Psych · Emergency psychiatry — self-harm and crisis
Self-harm and crisis intervention
Also known as Deliberate self-harm · Non-suicidal self-injury · NSSI · Self-injury · Crisis intervention psychiatry · Psychosocial assessment after self-harm · Safety planning self-harm · Hospital-treated self-harm
Exam-exhaustive fellowship reference on self-harm presentations and crisis response — NSSI vs suicide attempt on the intent continuum; epidemiology and repetition/suicide risk after hospital-treated self-harm; affect-regulation functions; NICE-style medical-then-psychosocial assessment; Stanley-Brown safety planning; brief contact and psychological interventions; disposition; youth vs adult; cultural safety and non-stigmatising language. Distinct from suicide-risk-assessment (focus here is self-harm care pathway). FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
12 MCQs with explanations
Target exams
Red flags
Overview and definition
Self-harm and crisis intervention is a core emergency psychiatry skillset: recognising presentations of intentional self-injury or self-poisoning, clarifying intent on a continuum, treating medical need first, completing a structured psychosocial assessment, and implementing crisis and aftercare interventions that reduce repetition and suicide risk.[1][11]
This topic is related to but distinct from suicide risk assessment. Here the centre of gravity is the self-harm presentation and care pathway — classification (NSSI vs attempt), hospital aftercare evidence, NICE-style process standards, brief interventions, and youth vs adult differences — not a full deep-dive on ideation-to-action models or anti-suicide pharmacology (those live primarily in the suicide-risk-assessment topic).[1][7]
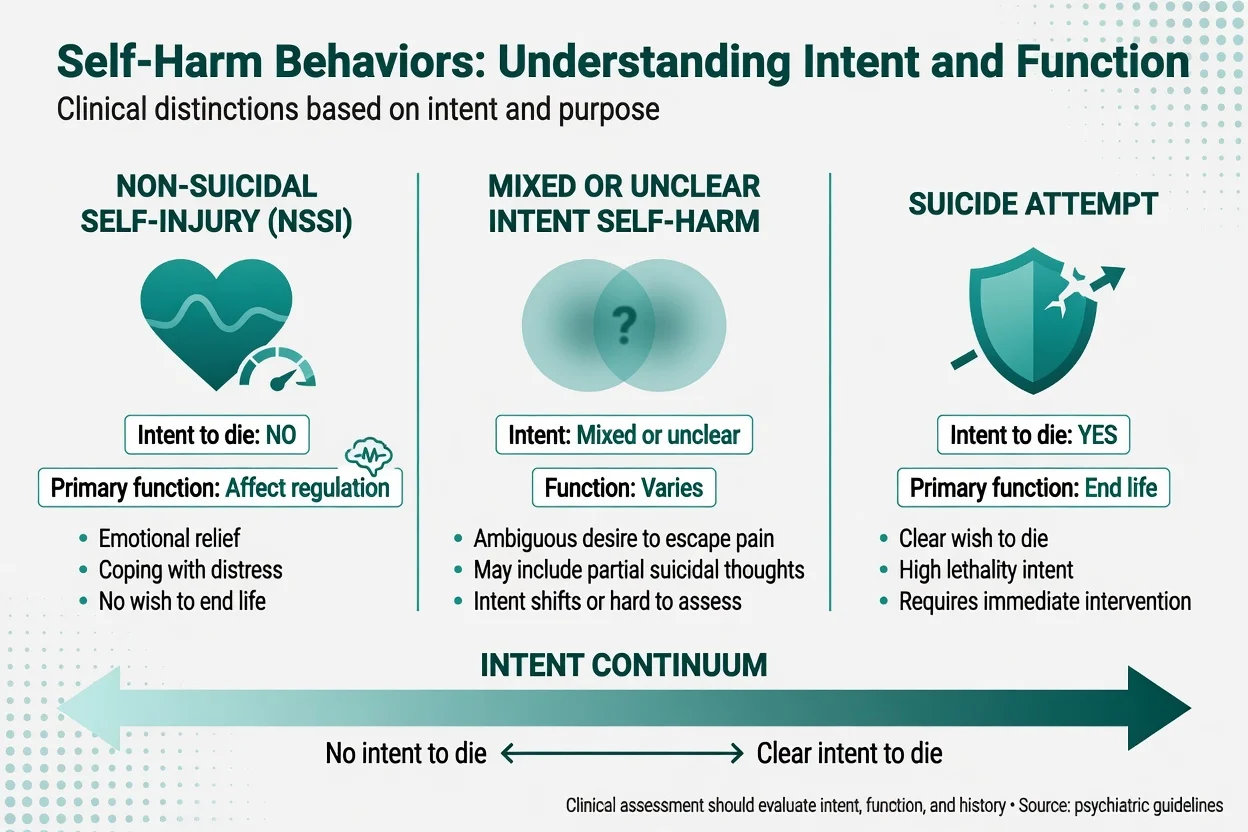
Operational definitions examiners expect (service definitions of self-harm span intentional self-poisoning or self-injury irrespective of suicidal intent; NSSI is self-injury without intent to die; suicide attempt includes at least some intent to die; mixed intent is common and should be documented as such; crisis intervention covers immediate safety through booked follow-up).[1][4][21]
| Term | Working meaning |
|---|---|
| Self-harm (service/research sense) | Intentional self-poisoning or self-injury irrespective of suicidal intent (UK multicentre and NICE-style usage) |
| NSSI | Self-injury without intent to die; often affect regulation, self-punishment, or interpersonal functions |
| Suicide attempt | Self-injurious behaviour with at least some intent to die |
| Mixed / unclear intent | Elements of both; ambivalence common — document both poles |
| Crisis intervention | Immediate safety, engagement, formulation, safety plan, disposition, and rapid follow-up |
Language is clinical and ethical: prefer self-harm, suicide attempt, died by suicide, and NSSI. Avoid pejorative labels (attention-seeking, manipulative, committed suicide). Asking about self-harm and suicide does not implant the behaviour; silence and stigma do harm engagement.[1]
Classification — intent continuum
NSSI vs suicide attempt (exam discriminator)
NSSI is typically used to reduce aversive affect, generate feeling when numb, self-punish, or influence a relationship context — not to die. Suicide attempts include at least partial intent to die; expected lethality and planning vary. People can move between categories over time; chronic NSSI elevates lifetime suicide attempt risk and must not be dismissed as trivial.[3][4][23]
DSM-5-TR places NSSI as a condition for further study with research criteria emphasising intentional self-injury on multiple days, psychological precipitants, and exclusion of socially sanctioned practices. ICD-11 and service data often code intentional self-harm behaviourally. Fellowship answers state the divergence rather than forcing one taxonomy onto every presentation.[1][2]
- No intent to die
- Affect regulation common
- Often repeated pattern
- Still needs full assessment
- May coexist with SI
- Ambivalence about dying
- Partial suicidal thoughts
- Hard to rate at first interview
- Document both poles
- Treat highest credible risk
- Some intent to die
- May be impulsive or planned
- Lethality expectation matters
- Peak near-term risk window
- Safety plan + disposition
Epidemiology and risk factors
Nonclinical meta-analytic work shows NSSI is common in community samples, especially adolescents and young adults; population surveys document substantial non-suicidal self-harm with incomplete service contact.[2][5]
Hospital-treated self-harm is a major liaison psychiatry workload. After an episode, non-fatal repetition is common, and suicide risk is elevated for years — not only in the first week. Multicentre English data link self-harm presentations to subsequent suicide; child and adolescent cohorts show important mortality risk after non-fatal self-harm even though absolute rates differ from adults.[6][7][8][9]
Risk factors for NSSI (Fox meta-analysis) include prior NSSI, hopelessness, depression, cluster B traits, affect dysregulation, and trauma-related factors. Markers linked to suicide after self-harm in multicentre work include older age, male sex (for death by suicide in many settings), psychiatric disorder, prior attempts, and method/clinical severity markers — always integrated in formulation, not used as a score that replaces judgement.[3][7][8][22]
Cross-national data on suicidal ideation, plans, and attempts remind examiners that base rates are high enough that every psychiatrist will manage self-harm repeatedly, yet most people with ideation never die by suicide — prediction of individual death remains weak.[24][22]
Pathophysiology and functions
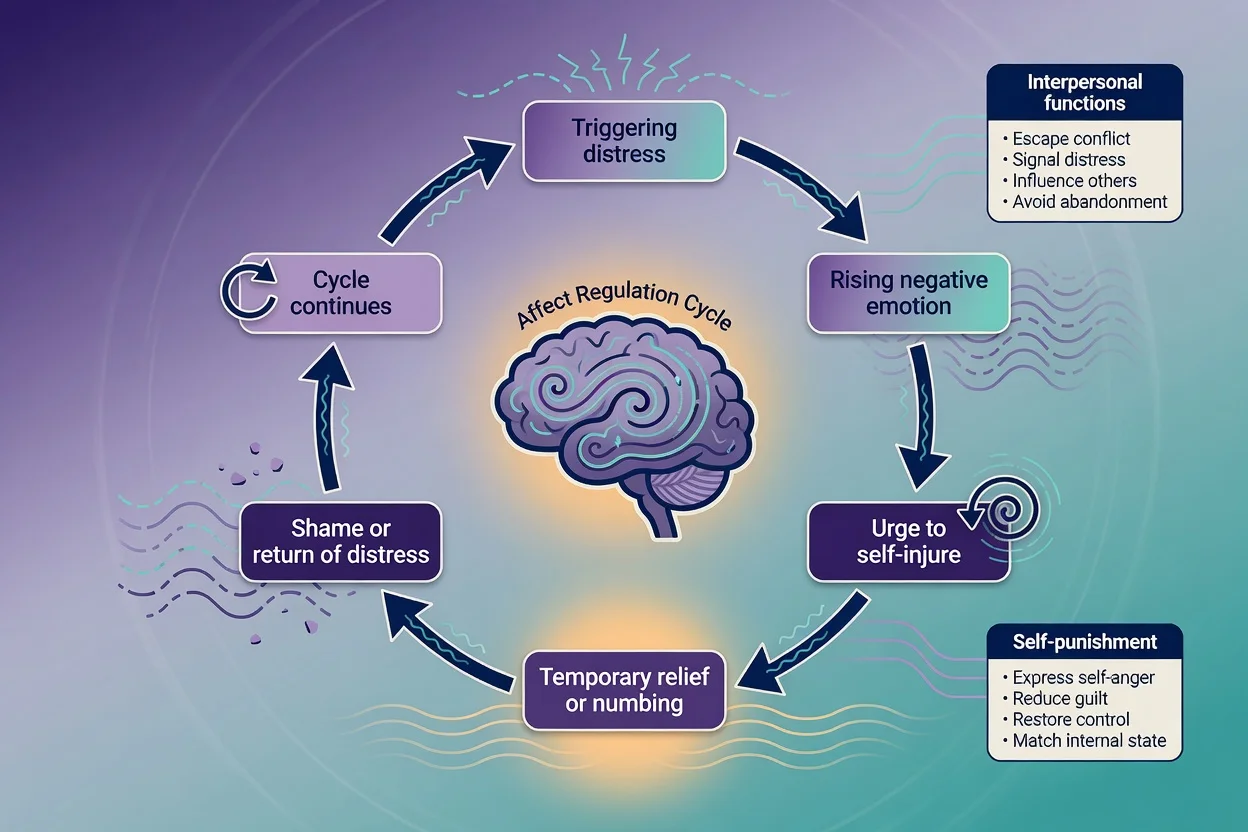
The dominant psychological model for NSSI is affect regulation: aversive emotion rises, urge intensifies, the act produces temporary relief or feeling generation, then shame and return of distress sustain the cycle.[4]
Klonsky's evidence review groups functions as intrapersonal (affect regulation, anti-dissociation, anti-suicide as a stopgap, self-punishment) and interpersonal (help-seeking, interpersonal influence, peer bonding). Naming functions is not moralising — it identifies targets for DBT skills, emotion regulation work, and safety planning for urges as well as suicidal crises.[4]
Where suicidal intent is present, stress-diathesis and ideation-to-action frameworks apply (see suicide-risk-assessment topic). Substance intoxication increases impulsivity and can convert chronic NSSI or passive ideation into more dangerous acts in a single night.[1]
Clinical presentation
Presentations include ED after self-poisoning or self-injury, medical ward liaison, crisis team community visits, CAMHS crisis, custody healthcare, and outpatient disclosure of ongoing NSSI.[11]
MSE themes: shame, minimisation after survival, relief versus disappointment, intoxication, dissociation after NSSI, hopelessness, and fluctuating intent within one interview. Atypical patterns examiners probe: older adult high-lethality acts framed as accidents; youth impulsive interpersonal-crisis NSSI; cultural idioms; chronic daily NSSI in personality pathology with acute escalation.[1][9]
Differential diagnosis
Discriminators matter more than lists. NSSI vs suicide attempt vs mixed intent — ask expected outcome and wish to die; do not infer intent from method alone.[21][23] Body-focused repetitive behaviours (skin picking) and self-injury in intellectual disability — different functional analysis (sensory, pain, environment).[1] Factitious injury — rare first hypothesis; requires careful collateral and pattern review.[1] Organic drivers of impulsivity or despair: intoxication/withdrawal, delirium, severe pain, steroid or other medication effects, akathisia from antipsychotics or antidepressants.[1] Primary mood, psychosis, PTSD, eating disorder, personality disorder as treatable drivers of the behaviour, not alternative excuses to skip risk work.[3][19] Avoid pejorative "manipulative" as a default formulation — it shuts down alliance and fails CASC communication standards.[1]
Clinical and bedside assessment
NICE-style process principles (exam gold)
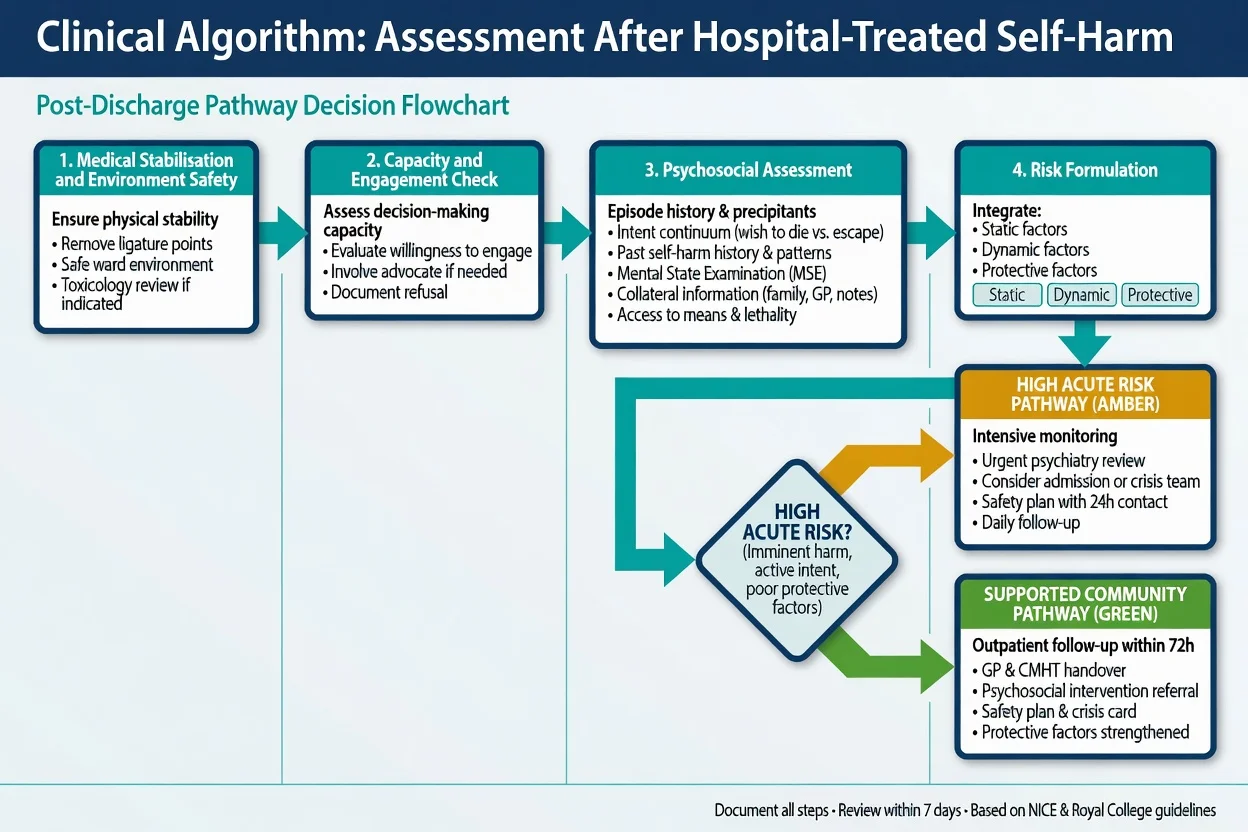
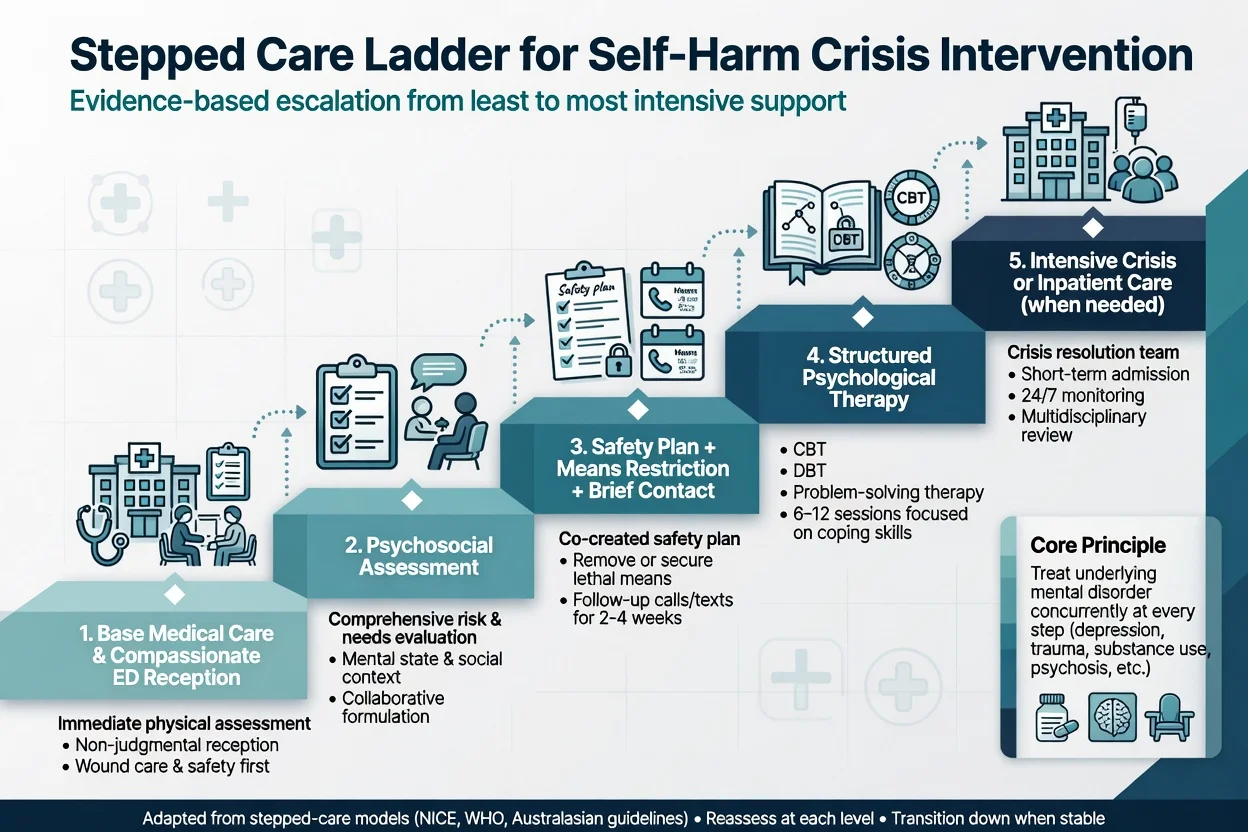
NICE-style process standards for hospital-treated self-harm include: (1) compassion and non-stigmatising care from first contact; (2) medical assessment and treatment first when injury or poisoning requires it; (3) offer psychosocial assessment to everyone presenting with self-harm — not only those labelled high risk; (4) assess needs, risks, and social context and involve family/carers when safe and consented; (5) provide information, safety planning, and aftercare with booked follow-up. These principles align with observational evidence that psychosocial assessment and higher-quality hospital management associate with better process outcomes and, in some analyses, lower subsequent mortality or repetition risk — assessment is an intervention, not paperwork.[10][11][12]
Structured episode history
Structured episode history covers precipitants (interpersonal, trauma reminders, substances, command voices, academic/work stress); intent continuum at the time and now with expectation of death and planning versus impulsivity; alcohol and other substances; past self-harm chronology and functions of NSSI; means access at home (medications, firearms where relevant — document clinically necessary detail without graphic method coaching); protective factors and reasons for living; full MSE with quoted suicidal or self-harm content; capacity, safeguarding (children, vulnerable adults), cultural safety, and interpreter needs; and collateral from family, school, GP, and prior notes (document refusals). C-SSRS concepts can structure ideation severity and behaviour enquiry; they do not replace formulation or guarantee prediction.[21][22]
Investigations
Investigations follow the medical presentation: observations, ECG when cardiotoxic overdose is possible, paracetamol and salicylate levels as indicated by history and local toxicology protocols, metabolic bloods, pregnancy test when relevant. Toxicology screens have false negatives and do not replace history.[1]
Organic red flags (fever, fluctuating consciousness, focal neurology, new severe headache) trigger broader medical work-up. Psychometrics (depression scales, NSSI functional checklists) are adjuncts — not discharge tickets.[22]
Management — immediate (resuscitation / crisis)
Immediate priorities: ABC and medical care for overdose or injury; environment safety with removal of accessible means and proportionate observation; treat pain, withdrawal, severe agitation, and akathisia; engage with calm, validating, non-stigmatising language in a private space when safe; do not use no-suicide contracts as the safety strategy — they lack evidence and create false reassurance; if risk is high and capacity is lacking for necessary care, use least restrictive legal pathways under jurisdiction-specific mental health law (name the principle; do not invent section numbers across countries).[1][13]
Management — definitive and stepwise
Safety planning (Stanley-Brown)
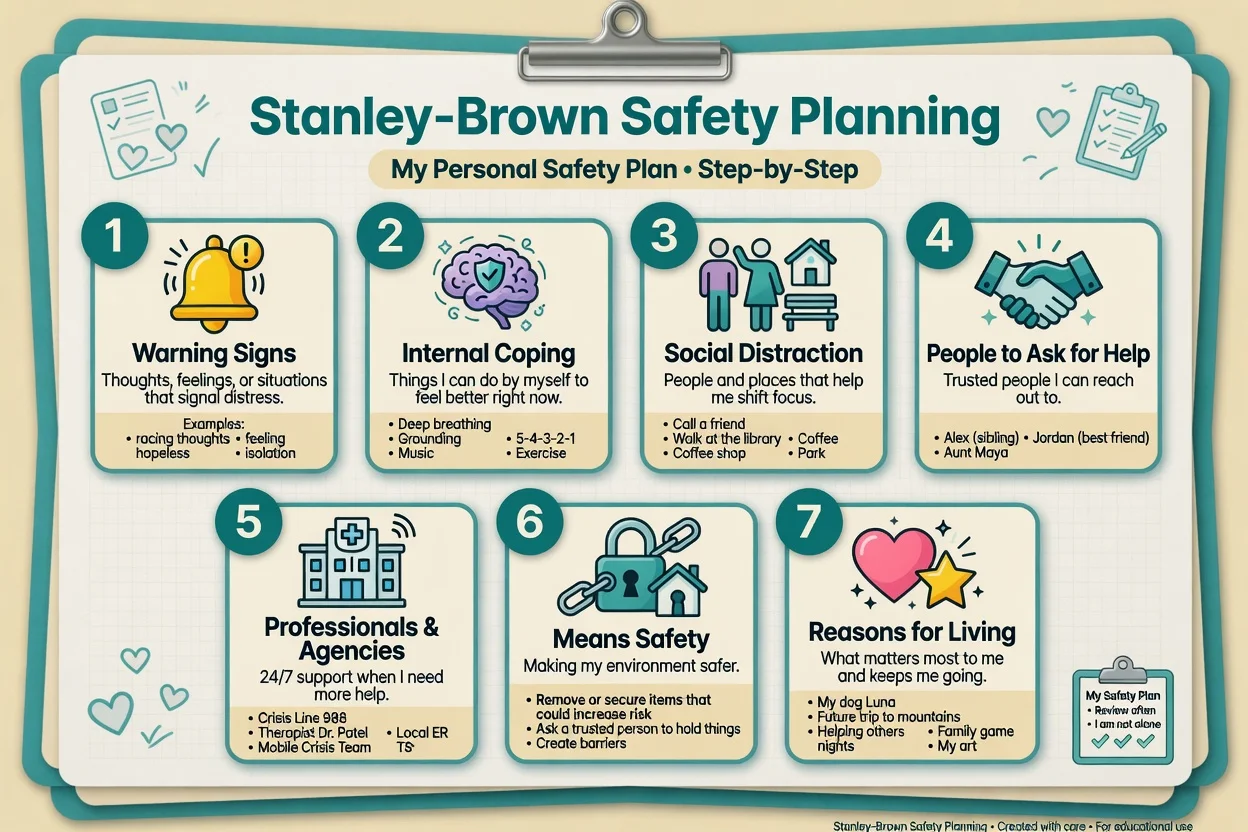
The Safety Planning Intervention with structured follow-up reduced suicidal behaviour versus usual ED care in a large RCT of suicidal ED patients — examiners expect the seven collaborative elements, written ownership by the patient, and concrete local crisis numbers (not vague "call someone").[13]
For NSSI-dominant presentations, add urge-surfing and function-matched skills (e.g. distress tolerance replacing affect-regulation cutting) while still assessing suicidal intent each contact.[4][19]
Brief contact interventions
- WHO Brief Intervention and Contact (BIC) after suicide attempts reduced subsequent suicide deaths in a multicentre RCT across five countries — brief education plus systematic contacts.[14]
- Postcard interventions (Carter Postcards from the EDge) reduced repetition of hospital-treated self-poisoning in an Australian RCT; effects are modest and implementation varies, but the principle of planned, non-demanding contact remains examinable.[15]
Structured psychological therapies
Cochrane reviews of psychosocial interventions for self-harm in adults and in children/adolescents support selected structured approaches (including CBT-informed therapies, DBT-informed care, problem-solving, and family-inclusive models) with moderate and heterogeneous evidence — not a single universal protocol.[16][17]
Landmark trials examiners name include DBT (Linehan) for recurrent suicidal behaviour and self-harm in borderline personality disorder — reduced suicide attempts versus therapy by experts in a two-year RCT context;[19] cognitive therapy for suicide attempt prevention (Brown et al.) which reduced repeat attempts versus enhanced usual care;[20] and the Ougrin meta-analysis supporting therapeutic interventions for adolescent suicide attempts and self-harm versus control conditions on average, with attention to treatment components and engagement.[18]
Pharmacotherapy is directed at underlying disorders (depression, psychosis, bipolar illness, ADHD as indicated). There is no single "anti-NSSI tablet". Discuss early monitoring when starting antidepressants in youth; do not withhold indicated treatment from fear alone. Lithium and clozapine anti-suicide evidence is covered in depth in the suicide-risk-assessment topic when mood or schizophrenia-spectrum indications apply.[1][16]
Means restriction
Collaborative, respectful restriction of accessible means (excess medication, firearms where relevant, other environmental hazards) is a core crisis intervention — not optional lifestyle advice. Avoid graphic method coaching; document what is clinically necessary.[13][1]
Specific subtypes and scenarios
| Scenario | Emphasis |
|---|---|
| First self-poisoning, ambivalent intent | Medical care; full psychosocial assessment; safety plan; rapid follow-up |
| Chronic NSSI, no current SI | Function analysis; skills pathway (often DBT); still screen SI each time |
| Escalating NSSI with emerging SI | Reformulate; increase intensity; means restriction |
| Adolescent interpersonal crisis | Family/school; safeguarding; CAMHS crisis; Witt/Ougrin evidence base |
| Older adult self-harm | High suicide concern; medical comorbidity; isolation; means |
| Psychosis or severe depression | Treat disorder urgently; observation; legal options if needed |
| Frequent ED attendance, personality pathology | Structured formulation; avoid pejorative framing; DBT pathway; crisis plan shared with ED |
| Cultural minority / Indigenous | Cultural safety, community supports, interpreter, trauma-informed stance |
Complications and pitfalls
- Assuming all self-harm is "low risk" or purely communicative
- Delaying medical treatment for a psych interview
- Omitting psychosocial assessment or documenting only a risk label
- No-suicide contracts; empty discharge plans; no means work
- Scale-only decisions without formulation
- Stigmatising language that blocks disclosure
- Graphic method discussion beyond clinical need
- Ignoring carers, school, or cultural context
- Missing the long tail of suicide risk after hospital-treated self-harm
Prognosis and disposition
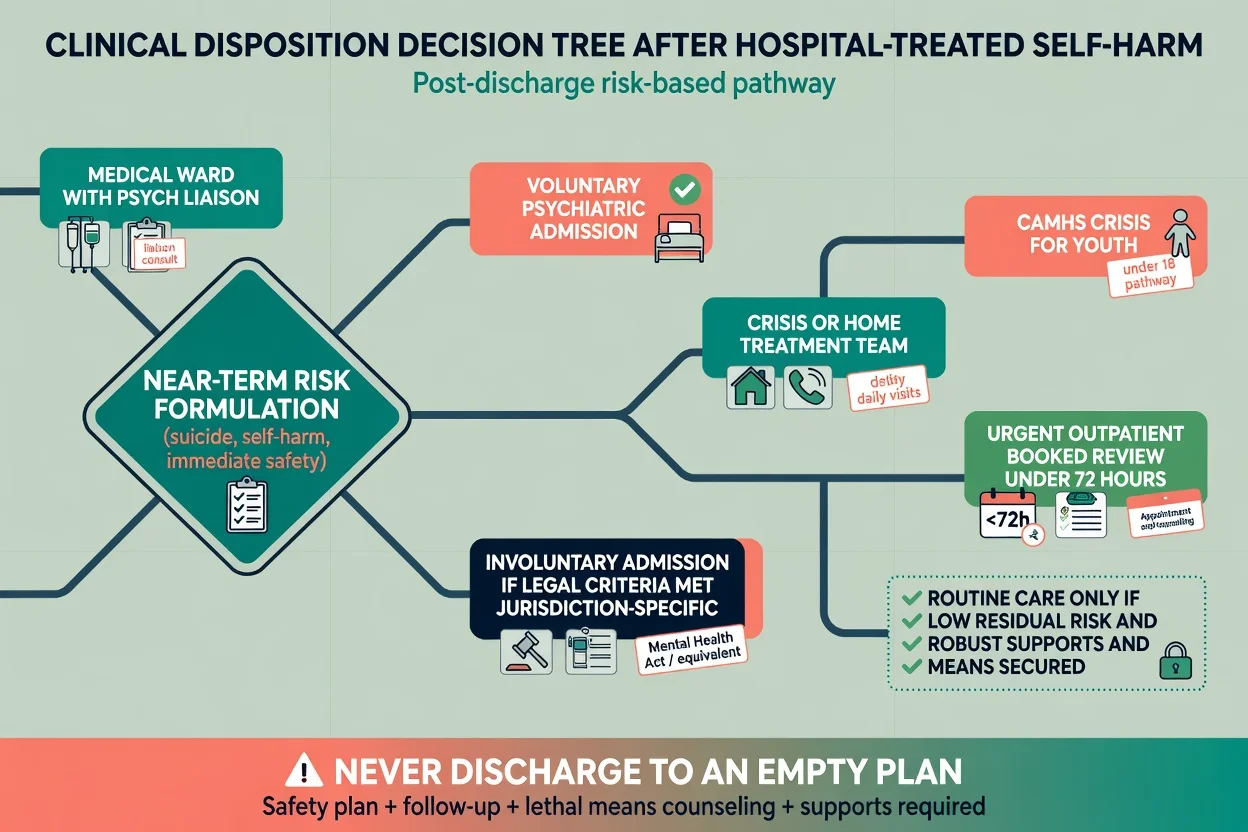
Repetition risk is highest early but suicide risk remains elevated long after the index episode. Disposition options: medical ward with psychiatry liaison; voluntary or involuntary psychiatric admission; crisis/home treatment; CAMHS crisis; urgent outpatient with booked review (often within 24–72 hours when residual risk is present); routine care only when residual risk is low and supports and means control are robust.[6][7][8][13]
Special populations
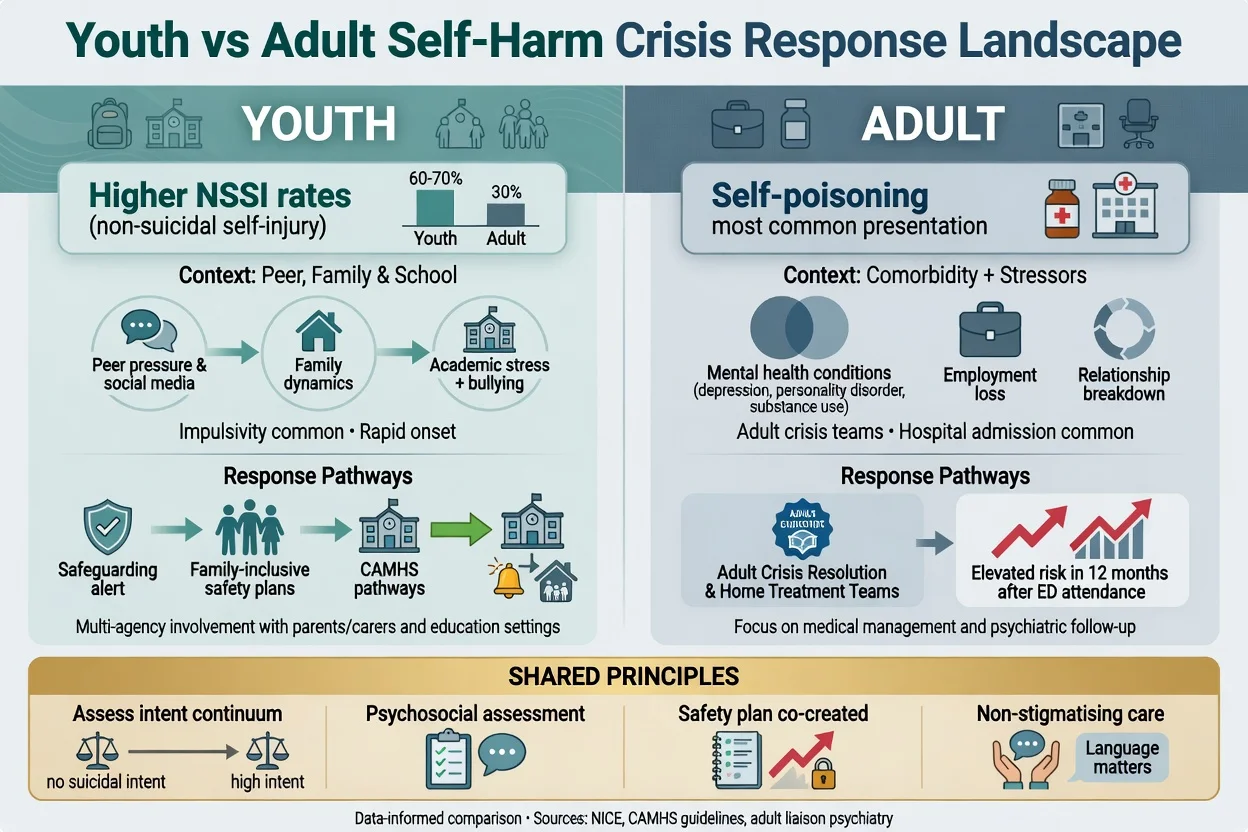
Children and adolescents. Higher community NSSI rates; peer, family, and school drivers; impulsivity; safeguarding duties; family-inclusive safety plans; evidence from Cochrane adolescent reviews and Ougrin meta-analysis favour structured interventions over generic advice alone.[9][17][18]
Older adults. Lower presentation rates in some services but higher lethality concern; loneliness, bereavement, medical illness, and means access dominate formulation.[7][8]
Perinatal. Dual patient consideration; maternity liaison; do not under-treat depression or psychosis from misplaced fear of services.[1]
Intellectual disability. Functional analysis of self-injury; sensory and environmental triggers; adapted communication.[1]
LGBTQ+ youth. Minority stress, bullying, and family rejection as drivers — address social context in the plan.[3]
Indigenous and culturally diverse people. Cultural safety, historical trauma awareness, community supports; avoid stereotyping rates as destiny.[1]
Custody. Environmental means control and observation protocols are part of the intervention.[1]
Evidence, guidelines, and regional differences
ANZ practice emphasises least restrictive care under state/territory mental health legislation, cultural safety (including Aboriginal and Torres Strait Islander and Māori frameworks as locally applicable), means restriction (including firearm safety where relevant), and integration with crisis assessment teams and ED protocols. Carter postcard evidence is Australian-origin.[15]
Controversies. Risk stratification categories have limited individual predictive validity; Large and colleagues argue against over-confidence in low/medium/high labels while still supporting intensive care for those with high dynamic risk. Resource pressure tempts services to skip psychosocial assessment for "low risk" self-harm — observational data and guideline principles push against that shortcut.[22][10]
Exam pearls
SAFETY+
- No-suicide contracts are an exam fail.
- Prior self-harm predicts repetition; hospital-treated self-harm elevates long-term suicide risk.[6][8]
- Name SPI steps, WHO BIC, Carter postcards, Witt Cochrane, Ougrin, Linehan DBT, Brown CT when asked for evidence.[13][14][15][16][18][19][20]
- Youth: carers, school, safeguarding, CAMHS — not adult-only plans copied down.
- CASC: calm pace, direct questions, collaborative plan, no graphic method coaching.
Self-test: 10-second disposition rule
If residual intent is high, means cannot be secured, supports are absent, or medical risk remains — step up (crisis team or admission). If residual risk is lower but not trivial — urgent booked follow-up + safety plan + means work. If truly low residual risk with robust supports — routine pathway still includes clear safety-net advice. Empty plans are never acceptable.[13][10]
References
- [1]Turecki G, Brent DA Suicide and suicidal behaviour Lancet, 2016.PMID 26385066
- [2]Swannell SV, Martin GE, Page A, et al. Prevalence of nonsuicidal self-injury in nonclinical samples: systematic review, meta-analysis and meta-regression Suicide Life Threat Behav, 2014.PMID 24422986
- [3]Fox KR, Franklin JC, Ribeiro JD, et al. Meta-analysis of risk factors for nonsuicidal self-injury Clin Psychol Rev, 2015.PMID 26416295
- [4]Klonsky ED The functions of deliberate self-injury: a review of the evidence Clin Psychol Rev, 2007.PMID 17014942
- [5]McManus S, Gunnell D, Cooper C, et al. Prevalence of non-suicidal self-harm and service contact in England, 2000-14: repeated cross-sectional surveys of the general population Lancet Psychiatry, 2019.PMID 31175059
- [6]Owens D, Horrocks J, House A Fatal and non-fatal repetition of self-harm. Systematic review Br J Psychiatry, 2002.PMID 12204922
- [7]Hawton K, Bergen H, Cooper J, et al. Suicide following self-harm: findings from the Multicentre Study of self-harm in England, 2000-2012 J Affect Disord, 2015.PMID 25617686
- [8]Geulayov G, Casey D, Bale L, et al. Suicide following presentation to hospital for non-fatal self-harm in the Multicentre Study of Self-harm: a long-term follow-up study Lancet Psychiatry, 2019.PMID 31706930
- [9]Hawton K, Bale L, Brand F, et al. Mortality in children and adolescents following presentation to hospital after non-fatal self-harm in the Multicentre Study of Self-harm: a prospective observational cohort study Lancet Child Adolesc Health, 2020.PMID 31926769
- [10]Kapur N, Steeg S, Turnbull P, et al. Hospital management of suicidal behaviour and subsequent mortality: a prospective cohort study Lancet Psychiatry, 2015.PMID 26254717
- [11]Kapur N, Murphy E, Cooper J, et al. Psychosocial assessment following self-harm: results from the multi-centre monitoring of self-harm project J Affect Disord, 2008.PMID 17761308
- [12]Steeg S, Emsley R, Carr M, et al. Routine hospital management of self-harm and risk of further self-harm: propensity score analysis using record-based cohort data Psychol Med, 2018.PMID 28637535
- [13]Stanley B, Brown GK, Brenner LA, et al. Comparison of the Safety Planning Intervention With Follow-up vs Usual Care of Suicidal Patients Treated in the Emergency Department JAMA Psychiatry, 2018.PMID 29998307
- [14]Fleischmann A, Bertolote JM, Wasserman D, et al. Effectiveness of brief intervention and contact for suicide attempters: a randomized controlled trial in five countries Bull World Health Organ, 2008.PMID 18797646
- [15]Carter GL, Clover K, Whyte IM, et al. Postcards from the EDge project: randomised controlled trial of an intervention using postcards to reduce repetition of hospital treated deliberate self poisoning BMJ, 2005.PMID 16183654
- [16]Witt KG, Hetrick SE, Rajaram G, et al. Psychosocial interventions for self-harm in adults Cochrane Database Syst Rev, 2021.PMID 33884617
- [17]Witt KG, Hetrick SE, Rajaram G, et al. Interventions for self-harm in children and adolescents Cochrane Database Syst Rev, 2021.PMID 33677832
- [18]Ougrin D, Tranah T, Stahl D, et al. Therapeutic interventions for suicide attempts and self-harm in adolescents: systematic review and meta-analysis J Am Acad Child Adolesc Psychiatry, 2015.PMID 25617250
- [19]Linehan MM, Comtois KA, Murray AM, et al. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder Arch Gen Psychiatry, 2006.PMID 16818865
- [20]Brown GK, Ten Have T, Henriques GR, et al. Cognitive therapy for the prevention of suicide attempts: a randomized controlled trial JAMA, 2005.PMID 16077050
- [21]Posner K, Brown GK, Stanley B, et al. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults Am J Psychiatry, 2011.PMID 22193671
- [22]Large MM, Ryan CJ, Carter G, et al. Can we usefully stratify patients according to suicide risk? BMJ, 2017.PMID 29042363
- [23]Muehlenkamp JJ, Ertelt TW, Miller AL, et al. Borderline personality symptoms differentiate non-suicidal and suicidal self-injury in ethnically diverse adolescent outpatients J Child Psychol Psychiatry, 2011.PMID 20735511
- [24]Nock MK, Borges G, Bromet EJ, et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts Br J Psychiatry, 2008.PMID 18245022