Psych · Emergency psychiatry
Neuroleptic malignant syndrome
Also known as NMS · Neuroleptic malignant syndrome · Antipsychotic malignant syndrome · Malignant neuroleptic syndrome · Drug-induced hyperthermic rigidity syndrome
Exam-exhaustive fellowship topic on neuroleptic malignant syndrome — Gurrera international consensus diagnostic criteria with critical values, differentials (serotonin toxicity, malignant catatonia, heat stroke, malignant hyperthermia), CK and labs, stop dopamine antagonists, supportive/ICU care, bromocriptine/dantrolene/ECT debates, atypical SGA presentations, and delayed careful antipsychotic rechallenge. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Neuroleptic malignant syndrome (NMS) is rare, idiosyncratic, and still fatal when recognition is delayed. Fellowship examiners test three things above all: can you diagnose it with named criteria and thresholds, can you separate it from serotonin toxicity and malignant catatonia, and can you manage the medical emergency without pouring more antipsychotic into the fire.[3][6][9]
Overview and definition
NMS is a potentially life-threatening adverse reaction to dopamine D2 receptor antagonists — antipsychotics (first- and second-generation), and less often antiemetics such as metoclopramide or droperidol — or to abrupt withdrawal of dopaminergic agents in Parkinson disease. The clinical core is rigidity, hyperthermia, altered consciousness, and autonomic instability, with laboratory support from creatine kinase (CK) elevation and a work-up that excludes infection, toxic, metabolic, and structural alternatives.[1][3][4][6]
It is not a primary psychiatric diagnosis in DSM-5-TR or ICD-11; it is a medication-induced movement/systemic emergency that psychiatry owns jointly with acute medicine and intensive care.[6][9]
Classification and diagnostic criteria
Gurrera international expert consensus (IEC), 2011
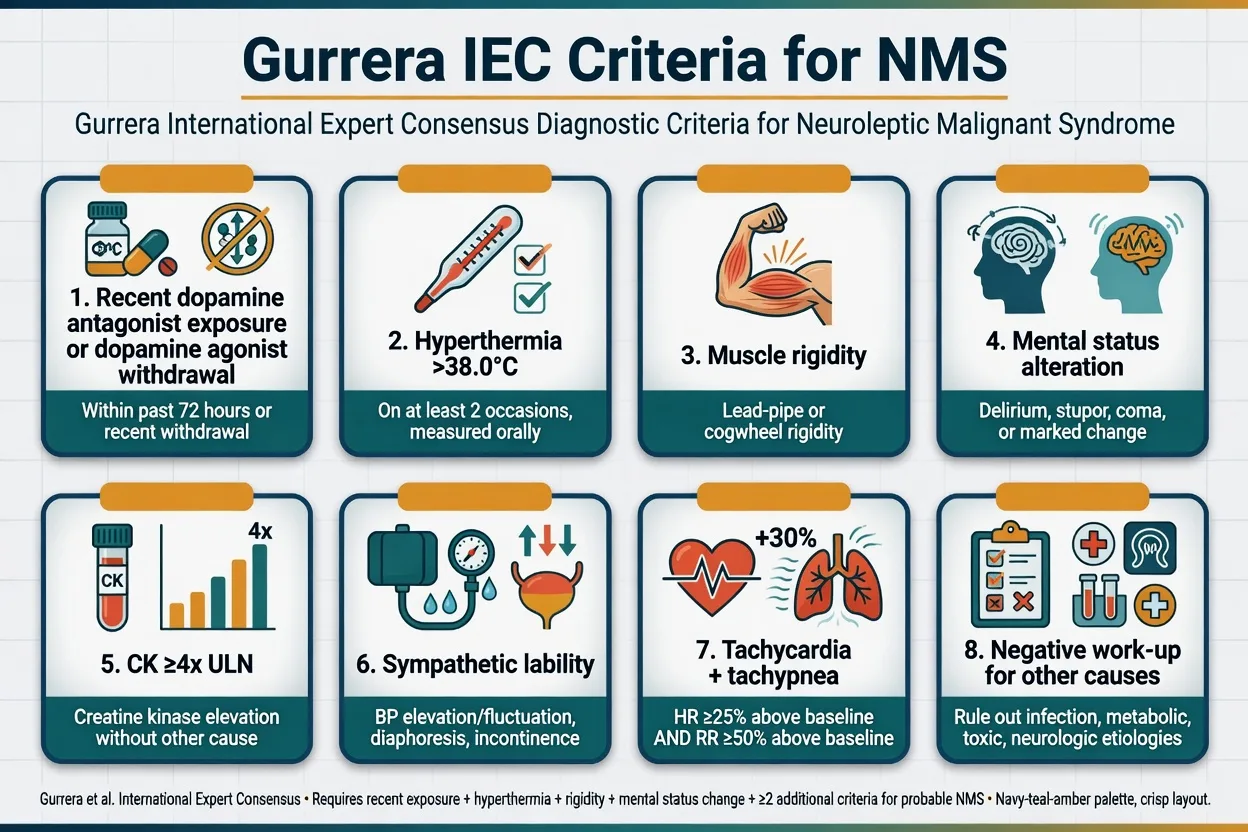
An international multispecialty Delphi panel reached consensus on diagnostic elements and critical values:[1]
| Element | Critical values / notes |
|---|---|
| Exposure | Recent dopamine antagonist exposure or dopamine agonist withdrawal |
| Hyperthermia | Temperature greater than 38.0 C (100.4 F) on at least 2 occasions |
| Rigidity | Muscle rigidity (classically lead-pipe) |
| Mental status | Reduced or fluctuating level of consciousness / delirium-stupor spectrum |
| CK | Elevation at least 4 times the upper limit of normal |
| Sympathetic lability | Examples include BP elevation ≥25% above baseline; BP fluctuation ≥20 mmHg diastolic or ≥25 mmHg systolic within 24 h; diaphoresis; urinary incontinence |
| Hypermetabolism | Heart rate ≥25% above baseline and respiratory rate ≥50% above baseline |
| Exclusion | Negative work-up for infectious, toxic, metabolic, and neurologic alternatives |
These criteria were designed to reduce theoretical bias and to support research consistency; they still require clinical judgment and exclusion of mimics.[1][2]
Validation and priority scoring (2017)
Gurrera and colleagues validated IEC criteria against DSM-IV-TR research standards in clinician consultation cases. Receiver-operating characteristics were best against modified DSM-IV-TR criteria (accepting less than "severe" rigidity). An IEC priority-point cutoff of 74 showed about 69.6% sensitivity and 90.7% specificity versus that modified reference in their sample — useful for structured thinking, not a bedside calculator that replaces judgment.[2]
Historical and DSM-framed criteria
Levenson's 1985 criteria (major: fever, rigidity, raised CK; minor: tachycardia, abnormal BP, tachypnoea, altered consciousness, diaphoresis, leukocytosis) still appear in older stems. DSM-IV-TR research criteria required severe muscle rigidity and elevated temperature after neuroleptic exposure plus two or more of diaphoresis, dysphagia, tremor, incontinence, altered consciousness, mutism, tachycardia, elevated or labile BP, leukocytosis, or laboratory evidence of muscle injury. Know the IEC thresholds for modern viva answers; know Levenson/DSM as historical distractors.[5][2][3]
Atypical NMS
Second-generation antipsychotics (SGAs) can cause NMS with less extreme rigidity or fever, and clozapine-, aripiprazole-, and amisulpride-associated cases more often look "atypical." Do not withhold the diagnosis until the full classic tetrad appears.[12][13][7]
Epidemiology and risk factors
Incidence fell from historical estimates near 0.2% with high-potency first-generation agents and less monitoring, but NMS has not disappeared in the SGA era.[8][12][13]
Risk factors examiners expect: high-potency D2 antagonists, rapid dose escalation, parenteral administration, dehydration, exhaustion or restraint, agitation, young male sex in some series, prior NMS, organic brain disease, iron deficiency, and concurrent lithium in selected reports. Depot antipsychotics can prolong the syndrome because of long drug residence time.[3][6][7][8]
Pathophysiology
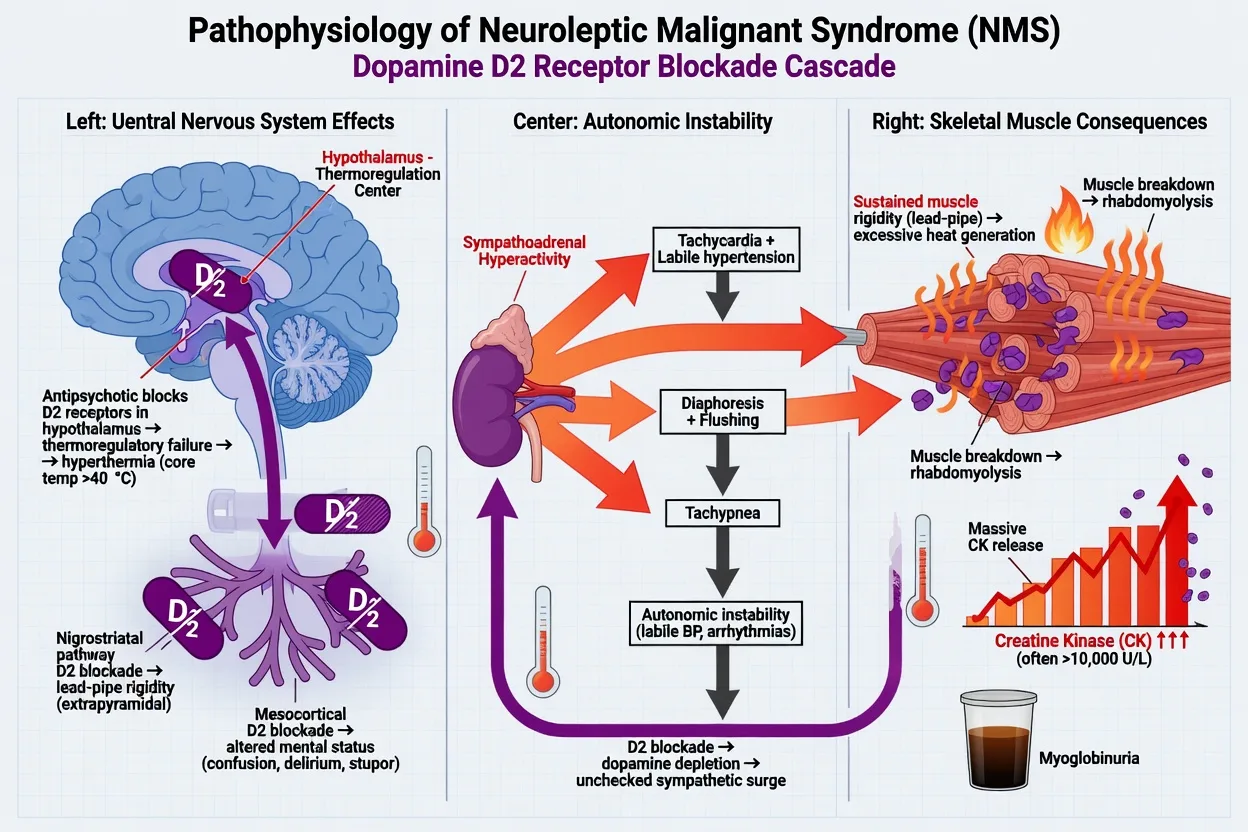
The leading model is acute central dopamine D2 hypofunction: nigrostriatal blockade produces lead-pipe rigidity; hypothalamic blockade impairs thermoregulation; mesocortical/arousal network effects alter mental status; and sympathoadrenal hyperactivity links autonomic lability (Gurrera hypothesis).[22][3][6]
Sustained rigidity drives heat production, rhabdomyolysis, CK release, myoglobinuria, and acute kidney injury. Whether NMS sits on a continuum with malignant catatonia remains debated; clinically you treat the emergency physiology and keep both labels active when exposure history is ambiguous.[20][21][4]
NMS is not the same disease as anaesthetic malignant hyperthermia (RYR1, volatile agents/suxamethonium), though both are hyperthermic rigidity syndromes and dantrolene appears in both conversations for different reasons.[4][6]
Clinical presentation
Classic tetrad
- Altered mental status — confusion, mutism, stupor, fluctuating consciousness.
- Muscle rigidity — lead-pipe; may be extreme.
- Hyperthermia — often high and poorly antipyretic-responsive.
- Autonomic instability — labile BP, tachycardia, tachypnoea, diaphoresis, incontinence.[3][6][1]
Tempo and progression
Onset is typically over hours to days after start or escalation of a dopamine antagonist, though cases occur on stable long-term therapy. Velamoor and colleagues described ordered progression in many cases: mental-status change and rigidity/autonomic signs often appear before peak fever — do not wait for extreme pyrexia to act.[16][3]
Complications at the bedside
Rhabdomyolysis, acute kidney injury, acute respiratory failure, aspiration, sepsis, metabolic acidosis, electrolyte storms, DIC, VTE, and seizures define severity. In large US inpatient data, rhabdomyolysis (~30%), AKI (~18%), and acute respiratory failure (~16%) were common; unadjusted mortality was 5.6%, with respiratory failure the strongest independent mortality predictor among analysed complications.[10]
Differential diagnosis — discriminators, not lists
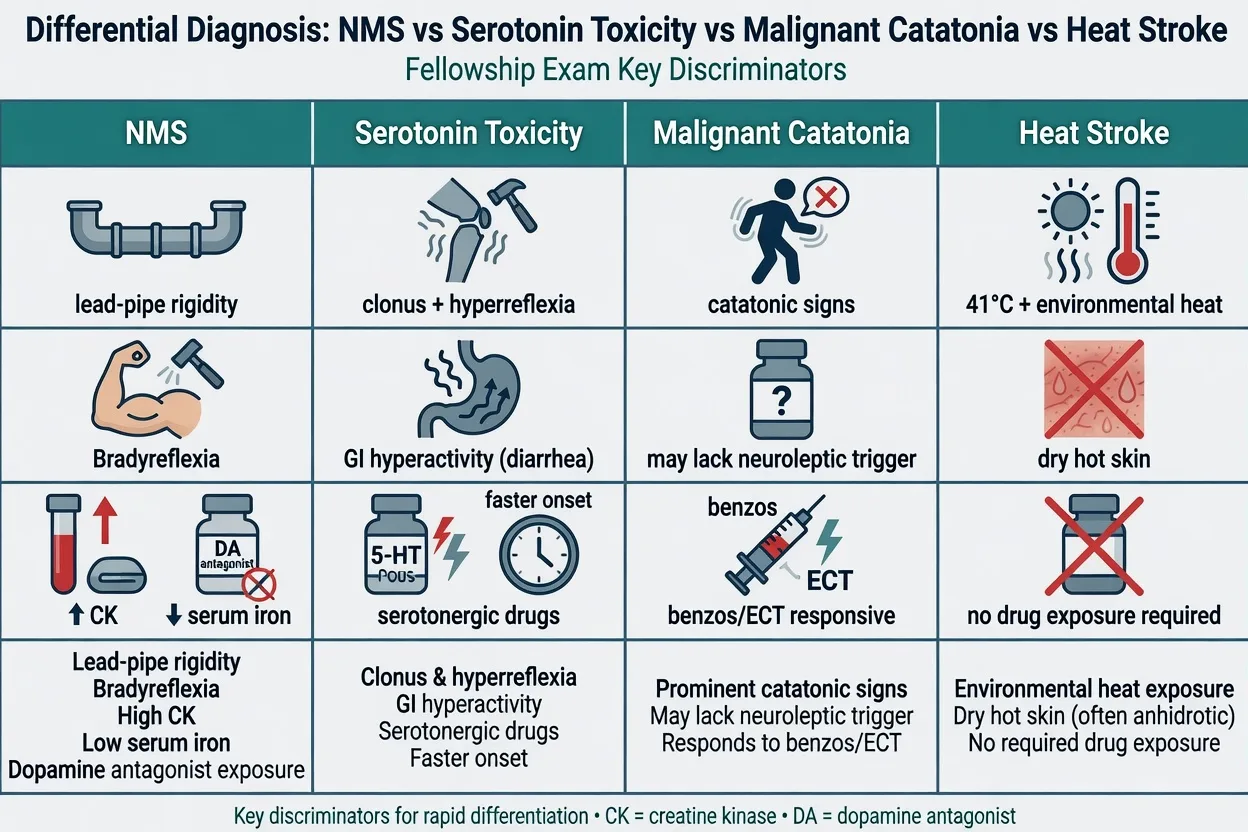
- Dopamine antagonist or agonist withdrawal
- Lead-pipe rigidity, bradyreflexia
- Slower onset (hours–days)
- CK often high; low serum iron supports NMS vs SS
- Stop antipsychotics; cool; support; ± bromocriptine/dantrolene/ECT
- Serotonergic agents (SSRI, MAOI, etc.)
- Clonus, hyperreflexia, myoclonus
- Faster onset (often hours)
- GI hyperactivity common
- Stop serotonergics; benzos; cyproheptadine considered
- Catatonic signs prominent
- May lack clear neuroleptic trigger
- Autonomic storm and fever possible
- Benzodiazepines first-line; ECT often definitive
- Overlaps NMS; BAP catatonia guidance applies
- Environmental heat/exertion
- Often hot dry skin (classic)
- No required drug exposure
- Cooling is definitive core therapy
- Still exclude drug toxicity
Serotonin toxicity is diagnosed with tools such as the Hunter Serotonin Toxicity Criteria (spontaneous clonus; inducible clonus plus agitation or diaphoresis; ocular clonus plus agitation or diaphoresis; tremor plus hyperreflexia; hypertonia plus temperature above 38 C plus ocular or inducible clonus) in the setting of a serotonergic agent.[18][19] When both drug classes are present, neuromuscular exam plus laboratory profile (higher CK and low serum iron favouring NMS) help, but stop all candidates if uncertain.[17]
Other can't-miss mimics: CNS infection/encephalitis, autoimmune encephalitis, status epilepticus, thyrotoxicosis, anticholinergic toxicity, sympathomimetic toxicity, withdrawal states, and anaesthetic malignant hyperthermia in the perioperative window.[6][9][3]
Clinical and bedside assessment
- ABCDE — airway risk from rigidity and aspiration; continuous temperature.
- Full medication timeline: antipsychotics (including depot and PRN), antiemetics, lithium, serotonergics, antiparkinsonian agents.
- Neurologic exam: tone (lead-pipe vs spasticity), reflexes (bradyreflexia vs clonus/hyperreflexia), myoclonus, catatonic signs (Bush-Francis elements).
- Autonomic charting against baseline HR/BP/RR (IEC critical deltas).
- Emergency MSE and capacity for specific treatment decisions; document least-restrictive legal basis under local law without inventing foreign statute numbers.
- Collateral and prior NMS history.[1][3][6][20]
Investigations
| Domain | Tests | Why |
|---|---|---|
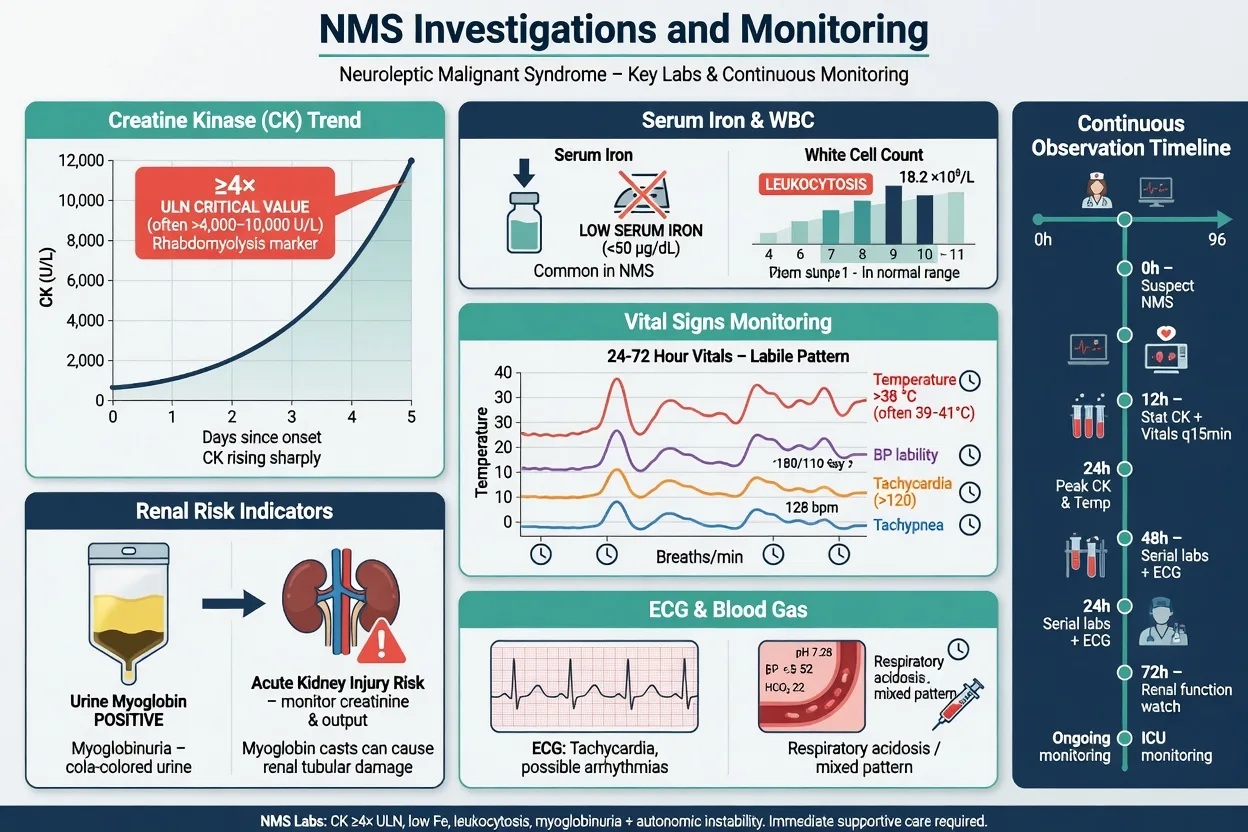
| Muscle injury | CK (serial), myoglobin, K+, phosphate | Rhabdomyolysis, arrhythmia risk |
| IEC support | CK ≥4× ULN; consider serum iron | Criteria and SS discrimination |
| Systemic | FBC (leukocytosis), U&E, LFTs, ABG/VBG, coagulation | Multi-organ involvement |
| Exclusion | Cultures, CXR, LP/imaging/EEG as indicated | Infection, encephalitis, seizure |
| Cardiac | ECG, troponin if indicated | Autonomic/ischaemic stress |
| Toxicology context | Directed screens | Do not delay care for UDS |
CK is supportive, not pathognomonic — restraint, intramuscular injections, and extreme agitation raise CK without NMS. Conversely, early or atypical NMS may have modest CK. Treat the syndrome, not a single number.[1][7]
Management — resuscitation
Immediate bundle: stop all dopamine antagonists and review antiemetics; escalate to ED/HDU/ICU capable of external cooling and airway support; ABCDE with high-flow oxygen as needed and airway protection; aggressive external cooling and cooled IV fluids per critical-care practice; IV volume resuscitation for rhabdomyolysis and autonomic losses with urine output and electrolyte monitoring; benzodiazepines for rigidity-associated agitation and catatonic features (for example lorazepam, titrated carefully with airway vigilance); thromboprophylaxis, aspiration precautions, pressure-care, and early complications search; continuous vital-sign and temperature monitoring with serial CK and renal panel.[3][6][8][9]
Management — definitive and stepwise
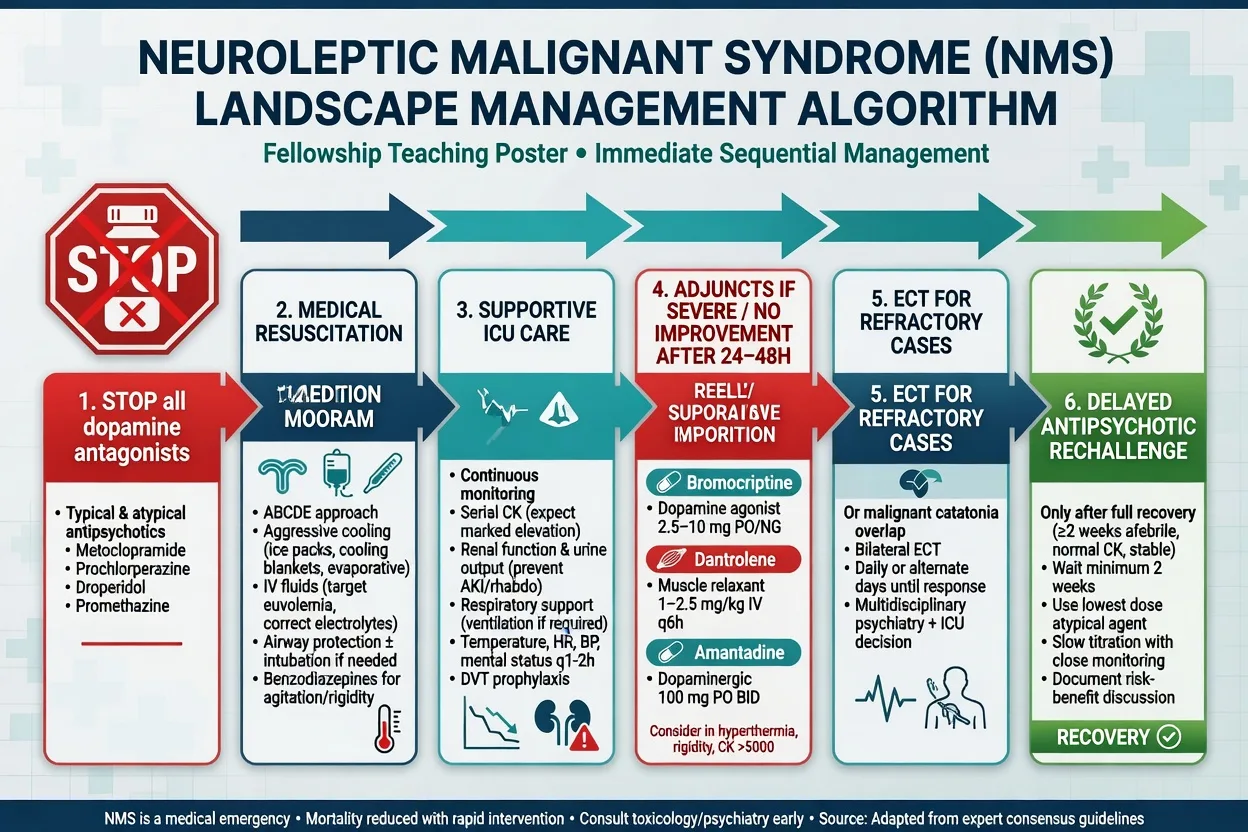
Supportive care is first-line
There are no large RCTs of NMS antidotes. Systematic case-series analysis (Kuhlwilm 2020, 405 cases) found no overall mortality or duration superiority of dantrolene, bromocriptine, or ECT versus pure supportive care, but in severe NMS a signal favoured specific therapy (pharmacotherapy or ECT) over supportive care alone, with ECT showing the lowest mortality in that severe subgroup analysis.[11] State this honestly in viva: support first; escalate specifics for severe or non-resolving disease.[8][11]
Bromocriptine (central dopamine agonist)
Used to reverse functional hypodopaminergia. Case-based regimens commonly start around bromocriptine 2.5 mg orally/NG two to three times daily, titrated (literature ranges often up to several times daily dosing under specialist supervision; follow local product information and critical-care advice). Continue until substantial recovery, then taper to avoid withdrawal worsening.[3][8][11]
Dantrolene (peripheral muscle relaxant)
Reduces excitation–contraction coupling and heat generation from rigidity. Case literature often cites IV dantrolene approximately 1–2.5 mg/kg, repeated as needed, with cumulative daily doses guided by response and local MH/NMS protocols (malignant-hyperthermia protocols historically reference higher cumulative ceilings — NMS use is off-label and specialist-supervised). Hepatotoxicity and muscle weakness are monitoring concerns.[3][8][11]
Amantadine
An alternative dopaminergic/NMDA-modulating option in some series when bromocriptine is unavailable or not tolerated; dosing is specialist and product-information dependent.[8][11]
ECT
Electroconvulsive therapy is indicated for refractory NMS and for malignant catatonia overlap, with multidisciplinary psychiatry–anaesthesia–ICU planning. BAP 2023 catatonia consensus explicitly addresses NMS/malignant catatonia interfaces and supports benzodiazepines and ECT in the catatonic spectrum.[20][21][11]
Restarting antipsychotics later
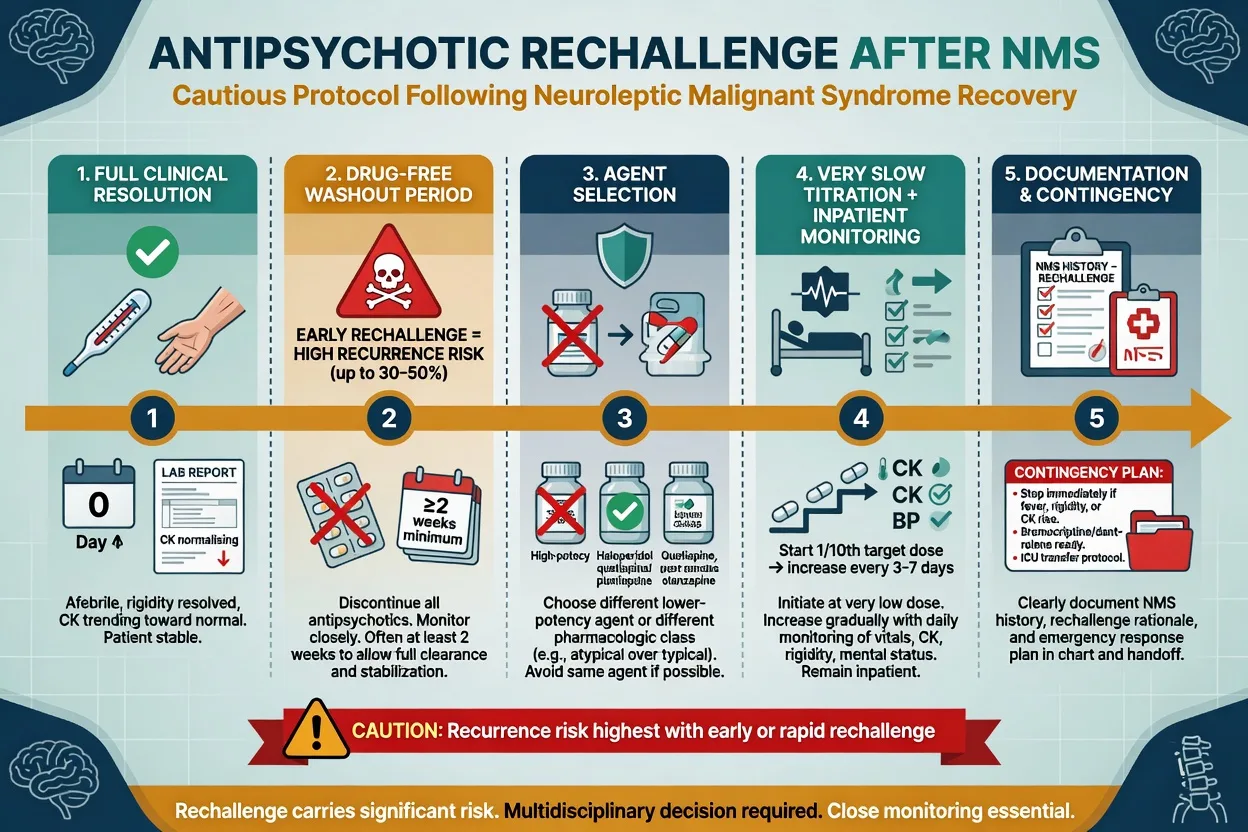
Most patients who need ongoing antipsychotic treatment can be carefully rechallenged, but recurrence is real.[15][8]
Rosebush and colleagues: of 15 patients with 20 rechallenges after NMS, 13/15 (87%) eventually tolerated neuroleptics again — successful rechallenge was highly related to time elapsed after resolution, more than to simply choosing a lower-potency drug.[15]
Practical fellowship algorithm:[15][8][14]
- Full clinical resolution (afebrile, rigidity resolved, CK trend normalising).
- Drug-free interval — often at least about 2 weeks after recovery is cited in reviews (longer after depot).
- Prefer a different agent, often lower D2 potency or different class; avoid the culprit if possible.
- Start low, go slow, preferably inpatient with temperature, tone, vitals, and CK surveillance.
- Document NMS as a serious adverse reaction and share contingency plans.
- Clozapine rechallenge after NMS is high-stakes and case-series based — specialist only (Lally systematic review).[14]
Specific subtypes and scenarios
| Scenario | Pearls |
|---|---|
| Classic FGA NMS | High-potency agents, parenteral escalation, textbook tetrad |
| SGA / atypical NMS | May lack extreme rigidity or fever; still stop drug |
| Clozapine NMS | Atypical features more often; rechallenge specialist |
| Antiemetic NMS | Metoclopramide/droperidol — stop D2 blockers in medical wards too |
| Parkinson withdrawal | Dopamine agonist cessation can trigger NMS-like syndrome — restore dopaminergics carefully |
| Depot-associated | Expect prolonged course; plan long washout |
| ICU multi-organ NMS | Respiratory failure and AKI drive mortality |
| Malignant catatonia overlap | Benzodiazepines + early ECT pathway |
Complications and pitfalls
- Treating evolving NMS as primary psychosis with more antipsychotic.
- Missing serotonin toxicity (wrong pathway).
- Attributing everything to "infection" while continuing the neuroleptic.
- Premature rechallenge.
- Ignoring aspiration and VTE risk during prolonged rigidity.
- Waiting for CK in the tens of thousands before acting.
- Confusing akathisia or simple EPS with NMS (no fever/autonomic storm).[3][10][17][8]
Prognosis and disposition
With early recognition, most patients recover over days to about 1–2 weeks (longer with depot). Contemporary mortality near 5–6% is better than historical rates but still substantial. Independent mortality associations include older age, acute respiratory failure, AKI, sepsis, and comorbid heart failure.[10][8]
Disposition: medical HDU/ICU until thermoregulation, airway safety, CK trajectory, and consciousness improve; psychiatry leads later rechallenge and mental-state care. Never discharge without clear adverse-drug documentation and follow-up ownership.[6][8]
Special populations
- Older adults: higher medical comorbidity and mortality risk; use lowest effective antipsychotic doses long-term.
- Children/adolescents: rare; same stop-and-support principles.
- Pregnancy: prioritise supportive care; ECT may be considered when indicated with obstetric anaesthesia planning.
- Intellectual disability / autism: catatonia overlap is common — examine carefully.
- Parkinson disease / DLB: extreme vulnerability to D2 blockade; prefer avoiding high-potency antipsychotics.
- Depot patients: prolonged syndrome and longer rechallenge delay.[6][7][20][3]
Evidence, guidelines, and regional practice
In Australia and New Zealand, NMS is managed as a medical emergency with local ICU/toxicology pathways. Psychiatry owns drug cessation, differential with catatonia/serotonin toxicity, and later rechallenge. There is no separate RANZCP "NMS protocol" that replaces critical-care standards — apply IEC diagnostic thinking, stop dopamine antagonists, and escalate early.[1][3][8]
Landmark teaching papers to name: Gurrera IEC 2011/2017, Strawn/Keck/Caroff 2007, Caroff/Mann reviews, Kuhlwilm 2020 therapy analysis, Rosebush rechallenge 1989, Hunter criteria and Boyer/Shannon for serotonin toxicity, BAP catatonia 2023.[1][2][3][11][15][18][19][20]
Exam pearls
NMS-STOP
- Clonus/hyperreflexia → think serotonin toxicity; lead-pipe/bradyreflexia → think NMS.[17][18]
- IEC: fever >38.0 C on ≥2 occasions; CK ≥4× ULN; HR ≥25% and RR ≥50% above baseline.[1]
- Priority score ~74 is the validated IEC research cutoff — know it exists.[2]
- Mortality drivers: respiratory failure, AKI, sepsis, age.[10]
- Rechallenge success tracks time since recovery more than magic drug choice.[15]
- Clozapine NMS can be atypical — still stop and support.[12][14]
- ECT is not last-ditch folklore when malignant catatonia/NMS refuses to turn.[20][11]
Self-test: 30-second stem
A 28-year-old man becomes mute and rigid with temperature 39.1 C, CK about twenty-fold above the upper limit of normal, BP swinging 90/50 to 170/100, and HR 130, three days after IM haloperidol escalation. He is on no serotonergic drugs. What is your first action and top differential split? Model: Stop all antipsychotics now; ABCDE/cooling/IV fluids; exclude infection; NMS far more likely than serotonin toxicity (rigidity without clonus/hyperreflexia, high CK, DA antagonist). Escalate HDU/ICU; consider bromocriptine/dantrolene if severe; ECT if refractory or catatonic malignant picture.[1][3][17]
References
- [1]Gurrera RJ, Caroff SN, Cohen A, et al. An international consensus study of neuroleptic malignant syndrome diagnostic criteria using the Delphi method J Clin Psychiatry, 2011.PMID 21733489
- [2]Gurrera RJ, Mortillaro G, Velamoor V, et al. A Validation Study of the International Consensus Diagnostic Criteria for Neuroleptic Malignant Syndrome J Clin Psychopharmacol, 2017.PMID 28027111
- [3]Strawn JR, Keck PE Jr, Caroff SN Neuroleptic malignant syndrome Am J Psychiatry, 2007.PMID 17541044
- [4]Caroff SN, Mann SC Neuroleptic malignant syndrome Med Clin North Am, 1993.PMID 8093494
- [5]Levenson JL Neuroleptic malignant syndrome Am J Psychiatry, 1985.PMID 2863986
- [6]Berman BD Neuroleptic malignant syndrome: a review for neurohospitalists Neurohospitalist, 2011.PMID 23983836
- [7]Tse L, Barr AM, Scarapicchia V, et al. Neuroleptic Malignant Syndrome: A Review from a Clinically Oriented Perspective Curr Neuropharmacol, 2015.PMID 26411967
- [8]Pileggi DJ, Cook AM Neuroleptic Malignant Syndrome Ann Pharmacother, 2016.PMID 27423483
- [9]Wijdicks EFM, Ropper AH Neuroleptic Malignant Syndrome N Engl J Med, 2024.PMID 39321364
- [10]Modi S, Dharaiya D, Schultz L, et al. Neuroleptic Malignant Syndrome: Complications, Outcomes, and Mortality Neurocrit Care, 2016.PMID 26223336
- [11]Kuhlwilm L, Schönfeldt-Lecuona C, Gahr M, et al. The neuroleptic malignant syndrome-a systematic case series analysis focusing on therapy regimes and outcome Acta Psychiatr Scand, 2020.PMID 32659853
- [12]Belvederi Murri M, Guaglianone A, Bugliani M, et al. Second-generation antipsychotics and neuroleptic malignant syndrome: systematic review and case report analysis Drugs R D, 2015.PMID 25578944
- [13]Ananth J, Parameswaran S, Gunatilake S, et al. Neuroleptic malignant syndrome and atypical antipsychotic drugs J Clin Psychiatry, 2004.PMID 15119907
- [14]Lally J, McCaffrey C, O'Murchu C, et al. Clozapine Rechallenge Following Neuroleptic Malignant Syndrome: A Systematic Review J Clin Psychopharmacol, 2019.PMID 31205196
- [15]Rosebush PI, Stewart TD, Gelenberg AJ Twenty neuroleptic rechallenges after neuroleptic malignant syndrome in 15 patients J Clin Psychiatry, 1989.PMID 2569457
- [16]Velamoor VR, Norman RM, Caroff SN, et al. Progression of symptoms in neuroleptic malignant syndrome J Nerv Ment Dis, 1994.PMID 7906709
- [17]Perry PJ, Wilborn CA Serotonin syndrome vs neuroleptic malignant syndrome: a contrast of causes, diagnoses, and management Ann Clin Psychiatry, 2012.PMID 22563571
- [18]Dunkley EJ, Isbister GK, Sibbritt D, et al. The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity QJM, 2003.PMID 12925718
- [19]Boyer EW, Shannon M The serotonin syndrome N Engl J Med, 2005.PMID 15784664
- [20]Rogers JP, Oldham MA, Fricchione G, et al. Evidence-based consensus guidelines for the management of catatonia: Recommendations from the British Association for Psychopharmacology J Psychopharmacol, 2023.PMID 37039129
- [21]Connell J, Oldham M, Pandharipande P, et al. Malignant Catatonia: A Review for the Intensivist J Intensive Care Med, 2023.PMID 35861966
- [22]Gurrera RJ Sympathoadrenal hyperactivity and the etiology of neuroleptic malignant syndrome Am J Psychiatry, 1999.PMID 9989551