Psych · Emergency psychiatry — police liaison and community emergency detention
Police liaison and community emergency detention
Also known as Police mental health liaison · Crisis Intervention Team CIT · Street triage · Co-responder model · Section 136 · Emergency psychiatric detention · Place of safety · Community emergency examination
Exam-exhaustive fellowship reference on police–mental-health liaison in the community, emergency detention principles (public-place vs private-premises pathways), place-of-safety standards, CIT and co-responder/street-triage models, medical-first assessment, least-restrictive alternatives, information-sharing, documentation, equity, and multi-region legal humility without inventing statutes. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Definition and classification
What this topic covers
Police are frequent first responders to people in mental-health crisis. Psychiatry exams test whether you can: (1) describe lawful emergency powers at principle level; (2) choose response models that divert from criminalisation; (3) prioritise medical safety and de-escalation; (4) complete assessment and disposition after conveyance; and (5) show jurisdiction humility.[1][11]
Core definitions
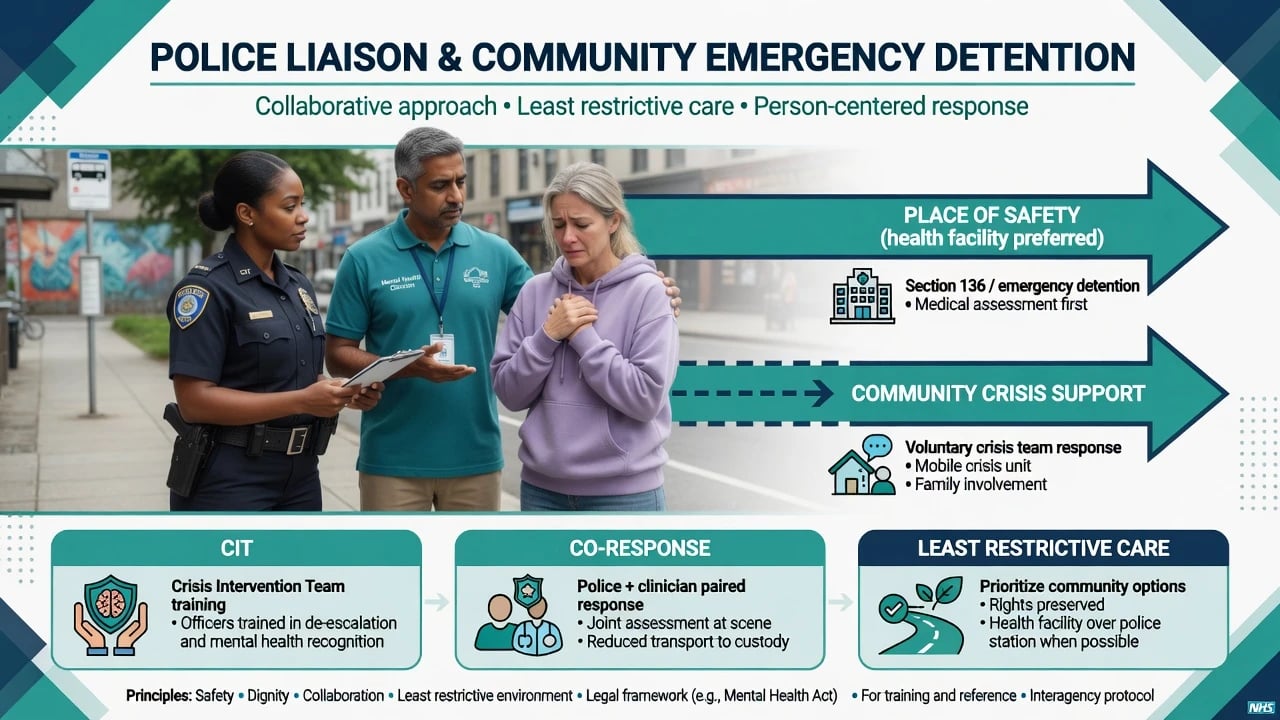
- Police–mental-health liaison: formal partnership (MOUs, joint training, shared pathways, drop-off agreements) between law enforcement and mental-health services, not only one-off phone calls.[1][3]
- Community emergency detention / police emergency power: statutory authority allowing officers (or authorised persons) to remove, convey, or briefly hold a person who appears to have a mental disorder and needs immediate care/control, for the purpose of assessment — not punishment.[13][14]
- Place of safety: location authorised for assessment under local rules. Health facilities are preferred when available and clinically/safe appropriate; police cells are a last-resort option in many modern policy frameworks.[13][11]
- Least-restrictive alternative: achieve necessary safety with the least intrusion on liberty — voluntary engagement, mobile crisis, informal support before compulsion when safe.[11][15]
Public place vs private premises (classic exam fork)
In England & Wales, examiners expect named landmark powers: Section 136 (public place — remove to place of safety for assessment) and Section 135 (warrant-based entry to private premises in defined circumstances). Detention duration and place-of-safety rules have been reformed over time — quote current local Code of Practice, not memory of an outdated hour limit as universal law.[13][14]
In ANZ, most US states, India, and Canada, analogous emergency examination / emergency hold / police apprehension powers exist but section numbers, time limits, who may authorise, and place-of-safety definitions differ. For FRANZCP/ABPN multi-board answers: state the principles (apparent mental disorder; serious risk or need for care/control; least restrictive; prompt specialist assessment; rights and review) and say you would verify the current local Act and policy — do not invent a number.[11][13]
Response-model typology
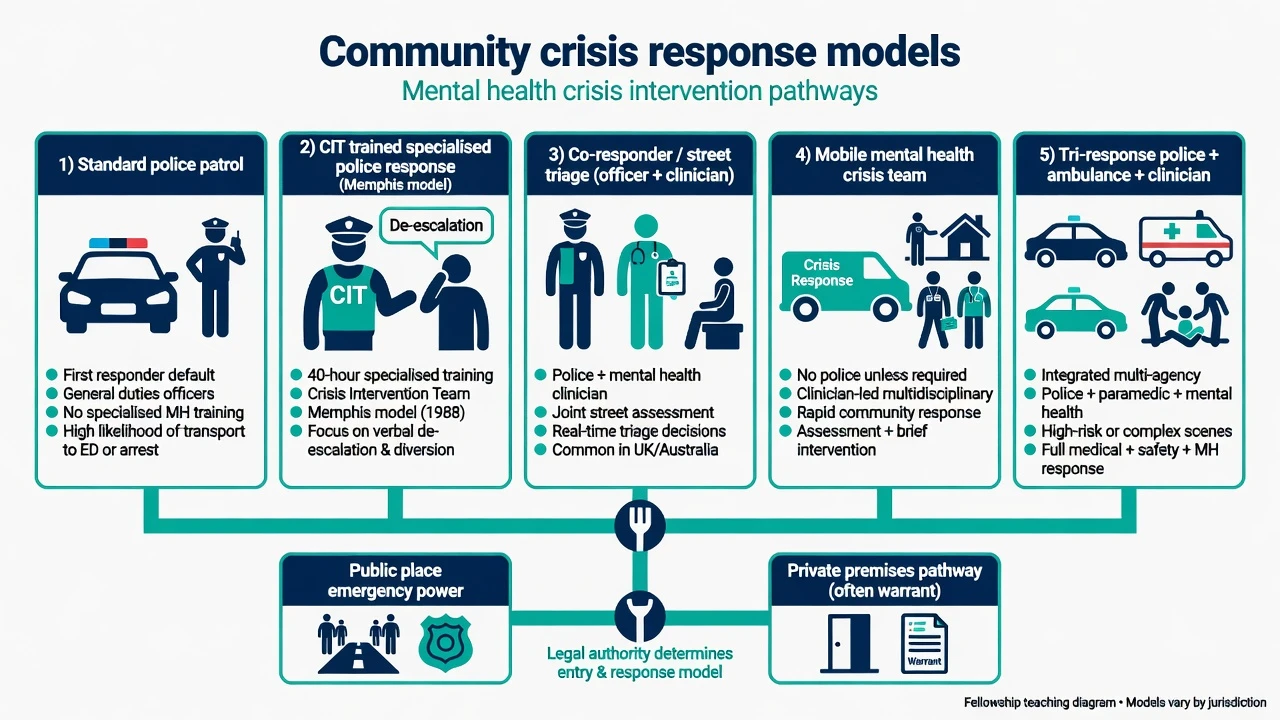
Deane and colleagues described specialised partnerships: police-based specialised police response, police-based specialised mental-health response, and mental-health-based specialised mental-health response.[1] Steadman compared outcomes across major models and found specialised approaches more often resolved incidents without arrest than non-specialised responses.[2] Contemporary practice adds co-responder/street triage (clinician with police at scene) and tri-response (police + ambulance + mental-health clinician).[10][12][17]
- Specialist police training
- De-escalation focus
- Needs drop-off facility
- Strong officer-level evidence
- Clinician at scene
- Real-time assessment
- Diversion potential
- Heterogeneous models
- Police + ambulance + MH
- Medical + safety + MH
- ANZ PACER-type examples
- Emerging evidence base
Epidemiology and system load
Police mental-health contacts are common; volume varies by city, availability of crisis alternatives, substance patterns, and housing precarity.[1][11] Officers report higher confidence when specialised programmes exist.[3]
UK Section 136 literature shows high rates of serious mental illness among detainees and historically incomplete knowledge of the power among ED staff and officers — training and joint protocols matter.[13][14]
Equity is not optional: in several systems, Indigenous peoples and ethnic minorities are over-represented in police mental-health contacts and restrictive outcomes. Monitor rates, use cultural supports and interpreters, and avoid criminalising distress shaped by trauma and disadvantage.[11]
Mechanisms and drivers
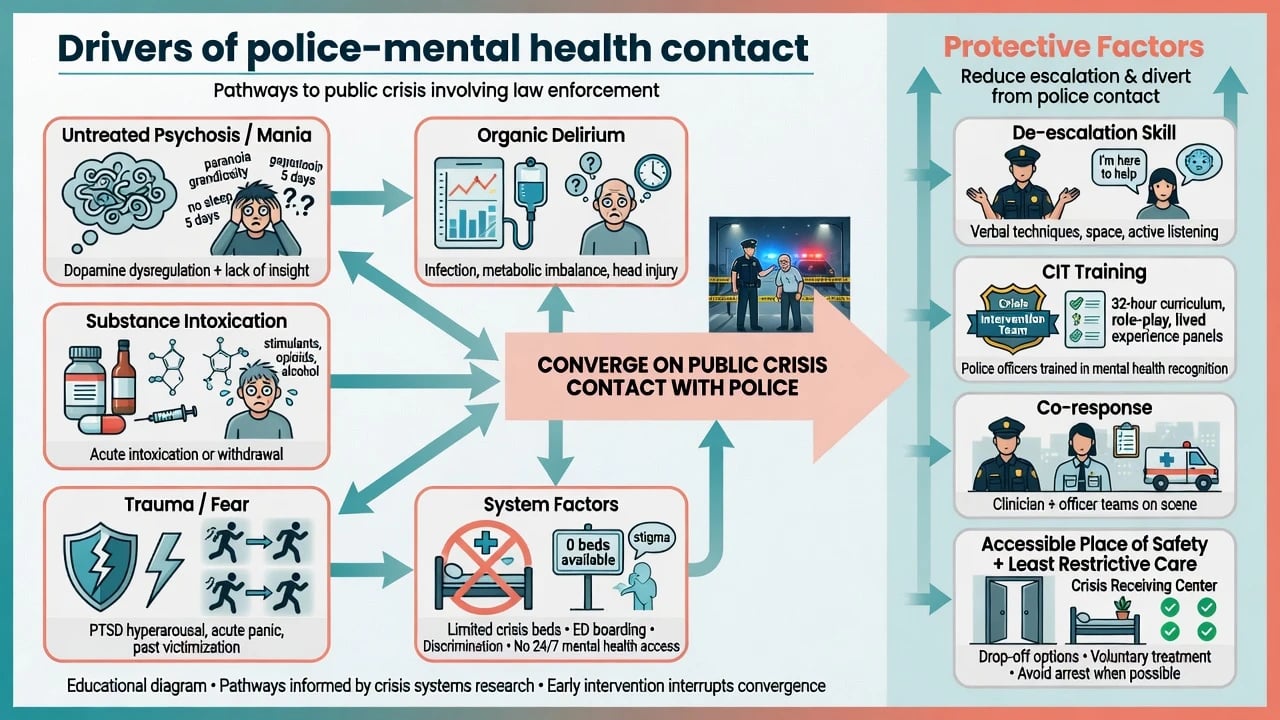
Drivers span clinical state (untreated psychosis, mania, severe suicidality, panic), substances (stimulants, alcohol), organic pathology (delirium, head injury, metabolic crisis), trauma/fear, and system gaps (no crisis beds, delayed community response, stigma). Force and custody escalate threat physiology; skilled de-escalation and health alternatives reduce need for physical intervention.[15][11]
Clinical presentation
Exam stems typically include: public psychotic agitation; welfare checks after family reports; self-harm threats in a park; weapons with agitation; “police brought for assessment” with sparse history; co-responder scene decisions; frequent callers cycling police–ED–street.[2][10]
Differential diagnosis
| Pattern | Think of | Do not miss |
|---|---|---|
| Acute behavioural change + vital sign instability | Organic/medical emergency | Hypoglycaemia, hypoxia, ICH, encephalitis |
| Intoxication timeline clear | Substance-driven crisis | Withdrawal seizures, serotonin toxicity |
| Persecutory psychosis, untreated | MH emergency detention pathway | Named victim risk / means |
| Planned offending without mental disorder | Criminal justice primary | Still screen for MH comorbidity |
| Private dwelling refusal | May need warrant pathway where law requires | Do not invent entry powers |
| Differential framing must separate organic emergency, intoxication, psychosis-driven crisis, pure criminal conduct, and private-premises legal pathways before choosing detention versus diversion.[15][11][13] |
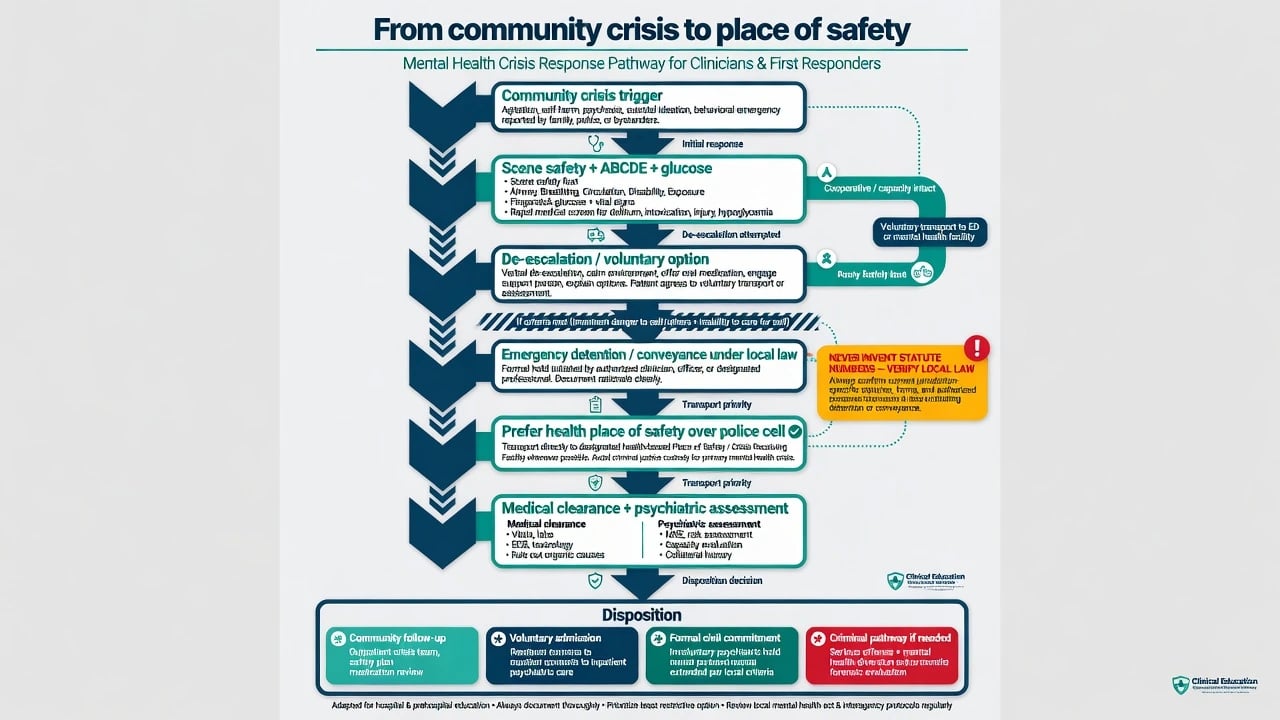
Always run ABCDE + glucose in parallel with behavioural assessment.[15][11]
Bedside and scene assessment
- Scene safety — exits, weapons, backup, one lead communicator; Project BETA verbal de-escalation when safe.[15]
- Medical screen — airway, breathing, circulation, disability, exposure; SpO2; fingerstick glucose; look for head injury, toxidromes, hyperthermia.
- Threshold for emergency power (principles) — does the person appear to have a mental disorder? Is there immediate need for care/control or serious risk? Are less restrictive options unsafe or refused?
- Public vs private setting — maps to different legal pathways; verify local rules.[13]
- MSE and risk — psychosis, mania, suicidality, intent/plan, weapon access, named third-party risk.
- Capacity — decision-specific capacity for accepting/refusing transfer (not a global label).
- Collateral — family, prior notes, crisis plan, alerts where lawful.
Investigations
Proportionate medical work-up based on risk of organic disease; toxicology when indicated; pregnancy test when relevant. Record search and prior risk information when lawful. Labs do not replace clinical–legal criteria for detention or release.[11]
Immediate management
On scene
- Protect public, person, and staff; remove weapons when safe and lawful.
- De-escalate first when clinically and operationally safe (space, calm voice, one speaker, offer choices).[15]
- Offer voluntary transfer to ED/crisis hub if capacity and safety allow.
- If criteria met: convey under local emergency powers to a preferred health place of safety.
- Treat life threats first (airway compromise, severe overdose, uncontrolled seizure, excited behavioural disturbance with hyperthermia — medical pathway).
At the place of safety / ED
- Handoff quality: reason for detention, verbatim threats, weapons, substances, medical issues, times, next of kin.
- Parallel medical clearance and psychiatric assessment — not endless “medically clear” bureaucracy that delays care for pure psychiatric presentations without medical red flags.
- Decide disposition: community follow-up with safety plan; voluntary admission; formal involuntary admission under local civil criteria; or criminal process if independent offending requires it.[2][11]
Rapid tranquillisation interface
If severe agitation threatens safety after de-escalation fails, use local RT protocols (agent, dose, route, monitoring — see acute agitation topic). This is clinical care under appropriate legal authority, not “chemical restraint for police convenience.” Document indication and observations.[15]
Definitive system management and models
Crisis Intervention Team (CIT)
Memphis-model CIT pairs specialist officer training (classically ~40 hours) with community partnership and a reliable psychiatric receiving facility / no-refusal drop-off concept.[4][7] Compton’s review synthesised early evidence; later paired studies showed improved officer knowledge, attitudes, and skills and examined force, referral, and arrest patterns.[4][5][6] Watson and colleagues conclude CIT can be considered an evidence-based practice for officer-level cognitive/attitudinal outcomes, with more work needed on broader system outcomes.[8] Rogers and colleagues review effectiveness analyses with similar nuance: training benefits are clearer than uniform effects on arrests or force across all settings.[9]
Co-responder / street triage
Puntis systematic review of co-responder “street triage” models found heterogeneous designs; programmes often aim to reduce unnecessary detention/arrest and speed clinical input, with limited high-quality outcome data overall — still a high-yield exam model to name.[10]
Continuum of crisis care
Balfour and colleagues frame collaborative crisis response as part of a continuum (someone-to-call, someone-to-respond, somewhere-to-go), arguing police should not be the only 24/7 behavioural-health system.[11]
Tri-response / PACER-type models
ANZ-relevant tri-response literature (police–ambulance–mental health) examines effects on involuntary detention and crisis outcomes; evidence is developing and model-dependent.[12][16][17]
Subtypes and high-yield scenarios
- Public-place psychotic crisis (UK s136-type stem): assess criteria; convey to health place of safety; specialist assessment; do not treat as arrest.[13]
- Private premises: may require warrant/authorised entry pathway — do not invent entry powers.[13]
- CIT first response: de-escalate, divert to care, document force avoidance when successful.[5][6]
- Co-response on scene: clinician assessment may avoid conveyance or refine destination.[10]
- Rural remote: long transport, limited places of safety, tele-psychiatry backup, plan fuel/staffing/risk.
- Youth: avoid police cells; involve caregivers; developmental communication.
- Indigenous / CALD: interpreter, cultural support person, equity lens on detention rates.[11]
- After use of force: medical review, injury documentation, psychological aftermath, governance review.
Complications and pitfalls
- Defaulting to police cells as place of safety.[13][11]
- Inventing statutes or exporting California/UK section numbers to the wrong country.
- Missing organic causes of agitation.[15]
- Criminalising pure illness when diversion exists — or ignoring criminal acts that need investigation.
- Poor handoffs (no history, no times, no risk summary).[14]
- Over-reliance on training without drop-off capacity and partnership (CIT without “somewhere to go”).[7][11]
- Releasing high-risk people without follow-up after brief assessment.
- Equity blindness and discriminatory over-detention.
Prognosis and disposition
Many contacts resolve with diversion, brief assessment, and community support. A subset require hospitalisation under civil criteria. System outcomes track crisis continuum capacity as much as officer skill.[2][11]
Disposition ladder (least → more restrictive examples): community crisis support with safety plan → voluntary ED/crisis hub → emergency detention for assessment under local power → formal involuntary admission → forensic/criminal pathway when independently indicated. Match intensity to dynamic risk and continuum capacity, not diagnosis alone.[2][11]
Special populations
Children/adolescents (developmental approach; avoid custody environments); older adults (delirium first); intellectual disability/autism (sensory strategies; avoid criminalising communication of distress); perinatal (infant safety, child protection interfaces); rural (logistics).[11]
Regional deltas
FRANZCP answers emphasise state/territory Mental Health Acts, police–health MOUs, PACER/tri-response and co-responder local models, cultural safety for Aboriginal and Torres Strait Islander and Māori peoples, and principle-level emergency powers. Name that detention criteria, authorised persons, and time limits are jurisdiction-specific — verify current Act; do not invent section numbers in the viva.[12][16][17]
Evidence and guidelines (exam map)
- Partnership typology and comparative diversion outcomes: Deane, Steadman, Borum.[1][2][3]
- CIT evidence: Compton reviews/trials; Watson primer and EBP analysis; Rogers effectiveness review.[4][5][6][7][8][9]
- Co-response/street triage: Puntis systematic review.[10]
- Continuum collaborative care: Balfour.[11]
- Tri-response/PACER: Heffernan series.[12][16][17]
- UK s136 literature and knowledge gaps: Borschmann, Lynch.[13][14]
- Scene de-escalation: Project BETA Richmond consensus.[15]
Exam pearls
POLICE
References
- [1]Deane MW, Steadman HJ, Borum R, et al. Emerging partnerships between mental health and law enforcement Psychiatr Serv, 1999.PMID 9890588
- [2]Steadman HJ, Deane MW, Borum R, et al. Comparing outcomes of major models of police responses to mental health emergencies Psychiatr Serv, 2000.PMID 10783184
- [3]Borum R, Deane MW, Steadman HJ, et al. Police perspectives on responding to mentally ill people in crisis: perceptions of program effectiveness Behav Sci Law, 1998.PMID 9924765
- [4]Compton MT, Bahora M, Watson AC, et al. A comprehensive review of extant research on Crisis Intervention Team (CIT) programs J Am Acad Psychiatry Law, 2008.PMID 18354123
- [5]Compton MT, Bakeman R, Broussard B, et al. The police-based crisis intervention team (CIT) model: I. Effects on officers' knowledge, attitudes, and skills Psychiatr Serv, 2014.PMID 24382628
- [6]Compton MT, Bakeman R, Broussard B, et al. The police-based crisis intervention team (CIT) model: II. Effects on level of force and resolution, referral, and arrest Psychiatr Serv, 2014.PMID 24382643
- [7]Watson AC, Fulambarker AJ The Crisis Intervention Team model of police response to mental health crises: a primer for mental health practitioners Best Pract Ment Health, 2012.PMID 24039557
- [8]Watson AC, Compton MT, Draine JN The crisis intervention team (CIT) model: An evidence-based policing practice? Behav Sci Law, 2017.PMID 28856706
- [9]Rogers MS, McNiel DE, Binder RL Effectiveness of Police Crisis Intervention Training Programs J Am Acad Psychiatry Law, 2019.PMID 31551327
- [10]Puntis S, Perfect D, Kirubarajan A, et al. A systematic review of co-responder models of police mental health 'street' triage BMC Psychiatry, 2018.PMID 30111302
- [11]Balfour ME, Hahn Stephenson A, Delany-Brumsey A, et al. Cops, Clinicians, or Both? Collaborative Approaches to Responding to Behavioral Health Emergencies Psychiatr Serv, 2022.PMID 34666512
- [12]Heffernan J, McDonald E, Hughes E, et al. Tri-Response Police, Ambulance, Mental Health Crisis Models in Reducing Involuntary Detentions of Mentally Ill People: Protocol for a Systematic Review Int J Environ Res Public Health, 2021.PMID 34360521
- [13]Borschmann RD, Gillard S, Turner K, et al. Section 136 of the Mental Health Act: a new literature review Med Sci Law, 2010.PMID 20349693
- [14]Lynch RM, Simpson M, Higson M, et al. Section 136, The Mental Health Act 1983; levels of knowledge among accident and emergency doctors, senior nurses and police constables Emerg Med J, 2002.PMID 12101134
- [15]Richmond JS, Berlin JS, Fishkind AB, et al. Verbal De-escalation of the Agitated Patient: Consensus Statement of the American Association for Emergency Psychiatry Project BETA De-escalation Workgroup West J Emerg Med, 2012.PMID 22461917
- [16]Heffernan J, et al. The association between the Police, Ambulance, Clinician Early Response (PACER) model and involuntary detentions of people living with mental illness: A retrospective observational study J Psychiatr Ment Health Nurs, 2024.PMID 38567862
- [17]Heffernan J, et al. Tri-Response Police, Ambulance, Mental Health Crisis Models in Reducing Involuntary Detentions of Mentally Ill People: A Systematic Review Healthcare (Basel), 2022.PMID 36548169