol versus intramuscular haloperidol plus promethazine BMJ, 2007.PMID 17954515
- [6]Raveendran NS, Tharyan P, Alexander J, et al. Rapid tranquillisation in psychiatric emergency settings in India: pragmatic randomised controlled trial of intramuscular olanzapine versus intramuscular haloperidol plus promethazine BMJ, 2007.PMID 17954514
- [7]Isbister GK, Calver LA, Page CB, et al. Randomized controlled trial of intramuscular droperidol versus midazolam for violence and acute behavioral disturbance: the DORM study Ann Emerg Med, 2010.PMID 20868907
- [8]Calver L, Page CB, Downes MA, et al. The Safety and Effectiveness of Droperidol for Sedation of Acute Behavioral Disturbance in the Emergency Department Ann Emerg Med, 2015.PMID 25890395
- [9]Foo LK, Duffull SB, Calver L, et al. Population pharmacokinetics of intramuscular droperidol in acutely agitated patients Br J Clin Pharmacol, 2016.PMID 27530285
- [10]Isbister GK, Calver LA, Downes MA, et al. Ketamine as Rescue Treatment for Difficult-to-Sedate Severe Acute Behavioral Disturbance in the Emergency Department Ann Emerg Med, 2016.PMID 26899459
- [11]Ostinelli EG, Brooke-Powney MJ, Li X, et al. Haloperidol for psychosis-induced aggression or agitation (rapid tranquillisation) Cochrane Database Syst Rev, 2017.PMID 28758203
- [12]Huf G, Alexander J, Gandhi P, et al. Haloperidol plus promethazine for psychosis-induced aggression Cochrane Database Syst Rev, 2016.PMID 27885664
- [13]Anderson EL, Nordstrom K, Wilson MP, et al. American Association for Emergency Psychiatry Task Force on Medical Clearance of Adults Part I: Introduction, Review and Evidence-Based Guidelines West J Emerg Med, 2017.PMID 28210358
- [14]Wilson MP, Nordstrom K, Anderson EL, et al. American Association for Emergency Psychiatry Task Force on Medical Clearance of Adult Psychiatric Patients. Part II: Controversies over Medical Assessment, and Consensus Recommendations West J Emerg Med, 2017.PMID 28611885
- [15]Spencer BWJ, Gergel T, Hotopf M, et al. Unwell in hospital but not incapable: cross-sectional study on the dissociation of decision-making capacity for treatment and research in in-patients with schizophrenia and related psychoses. Br J Psychiatry, 2018.PMID 29909778
- [16]Huf G, Coutinho ES, Adams CE, et al. Physical restraints versus seclusion room for management of people with acute aggression or agitation due to psychotic illness Psychol Med, 2012.PMID 22405443
- [17]Knox DK, Holloman GH Jr Use and avoidance of seclusion and restraint: consensus statement of the american association for emergency psychiatry project BETA seclusion and restraint workgroup West J Emerg Med, 2012.PMID 22461919
- [18]Stowell KR, Florence P, Harman HJ, et al. Psychiatric evaluation of the agitated patient: consensus statement of the american association for emergency psychiatry project BETA psychiatric evaluation workgroup West J Emerg Med, 2012.PMID 22461916