Psych · Emergency psychiatry
Acute behavioural disturbance and excited delirium presentations
Also known as Acute behavioural disturbance · Acute behavioral disturbance · Severe behavioural disturbance · Excited delirium · Excited delirium syndrome · Hyperactive delirium with severe agitation · Agitated delirium · Extreme agitation emergency
Fellowship-depth topic on extreme acute behavioural disturbance (ABD) and contested excited-delirium (ExDS) presentations — ABD-first framing, medical resuscitation, hyperthermia and rhabdomyolysis risk, restraint hazards including positional asphyxia, ANZ ED droperidol and ketamine evidence, Project BETA and BAP principles, capacity and least-restrictive care, custody interface. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Extreme behavioural emergencies sit at the interface of emergency medicine, toxicology, psychiatry, and — too often — custody. This leaf goes deeper than the general agitation and rapid-tranquillisation ladder: it is about physiology that can kill, language that can mislead, and systems that must prioritise medical care over forensic labelling.[2][3][11]
Overview and definition — ABD first
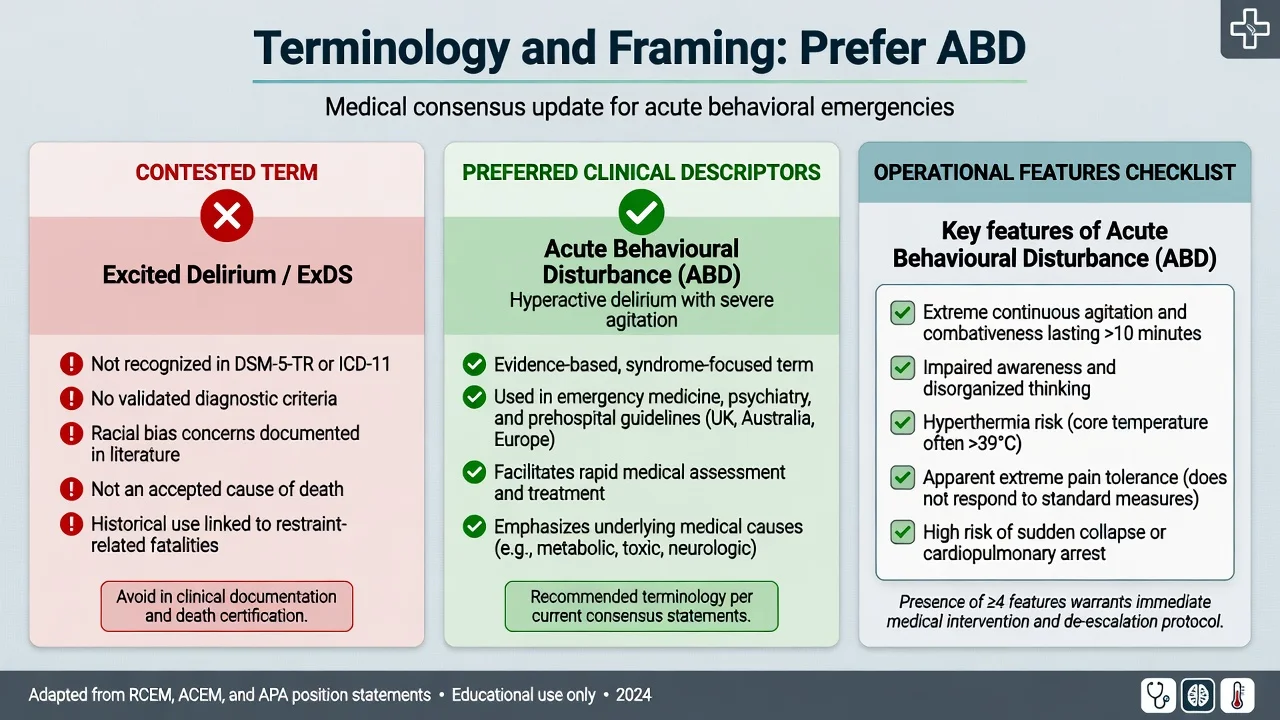
Acute behavioural disturbance (ABD) (also severe behavioural disturbance, SBD) is an operational clinical presentation: extreme agitation, aggression, and behavioural dysregulation that threatens safety and may be accompanied by medical instability. ABD is not a DSM-5-TR or ICD-11 diagnosis. You manage the syndrome while identifying stimulant toxicity, psychosis, mania, delirium, hypoxia, hypoglycaemia, head injury, encephalitis, or withdrawal as drivers.[2][11][13]
Excited delirium / excited delirium syndrome (ExDS) historically described a constellation of extreme agitation, delirium, autonomic hyperactivity, and risk of sudden death, often in stimulant or restraint contexts.[4][5] That literature is real but contested: the construct is not a validated nosological entity in DSM-5-TR or ICD-11, evidence quality is low, and the term has been used as a cause of death in ways that can obscure trauma, positional asphyxia, and racial bias in custody deaths.[1][2][3][17]
Classification and contested terminology
| Construct | Status for exams | Clinical use |
|---|---|---|
| ABD / SBD | Preferred operational language (UK/ANZ ED culture) | Severity tiering and pathway activation |
| Hyperactive delirium with severe agitation | Descriptive medical syndrome language | Extreme agitation plus impaired awareness |
| Excited delirium / ExDS | Contested; ACMT and multiple colleges deprecate as diagnosis/cause of death | Historical literature only — do not certify death on this alone |
| Routine acute agitation | Separate RT ladder topic | De-escalation → oral → single IM agent |
The American College of Medical Toxicology (2023) explicitly recommends ending use of the term excited delirium because it is applied across heterogeneous causes and has become associated with racism and forensic misuse.[1] Systematic review evidence for ExDS as a discrete, well-defined entity is low to very low certainty.[3] Scoping reviews still show incomplete inter-specialty consensus — another reason to use descriptive ABD language and physiological facts.[17]
Severity for pathway choice maps intervention intensity to danger and monitoring need.
| Tier | Cues | Response |
|---|---|---|
| Mild–moderate agitation | Engageable, no continuous extreme motor storm | De-escalation ± oral RT (see RT topic) |
| Severe agitation | Imminent harm, oral impossible | Single-agent IM RT + monitoring |
| Extreme ABD / SBD | Continuous extreme agitation, hyperthermia risk, collapse risk, prolonged struggle | Medical resuscitation capacity, airway-ready sedation, safe positioning |
Epidemiology and risk context
Extreme ABD is less common than routine ED agitation but disproportionately drives prehospital, custody, and ED critical incidents. Stimulant intoxication (methamphetamine, cocaine, synthetic stimulants) is over-represented in severe Australian ED behavioural disturbance series that underpin droperidol and ketamine pathways.[7][8][10] Mortality risk concentrates where prolonged struggle, restraint (especially prone), hyperthermia, metabolic acidosis, and rhabdomyolysis coexist.[4][16] Historical ExDS death certifications have been disproportionately applied to Black men in custody — a fact every examiner-level candidate should be able to state and a reason to abandon the label as a diagnostic shortcut.[1][2]
Pathophysiology — final common pathway and restraint risk
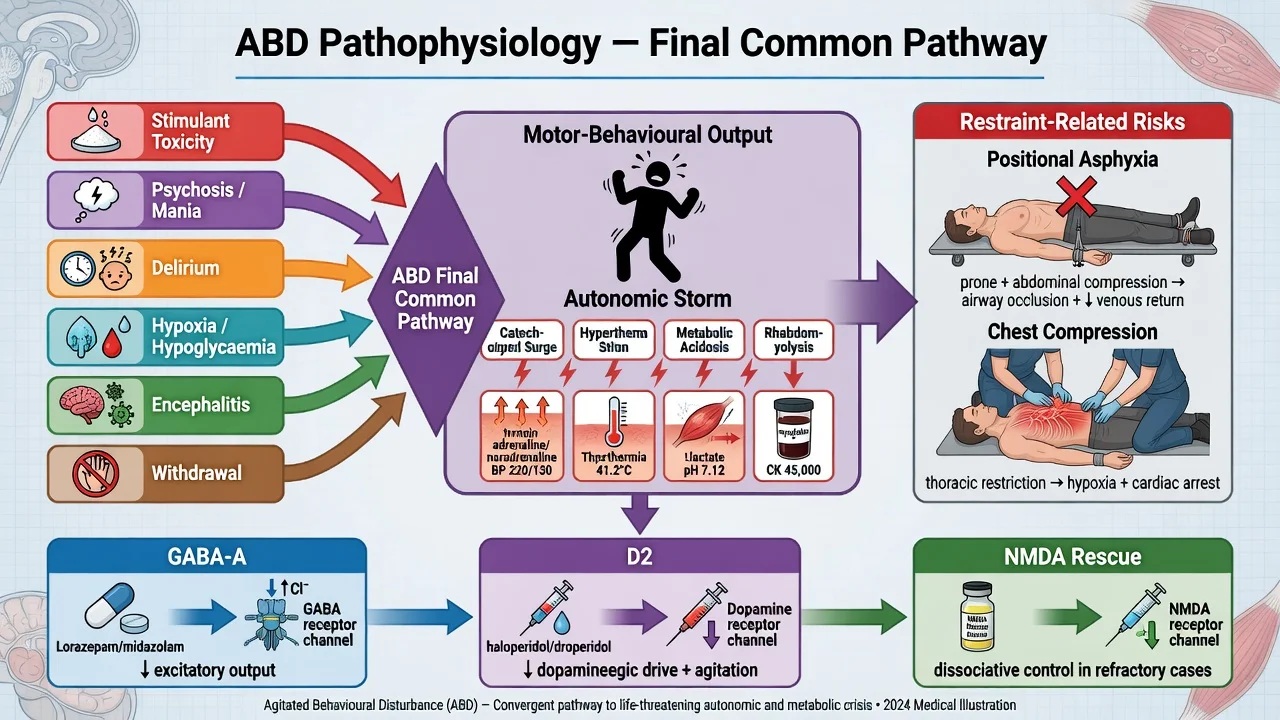
Many drivers converge on extreme motor output and a hyperadrenergic state: catecholamine surge, tachycardia, diaphoresis, hyperthermia, lactic acidosis, rhabdomyolysis, and risk of fatal arrhythmia or cardiorespiratory collapse after prolonged struggle.[4][5][6] Historical forensic neurochemistry work (for example dopamine transporter and heat-shock protein findings in postmortem series) has been used to argue a dopaminergic hyperdrive model; treat this as hypothesis-level forensic literature, not a bedside diagnostic test or a licence to stop looking for restraint contribution.[3][5]
Restraint is not pathophysiologically neutral. Prone restraint and chest compression can produce prone restraint cardiac arrest / positional asphyxia pathways that must be considered independently of any behavioural label.[16] In viva answers, always separate: (1) underlying medical/psychiatric/toxic drivers; (2) struggle physiology; (3) mechanical effects of restraint.
Pharmacological targets once behavioural control is needed:
- GABA-A positive modulation — benzodiazepines (anxiolysis/sedation; preferred when withdrawal or pure anxiety dominates)
- D2 antagonism — droperidol, haloperidol, olanzapine (psychotic drive and ED SBD protocols)
- NMDA antagonism — ketamine rescue for refractory severe ABD under critical-care governance
Clinical presentation
Scene and safety
Prehospital or ED handover after police involvement, chase, or restraint is classic. Clear the space of weapons and surplus audience; assign roles; one lead communicator if any verbal engagement is still possible. Heroism without a team is not a competency.[12][15]
Phenomenology of extreme ABD
Expect continuous extreme motor activity, shouting or incoherent speech, apparent indifference to pain or injury, invasion of space, diaphoresis, marked tachycardia, and temperature elevation or heat-risk environment. Sudden quietness after struggle can mean impending collapse, not successful de-escalation.[4][5][13] Distinguishing disorganised, delirious agitation from purposeful instrumental aggression matters for differential and for how you staff the room.
MSE under constraint
Capture what you safely can: orientation and attention fluctuation, threat content, substance clues, suicidality if accessible, and medical red flags (focal neurology, trauma marks, meningism cues). Full formal MSE waits until the person is calm and oxygenating.[13]
Differential diagnosis — medical mimics first
Never-miss list with discriminators:
- Stimulant / sympathomimetic toxicity — mydriasis, tachycardia, hyperthermia, paranoia after methamphetamine or cocaine
- Primary psychosis or mania — after medical screen; less likely pure first presentation of “ExDS” without work-up
- Delirium (sepsis, hypoxia, metabolic, trauma, encephalitis including autoimmune) — inattention and fluctuation
- Alcohol or sedative withdrawal / DT — tremor, autonomic arousal, seizures
- Serotonin toxicity / NMS / anticholinergic toxicity — tempo, clonus versus lead-pipe rigidity, drug history
- Hypoglycaemia, hypoxia, post-ictal state, thyroid storm
- Head injury after struggle or fall
Medical evaluation is history- and examination-driven, not a ritual pan-lab for every mild agitation — but extreme ABD with hyperthermia or collapse demands aggressive physiological assessment.[13]
Clinical and bedside assessment
- ABCDE + capillary glucose + SpO2 + temperature
- Scene safety and team roles
- Focused history: tempo, substances, trauma, medical disease, psychiatric diagnoses, medications
- Dynamic violence risk and collapse risk
- Capacity when safe enough to assess (often impaired in extreme ABD)
- Legal status and least-restrictive options for ongoing care
- Collateral and police/ambulance timeline including restraint duration and position
ED protocols may use a Sedation Assessment Tool or RASS-style scores to structure observation; they do not replace clinical judgment or disposition thinking.[8]
Investigations
| Priority | Test | Why |
|---|---|---|
| Immediate | Vitals, glucose, SpO2, temperature | Hypoglycaemia, hypoxia, hyperthermia kill first |
| Concurrent with sedation plan | ECG (QTc) as soon as practicable | Butyrophenone cardiac risk context |
| Extreme exertion / restraint | CK, U&E, FBC, VBG/ABG | Rhabdomyolysis, acidosis, renal injury |
| Overdose context | Paracetamol ± others | Concurrent self-poisoning |
| Red flags | Imaging, LP, EEG, infection/autoimmune panels | Do not delay life-saving care for low-yield tests |
| Substance | UDS with known limitations | Negative screen does not exclude |
Do not delay necessary parenteral sedation of extreme ABD for a urine drug screen.[13][14]
Management — resuscitation of extreme ABD
Principles
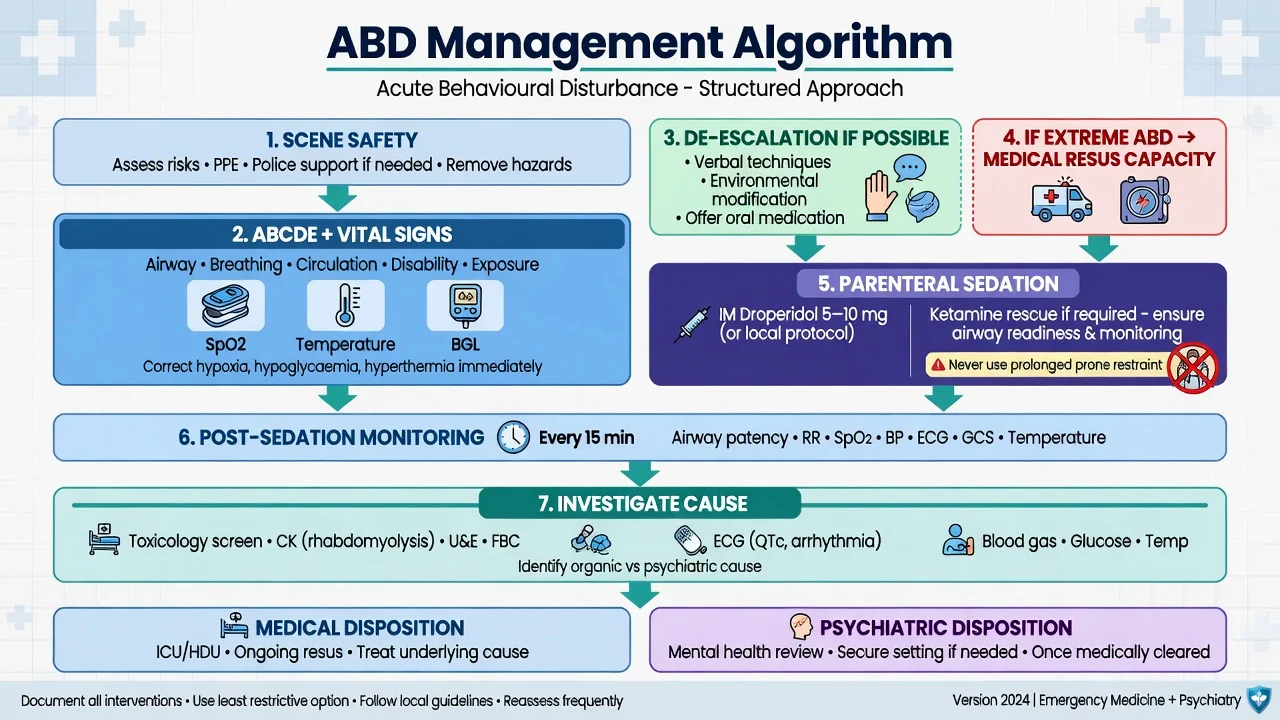
- Treat extreme ABD as a medical emergency with airway-ready staff.
- De-escalate if still possible (Project BETA: one communicator, respect space, concise language, offer choices).[12]
- Control behaviour quickly enough to allow assessment — endpoint calm and rousable, not unconscious.[11][14]
- Never prolonged prone restraint; minimise physical force duration; reassess airway and ventilation continuously during any hold.[15][16]
- Cool if hyperthermic; support circulation; plan for rhabdomyolysis.
- Document physiology and restraint details; avoid ExDS as a standalone diagnosis.[1][2]
Named parenteral options for extreme ABD (adult, setting-specific)
These sit alongside the general RT ladder in the companion topic; extreme ED/prehospital ABD often follows local toxicology-led protocols rather than ward BAP first-line alone.[7][11]
| Agent | Typical dose / route | Notes |
|---|---|---|
| Droperidol | 5–10 mg IM (often 10 mg initial in ED series) | ANZ ED first-line for undifferentiated ABD/SBD; DORM and multi-centre safety data; ECG context |
| Midazolam | 5–10 mg IM | Rapid; more airway/oversedation vigilance and redosing in comparative work |
| Ketamine rescue | Approximately 4–5 mg/kg IM under local protocol | Difficult-to-sedate severe ABD; prehospital and ED series; airway readiness mandatory |
| Lorazepam | 1–2 mg IM | Useful when anxiety/withdrawal dominates; single-agent logic on wards |
| Olanzapine | 5–10 mg IM | Not with parenteral benzodiazepine |
| Haloperidol + promethazine | 5 mg + 25–50 mg IM | TREC-backed psychiatric RT combination when cardiac risk allows |
Absolute combination ban: never give IM olanzapine with a parenteral benzodiazepine (profound respiratory depression risk). If one has been given, wait at least 1 hour, monitor continuously, and only then consider the other under senior oversight.[11][14]
Ketamine is rescue or specialised extreme-ABD control under ED/critical-care governance — not default first-line on a general psychiatry ward without airway support.[9][10]
Post-sedation monitoring
After parenteral sedation for ABD:
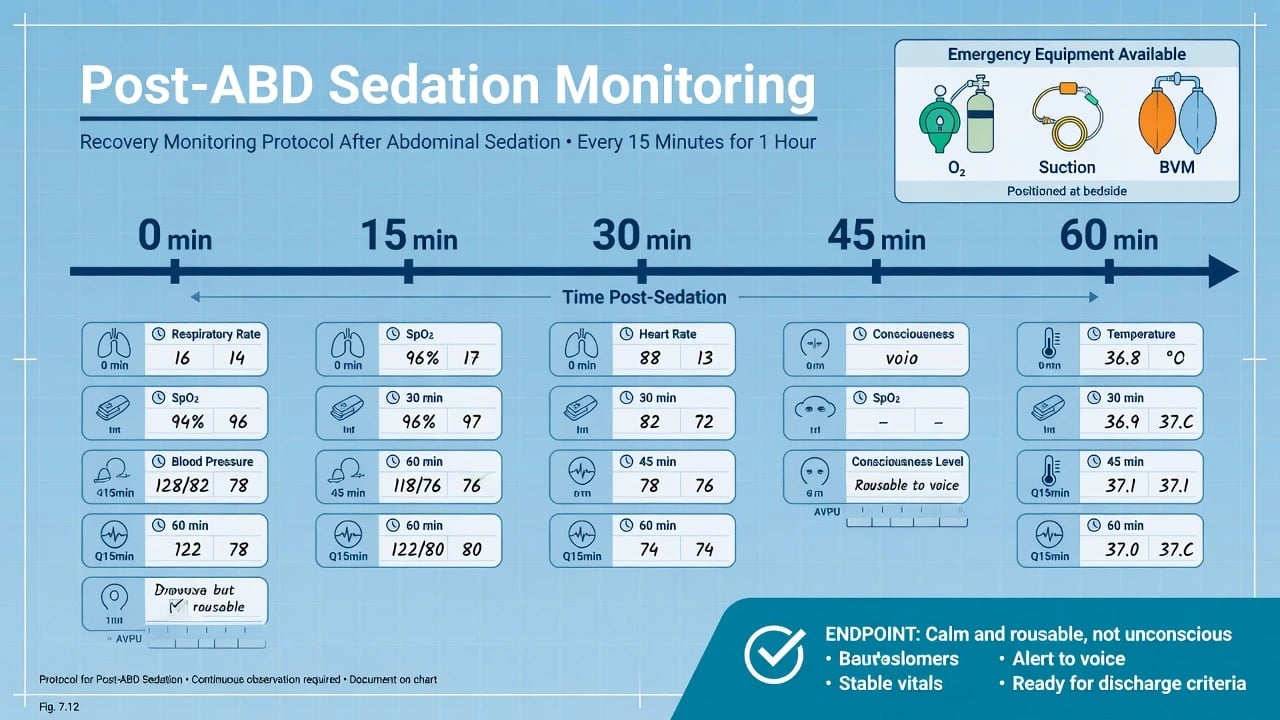
- Continuous observation until ambulatory and conversant when possible
- Respiratory rate, SpO2, BP, HR, consciousness, temperature every 15 minutes for at least 1 hour
- Oxygen, suction, bag-valve-mask available
- Recheck CK/U&E trajectory if extreme exertion
- Document recovery and any further doses
After the calm — definitive care
Treat the driver: stimulant observation, psychosis/mania pathway, delirium work-up, withdrawal protocols. Debrief patient and staff after restrictive practices. Write a contemporaneous note covering risks, de-escalation attempts, restraint position and duration, capacity, legal basis, agent/dose/route/time, monitoring, response, and review plan.[11][15][18]
Specific scenarios
Methamphetamine ED ABD. Medical observations for hyperthermia and arrhythmia; ANZ evidence supports IM droperidol; midazolam alternative; ketamine if refractory under protocol.[7][8][9]
Police/custody interface. Prioritise medical assessment over narrative labels; record restraint details; transfer to ED with full timeline; avoid ExDS as a bureaucratic cause-of-death shortcut.[1][2][16]
Inpatient escalation. Follow BAP/NAPICU oral-then-single-IM principles for severe agitation; if physiology becomes extreme (hyperthermia, collapse risk), escalate to medical emergency response and ED-level monitoring rather than stacking unmonitored sedatives on the ward.[11]
Post-restraint collapse. Immediate ALS approach; consider acidosis, hyperkalaemia from rhabdomyolysis, trauma, and asphyxia mechanisms — not “excited delirium arrest” as a thought-terminating cliché.[16]
Complications and pitfalls
- Positional asphyxia / prone restraint cardiac arrest
- Respiratory depression and aspiration from polypharmacy
- Hyperthermia, rhabdomyolysis, acute kidney injury, arrhythmia
- Missed medical mimic labelled “behavioural”
- Using ExDS language to skip investigation of trauma or restraint contribution
- Akathisia misread as worsening agitation
- Inventing Mental Health Act section numbers across jurisdictions
- Racial bias and dehumanising language in documentation
Prognosis and disposition
| Destination | When |
|---|---|
| Medical ED / ICU | Unstable vitals, severe hyperthermia, deep sedation, rhabdomyolysis, airway need |
| ED observation | Evolving toxicity, incomplete work-up, short-term safety |
| Psychiatric inpatient (voluntary) | Residual psychiatric risk, accepts care, medical risk controlled |
| Involuntary pathway | Serious risk + statutory criteria; least-restrictive rationale documented |
| Immediate discharge | Rare after true extreme ABD |
Handover must include agents, doses, times, vital-sign trajectory, temperature, restraint details, residual risk, and outstanding investigations.[11]
Special populations
Older adults. Delirium until proven otherwise; start at approximately half adult sedation doses; high fall and QTc risk.[11][13]
Pregnancy. Avoid prone restraint; involve obstetrics early; agent choice with specialist advice.[11][15]
Intellectual disability / autism. Sensory overload and pain may drive behaviour; environmental modification first; high risk of traumatic restraint experiences.[11]
Racially minoritised patients. Contested ExDS terminology has been applied disproportionately in custody deaths of Black people; use descriptive ABD language and document facts, not stereotypes.[1][2]
Children and adolescents. Weight-based dosing under paediatric/CAMHS sedation governance; minimise restraint trauma.[11]
Capacity, law and least-restrictive care
Capacity is decision-specific and time-specific: understand, retain, use/weigh, communicate. Extreme ABD often impairs capacity for treatment and remaining in care, but assessment must still be explicit when feasible.[18] Prefer voluntary care and oral options when safe. Involuntary treatment and restrictive practices require serious risk (or statutory criteria), documented failure of less restrictive options, and scheduled review. Do not invent section numbers for Australia, New Zealand, England, or the United States — state principles and apply local statute with senior advice.[11][15][18]
Evidence, guidelines and regional differences
Landmark evidence to name: ACMT 2023 (end ExDS term); McGuinness and Lipsedge 2022 (ABD and diagnostic critique); Gonin 2018 systematic review (low certainty for ExDS construct); Takeuchi 2011 and Vilke reviews (historical ExDS clinical descriptions and treatment considerations); DORM 2010 and Calver 2015 (droperidol); Isbister 2016 and Isoardi 2021 (ketamine); BAP/NAPICU 2018; Project BETA suite; Weedn 2022 (prone restraint cardiac arrest).[1][2][3][4][5][7][8][9][10][11][16]
Exam pearls
ABD-SAFE
- Prefer ABD framing; know why ExDS is contested.
- Name droperidol 5–10 mg IM and ketamine rescue doses with governance.
- Never IM olanzapine + parenteral BZD.
- Endpoint is calm and rousable; observations every 15 minutes for ≥1 hour.
- Prone restraint is a death pathway, not a technique of last resort to leave unsupervised.
- Capacity is decision-specific; statutes are jurisdiction-specific.
- Classic stem: hot day, methamphetamine, police struggle, hyperthermia — medical resus, not a label.
References
- [1]Stolbach AI, Dargan PI, Greller HA, et al. ACMT Position Statement: End the Use of the Term "Excited Delirium" J Med Toxicol, 2023.PMID 37349654
- [2]McGuinness T, Lipsedge M 'Excited Delirium', acute behavioural disturbance, death and diagnosis Psychol Med, 2022.PMID 35546291
- [3]Gonin P, Beysard N, Yersin B, Carron PN Excited Delirium: A Systematic Review Acad Emerg Med, 2018.PMID 28990246
- [4]Takeuchi A, Ahern TL, Henderson SO Excited delirium West J Emerg Med, 2011.PMID 21691475
- [5]Vilke GM, DeBard ML, Chan TC, et al. Excited Delirium Syndrome (ExDS): defining based on a review of the literature J Emerg Med, 2012.PMID 21440403
- [6]Vilke GM, Bozeman WP, Dawes DM, et al. Excited delirium syndrome (ExDS): treatment options and considerations J Forensic Leg Med, 2012.PMID 22390995
- [7]Isbister GK, Calver LA, Page CB, et al. Randomized controlled trial of intramuscular droperidol versus midazolam for violence and acute behavioral disturbance: the DORM study Ann Emerg Med, 2010.PMID 20868907
- [8]Calver L, Page CB, Downes MA, et al. The Safety and Effectiveness of Droperidol for Sedation of Acute Behavioral Disturbance in the Emergency Department Ann Emerg Med, 2015.PMID 25890395
- [9]Isbister GK, Calver LA, Downes MA, Page CB Ketamine as Rescue Treatment for Difficult-to-Sedate Severe Acute Behavioral Disturbance in the Emergency Department Ann Emerg Med, 2016.PMID 26899459
- [10]Isoardi KZ, Parker LE, Page CB, et al. Ketamine as a rescue treatment for severe acute behavioural disturbance: A prospective prehospital study Emerg Med Australas, 2021.PMID 33202484
- [11]Patel MX, Sethi FN, Barnes TR, et al. Joint BAP NAPICU evidence-based consensus guidelines for the clinical management of acute disturbance: De-escalation and rapid tranquillisation J Psychopharmacol, 2018.PMID 29882463
- [12]Richmond JS, Berlin JS, Fishkind AB, et al. Verbal De-escalation of the Agitated Patient: Consensus Statement of the American Association for Emergency Psychiatry Project BETA De-escalation Workgroup West J Emerg Med, 2012.PMID 22461917
- [13]Nordstrom K, Zun LS, Wilson MP, et al. Medical evaluation and triage of the agitated patient: consensus statement of the american association for emergency psychiatry project BETA medical evaluation workgroup West J Emerg Med, 2012.PMID 22461915
- [14]Wilson MP, Pepper D, Currier GW, et al. The psychopharmacology of agitation: consensus statement of the american association for emergency psychiatry project Beta psychopharmacology workgroup West J Emerg Med, 2012.PMID 22461918
- [15]Knox DK, Holloman GH Jr Use and avoidance of seclusion and restraint: consensus statement of the american association for emergency psychiatry project BETA seclusion and restraint workgroup West J Emerg Med, 2012.PMID 22461919
- [16]Weedn V, Steinberg A, Speth P Prone restraint cardiac arrest in in-custody and arrest-related deaths J Forensic Sci, 2022.PMID 35869602
- [17]Slocum S, Fiorillo M, Harding E, et al. In pursuit of inter-specialty consensus on excited delirium syndrome: a scoping literature review Forensic Sci Med Pathol, 2023.PMID 36350497
- [18]Spencer BWJ, Gergel T, Hotopf M, Owen GS Unwell in hospital but not incapable: cross-sectional study on the dissociation of decision-making capacity for treatment and research in in-patients with schizophrenia and related psychoses. Br J Psychiatry, 2018.PMID 29909778