Psych · Emergency psychiatry
Overdose and toxicology for psychiatrists
Also known as Deliberate self-poisoning · Psychotropic overdose · Toxicology for psychiatry · Self-poisoning assessment · Toxidrome approach psychiatry
Exam-exhaustive fellowship hub on overdose and clinical toxicology for psychiatrists — toxidrome approach, relative toxicity of psychotropics (TCA, venlafaxine, SSRIs, antipsychotics, lithium, benzodiazepines), always-screen paracetamol, antidotes (bicarbonate, NAC, naloxone, cyproheptadine), decontamination rules, EXTRIP lithium interface, flumazenil cautions, medical clearance and post-OD suicide risk disposition. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overdose and clinical toxicology sit at the centre of emergency psychiatry. Fellowship examiners expect more than “supportive care”: they want a toxidrome language, a relative toxicity ladder for psychotropics, named antidotes with indications and cautions, and a disciplined sequence of medical stabilisation before risk assessment and disposition.[3][16][18]

Overview and definition
Deliberate self-poisoning is intentional ingestion (or other exposure) of a substance in excess of therapeutic intent as a method of self-harm or suicide attempt. Accidental overdose, therapeutic misadventure (wrong dose, interaction, accumulation), and body packing/stuffing are distinct exposure contexts with different forensic and clinical implications.[16][18]
This is not a DSM-5-TR or ICD-11 primary psychiatric diagnosis. It is a medical emergency that psychiatry must own because psychiatrists prescribe high-risk agents, assess aftercare, and decide on means access — while ED and ICU deliver resuscitation.[16][17]
Classification — toxidromes and exposure patterns
Toxidrome map (exam staple)
| Toxidrome | Key discriminators | Psychiatry-relevant agents |
|---|---|---|
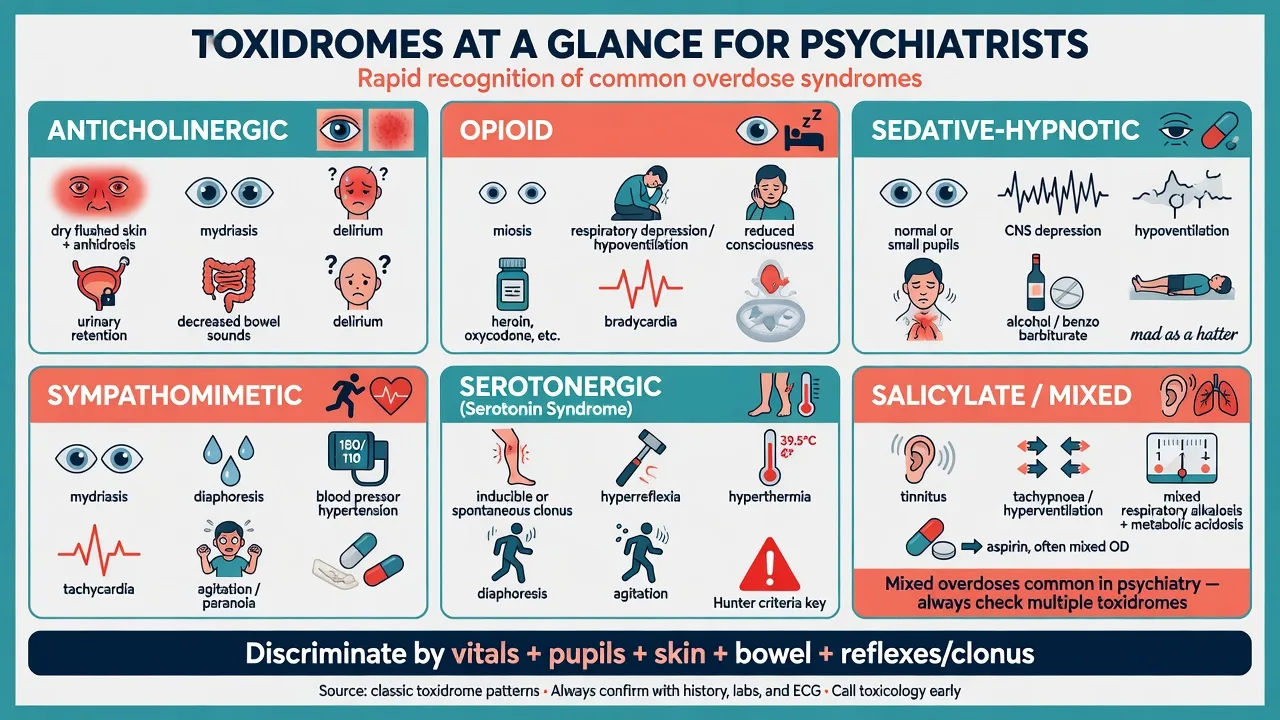
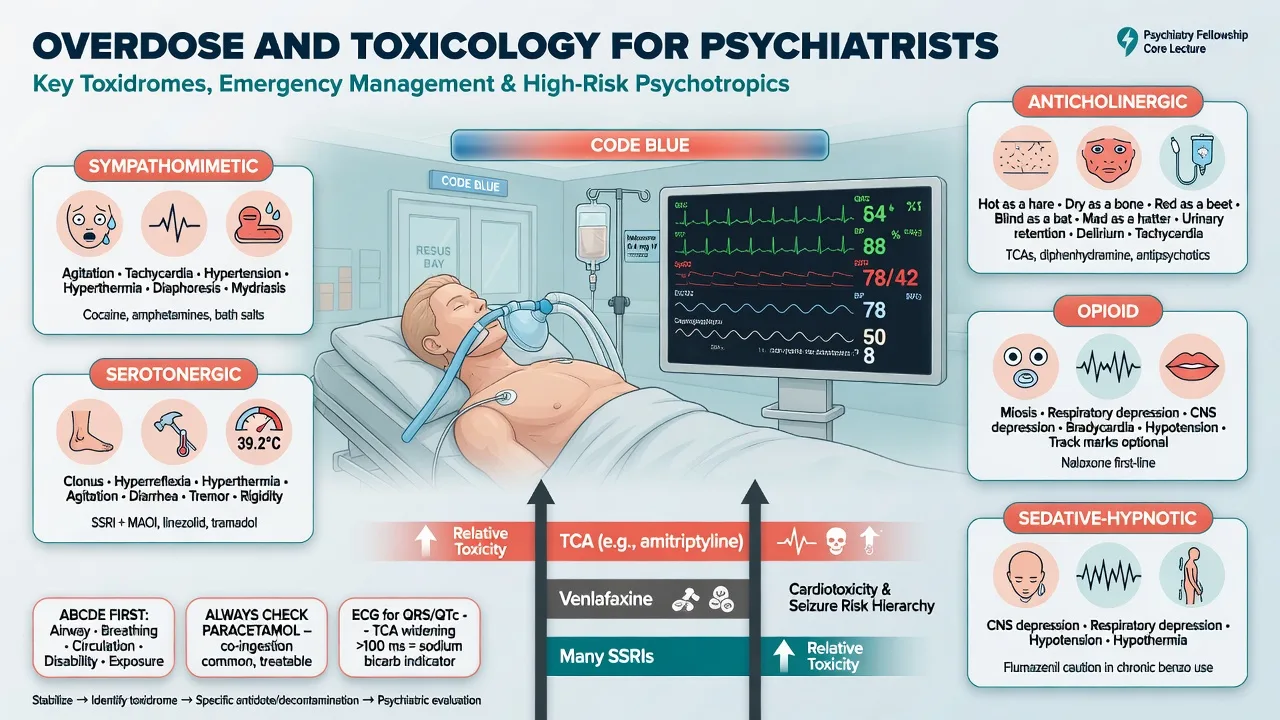
| Anticholinergic | Dry skin, mydriasis, urinary retention, delirium, reduced bowel sounds | TCAs, some antipsychotics (e.g. quetiapine), antihistamines |
| Opioid | Miosis, respiratory depression, reduced consciousness | Heroin, methadone, oxycodone, fentanyl; tramadol nuances |
| Sedative-hypnotic | CNS depression, hypoventilation, often small/normal pupils | Benzodiazepines, Z-drugs, alcohol, barbiturates |
| Sympathomimetic | Agitation, diaphoresis, mydriasis, hypertension, tachycardia | Amphetamines, cocaine, some ADHD stimulants in overdose |
| Serotonergic | Clonus/hyperreflexia, diaphoresis, hyperthermia, agitation | SSRI/SNRI stacks, MAOI combinations, MDMA contexts |
| Salicylate / mixed | Tinnitus, tachypnoea, acid-base chaos | OTC co-ingestants; do not force a single label in polypharmacy |
Exposure patterns
- Acute single ingestion — classic intentional OD stem.
- Staggered / repeated — especially paracetamol; nomogram interpretation changes; risk of delayed presentation with established injury.[11]
- Chronic accumulation — lithium with reduced clearance (classic old-age and interaction story).[8]
- Acute-on-chronic — extra load on tissue stores (lithium, sometimes anticonvulsant mood stabilisers).[7][8]
Epidemiology and risk
Self-poisoning remains a leading method of hospital-presenting self-harm. Psychotropics and paracetamol dominate psychiatric-context ingestions; alcohol co-ingestion is common and worsens airway risk and assessment reliability.[11][16][17]
Risk anchors for the viva
High-yield risk amplifiers: prior self-harm, severe depression or psychosis, substance use disorders, stockpiled tablets, social isolation, access to parental or partner medication, and recent discharge without means counselling.[16][17]
Pathophysiology — mechanisms that drive management
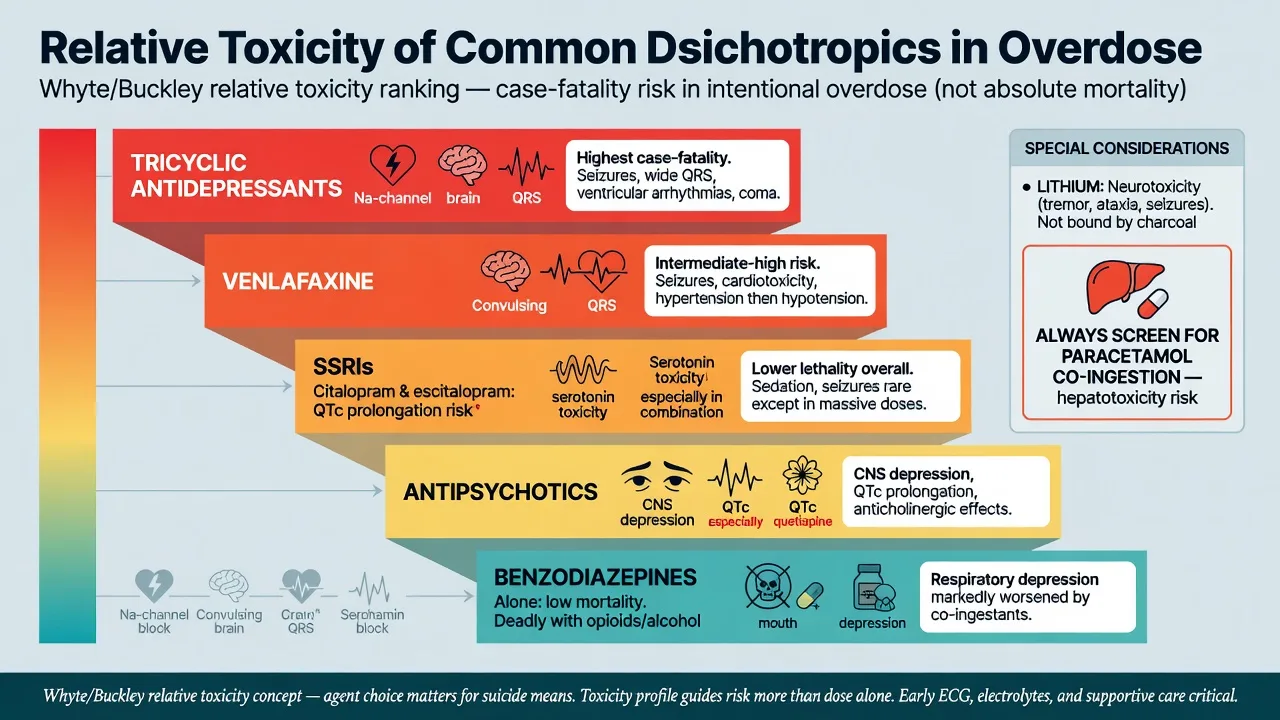
Tricyclic antidepressants. Fast sodium-channel blockade slows phase-0 depolarisation → QRS widening, ventricular dysrhythmias, seizures; muscarinic blockade drives anticholinergic features; alpha-1 blockade contributes to hypotension. Alkalinisation with sodium bicarbonate is the cardiotoxicity cornerstone.[5][6]
SSRIs. Generally lower case fatality in pure overdose than TCAs, but seizures and QTc issues occur (notably citalopram/escitalopram), and combinations drive serotonin toxicity.[4][9][10]
Venlafaxine. Intermediate-to-high relative toxicity versus many SSRIs in Hunter-area analyses — seizures and cardiotoxicity feature in exam stems; do not treat as "just an SSRI."[3]
Lithium. Freely filtered then reabsorbed with sodium; volume depletion and interacting drugs raise levels; brain concentration lags serum — clinical neurotoxicity can outlast the peak number.[7][8]
Opioids. Mu-receptor mediated respiratory depression; naloxone is a competitive antagonist — titration and observation matter because antagonist duration may be shorter than the opioid.[13][14]
Paracetamol. Excess NAPQI after glutathione depletion causes centrilobular hepatic necrosis; N-acetylcysteine replenishes glutathione and remains highly effective when given early.[11][12]
Benzodiazepines. GABA-A facilitation → CNS and respiratory depression, especially with alcohol or opioids. Flumazenil antagonises the receptor but can precipitate seizures and acute withdrawal — restricted role.[15]
Serotonin toxicity. Excess 5-HT activity with neuromuscular hyperreactivity (clonus/hyperreflexia); diagnosed clinically (Hunter criteria preferred); managed by cessation, benzodiazepines, cooling, and cyproheptadine when indicated.[9][10]
Clinical presentation
Tempo is diagnostic. TCA overdose can collapse within hours (coma, seizures, wide-complex tachycardia). Paracetamol may look well early and declare hepatotoxicity at 12–72 hours. Lithium chronic toxicity presents with coarse tremor, ataxia, dysarthria and confusion after a clearance insult. Serotonin toxicity usually evolves over hours after a serotonergic stack or overdose context.[5][8][10][11]
Mixed pictures dominate real life. Alcohol plus benzodiazepine plus antidepressant is more common than a pure textbook toxidrome — document what you see (pupils, reflexes, skin, bowel, ECG) rather than forcing a single label.[16][18]
Differential diagnosis
| Mimic | Clues favouring toxin | Clues favouring alternative |
|---|---|---|
| Primary psychosis/agitation | Packet evidence, vital-sign toxidrome, ECG changes | Clear sensorium without autonomic package |
| Hypoglycaemia / hypoxia / stroke | Correctable labs/gas; toxin history still sought | Focal neurology, hypoglycaemia on stick |
| NMS | Dopamine antagonist, slower onset, bradyreflexia | Serotonergic drug + clonus → serotonin toxicity |
| Anticholinergic delirium | Dry skin, retention, mydriasis + culprit drug | Wet skin + clonus → serotonergic/sympathomimetic |
| Head injury after collapse | Trauma signs, imaging when indicated | Pure toxidrome without trauma |
Assessment
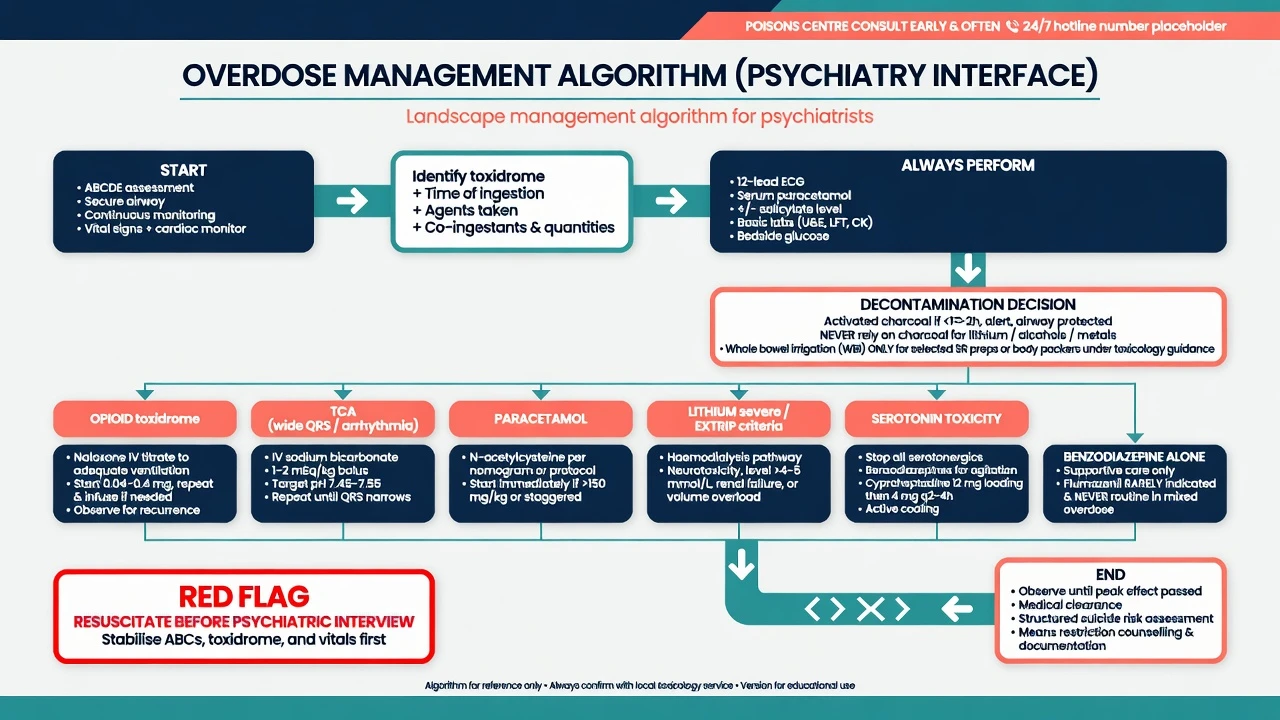
- ABCDE first — airway protection if GCS falling or aspiration risk; oxygen; circulation; disability (glucose, pupils, tone, clonus); exposure and temperature.[16][18]
- History that scores marks: agents, estimated doses, times, immediate vs sustained-release, empty blister packs, intent and planning, co-ingestants (alcohol, OTC, illicit), last meal, vomiting, pregnancy possibility, chronic medicines, prior OD, access to stockpiles.[16]
- Toxidrome exam + ECG early.
- Capacity and risk after medical stabilisation — document emergency treatment if capacity is lost.
- Call poisons information early when agent, dose, or timing is uncertain or severe features appear.[16][18]
Investigations
- ECG in any serious psychotropic overdose — QRS duration, QTc, terminal R wave in aVR (TCA teaching pearl).[5][6]
- Paracetamol level timed from ingestion in all deliberate self-poisonings (and salicylate when clinically indicated).[11]
- U and E, creatinine, glucose, LFTs, INR/coagulation, blood gas/lactate, CK as indicated.
- Lithium level if lithium is possible; serial levels if toxic.
- Valproate level and ammonia when valproate overdose is on the table.
- Pregnancy test when relevant.
- Imaging for trauma, unexplained focal signs, or packing suspicion.
Acute management
Decontamination (position-paper discipline)
Single-dose activated charcoal may benefit selected recent ingestions (generally most useful within about 1 hour) when the airway is protected and the toxin is adsorbed by charcoal. It is not useful for lithium, alcohols, or metals, and it is dangerous if the patient vomits or aspirates with an unprotected airway.[1]
Whole bowel irrigation is reserved for selected large sustained-release ingestions or body-packer scenarios under toxicology guidance — not routine for every psychiatric overdose.[2]
Supportive care is first-line
IV access, monitoring, fluids for hypotension, temperature control, benzodiazepines for toxin-related seizures and severe agitation, and early ICU involvement for airway compromise, refractory shock, severe cardiotoxicity, or severe hyperthermia.[16][18]
Agent-specific definitive management
Tricyclic antidepressants
- Continuous cardiac monitoring; serial ECGs.
- IV sodium bicarbonate for wide QRS, ventricular arrhythmias, or severe acidaemia — alkalinisation and sodium loading are the mechanistic therapy; optimise per local critical-care/toxicology protocol and reassess QRS response.[5][6]
- Benzodiazepines for seizures; avoid class Ia/Ic antiarrhythmics that worsen Na-channel block.
- Lipid emulsion considered for refractory life-threatening cardiotoxicity under specialist guidance.[5]
Paracetamol
- Risk-stratify with timed plasma paracetamol against the local treatment nomogram (regional thresholds differ — UK, ANZ, North America variants exist; follow local protocol).
- Start N-acetylcysteine when indicated without waiting for late enzyme rises; early NAC is highly effective; established liver failure needs specialist/transplant pathway thinking (King’s College criteria heritage in severe ALF discussions).[11][12]
Opioids
- Support ventilation first.
- Naloxone titrated to restore adequate ventilation — not necessarily full arousal (precipitated withdrawal and agitation if over-bolused).
- Observe for re-narcotisation, especially with long-acting opioids (methadone) or high-potency synthetics; community naloxone programmes reduce deaths in public-health data.[13][14]
Lithium
- Stop lithium and interacting drugs; correct volume depletion with isotonic saline when depleted; serial levels and neurology.
- Charcoal does not bind lithium.
- Escalate to extracorporeal treatment when EXTRIP criteria are met (e.g. severe poisoning; impaired kidney function with high level; decreased consciousness, seizures, or life-threatening dysrhythmias irrespective of concentration — cite the workgroup recommendations in viva).[7][8]
Benzodiazepines
- Supportive care and airway management are primary.
- Flumazenil is not routine in unknown mixed OD, chronic benzodiazepine dependence, or possible TCA co-ingestion — seizures and acute withdrawal are the traps. NPIS-linked surveillance underscores selective use only.[15]
Serotonin toxicity (overdose / combination interface)
- Stop serotonergics; benzodiazepines; active cooling; cyproheptadine (typical load 12 mg oral/NG, then 2 mg every 2 hours if ongoing; maintenance often 8 mg every 6 hours — Boyer and Shannon teaching regimen).
- Diagnose with Hunter criteria when a serotonergic agent is present.
- Do not treat as NMS with bromocriptine.[9][10]
Antipsychotics and valproate (high-yield notes)
- Antipsychotic overdose: CNS depression, QTc prolongation, anticholinergic features (quetiapine classic); supportive care, ECG monitoring, benzodiazepines for seizures.[16][18]
- Valproate overdose: CNS depression, hyperammonaemia; specialist use of L-carnitine in severe hyperammonaemic encephalopathy — involve toxicology early.[16][18]
Subtypes and exam scenarios
- Adolescent stockpile of parental amitriptyline or lithium — means access counselling for the household.
- Staggered paracetamol in severe depression — early enzymes may mislead; protocolised NAC decisions.[11]
- Venlafaxine large overdose with seizures — relative toxicity teaching case.[3]
- MAOI + tramadol after pain treatment → serotonin toxicity (cross-link).[9][10]
- Custody body stuffing of illicit drugs — delayed severe toxicity.[16]
- Older adult chronic lithium after thiazide start — not always "an overdose number."[7][8]
Complications and pitfalls
- Missing paracetamol.
- Charcoal aspiration.
- Flumazenil-triggered seizures.
- Discharging lithium toxicity on a falling number while still encephalopathic.
- Under-calling venlafaxine/TCA risk because “antidepressant OD is usually fine.”
- Psychiatric interview before ECG and resuscitation are complete.
- Incomplete observation after naloxone response.[3][7][11][15]
Prognosis and disposition
Most pure modern SSRI overdoses do well with observation and supportive care; TCAs, large multi-drug ODs, delayed paracetamol, and severe lithium neurotoxicity still kill or leave residual injury.[3][4][11][17]
Disposition framework: observe until past expected peak effect for the agent and formulation; ICU for airway, refractory cardiotoxicity, need for ECTR, or severe hyperthermia; after medical clearance, perform structured suicide risk assessment, address drivers (depression, psychosis, substance use, interpersonal crisis), implement means restriction (dispose excess stock, supervised dispensing, blister packs), and choose least-restrictive safe aftercare (home with supports vs psychiatric admission under relevant mental health law).[16]
Special populations
- Children/adolescents: exploratory ingestions can reach toxic milligram-per-kilogram thresholds quickly; intentional overdose needs family systems and safeguarding.[16]
- Older adults: reduced reserve, chronic lithium accumulation, polypharmacy delirium.[7][8]
- Pregnancy: treat the mother aggressively (including NAC for paracetamol); avoid delays for fetal concerns that worsen maternal outcome.[11][12]
- Intellectual disability: collateral history essential; capacity and safeguarding.[16]
- Cultural safety: interpreters, family, Indigenous liaison where relevant; postvention after serious attempts.[16]
Evidence and guidelines (regional deltas)
[3] [11] [14] [15]Landmark anchors for exams: AACT charcoal and WBI position papers; Whyte/Buckley/Isbister relative toxicity series; Hunter serotonin criteria; Boyer and Shannon SS review; EXTRIP lithium; TCA alkalinisation literature; Smilkstein/Bateman paracetamol–NAC lineage; naloxone EMS/community evidence.[1][2][3][5][7][9][11][13]
Exam pearls
TOX-PSYCH checklist
- TCA: QRS widening and R in aVR → think bicarbonate.
- Lithium: no charcoal; think EXTRIP.
- Flumazenil: not a mixed-overdose diagnostic test.
- Venlafaxine is not a "safe SSRI profile" in overdose rankings.
- Medical first, psychiatry second — but never discharge without risk assessment and means plan.[3][5][7][15]
Related topics
Cross-link deep dives: lithium toxicity, serotonin syndrome, neuroleptic malignant syndrome, suicide risk assessment, self-harm and crisis intervention, acute agitation and rapid tranquillisation, and individual psychopharmacology monographs for therapeutic (non-overdose) detail.[16]
References
- [1]Chyka PA, Seger D, Krenzelok EP, Vale JA Position paper: Single-dose activated charcoal. Clin Toxicol (Phila), 2005.PMID 15822758
- [2]Thanacoody R, Caravati EM, Downs J, et al. Position paper update: Whole bowel irrigation for gastrointestinal decontamination of overdose patients. Clin Toxicol (Phila), 2015.PMID 25511637
- [3]Whyte IM, Dawson AH, Buckley NA Relative toxicity of venlafaxine and selective serotonin reuptake inhibitors in overdose compared to tricyclic antidepressants. QJM, 2003.PMID 12702786
- [4]Isbister GK, Bowe SJ, Dawson A, et al. Relative toxicity of selective serotonin reuptake inhibitors (SSRIs) in overdose. J Toxicol Clin Toxicol, 2004.PMID 15362595
- [5]Liebelt EL, Francis PD, Woolf AD Targeted management strategies for cardiovascular toxicity from tricyclic antidepressant overdose: the pivotal role for alkalinization and sodium loading. Pediatr Emerg Care, 1998.PMID 9733258
- [6]Pai K, Roberts DM, et al. Optimising alkalinisation and its effect on QRS narrowing in tricyclic antidepressant poisoning. Br J Clin Pharmacol, 2022.PMID 34312917
- [7]Decker BS, Goldfarb DS, Dargan PI, et al. Extracorporeal Treatment for Lithium Poisoning: Systematic Review and Recommendations from the EXTRIP Workgroup. Clin J Am Soc Nephrol, 2015.PMID 25583292
- [8]Baird-Gunning J, Lea-Henry T, Hoegberg LCG, et al. Lithium Poisoning. J Intensive Care Med, 2017.PMID 27516079
- [9]Dunkley EJ, Isbister GK, Sibbritt D, et al. The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity. QJM, 2003.PMID 12925718
- [10]Boyer EW, Shannon M The serotonin syndrome. N Engl J Med, 2005.PMID 15784664
- [11]Bateman DN, Dear JW, Thanacoody HK, Thomas SHL Fifty years of paracetamol (acetaminophen) poisoning: the development of risk assessment and treatment 1973-2023 with particular focus on contributions published from Edinburgh and Denver. Clin Toxicol (Phila), 2023.PMID 38197864
- [12]Smilkstein MJ, Knapp GL, Kulig KW, Rumack BH Efficacy of oral N-acetylcysteine in the treatment of acetaminophen overdose. Analysis of the national multicenter study (1976 to 1985). N Engl J Med, 1988.PMID 3059186
- [13]Williams K, Lang ES, Panchal AR, et al. Evidence-Based Guidelines for EMS Administration of Naloxone. Prehosp Emerg Care, 2019.PMID 30924736
- [14]Walley AY, Xuan Z, Hackman HH, et al. Opioid overdose rates and implementation of overdose education and nasal naloxone distribution in Massachusetts: interrupted time series analysis. BMJ, 2013.PMID 23372174
- [15]Veiraiah A, Phua CW, Leman P, Greene SL Flumazenil use in benzodiazepine overdose in the UK: a retrospective survey of NPIS data. Emerg Med J, 2012.PMID 21785147
- [16]Parris MA, Ragan FA, Lin A Found Down: Approach to the Patient with an Unknown Poisoning. Emerg Med Clin North Am, 2022.PMID 35461619
- [17]Brett J, Wylie CE, Raubenheimer J, Isbister GK, et al. The relative lethal toxicity of pharmaceutical and illicit substances: A 16-year study of the Greater Newcastle Hunter Area, Australia. Br J Clin Pharmacol, 2019.PMID 31173392
- [18]Hüser C, Persaud P, Jain N, et al. Critical care management of the patient with pharmaceutical poisoning. Intensive Care Med, 2025.PMID 41222651