Psych · Emergency psychiatry
Serotonin syndrome
Also known as Serotonin toxicity · Serotonergic syndrome · 5-HT syndrome · Hunter criteria serotonin · Sternbach serotonin syndrome
Exam-exhaustive fellowship topic on serotonin toxicity — Hunter criteria (preferred) versus historical Sternbach, toxidrome with neuromuscular hyperreactivity, high-risk combinations (MAOI+SSRI, linezolid, methylene blue, tramadol, pethidine), severity-based management (stop agents, benzodiazepines, cyproheptadine doses, cooling, ICU paralysis), differential from NMS, complications and special populations. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Serotonin syndrome (better framed by toxicologists as serotonin toxicity) is a preventable medical emergency that sits at the junction of psychiatry, emergency medicine, anaesthetics, and infectious diseases. Fellowship examiners test three things relentlessly: accurate criteria (Hunter over Sternbach), recognition of the neuromuscular signature, and a named management ladder including high-risk drug traps such as MAOI combinations, linezolid, and methylene blue.[1][3][4][12]
Overview and definition
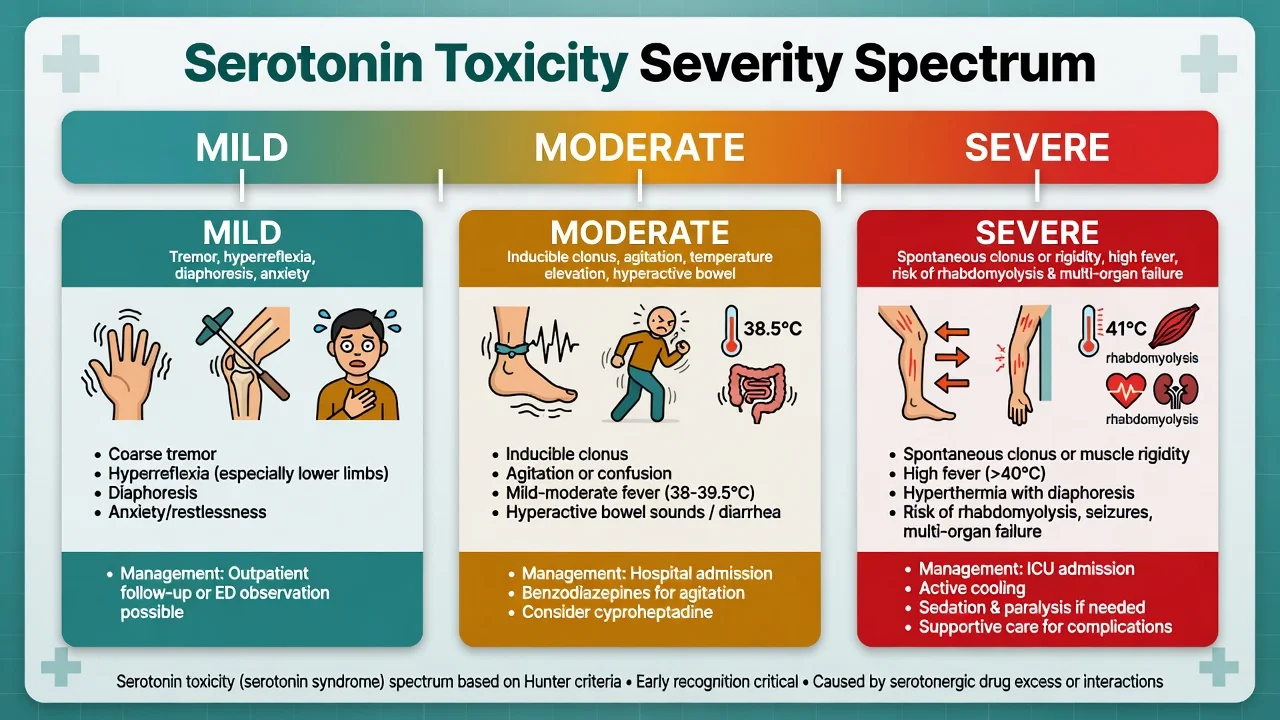
Serotonin toxicity is a concentration-dependent continuum of clinical effects from excess serotonergic neurotransmission, usually after therapeutic combinations, dose escalation, or overdose — not a single all-or-none disease entity.[4][5][14] Mild cases show tremor and hyperreflexia; severe cases produce rigidity, marked hyperthermia, and multi-organ failure risk.[3][7]
It is not a DSM-5-TR or ICD-11 primary psychiatric diagnosis. It is an iatrogenic or toxicological syndrome that psychiatry must own because psychiatrists prescribe most of the culprits and will be the ones asked to differentiate it from NMS, akathisia, and agitated delirium at 2 a.m.[7][8]
Classification — Hunter preferred; Sternbach historical
Hunter Serotonin Toxicity Criteria (reproduce accurately)
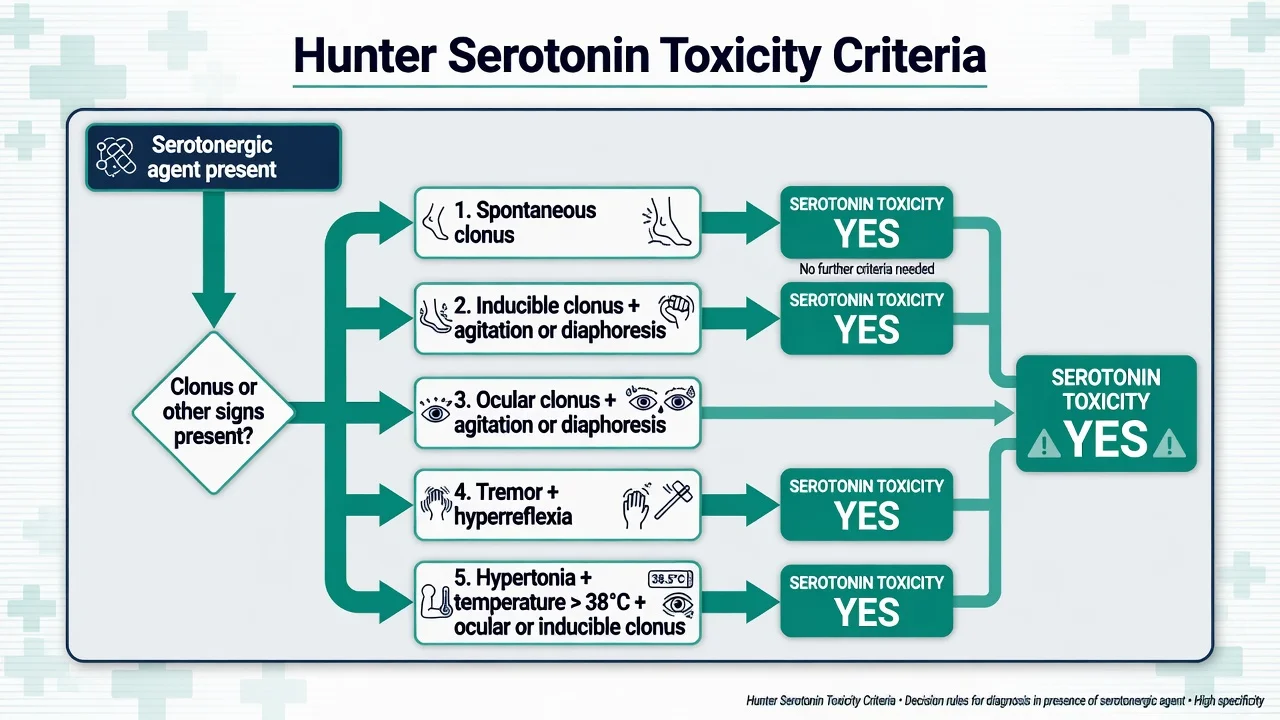
In the presence of a serotonergic agent, serotonin toxicity is present if any of the following is true:[1][4]
- Spontaneous clonus
- Inducible clonus plus agitation or diaphoresis
- Ocular clonus plus agitation or diaphoresis
- Tremor plus hyperreflexia
- Hypertonia plus temperature greater than 38 °C plus ocular clonus or inducible clonus
Hunter rules were derived from a large toxicology dataset and are more specific and simpler than Sternbach for clinical decision-making. They privilege clonus and hyperreflexia — the neuromuscular signature of excess serotonin.[1][5][14]
Sternbach criteria (1991) — know, then prefer Hunter
Sternbach required recent addition or increase of a serotonergic agent, at least three of ten clinical features (mental status changes, agitation, myoclonus, hyperreflexia, diaphoresis, shivering, tremor, diarrhoea, incoordination, fever), exclusion of other aetiologies, and no recent neuroleptic introduction or increase.[2] Limitations: less specific, includes non-discriminating features, and can misclassify mixed toxidromes. Still appears in older stems and some guidelines — cite it as historical and state why Hunter is preferred.[1][2][14]
Radomski revised criteria
Radomski and colleagues proposed a revised structure with major/minor features; useful historically but not the modern default in clinical toxicology practice compared with Hunter.[6][14]
Severity spectrum
| Severity | Typical features | Default intensity of care |
|---|---|---|
| Mild | Tremor, hyperreflexia, diaphoresis, anxiety, mydriasis | Stop agent(s), observe, benzodiazepine if agitated |
| Moderate | Inducible clonus, agitation, rising temperature, hyperactive bowel | Admit, benzos, cooling, consider cyproheptadine |
| Severe | Spontaneous clonus or marked rigidity, high fever, instability | ICU, aggressive cooling, consider paralysis |
Epidemiology and risk context
True population incidence is under-estimated because mild cases are missed and labels are inconsistent.[7][9] Risk clusters where two or more serotonergic mechanisms stack — especially MAO inhibition plus reuptake inhibition.[3][9][20]
SSRI overdose series show that pure SSRI toxicity is often milder than combination or MAOI-related toxicity, but agent-specific differences matter (for example relative seizure and cardiotoxicity differences across SSRIs in overdose cohorts).[13][17] Mortality is uncommon with early recognition and drug cessation, but severe hyperthermic cases can progress to rhabdomyolysis, renal failure, DIC, and death.[3][7][12]
Pathophysiology
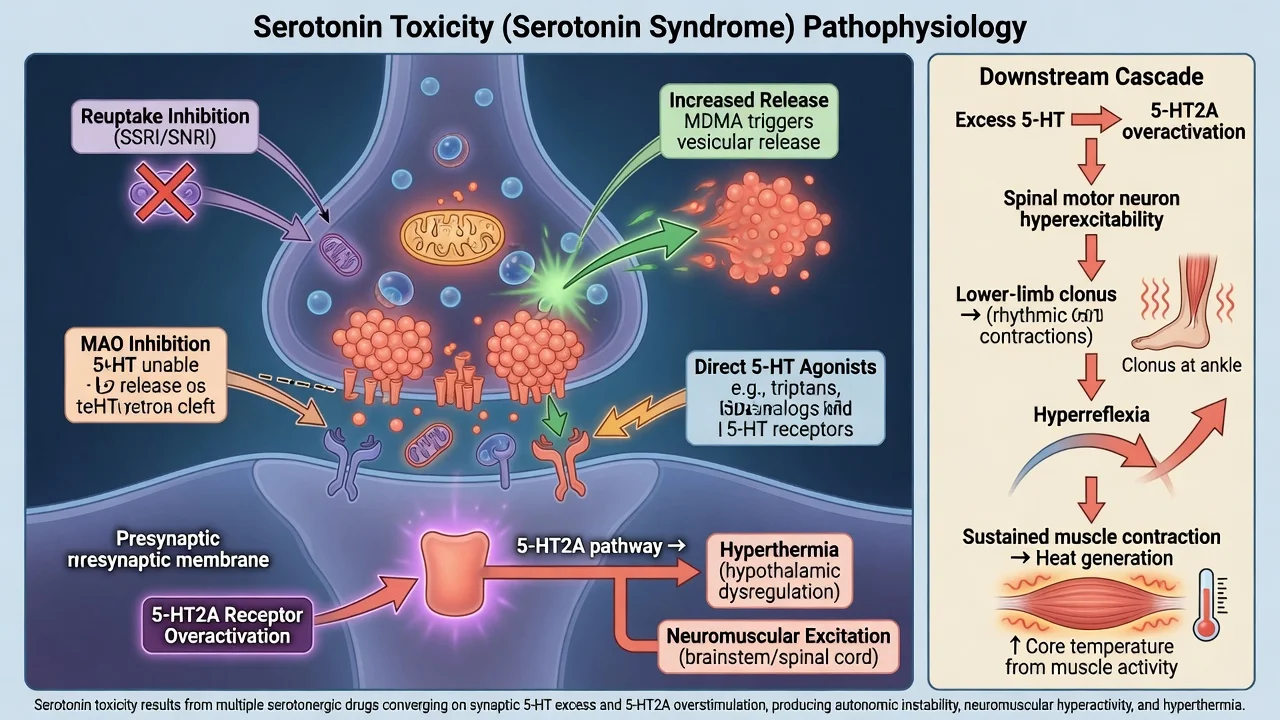
Excess 5-HT acts at central and peripheral synapses. Mechanisms include:[5][9]
- Reuptake inhibition — SSRIs, SNRIs, many TCAs, tramadol (partial), some opioids
- MAO inhibition — irreversible non-selective MAOIs, linezolid (weak MAOI), methylene blue (potent MAO-A inhibition in relevant doses)
- Increased release — MDMA, some amphetamines
- Direct agonism — some triptans and other agonists (absolute clinical risk of severe toxicity when combined with SRIs is debated; see evidence section)
- Reduced metabolism / pharmacokinetic interactions that raise levels of serotonergic drugs
Neuromuscular hyperreactivity (hyperreflexia, inducible/spontaneous/ocular clonus — often lower-limb predominant) is the clinical signature that separates serotonergic toxicity from many mimics.[1][4][5] Hyperthermia is driven substantially by muscle activity plus central effects; that is why cooling and stopping muscle hyperactivity matter more than antipyretics alone.[3][5][12]
Animal data show that potent 5-HT2A antagonists prevent hyperthermia in 5-HT syndrome models — the mechanistic backbone for cyproheptadine use.[18]
Clinical presentation
The toxidrome triad
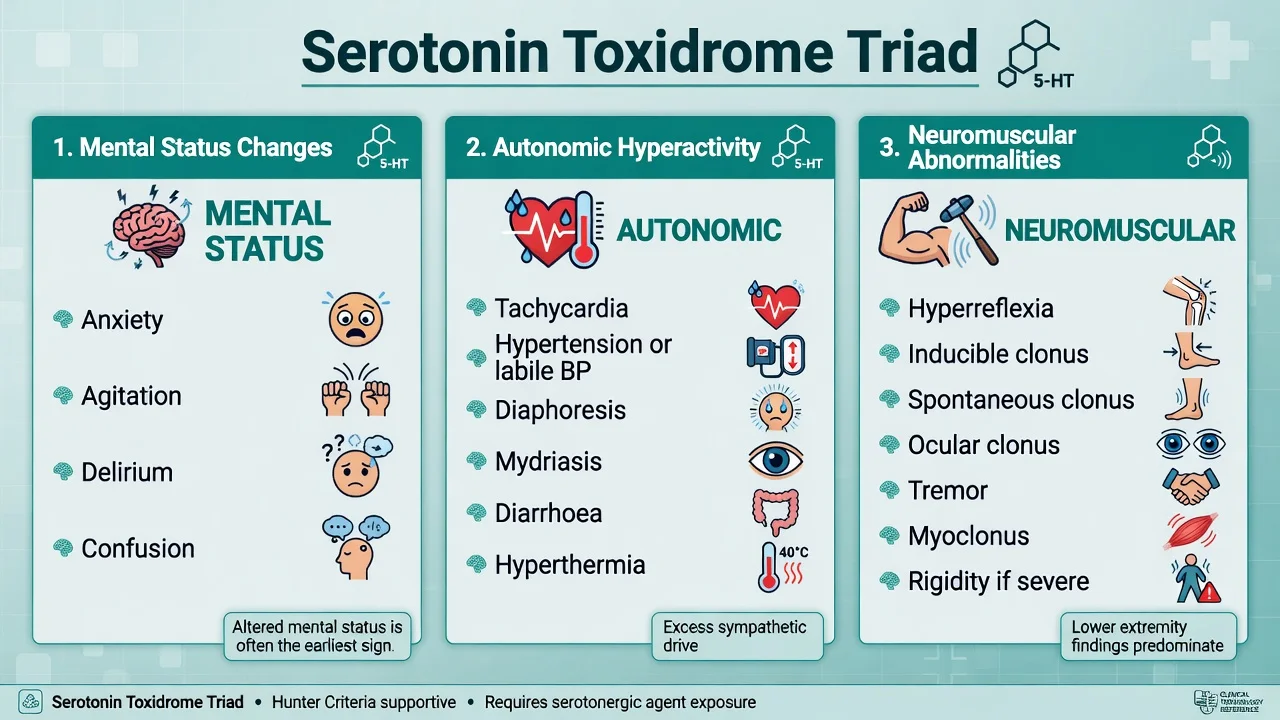
1. Altered mental status — anxiety, restlessness, agitation, delirium; rarely a pure psychiatric presentation without somatic signs if you examine carefully.[3][7]
2. Autonomic hyperactivity — tachycardia, hypertension or blood-pressure lability, diaphoresis, mydriasis, hyperactive bowel sounds/diarrhoea, hyperthermia.[3][7]
3. Neuromuscular abnormalities — hyperreflexia, clonus (inducible, spontaneous, ocular), tremor, myoclonus; rigidity appears as severity escalates and can obscure hyperreflexia if profound.[1][3][4]
Tempo
Onset is typically within hours of a dose change, new combination, or overdose (often within 24 hours) — a key discriminator from classic NMS, which more often evolves over days.[3][8]
Atypical and trap presentations
- Post-operative patient after methylene blue for parathyroid surgery or vasoplegia while still on an antidepressant.[10]
- Medical patient started on linezolid while continuing an SSRI/SNRI.[19]
- Pain regimen adding tramadol or pethidine to a serotonergic antidepressant.[11][20]
- Recreational MDMA with or without prescribed serotonergics.[3][9]
- Older adult with polypharmacy and fluctuating attention — do not call it “just delirium” without a drug review and neurological exam for clonus.[7]
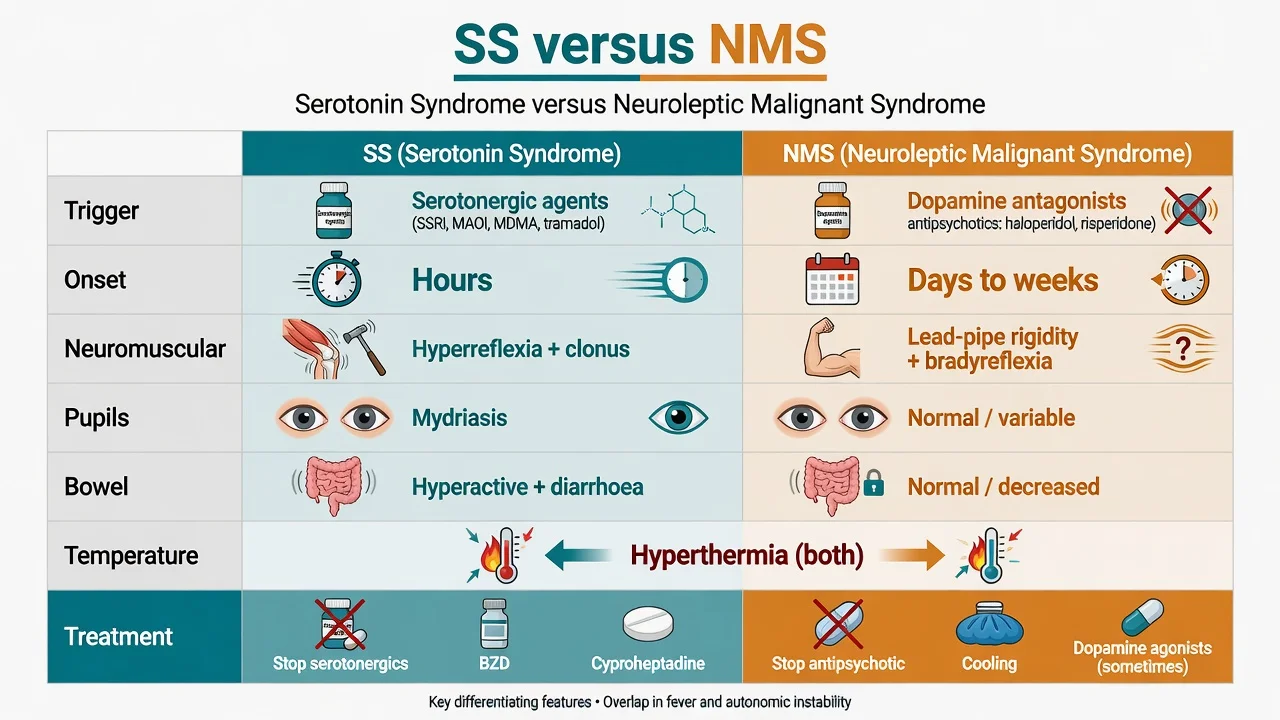
Differential diagnosis
- Serotonergic drug exposure
- Onset hours
- Hyperreflexia and clonus
- Hyperactive bowel / diarrhoea common
- Mydriasis often
- Stop serotonergics; BZD; cyproheptadine
- Dopamine antagonist or agonist withdrawal
- Onset days to weeks
- Lead-pipe rigidity; bradyreflexia
- Bowel often normal or reduced
- Stop antipsychotic; cool; supportive; consider dopaminergic strategies carefully
- Dry skin and mucosa
- Urinary retention, decreased bowel sounds
- Delirium, mydriasis
- Less true inducible clonus
- Supportive care; physostigmine only in selected settings
Expanded can't-miss list
- Sympathomimetic toxicity — hyperadrenergic state; less consistent lower-limb clonus signature.[3]
- Malignant hyperthermia — anaesthetic trigger history.[3]
- Thyroid storm, heat stroke, sepsis, meningoencephalitis — fever work-up when infectious features dominate.[7]
- Alcohol or sedative-hypnotic withdrawal — tremor and autonomic surge without serotonergic clonus package.[3]
- Excited catatonia / severe behavioural disturbance — may coexist with medical toxicity; treat physiology first.[8]
- Akathisia — inner restlessness after antipsychotics without the autonomic-clonus package; wrong move is more D2 blockade.[8]
Clinical and bedside assessment
- ABCDE, continuous monitoring, core temperature, glucose, SpO2.
- Full drug history including OTC cough mixtures (dextromethorphan), tramadol/pethidine/fentanyl, St John's wort, recreational drugs, linezolid, methylene blue, triptans, MAOIs (including selegiline/rasagiline context).
- Focused neurological exam: ankle clonus, deep tendon reflexes (compare upper vs lower limbs), ocular clonus, tone, coordination.
- Emergency MSE: agitation versus fluctuating delirium; suicidality if overdose; capacity for treatment decisions.
- Collateral and medication reconciliation from pharmacy/GP records when the patient cannot list agents.
- Legal status if involuntary detention or incapacity for medical treatment is relevant — use jurisdiction-specific Mental Health Act principles without inventing foreign section numbers.[3][4][12]
CLONUS
Investigations
There is no confirmatory serum serotonin assay for diagnosis. Diagnosis is clinical, preferably with Hunter criteria.[1][3][4]
| Priority | Tests | Rationale |
|---|---|---|
| Immediate | Vitals, glucose, ECG | Instability, co-ingestant cardiotoxicity (e.g. citalopram/TCA context) |
| Standard labs | U and E, CK, FBC, LFTs, coagulation, lactate, ABG/VBG | Rhabdomyolysis, organ injury, acidosis |
| OD context | Paracetamol, salicylate, other indicated levels | Concurrent self-poisoning |
| Directed | Pregnancy test, infection work-up, imaging/LP | Alternative diagnoses only when indicated |
Do not delay resuscitation for a urine drug screen. Negative screens do not exclude MDMA or many agents.[3]
Management — resuscitation
Immediate priorities
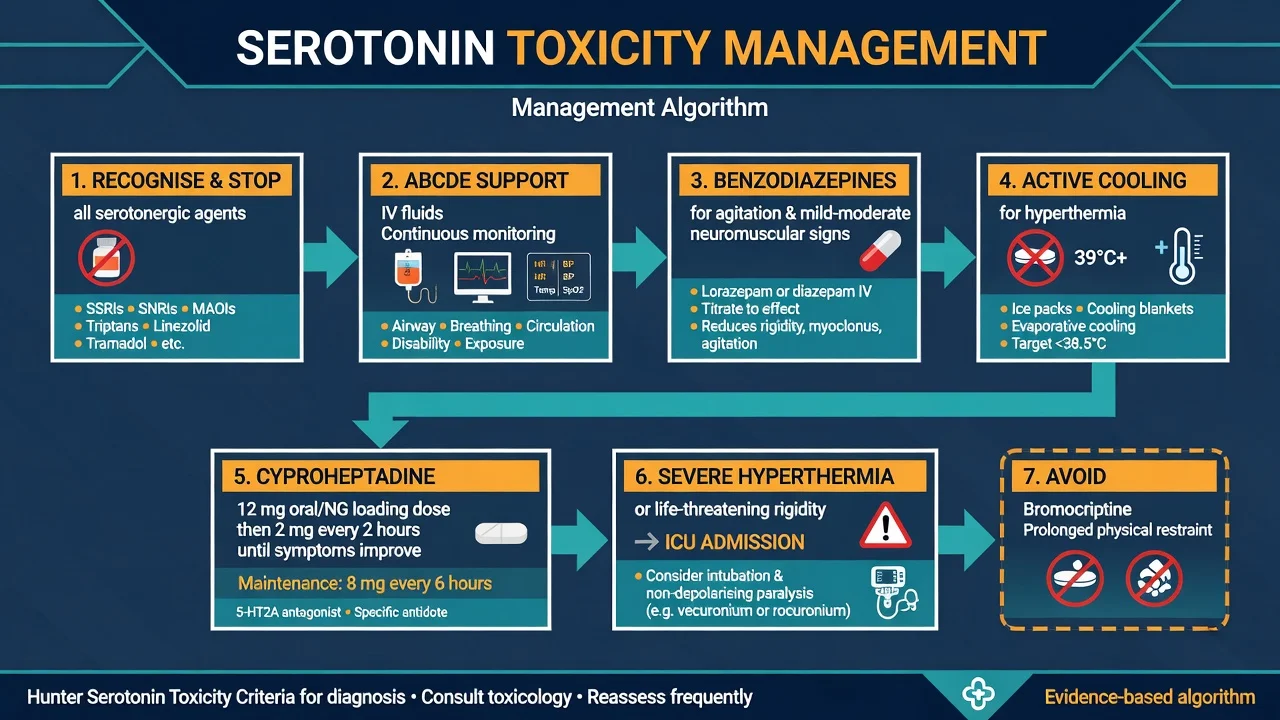
- Stop all serotonergic agents immediately (including accidental ongoing ward doses).[3][4][12]
- Supportive care — airway protection if needed, oxygen as indicated, IV crystalloid for volume losses/diaphoresis, continuous cardiac and temperature monitoring.[3][12]
- Benzodiazepines for agitation and mild-to-moderate neuromuscular hyperactivity — reduce excess muscle activity and distress. Practical adult examples used in clinical reviews: lorazepam 1–2 mg IV/IM (or equivalent oral if mild and cooperative), or diazepam titrated IV in monitored settings; repeat cautiously to effect while protecting airway. Follow local formulary and toxicology advice for cumulative dosing.[3][4][12]
- Active external cooling for hyperthermia (cooling blankets, ice packs to groin/axillae/neck, evaporative cooling). Antipyretics alone do not treat toxidrome-driven hyperthermia.[3][12]
- Avoid prolonged physical restraint — isometric muscle contraction worsens heat generation.[3][7]
Cyproheptadine (5-HT2A antagonist)
Cyproheptadine is the most cited specific pharmacologic adjunct for moderate-to-severe serotonin toxicity when oral/NG route is available. Classic regimen from major clinical reviews:[3][4][7]
- Loading dose: 12 mg oral or via nasogastric tube
- Then 2 mg every 2 hours if symptoms continue
- Maintenance commonly 8 mg every 6 hours once controlled
- Maximum daily exposure often discussed around 32 mg/day in classic sources — confirm local product information
It is not available as a reliable IV product in most hospitals. Observational data support continued clinical use; high-quality RCTs remain limited, so position it as a targeted adjunct after cessation and benzodiazepines, not as a substitute for cooling and ICU care in severe cases.[12][15][18]
Severe hyperthermia and life-threatening rigidity
If temperature is high and rising with severe rigidity or multi-organ threat: ICU, aggressive cooling, and consider intubation with non-depolarising neuromuscular paralysis (for example vecuronium or rocuronium per ICU protocol) to abolish muscle heat generation. Avoid suxamethonium if rhabdomyolysis/hyperkalaemia risk is high.[3][12]
What not to do
- Do not give bromocriptine or amantadine for presumed NMS if the diagnosis is serotonin toxicity — dopaminergic agents can worsen serotonergic states.[3][8]
- Dantrolene is not first-line therapy for serotonin toxicity (its primary exam home is malignant hyperthermia; NMS use is itself nuanced).[3][8]
- Do not restart the culprit serotonergic regimen the next morning out of habit.[4][12]
Management — definitive and stepwise
Severity-matched pathway
| Step | Mild | Moderate | Severe |
|---|---|---|---|
| Cessation | Yes | Yes | Yes |
| Observation | ED/ward short | Admit | ICU |
| Benzodiazepine | As needed | Yes | Yes (while preparing definitive airway plan) |
| Cooling | If febrile | Active | Aggressive |
| Cyproheptadine | Optional/selected | Usually yes | Yes if NG/oral accessible; do not delay ICU measures |
| Paralysis | No | Rare | Consider for refractory hyperthermia |
After the crisis
- Document culprits, onset, criteria used (Hunter), peak temperature, CK, treatments, response.
- Educate patient and carers about combination risks.
- Deprescribe unnecessary serotonergics; when depression/anxiety still needs treatment, plan a safer regimen with washout appropriate to half-life (fluoxetine/norfluoxetine needs longer caution before MAOI exposure).
- Involve clinical toxicology early for severe or unclear cases (ANZ practice strength).[4][12][17]
- Report significant adverse drug reactions through local systems.
Specific subtypes and scenarios
MAOI plus SSRI/SNRI (or other SRI)
The classic catastrophic combination. Irreversible MAO inhibition plus reuptake blockade can produce severe toxicity even at therapeutic doses. Never casually co-prescribe; observe washout rules when switching.[3][9][20]
Opioid serotonergic traps
Pethidine (meperidine), tramadol, and to a variable extent other opioids (including fentanyl in some reports/contexts) can contribute, especially with MAOIs. Gillman emphasises particular danger of MAOI plus pethidine/tramadol/dextromethorphan-type agents.[11][20]
Linezolid
Linezolid has MAOI activity. Post-marketing data associate it with serotonin toxicity when combined with serotonergic antidepressants — screen medication lists before starting, and monitor or hold SRI agents per infectious disease/toxicology guidance when alternatives are limited.[19]
Methylene blue
Methylene blue is a potent MAO-A inhibitor at clinically used IV doses. Systematic review supports a definite causal link with serotonin toxicity when combined with serotonergic psychiatric medicines — flag on the anaesthetic chart before parathyroidectomy or vasoplegic shock treatment.[10]
SSRI overdose
Single-agent SSRI overdose often produces milder serotonergic signs than multi-mechanism combinations, but seizures, QT effects, and agent-specific toxicity still matter. Predictive work continues on who develops clinically important toxicity after SRI overdose.[13][17]
Triptans plus SRI
FDA labelling raised concern about triptan plus SSRI/SNRI combinations. The American Headache Society position paper argued that available evidence did not support prohibiting necessary combinations for most patients and that true serotonin toxicity risk appeared low — know both the regulatory caution and the specialty counter-position for balanced viva answers.[16][9]
Complications and pitfalls
- Hyperthermia, seizures, rhabdomyolysis, acute kidney injury, metabolic acidosis, DIC, ARDS, death in severe untreated cases.[3][7][12]
- Missed diagnosis → continued ward doses of the culprit.
- Mislabelled NMS → wrong pharmacology.
- Over-calling mild jitteriness after a single low-risk drug as full syndrome without Hunter features.
- Under-examining for ocular and ankle clonus.
- Stacking sedatives without airway readiness in severe agitation.
Prognosis and disposition
Most mild-to-moderate cases improve within 24 hours after cessation of short-acting agents, though recovery can be longer with long half-life drugs (fluoxetine/norfluoxetine) or ongoing active metabolites.[3][4][7] Severe cases require ICU and may have prolonged multi-organ recovery.
Disposition thinking: discharge only if mild, clearly improving, safe supports, education given, and no significant CK rise or ongoing hyperthermia. Otherwise observe, admit, or ICU. Arrange psychiatric follow-up for the underlying illness and a redesigned psychotropic plan.[4][12]
Special populations
- Older adults — polypharmacy, delirium overlap, lower reserve for hyperthermia; start low with any sedative and prioritise drug cessation.[7]
- Pregnancy — supportive care first; choose agents with obstetric/toxicology input; fetal monitoring as indicated.[7]
- Paediatric/adolescent — intentional overdose and MDMA contexts; weight-based benzos; early toxicology involvement.[3]
- Parkinson disease on MAO-B inhibitors — still respect serotonergic stacking risks with antidepressants and certain opioids.[9][20]
- Intellectual disability / limited history — examination for clonus still works when history does not.
Evidence, guidelines, and regional differences
Landmark diagnostic contribution: Dunkley et al., Hunter Serotonin Toxicity Criteria (QJM 2003) — preferred modern decision rules.[1] Historical diagnostic frame: Sternbach 1991.[2] Classic clinical synthesis: Boyer and Shannon, NEJM 2005.[3] ANZ practical toxicology: Isbister, Buckley, Whyte (MJA 2007) and ongoing updates including Chiew and Isbister 2025 management review and Chiew and Buckley 2022 critique of criteria shortfalls across related syndromes.[4][12][14]
ANZ clinical toxicology services (Hunter legacy and national networks) strongly influence fellowship-level answers: use Hunter criteria, early toxicology consult for severe cases, and be fluent with methylene blue/linezolid traps in hospital systems. There is no single RANZCP disease-specific serotonin-syndrome guideline that replaces toxicology principles — answer with toxicology evidence plus local hospital protocols.[1][4][12]
Cyproheptadine evidence: strong mechanistic animal support for 5-HT2A blockade preventing hyperthermia, plus clinical use and retrospective series — not a large modern RCT portfolio. State that honestly in viva.[15][18]
Exam pearls
- Recite Hunter five rules without fumbling.[1]
- Lower-limb clonus/hyperreflexia is the gift finding.[1][4]
- Onset hours (SS) versus days–weeks (NMS).[8]
- Name the MAOI + SRI disaster combination and the methylene blue / linezolid traps.[10][19][20]
- Cyproheptadine 12 mg load, then 2 mg q2h, maintenance 8 mg q6h — oral/NG only in most hospitals.[3]
- Never “treat SS as NMS” with bromocriptine.[3][8]
- Endpoint of care is resolution of toxicity and a safer long-term regimen — not deep unconsciousness.[3][12]
High-risk drug combinations (quick map)
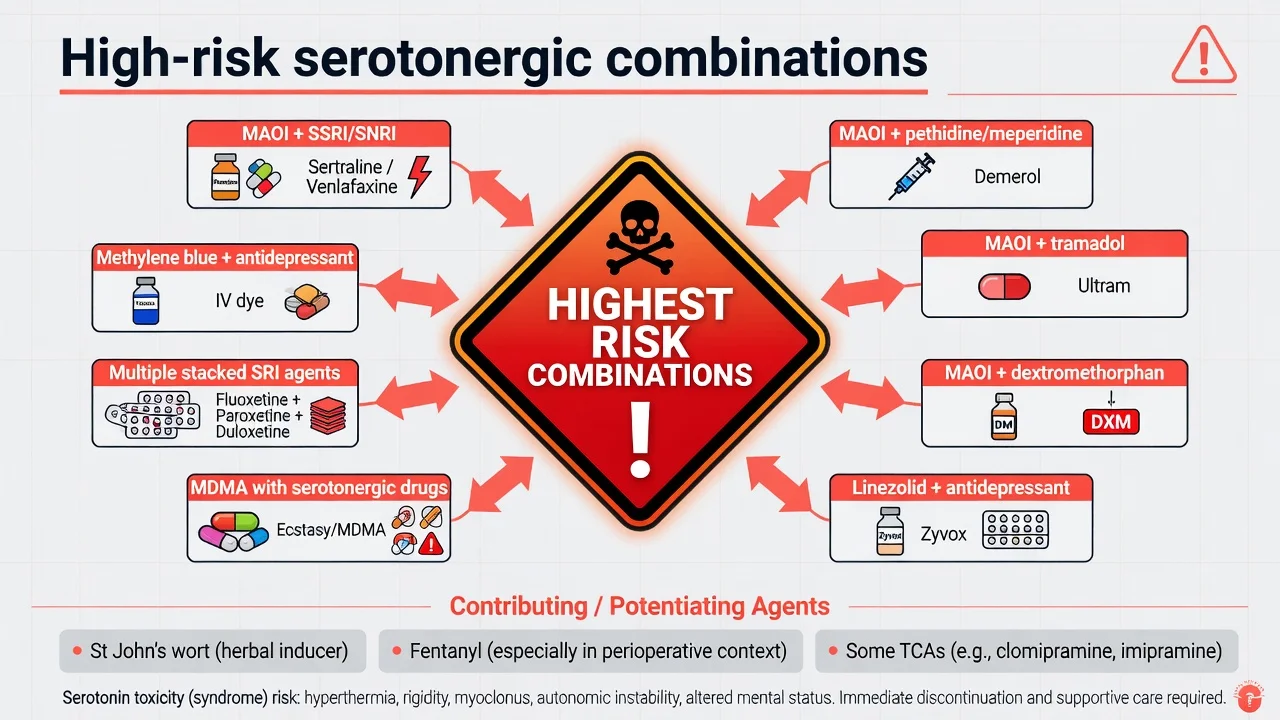
| Combination / context | Why examiners care |
|---|---|
| MAOI + SSRI/SNRI/TCA-SRI | Highest classic risk |
| MAOI + pethidine / tramadol / dextromethorphan | Anaesthetic and pain traps |
| Linezolid + antidepressant | Medical ward antimicrobial trap |
| Methylene blue + antidepressant | Theatre / ICU trap |
| Multiple stacked SRIs or SRI + MDMA | Overdose and recreational |
| Triptan + SRI | Regulatory vs specialty nuance |
Red flags and clinical pearls
[1] [3] [12] [1] [3] [12]Self-test: name the Hunter rules from memory
In the presence of a serotonergic agent: (1) spontaneous clonus; (2) inducible clonus + agitation or diaphoresis; (3) ocular clonus + agitation or diaphoresis; (4) tremor + hyperreflexia; (5) hypertonia + temperature greater than 38 °C + ocular or inducible clonus.[1]
References
- [1]Dunkley EJ, Isbister GK, Sibbritt D, et al. The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity. QJM, 2003.PMID 12925718
- [2]Sternbach H The serotonin syndrome. Am J Psychiatry, 1991.PMID 2035713
- [3]Boyer EW, Shannon M The serotonin syndrome. N Engl J Med, 2005.PMID 15784664
- [4]Isbister GK, Buckley NA, Whyte IM Serotonin toxicity: a practical approach to diagnosis and treatment. Med J Aust, 2007.PMID 17874986
- [5]Isbister GK, Buckley NA The pathophysiology of serotonin toxicity in animals and humans: implications for diagnosis and treatment. Clin Neuropharmacol, 2005.PMID 16239759
- [6]Radomski JW, Dursun SM, Reveley MA, et al. An exploratory approach to the serotonin syndrome: an update of clinical phenomenology and revised diagnostic criteria. Med Hypotheses, 2000.PMID 10985912
- [7]Volpi-Abadie J, Kaye AM, Kaye AD Serotonin syndrome. Ochsner J, 2013.PMID 24358002
- [8]Perry PJ, Wilborn CA Serotonin syndrome vs neuroleptic malignant syndrome: a contrast of causes, diagnoses, and management. Ann Clin Psychiatry, 2012.PMID 22563571
- [9]Sun-Edelstein C, Tepper SJ, Shapiro RE Drug-induced serotonin syndrome: a review. Expert Opin Drug Saf, 2008.PMID 18759711
- [10]Ng BK, Cameron AJ The role of methylene blue in serotonin syndrome: a systematic review. Psychosomatics, 2010.PMID 20484716
- [11]Beakley BD, Kaye AM, Kaye AD Tramadol, Pharmacology, Side Effects, and Serotonin Syndrome: A Review. Pain Physician, 2015.PMID 26218943
- [12]Chiew AL, Isbister GK Management of serotonin syndrome (toxicity). Br J Clin Pharmacol, 2025.PMID 38926083
- [13]Cooper J, Duffull SB, Isbister GK Predicting serotonin toxicity in serotonin reuptake inhibitor overdose. Clin Toxicol (Phila), 2023.PMID 36444913
- [14]Chiew AL, Buckley NA The serotonin toxidrome: shortfalls of current diagnostic criteria for related syndromes. Clin Toxicol (Phila), 2022.PMID 34806513
- [15]Prakash S, Patel H, Kumar S, et al. Cyproheptadine in serotonin syndrome: A retrospective study. J Family Med Prim Care, 2024.PMID 38827706
- [16]Evans RW, Tepper SJ, Shapiro RE, et al. The FDA alert on serotonin syndrome with use of triptans combined with selective serotonin reuptake inhibitors or selective serotonin-norepinephrine reuptake inhibitors: American Headache Society position paper. Headache, 2010.PMID 20618823
- [17]Isbister GK, Bowe SJ, Dawson A, et al. Relative toxicity of selective serotonin reuptake inhibitors (SSRIs) in overdose. J Toxicol Clin Toxicol, 2004.PMID 15362595
- [18]Nisijima K, Yoshino T, Yui K, et al. Potent serotonin (5-HT)(2A) receptor antagonists completely prevent the development of hyperthermia in an animal model of the 5-HT syndrome. Brain Res, 2001.PMID 11164765
- [19]Lawrence KR, Adra M, Gillman PK Serotonin toxicity associated with the use of linezolid: a review of postmarketing data. Clin Infect Dis, 2006.PMID 16652315
- [20]Gillman PK Monoamine oxidase inhibitors, opioid analgesics and serotonin toxicity. Br J Anaesth, 2005.PMID 16051647