Psych · Emergency psychiatry
Psychiatric emergencies
Also known as Acute agitation · Rapid tranquillisation · Severe behavioural disturbance · Excited delirium · Suicidal crisis · NMS · Serotonin syndrome · Catatonic emergency · Psychiatric emergency
Exam-exhaustive fellowship hub on psychiatric emergencies — agitation ladders with doses, suicidal crisis, medical mimics, SBD/ExDS frameworks, NMS and serotonin toxicity discriminators, lithium toxicity, catatonic emergency, capacity and least-restrictive involuntary care, ED-psych liaison and disposition. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Psychiatric emergencies are not a single disease. They are a set of time-critical clinical and legal problems — acute agitation, suicidal crisis, severe behavioural disturbance, toxicological disasters, and catatonic collapse — that every FRANZCP, MRCPsych and ABPN candidate must manage as a consultant would. The examinable skill is structured sequence under uncertainty: scene safety, medical exclusion, risk formulation, pharmacological restraint used only when necessary, and lawful least-restrictive disposition. This hub is written as algorithms and ladders, not as a disease monograph.[1][14]
Overview and definition
A psychiatric emergency is any presentation in which mental disorder, substance intoxication or withdrawal, or a medical mimic creates imminent risk of death, serious harm, or irreversible deterioration, requiring immediate assessment and intervention. The label is functional, not nosological: the same syndrome may be primary psychosis one night and encephalitis the next.[14][15]
Core emergency clusters you must own:[1]
- Acute agitation and aggression
- Suicidal crisis and near-lethal self-harm
- Severe behavioural disturbance / excited delirium frameworks
- Catatonic emergency (retarded or excited; malignant)
- Drug emergencies: NMS, serotonin toxicity, lithium toxicity, acute dystonia
- Capacity and involuntary treatment crises
- ED boarding and liaison failures that create secondary harm[4]
DSM-5-TR / ICD-11 note. Emergencies are managed by syndrome and risk, not by waiting for a final spectrum diagnosis. Catatonia is diagnosed by operational motor-behavioural criteria (DSM-5-TR: three or more of twelve features) and is treated as a syndrome across medical and psychiatric aetiologies.[8][10]
Classification of emergency presentations
| Cluster | Time pressure | Primary risk | First team move |
|---|---|---|---|
| Agitation / violence | Minutes | Assault, restraint injury, absconding | Safety + de-escalation |
| Suicidal crisis | Minutes–hours | Completed suicide, means access | Means restriction + structured risk |
| SBD / ExDS-type | Minutes | Collapse, hyperthermia, rhabdomyolysis | Medical resuscitation readiness |
| Catatonia | Hours | Dehydration, VTE, malignant conversion | Lorazepam pathway |
| NMS | Hours–days | Multi-organ failure | Stop dopamine antagonists |
| Serotonin toxicity | Hours | Hyperthermia, seizures | Stop serotonergics |
| Lithium toxicity | Hours | Neurotoxicity, arrhythmia, renal failure | Levels + fluids ± dialysis |
This is an approach topic: every row is a mini-protocol. Examiners reward candidates who name the protocol rather than narrate vaguely about “settling the patient.”[1][6][4]
Epidemiology and risk context
Psychiatric presentations occupy a large fraction of ED and inpatient crisis work. Violence in clinical settings is uncommon relative to total contacts but concentrates among people with prior violence, active intoxication, paranoia with threat content, command hallucinations to harm, and chaotic environments.[1]
Suicide. Lifetime completed suicide in schizophrenia is approximately 5 percent, with attempts far more common; early illness and post-discharge periods are high-yield risk windows.[16] Categorical “low / medium / high” risk labels have poor positive predictive value for imminent suicide among psychiatric inpatients — they can create false reassurance. Use structured enquiry and concrete safety actions, not score theatre.[16][17]
Restraint and seclusion themselves carry morbidity (asphyxia risk, rhabdomyolysis, psychological trauma). Evidence comparing restraint versus seclusion is limited; minimisation and rapid review are the ethical and clinical defaults.[20]
Mechanisms — why behavioural emergencies escalate
Agitation is a final common pathway. Psychosis, mania, fear, pain, hypoxia, hypoglycaemia, head injury, intoxication, withdrawal and delirium all converge on the same motor-behavioural output. That is why ABCDE and glucose are not optional “medical bits” — they are the psychiatry exam content.[14]
NMS. Idiosyncratic reaction to dopamine D2 antagonism (antipsychotics, antiemetics such as metoclopramide): severe rigidity, reduced consciousness, autonomic instability and hyperthermia evolving over hours to days. International consensus criteria (Delphi) and subsequent validation define the construct examiners expect you to recognise.[6][7]
Serotonin toxicity. Excess serotonergic tone (especially 5-HT2A) from drug interactions (for example MAOI plus serotonergic agent). Onset is typically hours, with neuromuscular hyperexcitability — clonus and hyperreflexia, often lower-limb predominant — as the diagnostic hallmark in the Hunter criteria.[4][5]
Lithium. Narrow therapeutic index; toxicity rises with sodium loss, dehydration, intercurrent illness, and interacting drugs (NSAIDs, ACE inhibitors, thiazides). Acute overdose and chronic accumulation differ in tissue distribution and dialysis urgency; EXTRIP provides extracorporeal treatment thresholds.[18]
Catatonia. Motor-behavioural syndrome with GABAergic treatment response. Lorazepam and ECT are disease-modifying, not cosmetic sedation — a classic viva hinge.[9][10]
Clinical presentation
Scene and interview safety
Before phenomenology, set the room: clear exit for you and the patient, remove potential weapons, adequate staffing, no cornering, calm voice, one primary speaker, offer water and seating. State your role and intention to help. If violence is imminent, withdraw and call security/police per local protocol — heroism is not a competency.[1][2]
Acute agitation
Look for pacing, clenched fists, loud speech, invasion of space, throwing objects, threat content, and escalating autonomic signs. Ask about fear, command voices, pain, and intoxication. Document verbatim threats. Distinguish purposeful aggression (instrumental) from disorganised agitation (delirium, excited catatonia, stimulant toxicity).[1]
Suicidal crisis
Enquire specifically: ideation, plan, intent, timing, preparatory acts, access to means, prior attempts (especially near-lethal), hopelessness, command hallucinations to die, alcohol/drugs, protective factors (children, faith, future goals, therapeutic alliance). Near-fatal deliberate self-harm identifies a group requiring intensive aftercare thinking, not brief reassurance.[16][17]
Severe behavioural disturbance / excited delirium frameworks
Extreme continuous agitation, apparent pain tolerance, hyperthermia risk, incoherent speech, and sudden collapse risk define the operational emergency. Treat the physiology first. The historical “excited delirium” label is contested and has been criticised for racial bias and forensic misuse — prefer descriptive language (severe behavioural disturbance) and manage the medical syndrome without diagnostic grandstanding.[11][12]
Catatonia poles
Retarded: mutism, stupor, posturing, waxy flexibility, negativism.
Excited: purposeless motor agitation, stereotypy, grimacing.
Both can progress to malignant catatonia with fever and autonomic instability — overlapping the NMS clinical space and sometimes the same pathway.[8][10]
Differential diagnosis — medical mimics first
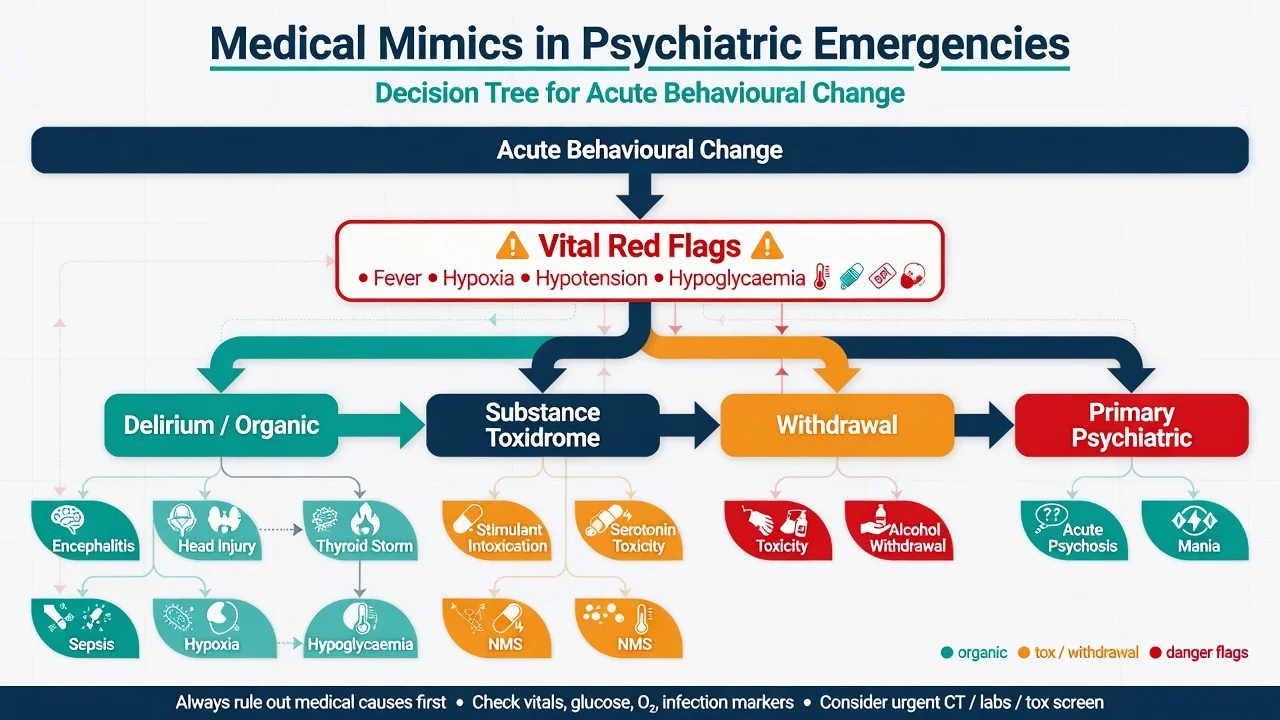
Never miss list (with discriminators):[1]
- Delirium — inattention, fluctuation, medical signs; not fixed delusional system alone
- Hypoglycaemia / hypoxia / hypercarbia — observations and gas exchange
- Head injury / intracranial event — trauma history, focal neurology, reduced consciousness
- Encephalitis (including anti-NMDAR) — new psychosis with dysautonomia, movement, seizure, female predominance classic but not exclusive
- Thyroid storm / phaeochromocytoma-like states — fever, tachycardia, hypertension
- Sepsis / meningitis — fever, meningism, source
- Alcohol or benzodiazepine withdrawal — tremor, diaphoresis, seizures, delirium
- Stimulant intoxication — mydriasis, tachycardia, paranoia, hyperthermia
- NMS / serotonin toxicity / anticholinergic toxicity — see toxidrome table
- Primary psychosis or mania — after the above are considered[4]
Medical clearance is targeted, not a fixed pan-lab ritual for every low-risk presentation. AAEP task force guidance emphasises history, examination and risk-based testing, with documentation of rationale.[14][15]
Clinical and bedside assessment
ABCDE always. Pulse oximetry, blood pressure, heart rate, respiratory rate, temperature, conscious level, capillary glucose. Then:[1]
- Scene safety and staff plan
- Focused history (onset tempo, substances, meds, medical disease, trauma)
- MSE for emergency content: suicidality, homicidality, command hallucinations, insight, attention
- Risk formulation (static + dynamic + protective + contextual)
- Capacity for the specific decision at hand
- Legal status and least-restrictive options
- Collateral and access to means[16]
Scales (Bush-Francis Catatonia Rating Scale, agitation scales) structure observation; they do not replace clinical judgment.[8][1]
Investigations
| Priority | Test | Why |
|---|---|---|
| Immediate | Observations + glucose | Hypoglycaemia and instability kill first |
| Before antipsychotics | ECG (QTc), pregnancy test if relevant | Safety of pharmacological RT |
| Agitation / restraint | CK, U&E, FBC | Rhabdomyolysis, renal failure |
| NMS suspicion | CK, WCC, U&E, LFT, ABG as needed | Severity and organ failure |
| Serotonin suspicion | Clinical (Hunter); labs supportive | Diagnosis is clinical |
| Lithium | Serum lithium, U&E, ECG | Level guides dialysis decisions |
| Overdose context | Paracetamol, salicylate ± others | Concurrent self-poisoning |
| Organic red flags | CT/MRI, LP, EEG, autoimmune panel | Encephalitis, seizure, mass lesion |
| Substance | UDS with known limitations | Negative screen does not exclude |
Do not delay life-saving treatment for a urine drug screen. Do not diagnose “functional” in the presence of fever and fluctuating attention without a medical work-up plan.[14][15][18]
Management — resuscitation and safety
Non-pharmacological first
Quiet space, reduce stimulation, remove audience, offer food/water, one calm communicator, avoid prolonged prone restraint, continuous observation if risk is high. De-escalation is first-line in BAP/NAPICU consensus frameworks; regional ED services also publish pragmatic SBD sedation pharmacokinetics (for example intramuscular droperidol programmes in Australia).[1][2]
Rapid tranquillisation ladder
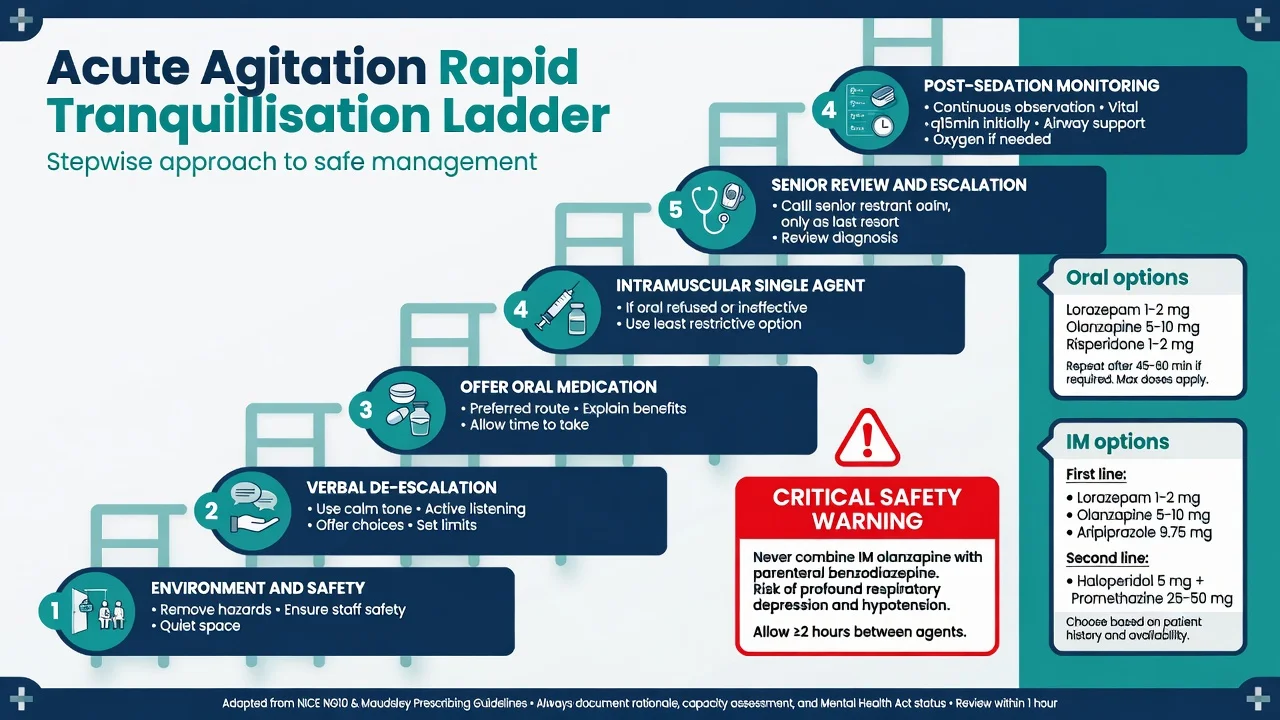
Principles (BAP/NAPICU and NICE-aligned):[1]
- De-escalate and treat causes (pain, fear, psychosis, delirium).
- Offer oral medication first if safe.
- If IM required, use a single agent where possible.
- Monitor airway, respiration, SpO2, BP, HR, consciousness after sedation.
- Document capacity, legal status, and least-restrictive rationale.[19]
Named oral options (adult, typical starting range)
Use local formulary and product information; reduce doses in older adults and medically frail patients.[1]
- Lorazepam 1–2 mg oral — anxiolysis and sedation; useful when psychosis is not the primary driver
- Olanzapine 5–10 mg oral (orodispersible if available) — antipsychotic plus sedation
- Risperidone 1–2 mg oral — antipsychotic option
- Promethazine 25–50 mg oral — sedating antihistamine option in some protocols
- Aripiprazole 10–15 mg oral — less sedating; useful when metabolic/QTc profile matters[1]
Named IM options (adult)
First-line single-agent IM options in UK consensus frameworks include:[1]
- IM lorazepam 1–2 mg
- IM olanzapine 5–10 mg (not with parenteral benzodiazepine)
- IM aripiprazole 5.25–15 mg (commonly 9.75 mg)[1]
Second-line / evidence-backed combination from TREC:
IM haloperidol 5 mg + IM promethazine 25–50 mg was superior to haloperidol alone for rapid tranquillisation in pragmatic Brazilian trials — promethazine reduces acute dystonia risk and improves early calm.[3]
ECG and ½-life caveats. Prefer avoiding IM haloperidol if QTc is prolonged or cardiac risk is high; obtain ECG as soon as practicable. Flumazenil is not a routine RT adjunct.[1]
Post-sedation monitoring
Minimum practical standard after parenteral RT: continuous observation until ambulatory and conversant; respiratory rate, SpO2, BP, HR, conscious level every 15 minutes for at least 1 hour, then as clinically indicated. Have oxygen, suction, and airway-skilled staff available. Document recovery.[1]
Severe behavioural disturbance rescue
If standard RT fails and danger remains extreme, ketamine has been studied as rescue for difficult-to-sedate SBD in ED settings and in prehospital paramedic protocols — use only within local ED/critical-care governance with airway readiness.[13]
Acute dystonia
Painful muscle spasm (oculogyric crisis, torticollis, laryngospasm risk) after antipsychotics is an emergency. Treat with an anticholinergic — for example benztropine 1–2 mg IM/IV or procyclidine 5–10 mg IM (local availability) — and review the antipsychotic plan.[1]
Management — definitive pathways by emergency type
Suicidal crisis
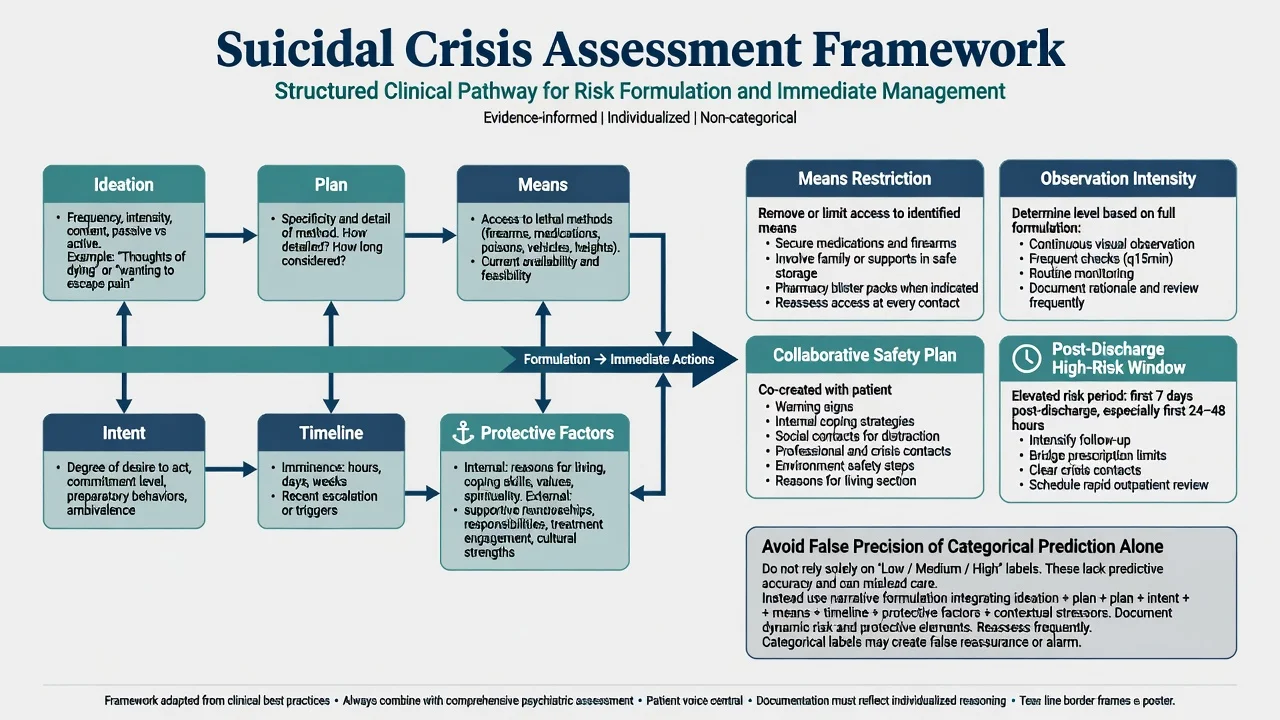
Immediate actions: remove or secure means (medications, firearms, ligatures, heights), continuous or intermittent observation matched to risk, treat intoxication and pain, address command hallucinations, involve supports with consent or under lawful information-sharing.[1]
Safety planning is collaborative and concrete: warning signs, internal coping, social contacts, professional contacts, means reduction, reasons for living. Disposition depends on residual risk after intervention, support at home, and ability to engage — not on a single score.[16][17]
NMS pathway
- Stop antipsychotics and other dopamine antagonists.
- ABCDE, cooling, IV fluids, critical care liaison for severe cases.
- Benzodiazepines for agitation and mild-moderate rigidity.
- Specialist discussion of bromocriptine or dantrolene in severe refractory cases (evidence imperfect; supportive care is foundational).
- Exclude serotonin toxicity, malignant hyperthermia (anaesthetic context), infection, and malignant catatonia.
- Restart antipsychotics later only with extreme caution, different agent, low dose, and monitoring.[6][7]
Serotonin toxicity pathway
- Stop all serotonergic agents.
- Supportive care and external cooling if hyperthermic.
- Benzodiazepines first-line for agitation and neuromuscular excitation.
- Consider cyproheptadine (serotonin antagonist) in moderate cases — commonly discussed loading around 12 mg orally/NG then 2 mg every 2 hours as needed within specialist toxicology advice and local protocol.
- Critical care for severe hyperthermia, rigidity, or multi-organ failure.[4][5]
Toxidrome comparison
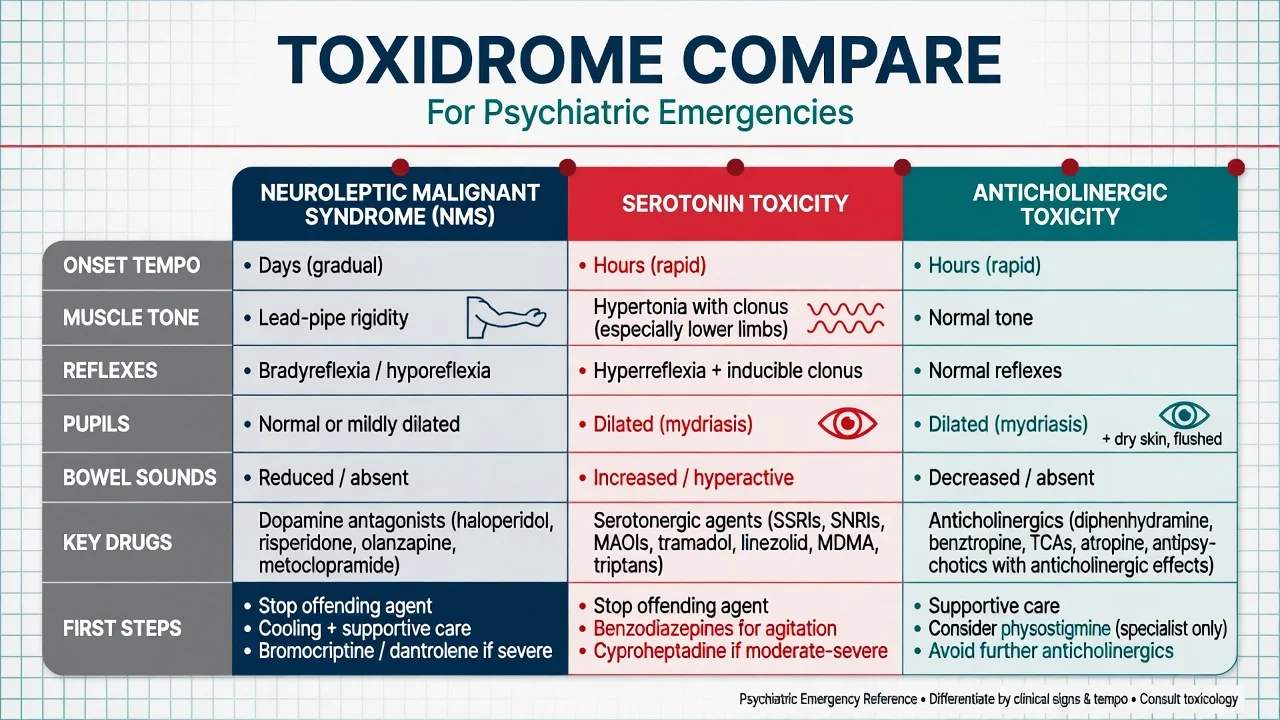
NMS
- Onset hours to days after dopamine blockade
- Lead-pipe rigidity
- Bradyreflexia / hyporeflexia
- Autonomic instability and fever
- Stop antipsychotics; support ± ICU
Serotonin toxicity
- Onset hours after serotonergic load
- Clonus and hyperreflexia (lower limbs)
- Diarrhoea, mydriasis, agitation
- Hunter criteria decision rules
- Stop serotonergics; benzos ± cyproheptadine
Anticholinergic
- Dry skin, urinary retention, delirium
- Normal tone and reflexes (no clonus)
- Mydriasis, decreased bowel sounds
- Avoid more anticholinergics
- Supportive care; specialist physostigmine only
Lithium toxicity
Check level, electrolytes, renal function and ECG. Give IV fluids. Contact toxicology. Extracorporeal treatment (haemodialysis) is recommended by EXTRIP for severe poisoning — examples include lithium level above 4.0 mmol/L in impaired kidney function, level above 5.0 mmol/L, or significant neurotoxicity/decreased consciousness; exact thresholds are in the EXTRIP review and must be applied with toxicology input.[18]
Catatonic emergency
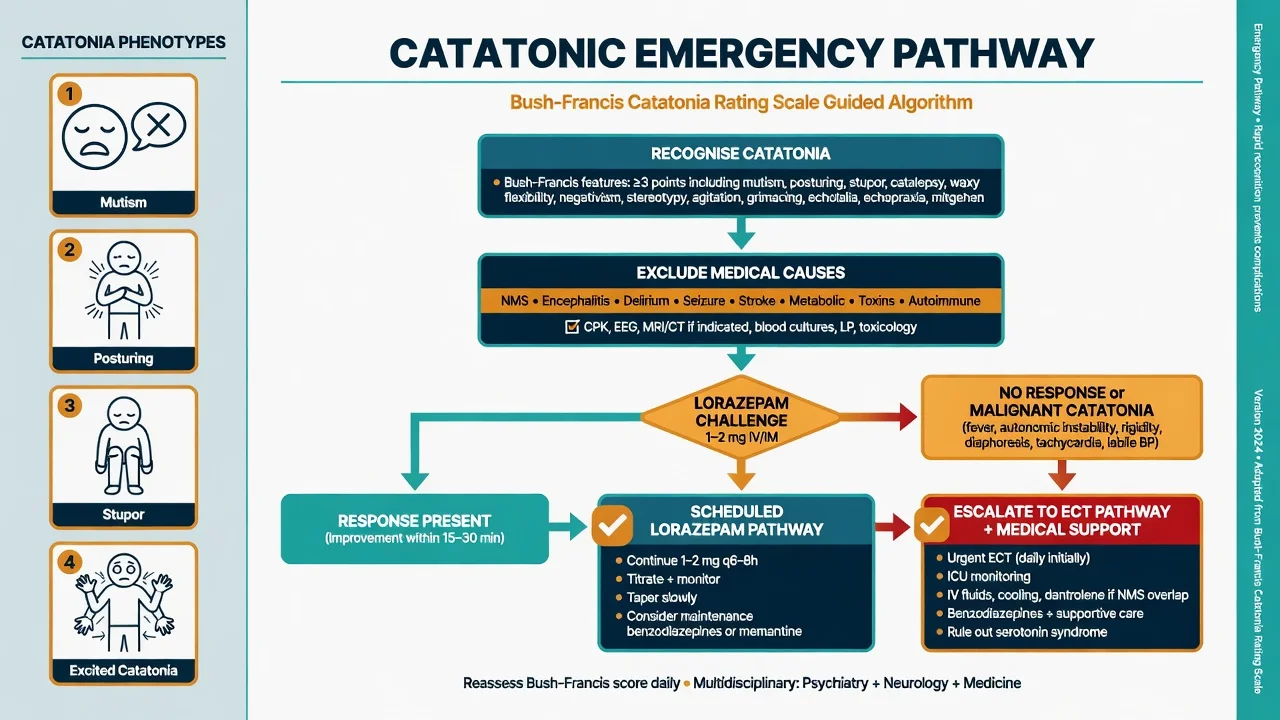
- Recognise with Bush-Francis style examination (mutism, posturing, stupor, negativism, echolalia/echopraxia, excitement, etc.).
- Exclude medical causes and NMS overlap.
- Lorazepam challenge: 1–2 mg IV/IM/oral, reassess in 5–30 minutes (route-dependent). Marked improvement supports the diagnosis and guides therapy.
- Scheduled lorazepam (divided daily dosing, titrated) if responsive.
- If non-response, or malignant features (fever, autonomic instability, rising CK, deterioration), escalate promptly to ECT with medical support — do not watch malignant catatonia for days while “hoping for oral meds.”[8][9][10]
Capacity, law and least-restrictive care
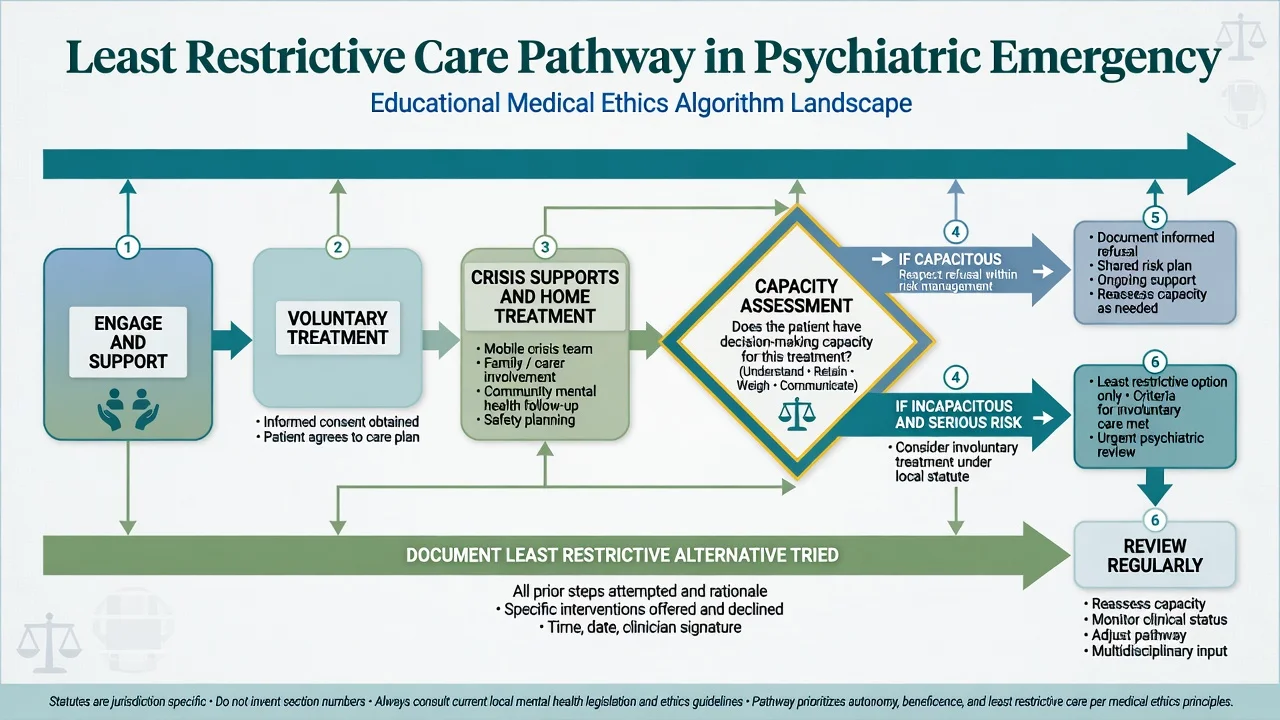
Capacity (functional test, broadly shared across common-law systems): can the person understand, retain, use/weigh, and communicate a decision? Capacity is decision-specific and time-specific. Being detained under a Mental Health Act does not automatically equal incapacity for every decision, and being unwell does not automatically equal incapacity.[19]
Least-restrictive principle. Prefer voluntary care, crisis supports, and home treatment when safe. Involuntary treatment is reserved for serious risk with impaired decision-making (or statutory criteria in your jurisdiction) after less restrictive options are unsuitable. Do not invent section numbers for Australia, New Zealand, England, or the United States in exams — name the principle and say you will apply the local statute with senior/legal advice.[19][1]
Document: risks, options considered, why less restrictive options failed or were unsafe, capacity findings, and review schedule.[19]
Disposition algorithm
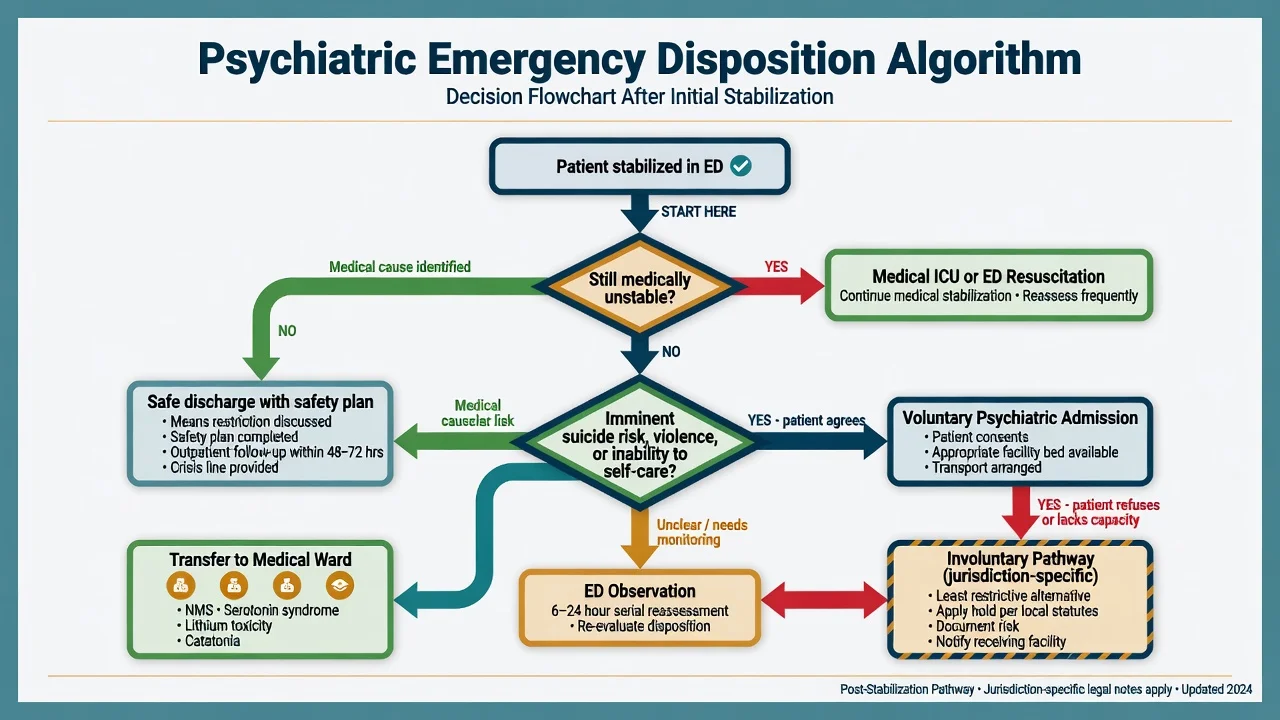
| Destination | When |
|---|---|
| Medical ED / ICU | Unstable vitals, severe toxidrome, malignant catatonia, SBD with hyperthermia/rhabdo |
| Psychiatric inpatient (voluntary) | High residual risk, accepts admission, needs containment |
| Involuntary pathway | Serious risk + statutory criteria met; least restrictive documented |
| ED observation | Evolving intoxication, awaiting collateral/means check, short-term safety |
| Discharge with plan | Risk reduced, supports present, means restricted, follow-up timed, crisis contacts given |
Safe discharge checklist after suicidal crisis: means restricted; collaborative safety plan written; supports contacted where lawful; follow-up within a defined short interval; no untreated medical emergency; documentation complete; patient understands how to re-access care.[16][17]
Special populations
Older adults. Delirium until proven otherwise. Use lower RT doses; high fall and QTc risk; avoid polypharmacy sedation.[14]
Children and adolescents. Consent/assent, family systems, lower dosing, avoid treating adolescent distress as adult personality pathology.[1]
Pregnancy. Avoid prone restraint; careful drug choice; postpartum psychosis is a true emergency with infanticide risk — low threshold for admission.[20]
Intellectual disability / autism. Sensory overload and pain may drive behaviour; consider catatonia of autism; environmental first.[9]
Indigenous and culturally diverse peoples (FRANZCP cultural safety). Interpreter, family/kinship decision structures, avoid coercive defaults born of communication failure.[1]
Custody / police interface. Medical assessment rights remain; do not accept “just behavioural” without vitals.[1][14]
Complications and pitfalls
- Labelling encephalitis or delirium as primary psychosis
- Combining IM olanzapine + parenteral benzodiazepine
- Akathisia mistaken for agitation → more antipsychotic
- Prolonged restraint without hydration, temperature monitoring, or repositioning
- False reassurance from “low risk” categories after near-lethal attempt
- Incomplete handover from ED to psych ward or crisis team
- Inventing cross-jurisdictional Mental Health Act sections
- Discharging without means restriction after concrete plan[14]
Evidence, guidelines and regional differences
| Source | Region | Exam use |
|---|---|---|
| BAP/NAPICU 2018 acute disturbance consensus | UK (globally influential) | RT ladder, monitoring, combination bans |
| BAP/NAPICU monitoring and combination rules | UK (global exam influence) | RT safety |
| TREC trials | Brazil / LMIC pragmatic | Haloperidol + promethazine evidence |
| Australian ED SBD literature (droperidol PK; ketamine rescue) | ANZ | SBD rescue pathways under ED governance |
| AAEP medical clearance task force | US | Targeted clearance standards |
| Hunter criteria; Boyer NEJM review | Global | Serotonin toxicity |
| Gurrera NMS Delphi + validation | Global | NMS recognition |
| Bush-Francis + lorazepam/ECT papers | Global | Catatonia |
| Large/Ryan suicide categorisation critique | ANZ-led, global | Risk philosophy |
| EXTRIP lithium | Global toxicology | Dialysis thresholds |
| ExDS bias critique | US/global | Language and equity |
Regional deltas. UK frameworks emphasise lorazepam and BAP/NAPICU process; Australian EDs often have strong droperidol/ketamine SBD experience under emergency medicine protocols; US practice varies by state emergency detention statutes. Always state which guideline you are applying.[1][2][3][13]
Exam pearls
SAFE-RT for agitation emergencies
- Clonus points to serotonin; lead-pipe + bradyreflexia points to NMS.
- Oral first, single IM agent, monitor SpO2.
- Never IM olanzapine + parenteral BZD.
- Catatonia responds to lorazepam/ECT — do not “wait and see” if malignant.
- Capacity is decision-specific; detention ≠ global incapacity.
- Suicide categories predict poorly; actions prevent.
- Statutes are local; principles are examinable.[4]
References
- [1]Patel MX, Sethi FN, Barnes TR, et al. Joint BAP NAPICU evidence-based consensus guidelines for the clinical management of acute disturbance: De-escalation and rapid tranquillisation J Psychopharmacol, 2018.PMID 29882463
- [2]Foo LK, Duffull SB, Calver L, et al. Population pharmacokinetics of intramuscular droperidol in acutely agitated patients Br J Clin Pharmacol, 2016.PMID 27530285
- [3]Huf G, Coutinho ES, Adams CE, et al. Rapid tranquillisation in psychiatric emergency settings in Brazil: pragmatic randomised controlled trial of intramuscular haloperidol versus intramuscular haloperidol plus promethazine BMJ, 2007.PMID 17954515
- [4]Dunkley EJ, Isbister GK, Sibbritt D, et al. The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity QJM, 2003.PMID 12925718
- [5]Boyer EW, Shannon M The serotonin syndrome N Engl J Med, 2005.PMID 15784664
- [6]Gurrera RJ, Caroff SN, Cohen A, et al. An international consensus study of neuroleptic malignant syndrome diagnostic criteria using the Delphi method J Clin Psychiatry, 2011.PMID 21733489
- [7]Gurrera RJ, Mortillaro G, Velamoor V, et al. A Validation Study of the International Consensus Diagnostic Criteria for Neuroleptic Malignant Syndrome J Clin Psychopharmacol, 2017.PMID 28027111
- [8]Bush G, Fink M, Petrides G, et al. Catatonia. I. Rating scale and standardized examination Acta Psychiatr Scand, 1996.PMID 8686483
- [9]Bush G, Fink M, Petrides G, et al. Catatonia. II. Treatment with lorazepam and electroconvulsive therapy Acta Psychiatr Scand, 1996.PMID 8686484
- [10]Fink M, Taylor MA The catatonia syndrome: forgotten but not gone Arch Gen Psychiatry, 2009.PMID 19884605
- [11]Vilke GM, Bozeman WP, Dawes DM, et al. Excited delirium syndrome (ExDS): treatment options and considerations J Forensic Leg Med, 2012.PMID 22390995
- [12]Walsh BM, Agboola IK, Coupet E Jr, et al. Revisiting Excited Delirium: Does the Diagnosis Reflect and Promote Racial Bias? West J Emerg Med, 2023.PMID 36976592
- [13]Isbister GK, Calver LA, Downes MA, et al. Ketamine as Rescue Treatment for Difficult-to-Sedate Severe Acute Behavioral Disturbance in the Emergency Department Ann Emerg Med, 2016.PMID 26899459
- [14]Anderson EL, Nordstrom K, Wilson MP, et al. American Association for Emergency Psychiatry Task Force on Medical Clearance of Adults Part I: Introduction, Review and Evidence-Based Guidelines West J Emerg Med, 2017.PMID 28210358
- [15]Wilson MP, Nordstrom K, Anderson EL, et al. American Association for Emergency Psychiatry Task Force on Medical Clearance of Adult Psychiatric Patients. Part II: Controversies over Medical Assessment, and Consensus Recommendations West J Emerg Med, 2017.PMID 28611885
- [16]Large M, Myles N, Myles H, et al. Suicide risk assessment among psychiatric inpatients: a systematic review and meta-analysis of high-risk categories Psychol Med, 2018.PMID 28874218
- [17]Large MM, Ryan CJ Suicide risk categorisation of psychiatric inpatients: what it might mean and why it is of no use Australas Psychiatry, 2014.PMID 24871970
- [18]Decker BS, Goldfarb DS, Dargan PI, et al. Extracorporeal Treatment for Lithium Poisoning: Systematic Review and Recommendations from the EXTRIP Workgroup Clin J Am Soc Nephrol, 2015.PMID 25583292
- [19]Spencer BWJ, Gergel T, Hotopf M, et al. Unwell in hospital but not incapable: cross-sectional study on the dissociation of decision-making capacity for treatment and research in in-patients with schizophrenia and related psychoses. Br J Psychiatry, 2018.PMID 29909778
- [20]Huf G, Coutinho ES, Adams CE, et al. Physical restraints versus seclusion room for management of people with acute aggression or agitation due to psychotic illness Psychol Med, 2012.PMID 22405443