Psych · Emergency psychiatry — suicide risk
Suicide risk assessment
Also known as Suicide risk · Suicidality · Safety planning · Means restriction · Self-harm risk assessment · Stanley-Brown safety plan · C-SSRS · Suicide prevention
Exam-exhaustive fellowship reference on suicide risk assessment and management — epidemiology; static vs dynamic vs protective factors; ideation-to-action models; structured interview and C-SSRS concepts; means restriction; Stanley-Brown safety planning; disposition; post-discharge peak risk; lithium and clozapine anti-suicide evidence; special populations; CASC communication. Non-stigmatising language. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Suicide risk assessment is a core emergency psychiatry skill: structured enquiry about thoughts of death and suicide, intent, planning, means access, context, and protective factors, integrated with diagnosis, capacity, and a concrete safety and disposition plan.[1][6]
Language matters. Prefer died by suicide, suicide attempt, and self-harm over pejorative or blaming terms. Distinguish the following operational terms used in structured assessment tools and clinical notes.[1][6]
| Term | Clinical meaning |
|---|---|
| Passive death wishes | Wanting to die or not wake up without active planning |
| Active suicidal ideation | Thoughts of ending one's life |
| Intent | Desire and resolve to act |
| Plan | Specific method, place, timing |
| Preparatory acts | Acquiring means, saying goodbye, arranging affairs |
| Suicide attempt | Self-injurious behaviour with at least some intent to die |
| Interrupted / aborted attempt | Stopped by self or other before injury completes |
| NSSI | Self-injury without intent to die (affect regulation) |
Examiners test whether you ask directly (asking does not implant suicide), whether you separate NSSI from suicidal intent, and whether your plan is operational rather than a signed "no-suicide contract".[1][16]
Classification — static, dynamic, protective
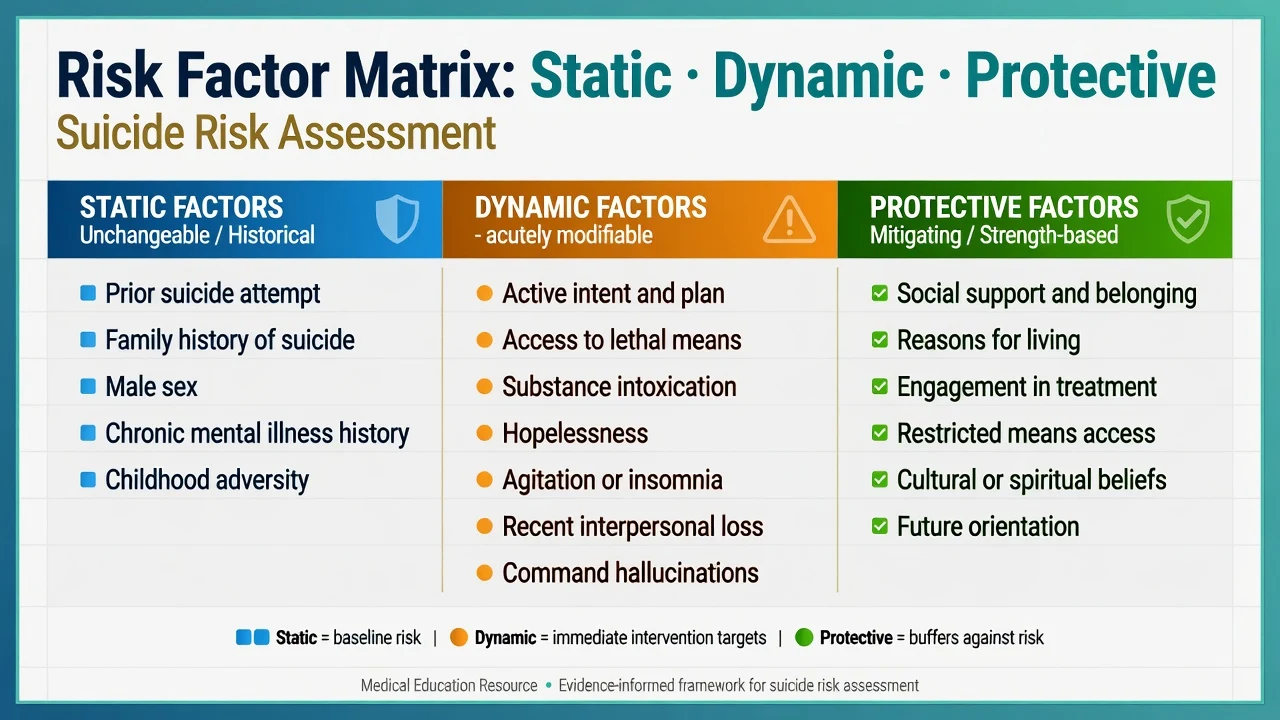
Static (historical / relatively fixed)
Prior suicide attempt is the strongest clinical predictor of future suicidal behaviour. Other static elements include family history of suicide, male sex for death by suicide in many populations, long-standing severe mental illness, and childhood adversity.[1][5][20]
Dynamic (acutely modifiable — exam gold)
Active intent and plan, access to lethal means, substance intoxication, hopelessness, agitation, severe insomnia, command hallucinations, recent interpersonal loss or discharge, untreated mood or psychotic episode, and social withdrawal. These are the levers for today's plan.[1][6]
Protective
Connectedness and belonging, reasons for living, engagement in care, restricted means, cultural or spiritual commitments, responsibility to dependents, and future orientation. Protective factors do not cancel high intent; they inform safety planning and disposition.[3][7]
- Prior attempt
- Demographics
- Long-term diagnosis
- Shape baseline concern
- Do not change overnight
- Intent, plan, means
- Intoxication
- Hopelessness, agitation
- Drive admission vs home
- Reassess after change
- Support and belonging
- Reasons for living
- Treatment alliance
- Means restricted
- Strengthen in safety plan
Epidemiology and risk factors
Cross-national data show that suicidal ideation, plans, and attempts are common enough that every psychiatrist will manage them repeatedly; transitions from ideation to plan to attempt vary by disorder, impulsivity, and means access.[5]
Psychological autopsy work finds mental disorder in a large majority of people who die by suicide, yet most people with mental disorder never die by suicide — base rates defeat naive prediction.[20][16]
Clinical clusters examiners expect: mood disorders, schizophrenia spectrum, substance use disorders, personality disorders (especially borderline), chronic pain, and combinations. Social drivers include isolation, relationship breakdown, unemployment, minority stress, Indigenous inequities, and incarceration transitions.[1][19]
Pathophysiology and models
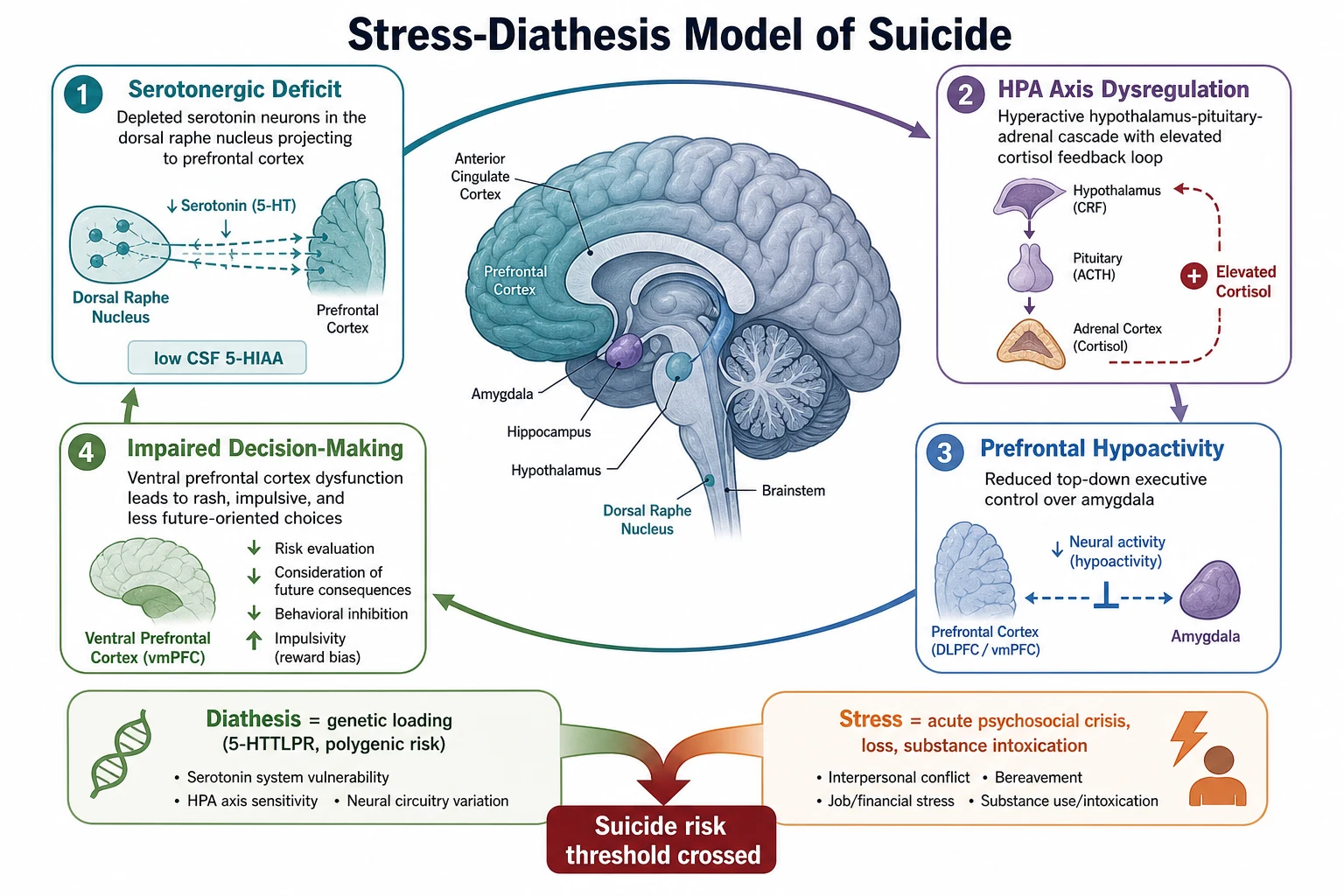
Mann's stress-diathesis framework posits trait vulnerability (serotonergic dysfunction with low CSF 5-HIAA associations, HPA dysregulation, impaired prefrontal decision-making and impulsivity) interacting with acute stressors, intoxication, and psychiatric state.[2]
Ideation-to-action frameworks
Interpersonal Theory of Suicide (IPTS). Desire for suicide arises from thwarted belongingness plus perceived burdensomeness; lethal attempt requires acquired capability (habituation to pain/fear, often via prior self-harm, exposure, or high-risk occupations).[3]
Integrated Motivational-Volitional (IMV) model. Defeat and entrapment drive ideation in the motivational phase; volitional moderators (means, impulsivity, planning, exposure) govern the transition to behaviour.[4]
Three-Step Theory (3ST). Pain plus hopelessness drive ideation; connectedness is a protective moderator; capacity enables the attempt. Useful bedside language for CASC and formulation alongside IPTS and IMV.[1][3][4]
These models do not replace enquiry; they structure why this person, why now, and which levers (belonging, burden, means, intoxication) to target.[1][3][4]
Clinical presentation
Presentations span ED after intentional overdose or self-injury, outpatient disclosure, collateral concern without self-report, medical ward after resuscitation, inpatient observation, crisis-team home visits, custody suites, and perinatal reviews.[1]
Warning signs (near-term behavioural red flags) differ from lifelong risk factors: talking about death or being a burden, seeking means, hopelessness, rage or recklessness, social withdrawal, dramatic mood change, saying goodbye.[1]
Atypical patterns examiners love include older adults with somatic focus, quiet resolve, and high-lethality means; youth with impulsive interpersonal crisis, social media factors, and alcohol; psychosis with command hallucinations and agitation; personality pathology with chronic ideation and acute crisis escalation after abandonment; and denial with high objective risk when farewell acts, means acquisition, or collateral planning contradict self-report. These presentations require full enquiry even when the patient minimises risk.[1][19]
Differential diagnosis
- Some intent to die
- Plan may be present
- Lethality variable
- Needs risk formulation and disposition
- No intent to die
- Affect regulation
- May still escalate risk later
- Explore intent every episode
- Intoxication/withdrawal
- Delirium, TBI, steroids
- Treat medical drivers
- Risk shifts as state clears
Always consider medical and substance contributions to impulsivity or despair. Do not assume malingering; secondary gain is a late, rare, carefully justified conclusion after thorough assessment.[1]
Clinical and bedside assessment
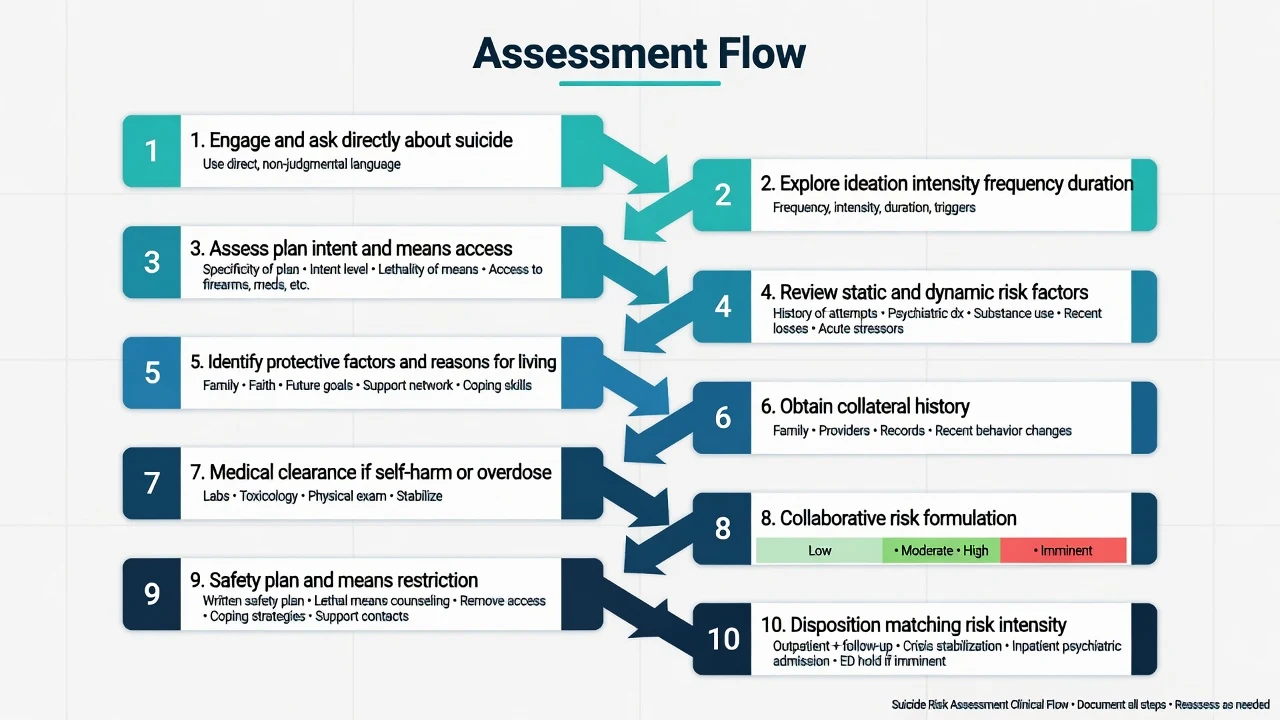
Interview structure
Structure the encounter as: engage (private space, empathy, cultural safety, interpreter if needed); ask directly about thoughts of ending life, desire to die, and whether a method has been considered; map ideation frequency, intensity, duration, controllability, and command quality; assess intent, plan, timeline, rehearsals, and preparatory acts without coaching novel methods; review means access (medications, firearms, context-specific pesticides, ligature, high places); explore triggers, substances, sleep, agitation, recent losses, and discharge stressors; elicit concrete protective factors and reasons for living; obtain collateral (family, GP, prior notes, EMS) and document refusals; judge capacity and least-restrictive legal options with jurisdiction-specific statutes named only when known; then write a formulation stating drivers, moderators, and the plan — not a single number. This structure aligns with severity and behaviour domains used in instruments such as the C-SSRS while remaining a clinical formulation, not a score alone.[6][1]
C-SSRS and scales
The Columbia-Suicide Severity Rating Scale structures ideation severity, intensity, and suicidal behaviour categories with validated psychometric support for assessment consistency.[6] Use scales to standardise enquiry, not to replace clinical judgement. Meta-analytic work shows risk scales after self-harm have limited ability to predict who will die; prioritise clinical factors and care pathways over cut-points.[18][17]
IDEATION
Investigations
After overdose or injury: ABC and medical stabilisation first. Check observations, ECG when cardiotoxic overdose possible, paracetamol and salicylate levels as indicated, blood glucose, pregnancy test when relevant, and targeted toxicology. UDS has timing and false-negative limits. Neuroimaging, EEG, or autoimmune work-up only when organic red flags appear. Document MSE with quoted suicidal content and insight.[1]
Management — immediate safety
No-suicide contracts are not a safety intervention and are marked down in exams. Use least-restrictive legal pathways when capacity is impaired and risk is high; statutes vary by jurisdiction — state principles, not invented section numbers. Medical clearance does not equal psychiatric safety. Immediate safety work prioritises environment, observation, means control, and an operational plan over paperwork promises.[7][16]
Management — definitive and stepwise
Safety planning (Stanley-Brown principles)
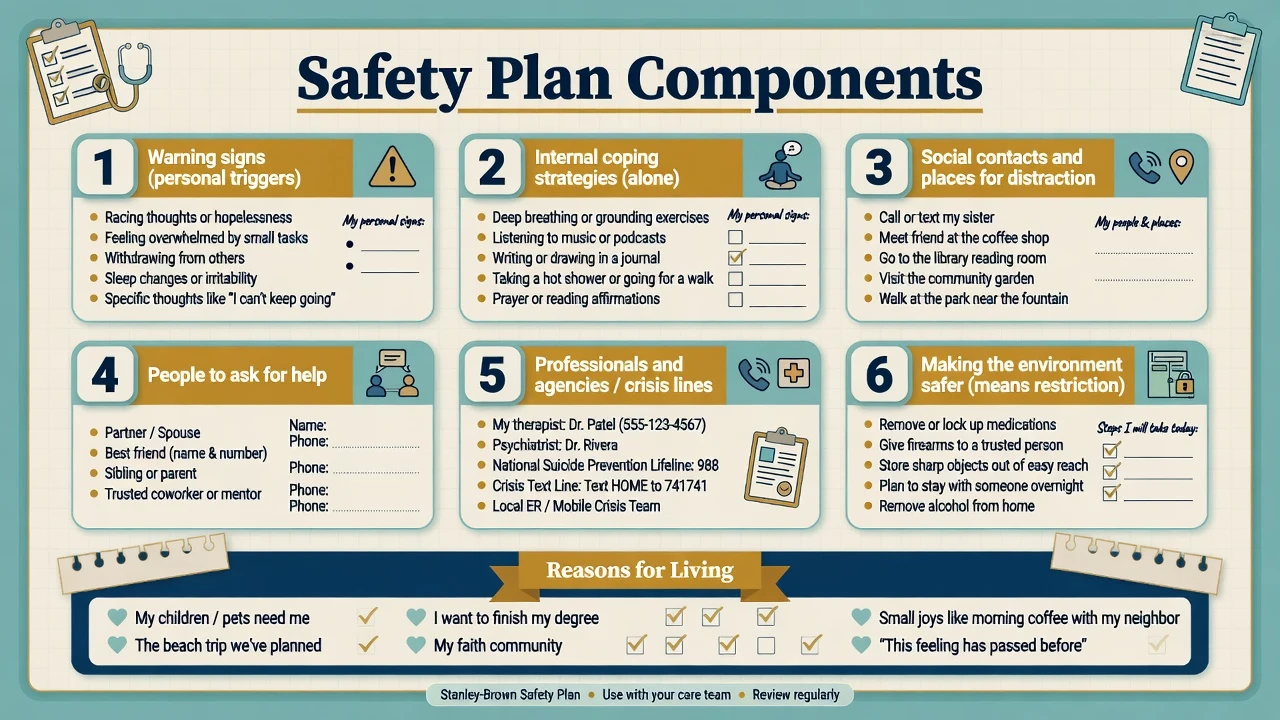
The Safety Planning Intervention (SPI) is a brief, collaborative, written plan. Core steps include personal warning signs; internal coping strategies usable alone; social contacts and places for distraction; people to ask for help; professionals and agencies (local crisis lines — do not assume US 988 in ANZ or UK); making the environment safer through means restriction; and, often integrated, reasons for living.[7]
SPI with structured follow-up reduced suicidal behaviour versus usual care in an ED randomised trial of suicidal patients.[7] Brief contact interventions (WHO multi-country brief intervention and contact; postcard contact after self-poisoning) support the principle of caring contacts after crisis presentations.[19]
Means restriction
Population and individual evidence supports restricting access to highly lethal methods (firearms, pesticides, toxic medications, ligature points, hotspots).[19] Collaborate respectfully: temporary transfer of firearms to a trusted person under local law, lockboxes for medication, limited dispensing after overdose, alcohol removal during acute crisis. Do not teach methods.
Psychotherapies with suicide-specific evidence
| Approach | Core evidence | Exam point |
|---|---|---|
| Cognitive therapy for suicide attempts | Brown et al. RCT — reduced reattempt vs usual care | Target suicidal cognitions specifically |
| DBT | Linehan — reduced suicidal behaviours in BPD | Skills, chain analysis, phone coaching model |
| Brief CBT (military) | Rudd et al. — fewer attempts over follow-up | Short, structured, crisis-focused |
| CAMS | Collaborative assessment of drivers of suicide | Alliance and co-authored plan |
Pharmacology with anti-suicide signal
Lithium in mood disorders is associated with reduced suicide risk in systematic review and meta-analysis — a key viva fact beyond anti-manic efficacy. Use within usual lithium monitoring (levels, renal, thyroid) and shared decision-making.[11]
Clozapine reduced suicidal behaviour versus olanzapine in schizophrenia/schizoaffective disorder in InterSePT — offer when indicated, with full clozapine monitoring infrastructure.[12]
Antidepressants treat depression that drives risk; discuss early activation, akathisia, and close monitoring especially in youth. Do not withhold indicated treatment solely from black-box fear. ECT remains relevant for severe depression with food refusal or high suicide risk.[1][19]
RANZCP-aligned practice emphasises comprehensive risk formulation, cultural safety (including Aboriginal and Torres Strait Islander and Māori contexts), means restriction including firearms legislation differences from the US, and local Mental Health Act principles. Crisis lines and aftercare pathways are state and territory-specific.[19][1]
Specific scenarios
- ED post-overdose: medical first, then full risk interview once lucid; SPI before discharge if community disposition; never "medically cleared equals free to go" without psychiatric plan.[7]
- Inpatient: environmental safety, observation level, leave decisions, family meetings, discharge planning as the highest-risk transition.[13][14]
- Chronic SI in personality disorder: validate chronicity, still reassess acute change, DBT and skills focus, avoid both abandonment and endless unplanned admission cycles without formulation.[9]
- Command hallucinations: treat psychosis urgently; observe; do not dismiss content.[1]
- Custody: entry and post-release peaks; multi-agency plan; ligature risk awareness without graphic detail.[19]
Complications and pitfalls
- Trusting denial when collateral is alarming.[1]
- Over-reliance on binary risk labels or scale cut-points.[16][18]
- No-suicide contracts.[16]
- Missing firearms or stockpiled medication.[19]
- Discharging into the post-discharge peak without same-week review.[13][15]
- Stigmatising language that shuts down disclosure.[1]
- Confusing NSSI with suicide attempt without intent enquiry.[1]
- Incomplete documentation (no formulation, no who was told, no review time).[16]
Prognosis and disposition
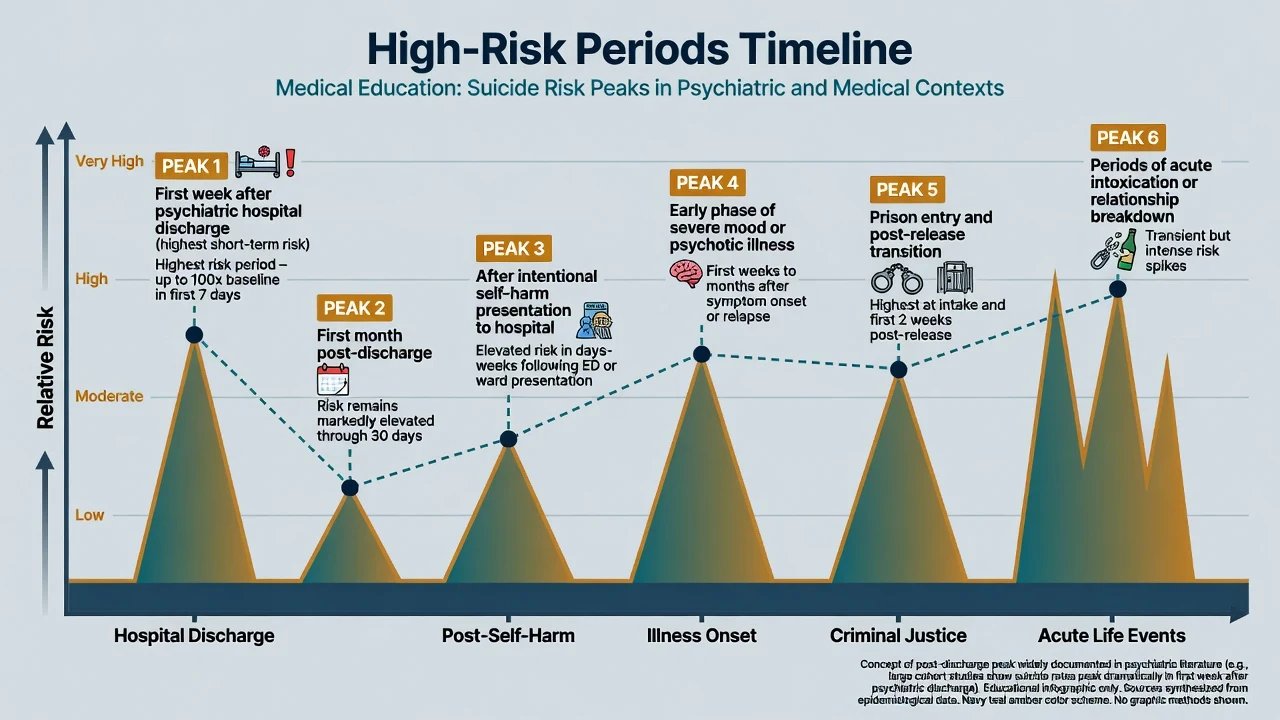
Register-based and meta-analytic evidence shows markedly elevated suicide rates after psychiatric hospitalisation, especially early after discharge.[13][14][15] Plan the transition: appointment booked, means restricted, family briefed, crisis contacts given, and primary care informed.
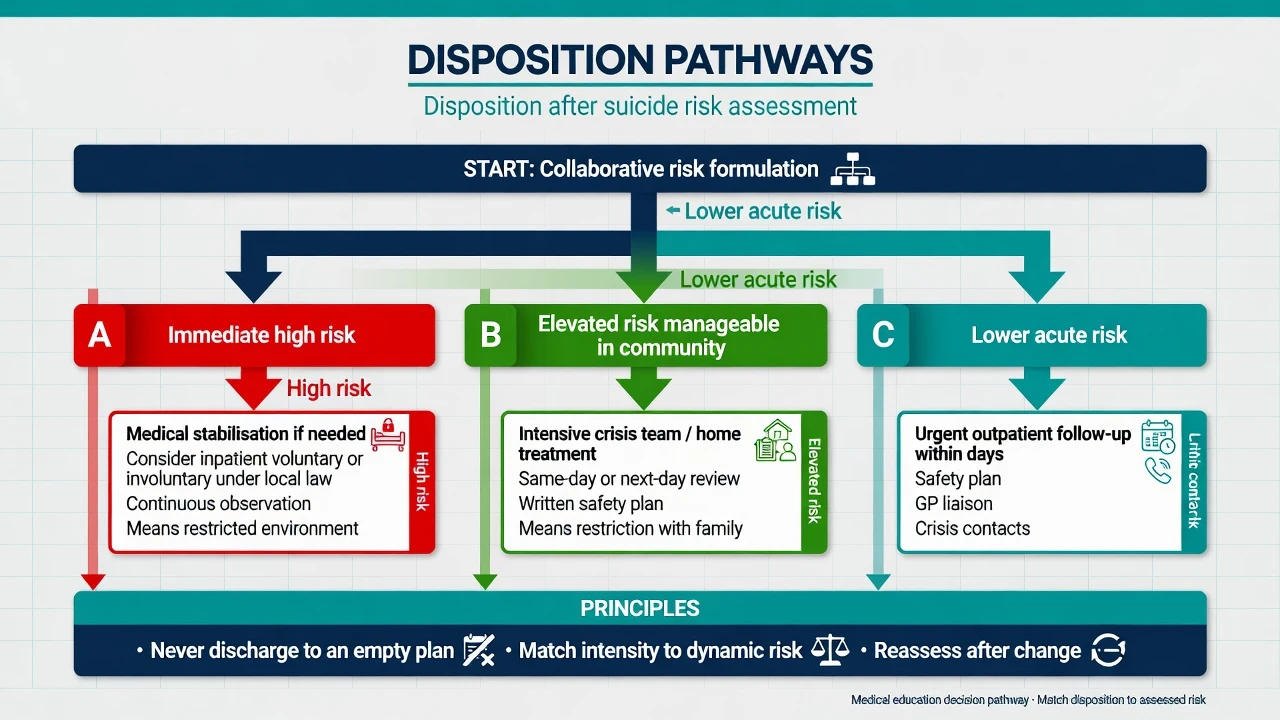
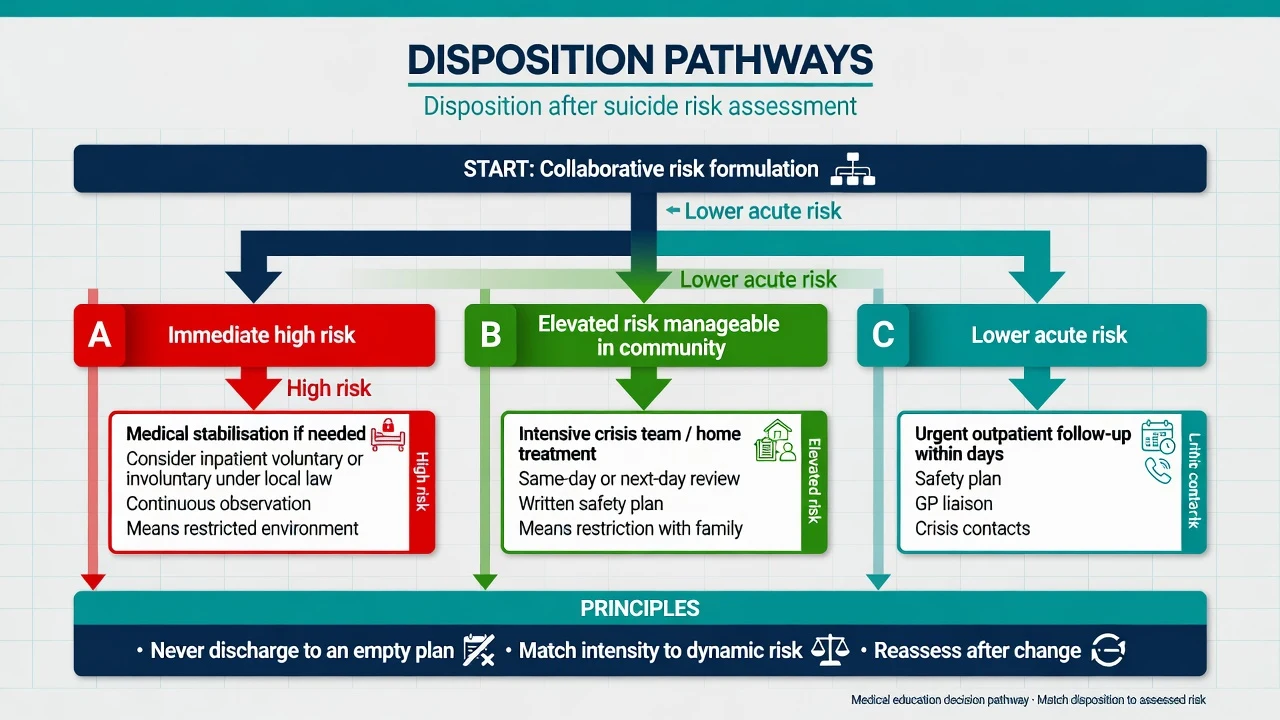
Documentation standard: risk formulation (drivers and buffers), specific plan, observation level if inpatient, means steps taken, who was informed, capacity and legal status, and review timeframe. Write for the next clinician at 3 a.m.[16][13]
Special populations
Special populations share the same assessment spine but differ in lethality patterns, communication of distress, and systems partners. Youth: impulsivity, peer and social media factors, family engagement, school liaison, home means access. Older adults: higher lethality, physical illness, isolation, firearms or stockpiled medication, under-detection of depression. Indigenous peoples: social determinants, cultural safety, community-led approaches — avoid deficit-only framing. Perinatal: maternal suicide risk, infant safety, shared medication and admission decisions. LGBTQ+: minority stress, rejection, affirmative care. Prisoners: entry and post-release peaks, multi-agency continuity. Intellectual disability or autism: atypical distress communication and essential carer collateral.[1][19]
Evidence, guidelines, and controversies
Landmark suicide-specific interventions: Brown cognitive therapy; Linehan DBT; Rudd brief CBT; Stanley SPI in ED; systems and means-restriction evidence in the Zalsman review.[8][9][10][7][19]
Medication: lithium meta-analysis; InterSePT clozapine.[11][12]
Controversy: risk categorisation. Large and colleagues argue useful individual prediction is limited and that services should ensure high-quality care for all presenting with self-harm or suicidality rather than diverting resources by inaccurate strata alone.[16][17] Fellowship answer: acknowledge limited predictive validity and still make a structured formulation that drives intensity of follow-up and means restriction.
Exam pearls
- Asking about suicide does not plant the idea.[1]
- Prior attempt is the strongest clinical marker.[1][5]
- Risk is dynamic — reassess after substances clear, after discharge, after loss.[13][16]
- Lithium and clozapine have the best drug-specific anti-suicide evidence in their populations.[11][12]
- No-suicide contracts fail exams.[16]
- Most suicides occur outside the "highest risk" bin at last contact — access and means matter at population level.[16][19]
- Post-discharge and post-self-harm periods are examinable high-risk windows.[13][15]
Self-test: post-discharge plan
A 34-year-old is discharged day 10 after a serious overdose in major depression. Passive SI only today, engaged, partner present, lithium started, meds locked, SPI completed, review in 48 hours booked. What is the single most important systems principle?[13]
Answer: Treat the post-discharge interval as a known peak-risk period — rapid follow-up, means restriction, and a living safety plan are non-negotiable even when today's interview is reassuring.[13][15][7]
References
- [1]Turecki G, Brent DA Suicide and suicidal behaviour Lancet, 2016.PMID 26385066
- [2]Mann JJ Neurobiology of suicidal behaviour Nat Rev Neurosci, 2003.PMID 14523381
- [3]Van Orden KA, Witte TK, Cukrowicz KC, et al. The interpersonal theory of suicide Psychol Rev, 2010.PMID 20438238
- [4]O'Connor RC, Kirtley OJ The integrated motivational-volitional model of suicidal behaviour Philos Trans R Soc Lond B Biol Sci, 2018.PMID 30012735
- [5]Nock MK, Borges G, Bromet EJ, et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts Br J Psychiatry, 2008.PMID 18245022
- [6]Posner K, Brown GK, Stanley B, et al. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults Am J Psychiatry, 2011.PMID 22193671
- [7]Stanley B, Brown GK, Brenner LA, et al. Comparison of the Safety Planning Intervention With Follow-up vs Usual Care of Suicidal Patients Treated in the Emergency Department JAMA Psychiatry, 2018.PMID 29998307
- [8]Brown GK, Ten Have T, Henriques GR, et al. Cognitive therapy for the prevention of suicide attempts: a randomized controlled trial JAMA, 2005.PMID 16077050
- [9]Linehan MM, Comtois KA, Murray AM, et al. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder Arch Gen Psychiatry, 2006.PMID 16818865
- [10]Rudd MD, Bryan CJ, Wertenberger EG, et al. Brief cognitive-behavioral therapy effects on post-treatment suicide attempts in a military sample: results of a randomized clinical trial with 2-year follow-up Am J Psychiatry, 2015.PMID 25677353
- [11]Cipriani A, Hawton K, Stockton S, et al. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis BMJ, 2013.PMID 23814104
- [12]Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT) Arch Gen Psychiatry, 2003.PMID 12511175
- [13]Chung DT, Ryan CJ, Hadzi-Pavlovic D, et al. Suicide Rates After Discharge From Psychiatric Facilities: A Systematic Review and Meta-analysis JAMA Psychiatry, 2017.PMID 28564699
- [14]Qin P, Nordentoft M Suicide risk in relation to psychiatric hospitalization: evidence based on longitudinal registers Arch Gen Psychiatry, 2005.PMID 15809410
- [15]Olfson M, Wall M, Wang S, et al. Short-term Suicide Risk After Psychiatric Hospital Discharge JAMA Psychiatry, 2016.PMID 27654151
- [16]Large MM, Ryan CJ, Carter G, et al. Can we usefully stratify patients according to suicide risk? BMJ, 2017.PMID 29042363
- [17]Large M, Kaneson M, Myles N, et al. Meta-Analysis of Longitudinal Cohort Studies of Suicide Risk Assessment among Psychiatric Patients: Heterogeneity in Results and Lack of Improvement over Time PLoS One, 2016.PMID 27285387
- [18]Chan MK, Bhatti H, Meader N, et al. Predicting suicide following self-harm: systematic review of risk factors and risk scales Br J Psychiatry, 2016.PMID 27340111
- [19]Zalsman G, Hawton K, Wasserman D, et al. Suicide prevention strategies revisited: 10-year systematic review Lancet Psychiatry, 2016.PMID 27289303
- [20]Cavanagh JT, Carson AJ, Sharpe M, et al. Psychological autopsy studies of suicide: a systematic review Psychol Med, 2003.PMID 12701661