Psych · Emergency psychiatry
Lithium toxicity
Also known as Lithium poisoning · Lithium intoxication · Chronic lithium toxicity · Acute-on-chronic lithium toxicity · Lithium overdose · SILENT lithium
Exam-exhaustive fellowship topic on lithium toxicity — acute vs chronic vs acute-on-chronic patterns, serum levels and timing, neurotoxicity and SILENT, renal/NDI mechanisms, interactions (NSAIDs, ACEI/ARB, thiazides, dehydration), supportive care, EXTRIP extracorporeal criteria, rebound, prevention and monitoring, special populations. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Lithium remains a gold-standard maintenance mood stabiliser with a unique anti-suicide signal among classic agents, which is precisely why fellowship examiners test toxicity competence hard: candidates must rescue patients without destroying future lithium access through careless restarts or missed SILENT risk.[13][3][19][20]
Overview and definition
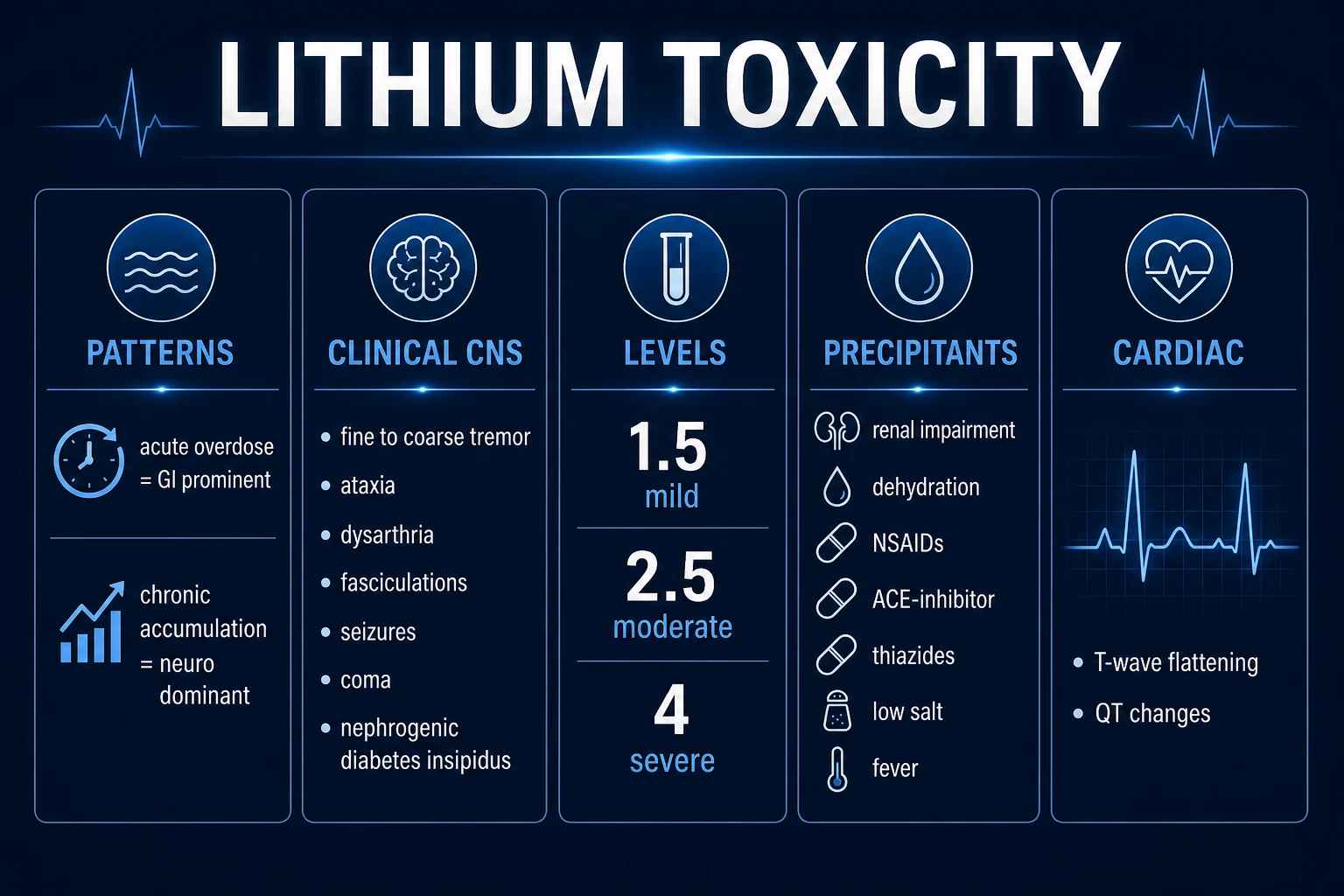
Lithium toxicity (poisoning) is clinical toxicity related to elevated lithium body burden — not a laboratory curiosity. A “toxic-looking” number without symptoms is not managed the same way as coarse tremor, ataxia, dysarthria and confusion with a modest chronic elevation. Conversely, severe neurological features force aggressive care even when the level is not astronomically high, especially in chronic accumulation where tissue stores are already saturated.[2][4][10][11]
Therapeutic adverse effects (fine resting/action tremor, mild nausea, polyuria) sit on a continuum with toxicity; the examiner wants the threshold language of coarse tremor, cerebellar signs, dysarthria, impaired consciousness and seizures as the toxicity phenotype.[3][10]
Classification — acute, chronic, acute-on-chronic
- Single large ingestion (often intentional)
- GI symptoms early (nausea, vomiting, diarrhoea)
- Serum peak may be high before brain fully loads
- Lithium-naive tissue stores may spare severe neurotoxicity early
- Therapeutic use + reduced clearance
- Neurotoxicity dominates
- Severity at lower serum levels than acute
- Precipitants: illness, dehydration, interacting drugs, declining GFR
- Extra load (overdose or accumulation) on tissue stores
- Often the most dangerous hospital phenotype
- High residual CNS risk after serum falls
- EXTRIP decisions often hinge here
Pattern of exposure predicts severity. Regional poisons-unit data show that chronic and acute-on-chronic exposures associate with more severe poisoning than isolated acute overdose at comparable serum numbers — a viva staple.[5]
Hansen and Amdisen’s classic case series framed mild/moderate/severe intoxication by clinical features and serum ranges; modern teaching still uses approximate bands (for orientation only — e.g. mild around 1.5 mmol/L band, moderate around 2.5, severe higher) while insisting that chronic neurotoxicity can be life-threatening below “severe” numerical cut-offs.[11][2][4]
Epidemiology and risk factors
Lithium’s narrow therapeutic index makes toxicity a recurring emergency and consultation-liaison presentation. Hospitalised intentional overdoses form one stream; community chronic accumulation in older adults and medically comorbid patients forms another.[14][2][3]
Risk anchors
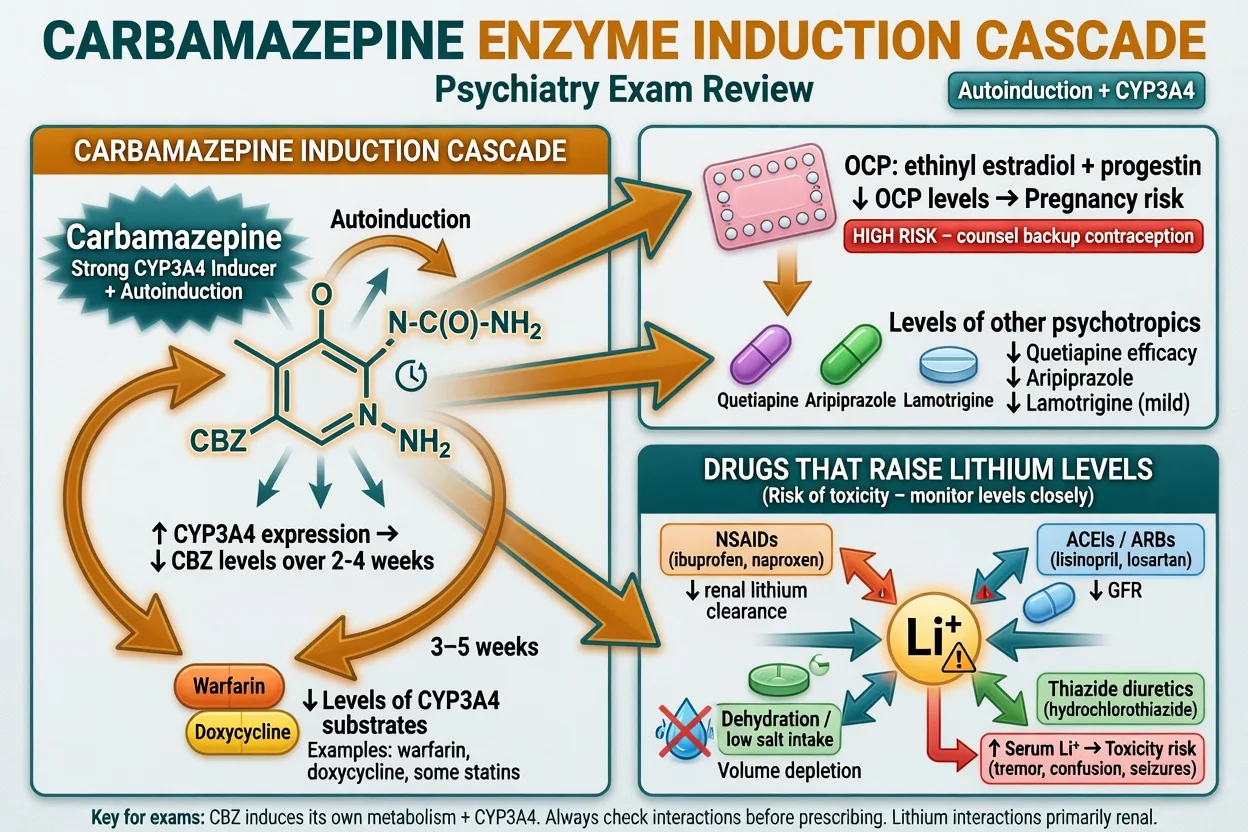
High-yield risk factors: older age, reduced eGFR, volume depletion (GI loss, poor intake, fever), low effective circulating volume, new NSAIDs, ACE inhibitors/ARBs, thiazides, low salt diets, deliberate overdose, sustained-release formulations prolonging absorption, and NDI-driven polyuria that worsens dehydration.[7][8][3][6]
Pathophysiology
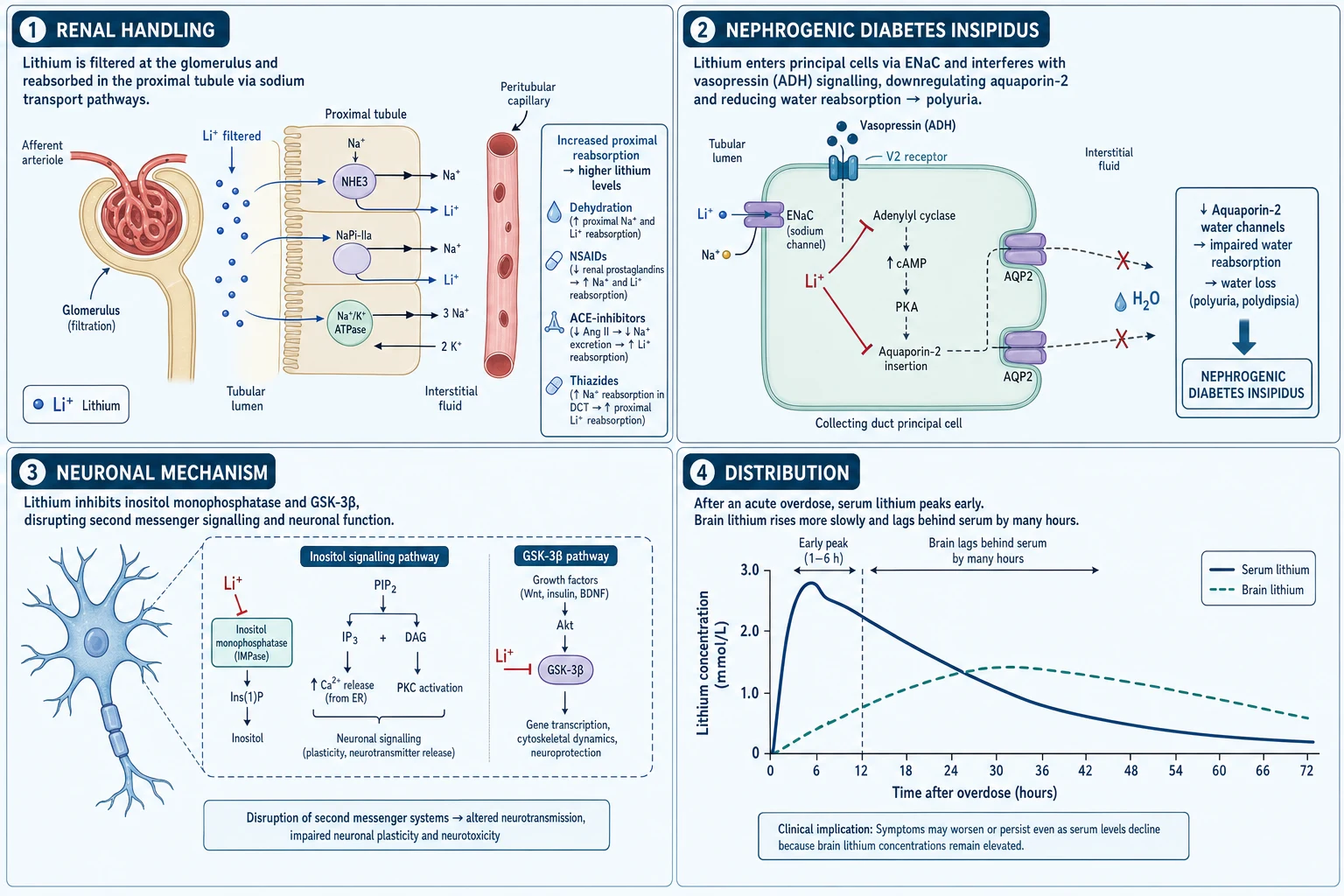
Renal handling. Lithium is freely filtered at the glomerulus and substantially reabsorbed in the proximal tubule via pathways that track sodium reabsorption. Anything that increases proximal sodium reclamation (volume depletion, thiazide-related sodium loss, reduced effective arterial blood volume) increases lithium reabsorption and raises serum levels.[6][2][10]
Interaction physiology.
- NSAIDs reduce renal prostaglandins → reduced afferent dilation / altered haemodynamics → reduced lithium clearance.[7]
- ACE inhibitors/ARBs reduce GFR and can promote lithium retention; clinical interaction data support monitoring after initiation.[8][7]
- Thiazides cause volume contraction and secondary proximal reabsorption of lithium — classic exam precipitant.[7][3]
Nephrogenic diabetes insipidus (NDI) spectrum. Chronic lithium downregulates aquaporin-2 water channels in collecting-duct principal cells, impairing concentrating ability → polyuria/polydipsia → volume depletion → further lithium retention. This vicious cycle appears in both chronic adverse-effect discussions and acute toxic presentations.[6][3][16]
Distribution lag. After acute overdose, serum lithium may peak early while brain concentrations rise more slowly and decline more slowly. Clinical implication: neurological status may worsen or persist after the serum peak falls — do not discharge on a falling number alone if the patient is still encephalopathic.[2][15][4]
Cellular teaching models. Lithium inhibits inositol monophosphatase and GSK-3β signalling; these models explain therapeutic actions and toxic neuronal dysfunction at fellowship depth without becoming speculative story-telling.[3]
Clinical presentation
Gastrointestinal: nausea, vomiting, diarrhoea — often early and prominent in acute overdose.[10][2]
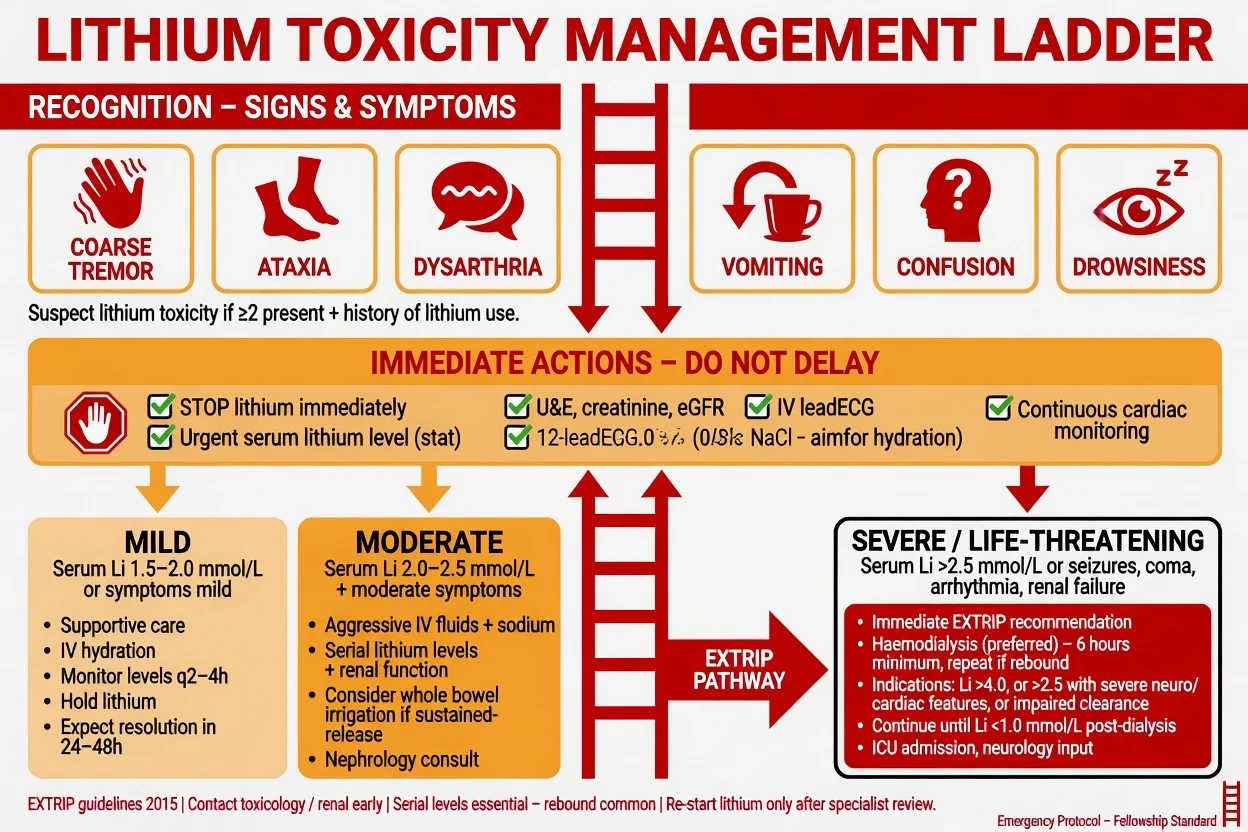
Neurological ladder (core phenotype): fine tremor becoming coarse, hyperreflexia, fasciculations, ataxia, dysarthria, nystagmus, confusion, delirium, myoclonus, seizures, coma.[10][11][2]
Chronic phenotype: neurological features dominate; GI may be quieter; serum level may be only moderately elevated relative to severity.[5][11]
Cardiac: T-wave flattening/inversion, QT changes; serious dysrhythmias are less common but are EXTRIP decision triggers when life-threatening.[2][1][10]
Atypical (examiner bait): older adult with “new delirium” after a thiazide start; polyuria from NDI misread as psychogenic polydipsia; therapeutic fine tremor mis-escalated as toxicity — or, worse, true toxicity dismissed as “usual lithium tremor.”[3][7]
Differential diagnosis
| Mimic | Discriminators favouring lithium toxicity | Discriminators favouring alternative |
|---|---|---|
| Cerebellar stroke | Progressive coarse tremor + drug history + level | Hyperacute focal onset, vascular risk, imaging |
| Wernicke encephalopathy | Lithium exposure, no ophthalmoplegia package | Alcohol/malnutrition, ophthalmoplegia, thiamine response |
| Serotonin toxicity | Lithium can contribute to serotonergic load in polypharmacy | Clonus, hyperreflexia with serotonergic agents, hyperthermia pattern |
| NMS | Rigidity less lead-pipe classic; lithium level abnormal | Antipsychotic context, marked rigidity, high CK, fever |
| Benzodiazepine/alcohol withdrawal | Li history and level | Autonomic hyperactivity, temporal link to cessation |
| Hyponatraemia/uraemia | May coexist with Li retention | Electrolyte/renal primary picture without Li exposure |
Always exclude medical drivers of agitation or reduced consciousness concurrent with lithium work-up (glucose, hypoxia, sepsis, head injury) — especially after intentional overdose or falls from ataxia.[2]
Clinical and bedside assessment
ABCDE first. Airway protection if drowsy; oxygen saturation; blood pressure and volume status; capillary glucose; temperature (hyperthermia opens NMS/serotonin/sympathomimetic differentials).[2][4]
History that scores marks: last dose time and formulation (immediate vs sustained-release), estimated total ingested if overdose, recent illness/vomiting/diarrhoea, new analgesics or antihypertensives, salt intake changes, baseline lithium dose and last known trough, suicide intent and co-ingestants, pregnancy possibility.[2][14]
Examination: cerebellar signs, myoclonus, consciousness, seizures, hydration, urine output (polyuria vs oliguria), ECG review.[10][2]
Capacity and risk. Toxicity can abolish capacity for treatment decisions; document emergency treatment rationale. After medical stabilisation, reassess suicide risk if intentional and plan psychiatric disposition.[14]
Investigations
- Serum lithium immediately — interpret with time since last dose, not as a 12-hour trough in the emergency setting. Serial levels every few hours until clearly falling and the patient is improving.[4][2][12]
- U&E, creatinine/eGFR, sodium — clearance and precipitants.[6][2]
- Calcium and TFT context for chronic lithium users (hyperparathyroidism/hypothyroidism background), though acute management is not driven by TFT alone.[17][16]
- ECG and continuous monitoring when moderate–severe or cardiac symptoms.[2]
- CK after prolonged seizures/immobility; pregnancy test when relevant; paracetamol/salicylate and other co-ingestant tests in deliberate overdose.[14][2]
Management — resuscitation
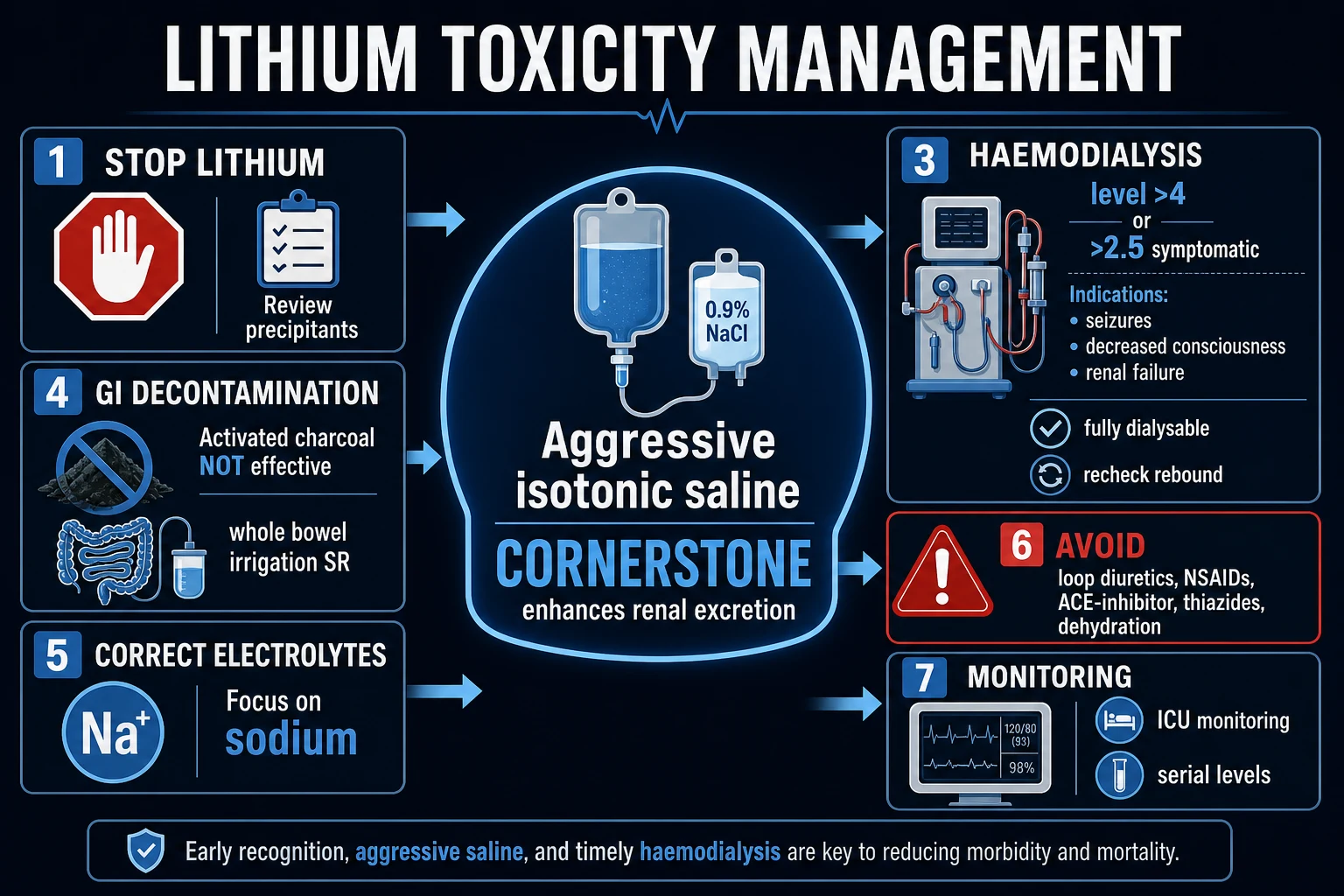
- Stop lithium and hold interacting drugs (NSAIDs, ACEI/ARB, thiazides) pending review.[4][7]
- Airway, breathing, circulation support; benzodiazepines as first-line for seizures in standard emergency frameworks.[2][4]
- IV isotonic saline to correct volume depletion and support renal perfusion/clearance when the patient is volume depleted — the supportive cornerstone in most series and reviews. Avoid treating euvolemic patients with reckless fluid overload; target euvolemia and urine output rather than forced diuresis mythology.[4][15][2]
- Do not use activated charcoal for lithium — lithium is not bound by charcoal. Whole bowel irrigation may be considered for large recent sustained-release ingestions under toxicology guidance (position-paper context for selected overdoses).[4][18][2]
- Avoid loop-diuretic “forced diuresis” as a primary detox strategy and avoid further nephrotoxic or lithium-retaining drugs.[4][6]
- Early toxicology and nephrology when features are more than mild or clearance is impaired.[1][2]
Management — definitive and EXTRIP
Supportive clearance and serial levels
Most mild–moderate cases resolve with lithium cessation, volume repletion, removal of precipitants, and observation with serial levels and neurological checks. Pharmacokinetic work shows clearance measures matter; extracorporeal therapy is reserved for severe or poorly clearing cases.[15][4][14]
EXTRIP extracorporeal treatment (must-know)
The Extracorporeal Treatments in Poisoning (EXTRIP) workgroup concluded lithium is dialyzable (evidence level A) and issued consensus recommendations (evidence quality is low overall — mostly case-level data — but these are the global exam standard).[1]
Recommended extracorporeal treatment (ECTR):
- Severe lithium poisoning; or
- Impaired kidney function and lithium greater than 4.0 mEq/L (mmol/L); or
- Decreased level of consciousness, seizures, or life-threatening dysrhythmias — irrespective of lithium concentration.[1]
Suggested ECTR:
- Lithium greater than 5.0 mEq/L; or
- Significant confusion; or
- Expected time to reduce lithium to less than 1.0 mEq/L with optimal management is greater than 36 hours.[1]
Continue ECTR until clinical improvement is apparent or lithium is less than 1.0 mEq/L. If the level is not readily measurable, continue at least 6 hours. Haemodialysis is preferred; continuous RRT is an acceptable alternative when HD is not available or not tolerated.[1]
After the crisis
- Document precipitant (drug, illness, overdose intent).
- Counsel on sick-day rules: hold lithium and seek advice with significant dehydration/vomiting/diarrhoeal illness per local protocol.
- Recheck interacting medicines with GP/pharmacy.
- Restart decision only after renal recovery, neurological recovery, and shared decision: lithium’s anti-suicide and maintenance value may still justify carefully supervised restart; alternatives if renal trajectory forbids it.[3][13][19][20]
- Intentional overdose: full suicide risk assessment, means restriction for remaining lithium supply, and appropriate psychiatric disposition.[14]
Specific subtypes and scenarios
Acute massive overdose (often lithium-naive). GI symptoms early; very high early levels possible; still watch for delayed neurotoxicity as distribution continues; SR products may need prolonged observation and toxicology-guided decontamination strategy.[2][14][18]
Chronic accumulation. Older adult, new thiazide/NSAID/ACEI, gastroenteritis, declining GFR — neuro-dominant toxicity at mid-range levels. Highest yield outpatient prevention scenario.[5][7][8]
Acute-on-chronic. Extra dose or reduced clearance on established body stores — often severe; EXTRIP thresholds more often met.[5][2]
Inpatient iatrogenic. Post-operative fluid restriction, NSAID analgesia, ACEI for hypertension, low-salt diet — systems failure as much as pharmacology.[7]
Complications and pitfalls
- SILENT (syndrome of irreversible lithium-effectuated neurotoxicity): persistent cerebellar, extrapyramidal, or cognitive deficits after lithium levels normalise — fear this more than transient tremor; early aggressive control of severe toxicity aims to reduce permanent injury risk.[9]
- Post-dialysis rebound.[1][15]
- Mis-timed levels (treating a random level as trough, or discharging on a falling level with ongoing encephalopathy).[12][2]
- Charcoal reflex without knowing lithium is not bound.[4]
- Restarting lithium unchanged into the same NSAID/thiazide/ACEI regimen.[7]
- Missing medical differentials (stroke, Wernicke, other toxidromes).[2]
Prognosis and disposition
Most patients recover with supportive care. Severity and residual neuro risk track exposure pattern (chronic/acute-on-chronic worse), peak clinical encephalopathy, seizures, and delayed treatment more than a single number.[5][11][9]
Disposition tree: home only if mild, precipitant fixed, levels falling, safe supports, follow-up timed; ward observation for moderate; HDU/ICU and dialysis-capable centre for severe neurological or cardiac features; psychiatric admission or intensive community follow-up after intentional overdose once medically stable.[2][14]
Special populations
Older adults. Lower maintenance targets often appropriate; reduced GFR; delirium as presentation; polypharmacy interaction risk. Interpret levels with frailty and timing.[12][3][16]
Renal impairment. Toxicity risk high; lithium often dose-reduced or avoided long-term; ECTR thresholds more readily met when clearance is poor.[1][6][17]
Pregnancy. Volume and GFR shifts change levels across trimesters and postpartum; toxicity and subtherapeutic states both possible. Ongoing lithium in pregnancy is a nuanced shared decision (cardiac malformation risk context from large cohort data is lower than older dogma but not zero) — coordinate perinatal psychiatry/obstetrics; toxicity management still follows medical principles with fetal monitoring as indicated.[3][19]
Youth. Chronic toxicity less common than adult long-term use, but intentional overdose occurs; involve caregivers and child/adolescent psychiatry for disposition.[14]
Prevention and monitoring
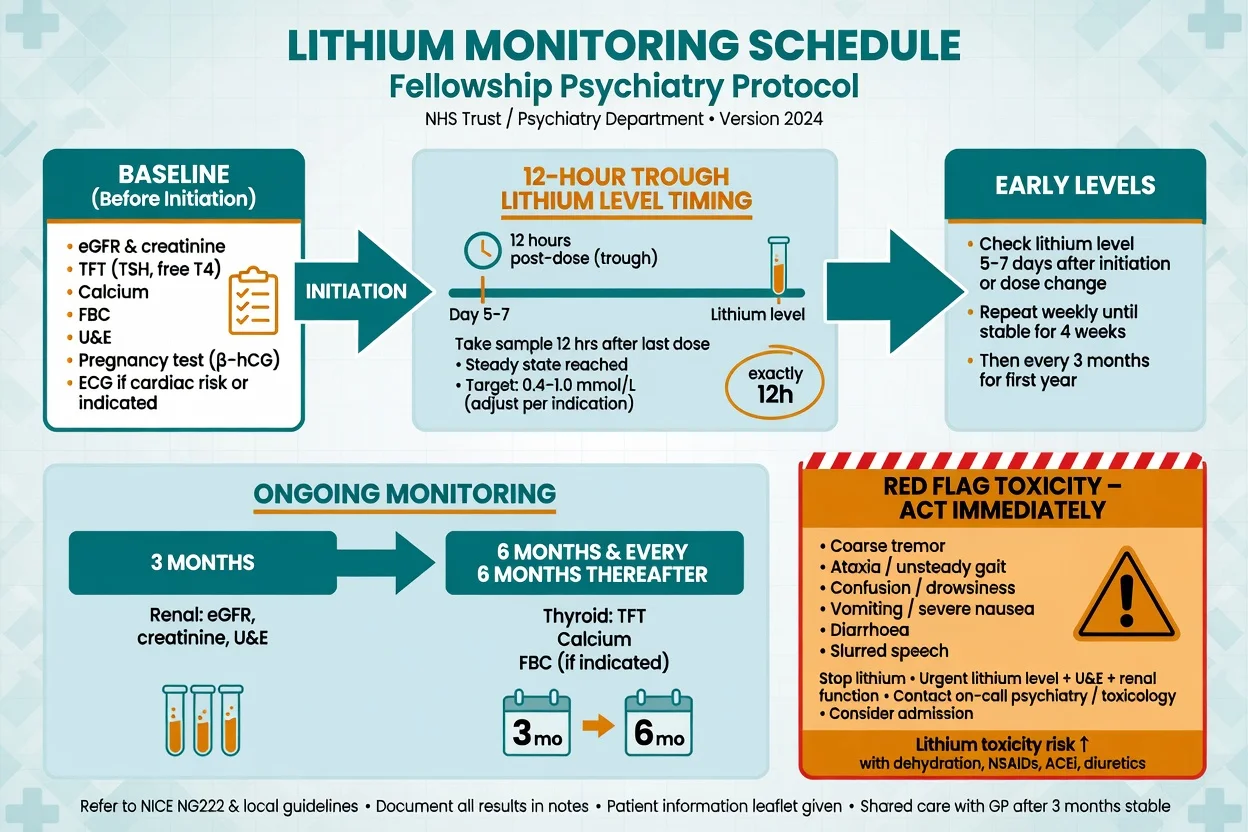
Baseline before lithium (maintenance practice): U&E/creatinine/eGFR, TFT, calcium, weight, pregnancy test when relevant, ECG if cardiac risk — then 12-hour troughs after initiation/dose change and periodic renal–thyroid–calcium surveillance.[12][3][20][19]
Target ranges. ISBD/IGSLI synthesises maintenance levels commonly around 0.6–0.8 mmol/L for many adults, with individualisation (often lower in older adults; higher short-term bands sometimes used in acute mania under close supervision).[12]
Sick-day and interaction counselling is part of every lithium prescription — not optional health promotion.[3][7]
Evidence, guidelines and regional differences
ANZ practice keeps lithium as a core bipolar maintenance option with structured monitoring (RANZCP-aligned culture) and low threshold for medical admission in toxicity. UK practice similarly emphasises lithium registers/shared-care monitoring infrastructure. North American sources commonly cite EXTRIP for extracorporeal decisions and CANMAT/ISBD hierarchical bipolar guidance for when lithium is worth preserving after recovery. The exam constant across regions: pattern recognition, interaction precipitants, EXTRIP thresholds, and rebound — not a single national fluid recipe.[1][19][20][12]
Landmark anchors to name: EXTRIP 2015 (Decker); Hansen–Amdisen classic intoxication series; Timmer JASN physiology; Waring exposure-pattern and management reviews; Baird-Gunning ICU poisoning review; Finley interaction updates; Gitlin side-effect strategies; McKnight toxicity-profile meta-analysis; Shine long-term renal/thyroid/parathyroid laboratory outcomes; ISBD/IGSLI level task force; Cipriani suicide meta-analysis (why lithium remains worth careful use).[1][11][6][5][4][2][7][3][16][17][12][13]
Exam pearls
LITHIUM
- Chronic toxicity can be severe at modest levels.[5][11]
- EXTRIP recommended: impaired kidney function + Li >4.0, or decreased consciousness / seizures / life-threatening dysrhythmias at any level, or severe poisoning generally.[1]
- EXTRIP suggested: Li >5.0, significant confusion, or expected time to Li <1.0 longer than 36 h.[1]
- HD preferred; watch rebound.[1]
- SILENT = irreversible neurotoxicity after levels normalise.[9]
- Do not casually abandon lithium forever after a precipitated chronic toxicity without fixing the precipitant — anti-suicide and maintenance value may still favour supervised restart.[13][3][19]
Self-test: name the EXTRIP recommended criteria
Recommended ECTR if severe lithium poisoning; or impaired kidney function with Li >4.0 mEq/L; or decreased consciousness, seizures, or life-threatening dysrhythmias at any Li concentration. Suggested if Li >5.0, significant confusion, or expected time to Li <1.0 mEq/L >36 h. Continue until clinical improvement or Li <1.0; HD preferred; recheck for rebound.[1]
References
- [1]Decker BS, Goldfarb DS, Dargan PI, et al. Extracorporeal Treatment for Lithium Poisoning: Systematic Review and Recommendations from the EXTRIP Workgroup Clin J Am Soc Nephrol, 2015.PMID 25583292
- [2]Baird-Gunning J, Lea-Henry T, Hoegberg LCG, et al. Lithium Poisoning J Intensive Care Med, 2017.PMID 27516079
- [3]Gitlin M Lithium side effects and toxicity: prevalence and management strategies Int J Bipolar Disord, 2016.PMID 27900734
- [4]Waring WS Management of lithium toxicity Toxicol Rev, 2006.PMID 17288494
- [5]Waring WS, Laing WJ, Good AM, et al. Pattern of lithium exposure predicts poisoning severity: evaluation of referrals to a regional poisons unit QJM, 2007.PMID 17412747
- [6]Timmer RT, Sands JM Lithium intoxication J Am Soc Nephrol, 1999.PMID 10073618
- [7]Finley PR Drug Interactions with Lithium: An Update Clin Pharmacokinet, 2016.PMID 26936045
- [8]Finley PR, O'Brien JG, Coleman RW Lithium and angiotensin-converting enzyme inhibitors: evaluation of a potential interaction J Clin Psychopharmacol, 1996.PMID 8834421
- [9]Adityanjee, Munshi KR, Thampy A The syndrome of irreversible lithium-effectuated neurotoxicity Clin Neuropharmacol, 2005.PMID 15714160
- [10]Okusa MD, Crystal LJ Clinical manifestations and management of acute lithium intoxication Am J Med, 1994.PMID 7942943
- [11]Hansen HE, Amdisen A Lithium intoxication. (Report of 23 cases and review of 100 cases from the literature) Q J Med, 1978.PMID 356084
- [12]Nolen WA, Licht RW, Young AH, et al. What is the optimal serum level for lithium in the maintenance treatment of bipolar disorder? A systematic review and recommendations from the ISBD/IGSLI Task Force on treatment with lithium Bipolar Disord, 2019.PMID 31112628
- [13]Cipriani A, Hawton K, Stockton S, et al. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis BMJ, 2013.PMID 23814104
- [14]Offerman SR, Alsop JA, Lee J, et al. Hospitalized lithium overdose cases reported to the California Poison Control System Clin Toxicol (Phila), 2010.PMID 20515402
- [15]Eyer F, Pfab R, Felgenhauer N, et al. Lithium poisoning: pharmacokinetics and clearance during different therapeutic measures J Clin Psychopharmacol, 2006.PMID 16702900
- [16]McKnight RF, Adida M, Budge K, et al. Lithium toxicity profile: a systematic review and meta-analysis Lancet, 2012.PMID 22265699
- [17]Shine B, McKnight RF, Leaver L, et al. Long-term effects of lithium on renal, thyroid, and parathyroid function: a retrospective analysis of laboratory data Lancet, 2015.PMID 26003379
- [18]Thanacoody R, Caravati EM, Troutman B, et al. Position paper update: whole bowel irrigation for gastrointestinal decontamination of overdose patients Clin Toxicol (Phila), 2015.PMID 25511637
- [19]Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder Bipolar Disord, 2018.PMID 29536616
- [20]Malhi GS, Gessler D, Outhred T The use of lithium for the treatment of bipolar disorder: Recommendations from clinical practice guidelines J Affect Disord, 2017.PMID 28437764