Psych · Emergency psychiatry — violence risk
Violence risk assessment
Also known as Aggression risk assessment · HCR-20 · Structured professional judgement · Dangerousness assessment · Violence risk formulation · DASA · Brøset Violence Checklist · Threat assessment psychiatry
Exam-exhaustive fellowship reference on violence risk assessment — static vs dynamic vs protective factors; HCR-20 and structured professional judgement concepts; imminence vs long-term tools; mental illness–violence relationship without stigma; command hallucinations; substance use; personality; risk formulation and management plans; least restrictive care; documentation; special populations. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
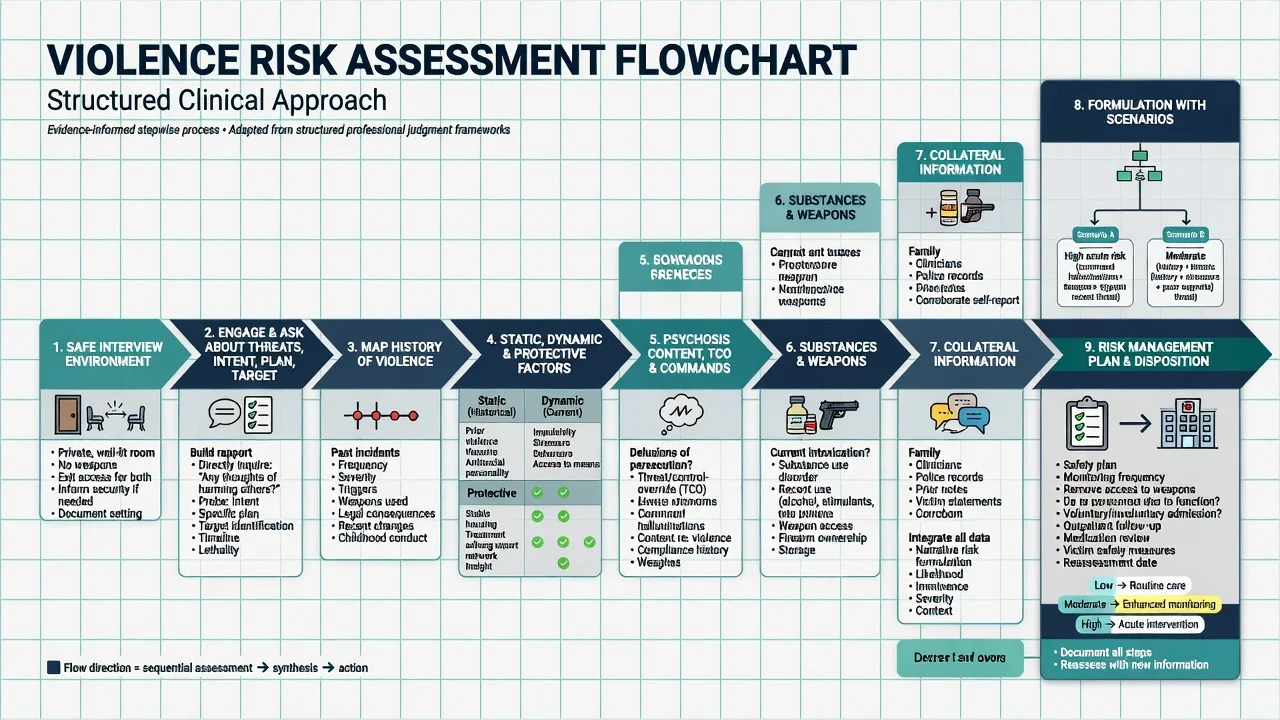
Violence risk assessment is a core emergency, inpatient, community, and forensic-interface skill: structured enquiry about past and current aggression, threats, targets, means, psychosis content, substances, personality traits, and situational triggers, integrated into a formulation that drives a concrete management plan rather than a crystal-ball score.[17][19]
Operational terms examiners expect include aggression (hostile behaviour that may or may not cause physical harm), violence (behaviour causing or intended to cause physical harm to others), imminent risk (hours to a few days — ward/ED window), intermediate or long-term risk (weeks to years — discharge and community planning), risk formulation (narrative of drivers, scenarios, and preventable pathways), and risk prediction (probabilistic estimate with modest group-level performance).[8][15][17]
Three assessment approaches structure the literature and viva answers. Unstructured clinical judgement is flexible but inconsistent. Actuarial tools use fixed factors and algorithms (for example VRAG-class instruments in forensic settings); they rank relative risk in research samples but are weak as a sole clinical plan. Structured professional judgement (SPJ) combines evidence-based item domains with clinical synthesis and risk management (HCR-20 family as the prototype). SPJ is not a single magic number.[8][9][10][17]
Meta-analyses of risk assessment instruments show moderate group-level predictive accuracy and limited ability to identify individuals who will offend with high certainty; tools inform, they do not replace, clinical responsibility.[8][9][10]
Classification — static, dynamic, protective, and SPJ domains
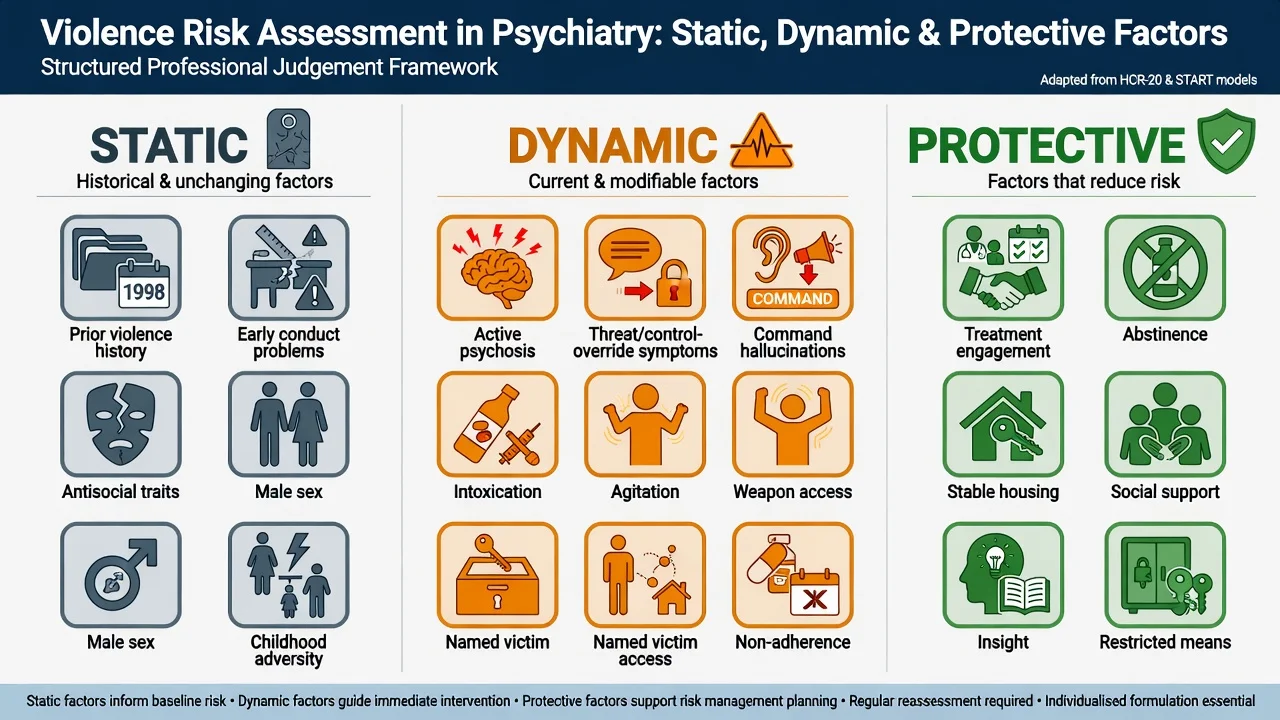
Static (historical / relatively fixed)
Prior violence is the single most important general predictor of future violence across psychiatric and general offender literatures. Other static elements include younger age at first violence, male sex in many samples, long-standing antisocial or psychopathic traits, childhood conduct problems and adversity, and chronic major mental illness history.[4][19]
Dynamic (acutely modifiable — exam gold)
Active psychosis (especially threat/control-override content), command hallucinations with compliance risk, mania with irritability, intoxication or withdrawal, agitation and akathisia, non-adherence, access to weapons, access to a named victim, interpersonal conflict, homelessness, and supervision failure. These are the levers for today's plan.[2][4][14]
Protective
Treatment engagement and insight, abstinence or controlled substance use, stable housing, personal support, structured routine, restricted means, and feasible future plans. Protective factors do not cancel active intent against a named victim; they shape what community care can safely support.[17][19]
HCR-20-style SPJ structure (conceptual)
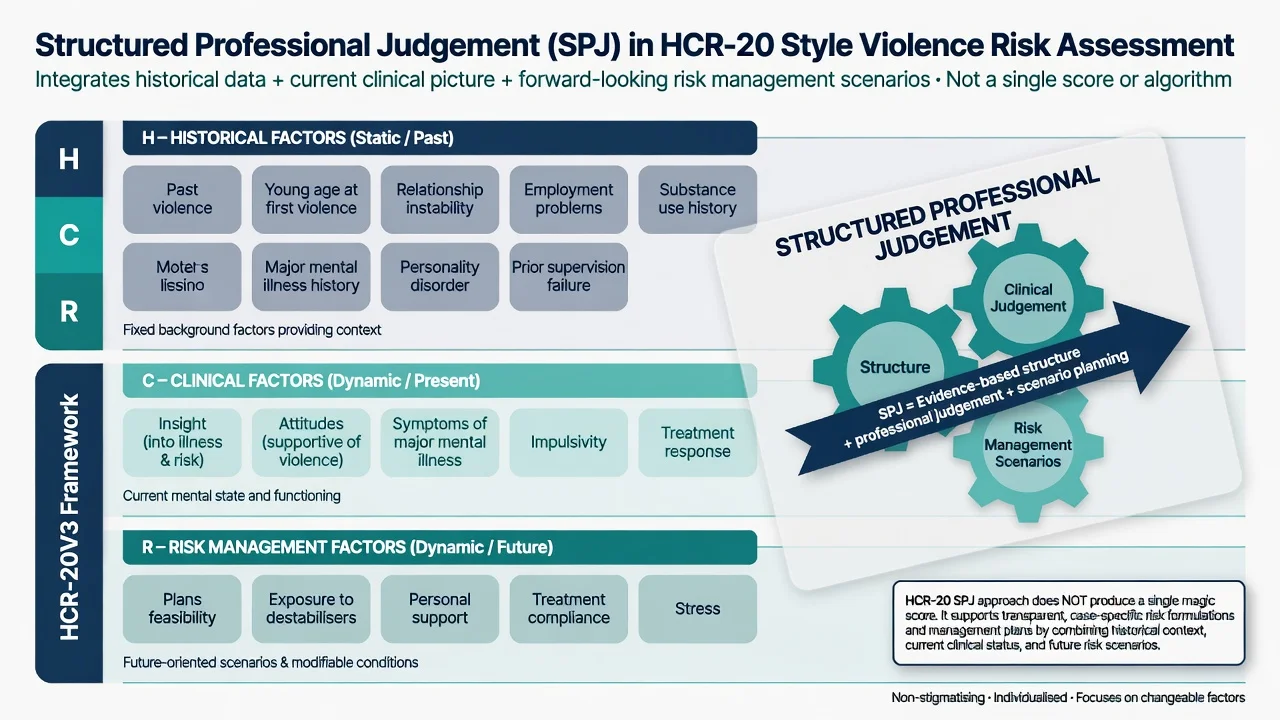
Think in three bands used across HCR-20 versions and teaching: Historical (past violence and related background vulnerabilities), Clinical (current insight, attitudes, symptoms, impulsivity, treatment response), and Risk management (feasibility of plans, exposure to destabilisers, support, compliance, stress). Use the framework to force complete enquiry and scenario planning. Do not claim you scored a specific total without training and the manual; examiners reward process and formulation.[8][9][17]
- Prior violence
- Early conduct/antisocial traits
- Long-term diagnosis history
- Shape baseline concern
- Change slowly
- Psychosis content, commands
- Intoxication, agitation
- Weapons and victim access
- Drive admission vs home
- Reassess after change
- Engagement and insight
- Supports and housing
- Abstinence
- Means restricted
- Strengthen in plan
Epidemiology and the mental illness–violence relationship
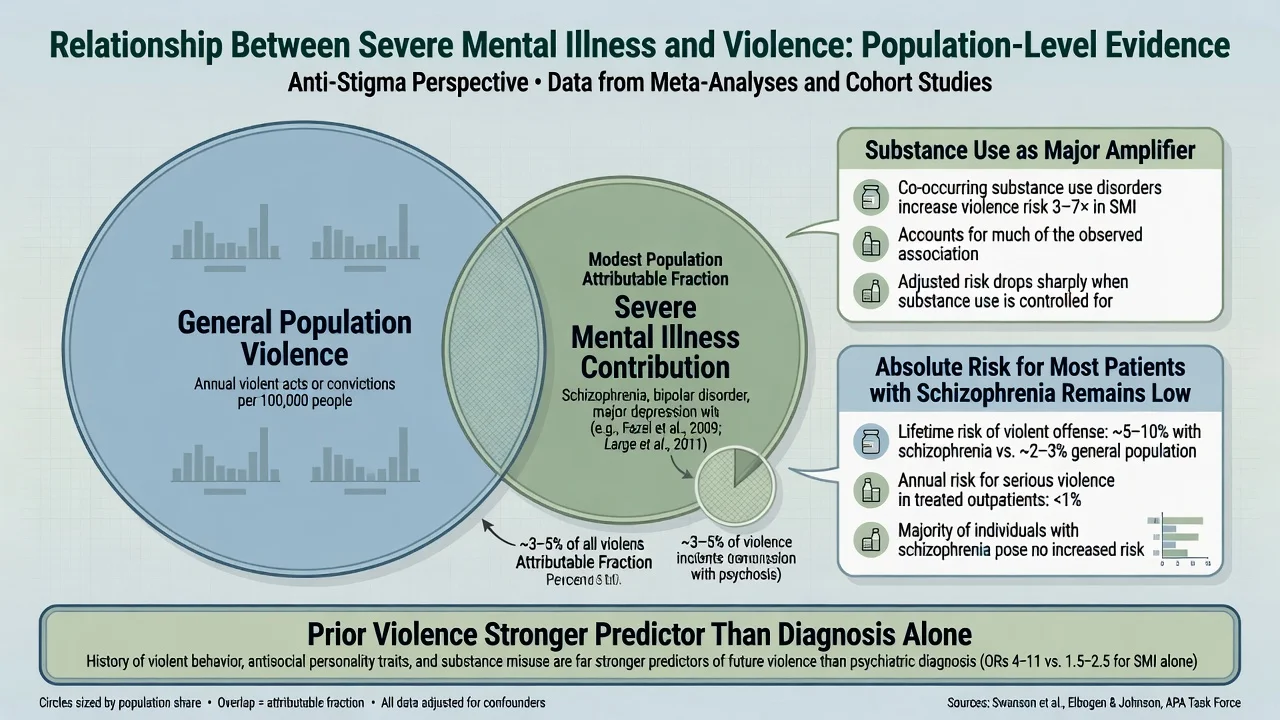
Nuance without denial. Schizophrenia spectrum disorders are associated with elevated odds of violence perpetration relative to the general population in meta-analyses, yet most people with schizophrenia are never violent, and severe mental illness accounts for only a modest fraction of all violent crime at population level.[3][5][18][20]
Taylor and Gunn's classic "myth and reality" framing remains examinable: media stereotypes overstate the share of homicide attributable to mental illness; clinical vigilance must still target high-risk subgroups without stigmatising the whole population in care.[20]
Substance use is the major amplifier. NESARC analyses show that the mental disorder–violence link is substantially driven by co-occurring substance use; when substance comorbidity is accounted for, excess risk shrinks though it does not always vanish entirely.[6][7]
First-episode psychosis (FEP) is a special window: systematic reviews find elevated rates of violence and a disproportionate share of psychosis-related homicide occurring before treatment, supporting assertive early intervention and risk enquiry in untreated FEP.[12][13]
MacArthur Violence Risk Assessment Study followed people discharged from acute psychiatric facilities and compared violence rates with neighbourhood controls: violence occurred, was often related to substance use and situational factors, and delusions alone were not a simple linear predictor of violence — a foundation for modern dynamic formulation.[1][2]
Psychosis as a risk factor for violence to others shows a positive association in meta-analysis, moderated by study design and comorbidity — consistent with treating acute psychotic risk states without equating "psychosis" with permanent dangerousness.[11]
Pathophysiology and mechanisms
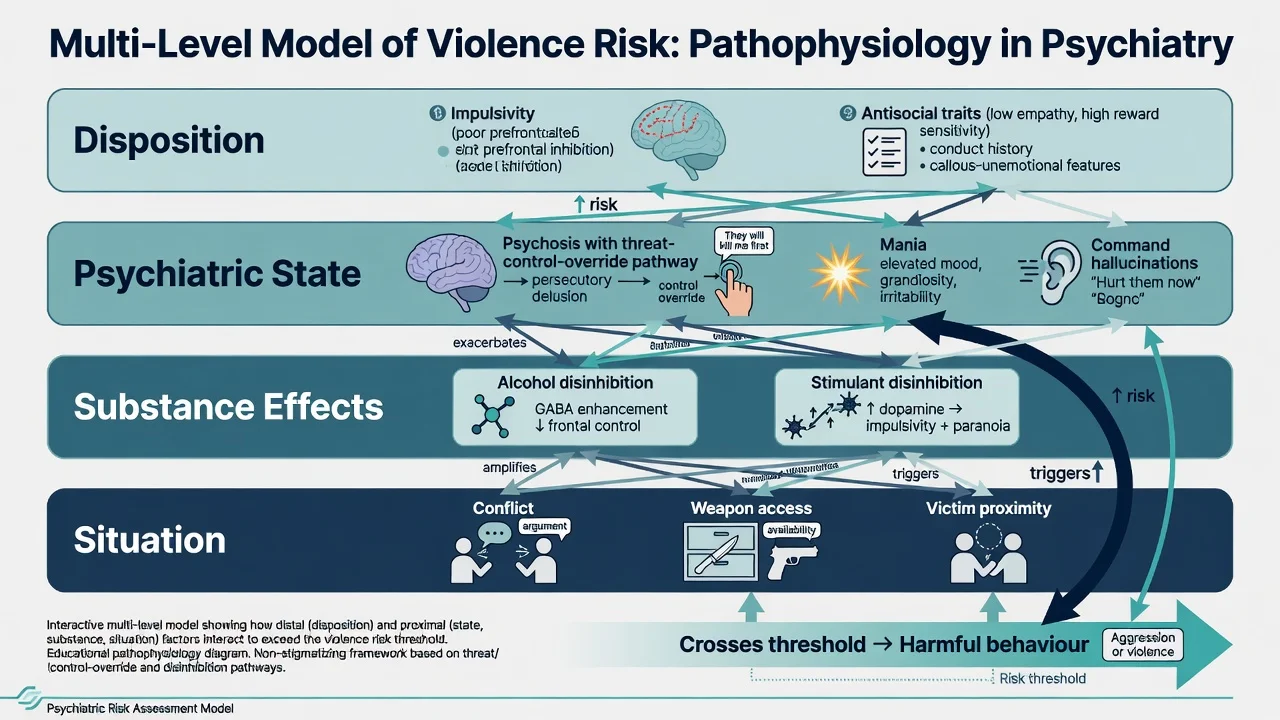
A practical multi-level model for formulation combines disposition (impulsivity, antisocial traits, cognitive style, developmental adversity), psychiatric state (active psychosis, mania, severe affective dysregulation, delirium), substance effects (alcohol and stimulants disinhibit; withdrawal can escalate agitation), and situation (conflict, weapons, victim proximity, supervision gaps, crowded wards).[4][6][19]
Threat/control-override (TCO)
Link and colleagues described threat/control-override symptoms: beliefs that others mean harm and that external forces control one's mind. These contents can organise defensive or pre-emptive aggression and remain a useful bedside prompt even when pure "delusion checklists" fail as predictors.[2]
Command hallucinations
Command hallucinations are associated with violence in some clinical samples, but compliance is not automatic. Assess content (harm to self vs others), voice identity and authority, emotional response, past compliance, and current resistance — then treat psychosis and secure environment accordingly.[14]
Personality and instrumental vs reactive aggression
Instrumental (goal-directed) violence is more linked to antisocial personality; reactive affective aggression is more linked to emotional dysregulation, intoxication, and acute psychosis. Discriminating motive guides victim safety planning and therapy targets.[19]
Clinical presentation
Presentations span ED after threats or assaults, inpatient aggression against staff or co-patients, community crisis with a named victim, domestic/intimate partner violence disclosed in clinic, stalking concerns, forensic court or prison referrals, and family fear without patient disclosure.[1][19]
Warning signs of rising imminence include escalating verbal threats, weapon seeking or brandishing, violation of boundaries, pacing and psychomotor agitation, target fixation, intoxication, command content increasing in urgency, and recent relationship rupture.[14][15]
Atypical patterns examiners probe: quiet persecutory resolve with planning; cultural idioms of anger misread as "normal conflict"; minimisation when collateral describes preparation; and people with severe mental illness who are victims more often than perpetrators — still assess perpetration risk when indicated without dismissing victimisation.[18][19]
Differential diagnosis
- TCO / command content
- First-episode untreated
- Responds to antipsychotic Rx
- Often reactive defensive
- Intoxication timeline
- Stimulant/alcohol pattern
- Clears with sobriety (partly)
- Treat SUD as risk Rx
- Planning and gain
- Limited remorse
- Personality history
- Forensic pathways
Always exclude organic drivers: delirium, traumatic brain injury sequelae, encephalitis, epilepsy-related aggression, and steroid or other drug-induced states. Personality disorder and pure antisocial violence can present without psychosis. Malingering is a late hypothesis after thorough assessment.[19]
Clinical and bedside assessment
Interview safety first
Choose a private but observable space, know your exit, consider a second clinician for high-arousal assessments, remove potential weapons from the environment, and use calm de-escalation stance. Parallel suicide and vulnerability assessment is mandatory — risk domains travel together.[15][17]
Structure the clinical interview
- Current — thoughts of harming others; intent; plan; timeline; named targets; weapon access; ability to resist.
- History of violence — what happened, to whom, triggers, weapons, injuries, legal outcomes, patterns (domestic vs stranger vs staff).
- Psychosis content — persecutory systems, TCO, commands, passivity experiences.
- Mood and impulsivity — mania, mixed states, rage episodes, self-control.
- Substances — type, timing, relationship to past violence.
- Personality and antisocial traits — conduct history, callousness, entitlement.
- Situation — housing, relationships, custody status, access to victims, recent stressors.
- Collateral — family, GP, police, prior notes, EMS; document refusals.
- Capacity and legal options — least restrictive pathway consistent with safety; statutes are jurisdiction-specific (do not invent section numbers).
Imminent tools on the ward
The Dynamic Appraisal of Situational Aggression (DASA) structures short-horizon prediction of inpatient aggression and supports staffing and intervention decisions.[15] The Brøset Violence Checklist (BVC) similarly rates imminent risk behaviours. A randomised trial of structured risk assessment on acute wards reduced violent incidents versus control — structure helps when it changes practice, not when it is form-filling alone.[16]
Longer-horizon instruments
SPJ instruments (HCR-20 family) and actuarial tools show moderate predictive validity in meta-analyses; comparative studies find no single tool is dramatically superior across all settings.[8][9][10] Clinical prediction tools such as OxMIV (low risk of violent crime in severe mental illness) illustrate scalable actuarial assistance for service design — still not a substitute for individual formulation.[19]
THREATENS
Investigations
Medical work-up when organic red flags (fever, fluctuating cognition, focal neurology, new-onset psychosis in later life): observations, bloods, toxicology as indicated, neuroimaging/EEG selectively. Document MSE with quoted threats, targets, and command content. Scales structure risk; they do not clear medical mimics.[15][19]
Management — immediate safety
Immediate priorities: environment search; separate potential victims; adequate staffing; verbal de-escalation; treat intoxication, withdrawal, pain, and akathisia; pharmacological management of severe agitation per local protocol (see acute agitation and rapid tranquillisation topic); continuous observation if required. Seclusion and restraint are last resort with monitoring and documentation.[15][16]
Management — definitive risk management plan
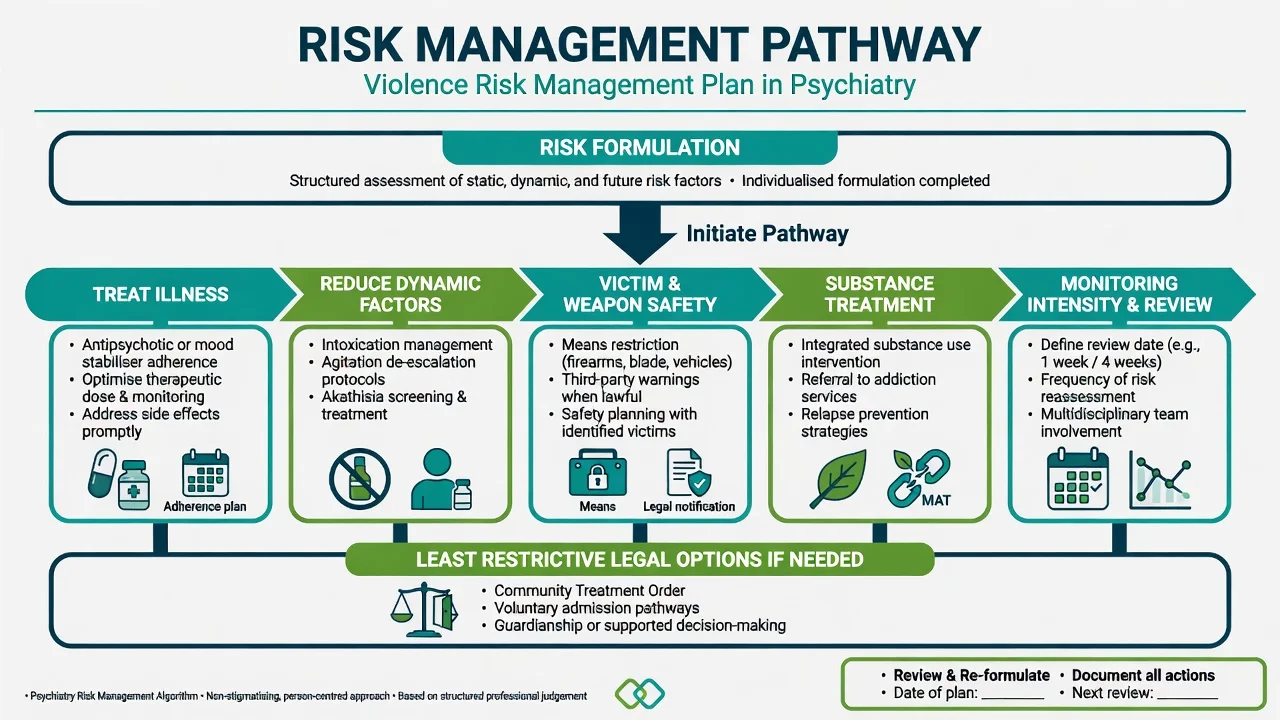
Convert formulation into actions across treat-illness steps (antipsychotic initiation or optimisation; mood stabiliser when indicated; address side effects that drive non-adherence; clozapine consideration for persistent aggression in schizophrenia under specialist pathways), dynamic-factor reduction (detox support; agitation ladder; sleep; akathisia treatment; leave restrictions), victim and weapon safety (temporary firearm transfer under local law; no-contact conditions; third-party warnings when lawful; safe housing away from target), integrated substance treatment, monitoring with a review date and multi-agency meetings, and legal options (voluntary care if safe; compulsory pathways if capacity and risk require — jurisdiction-labelled principles only).[4][6][17][19]
Imminence versus long-term tools
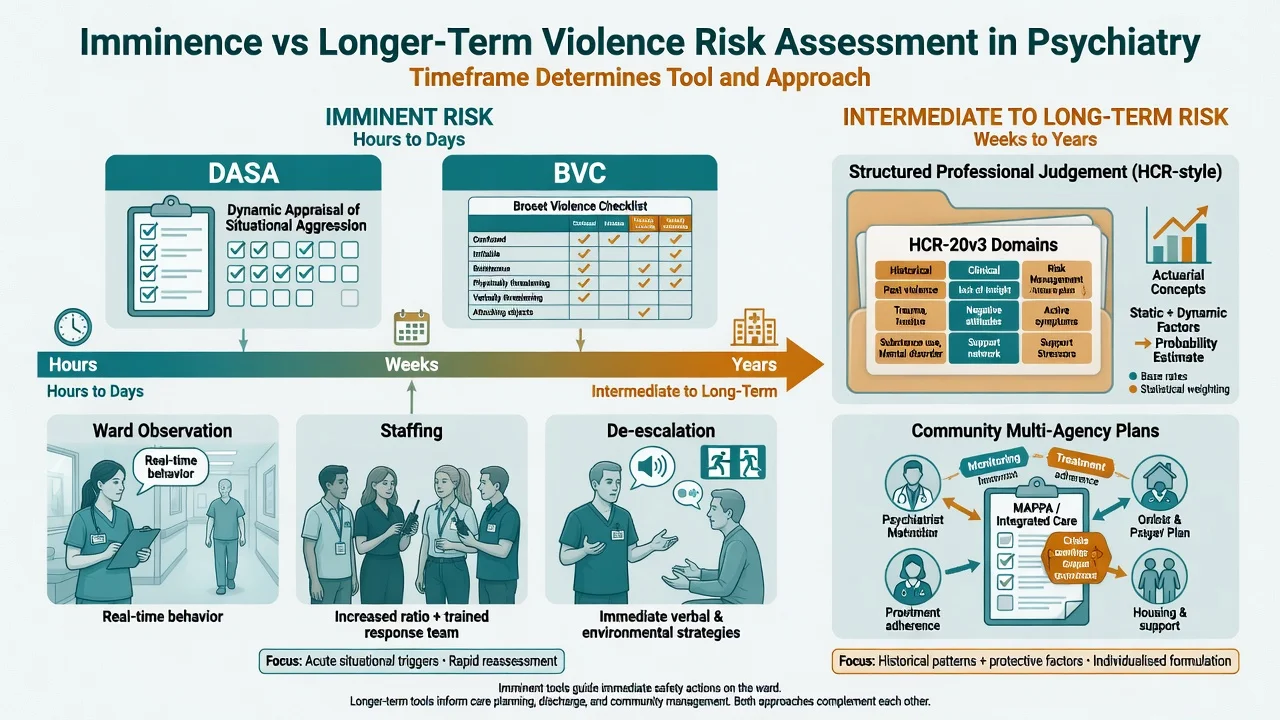
Use DASA/BVC and nursing observation for today's shift decisions; use SPJ-informed formulation for discharge and community planning. Mixing horizons is a classic exam trap (e.g. relying only on a historical actuarial score while ignoring rising ward agitation).[8][15][16]
Pharmacology notes examiners expect
Antipsychotics treat the psychotic state that can drive violence; adherence support is risk management. Clozapine has evidence signals for reducing aggression in treatment-resistant schizophrenia in specialist literature — offer only with full monitoring infrastructure. Lithium and mood stabilisers address manic irritability when bipolar spectrum is the driver. Do not use high-dose polypharmacy as a substitute for environmental and substance interventions.[4][19]
RANZCP-aligned practice emphasises comprehensive risk formulation, cultural safety (including Aboriginal and Torres Strait Islander and Māori contexts), multi-agency work with police and child protection when indicated, and Mental Health Act principles that are state/territory-specific. Firearms law and temporary surrender pathways differ from the US.[19]
Specific subtypes and scenarios
- Inpatient aggression: DASA/BVC trajectory, staffing, de-escalation, PRN ladder, seclusion last, post-incident review.[15][16]
- Named victim in community: assess access, lawful warnings, no-contact supports, possible admission.[17]
- Untreated FEP: assertive engagement, early antipsychotic treatment, family safety planning — pre-treatment homicide share is a viva classic.[12][13]
- Intimate partner violence: separate victim interview when safe; do not use couple therapy as first-line safety; child protection pathways if indicated.[19]
- Command hallucinations to harm others: treat psychosis urgently; observe; map compliance factors.[14]
- Personality + substances without psychosis: dual diagnosis and forensic interface; avoid "not psychiatric" dismissal when risk is high.[6][19]
- Forensic step-down / release: structured tools, gradual leave, multi-agency plan, substance monitoring.[8][19]
Complications and pitfalls
- Stigmatising overprediction that equates SMI with dangerousness and drives coercive care without dynamic factors.[18][20]
- Ignoring substance use and antisocial history while over-focusing on diagnosis alone.[6][4]
- Score-only decisions without scenario planning.[8][17]
- Missing weapons and victim access.[17]
- Incomplete documentation (no target, no plan, no review date).[17]
- Failing least-restrictive options when lower intensity would work — or failing to escalate when imminence is high.[16]
- Missing organic causes of aggression.[19]
Prognosis and disposition
Disposition ladders (least to most restrictive examples): supported community care with intensive monitoring; crisis/home treatment; voluntary admission; involuntary admission under local law; secure/forensic pathways when indicated. Match intensity to dynamic risk and victim safety, not diagnosis alone.[17][19]
Triggers for violent criminality in psychotic disorders include acute life events and substance-related exposures — reassess after clinical change, relationship rupture, non-adherence, and release from hospital or custody.[4][19]
Documentation standard: risk formulation (static/dynamic/protective), named scenarios (who/what/when), actions taken (including who was warned), observation level, legal status, and review timeframe. Write for the next clinician at 3 a.m.[17]
Special populations
- Youth / FEP: early intervention; family engagement; school/work context; substance use common.[12][13]
- Older adults: delirium and dementia-related aggression; different risk tools and medical work-up priority.
- Intellectual disability / autism: behavioural phenotypes, communication supports, avoid pure "forensic" framing without formulation.
- Perinatal: assess risk to infant and partner; joint mother–baby pathways when available; jurisdiction-specific child protection duties.
- Indigenous / cultural safety: higher system contact can reflect inequity and over-policing as well as illness; use culturally safe assessment and avoid stereotyping.[19]
- Custody: entry and release peaks; multi-agency plans; ligature and assault environment awareness without graphic method coaching.[19]
- Women: intimate partner dynamics; under-recognition of female perpetration and of victimisation.[19]
Evidence, guidelines, and regional differences
Landmark strands for exams: MacArthur study (Steadman, Appelbaum, Monahan); Fazel meta-analyses of schizophrenia and violence; Witt risk factors in psychosis; Whiting updates; Douglas psychosis–violence meta-analysis; instrument validity meta-analyses (Fazel, Singh, Yang); DASA/BVC and the Abderhalden RCT; population impact and myth/reality papers (Fazel and Grann; Taylor and Gunn).[1][2][3][4][5][8][11][16][18][20]
Guidelines (NICE violence/aggression short-term management; RANZCP risk standards; APA forensic principles) converge on prevention, de-escalation, least restrictive care, and structured assessment — regional deltas sit in firearms, duty-to-protect law, and Mental Health Act mechanisms.[16][19]
Exam pearls
- Prior violence predicts better than diagnosis alone.[4][19]
- Substance use is the key amplifier of the SMI–violence association.[6][7]
- Most people with schizophrenia are never violent; quote absolute risk framing and modest population attributable fraction.[3][18][20]
- Untreated first-episode period is a high-yield homicide window.[12]
- Command hallucinations: assess compliance likelihood, not a yes/no checkbox.[14]
- SPJ = structure + clinical judgement + risk management scenarios.[8][17]
- Match tool to horizon: DASA/BVC today; HCR-style SPJ for discharge/community.[15][16]
- Never invent Mental Health Act section numbers across jurisdictions.[17]
- Documentation without a review date is incomplete.
References
- [1]Steadman HJ, Mulvey EP, Monahan J, et al. Violence by people discharged from acute psychiatric inpatient facilities and by others in the same neighborhoods Arch Gen Psychiatry, 1998.PMID 9596041
- [2]Appelbaum PS, Robbins PC, Monahan J Violence and delusions: data from the MacArthur Violence Risk Assessment Study Am J Psychiatry, 2000.PMID 10739415
- [3]Fazel S, Gulati G, Linsell L, et al. Schizophrenia and violence: systematic review and meta-analysis PLoS Med, 2009.PMID 19668362
- [4]Witt K, van Dorn R, Fazel S Risk factors for violence in psychosis: systematic review and meta-regression analysis of 110 studies PLoS One, 2013.PMID 23418482
- [5]Whiting D, Gulati G, Geddes JR, et al. Association of Schizophrenia Spectrum Disorders and Violence Perpetration in Adults and Adolescents From 15 Countries: A Systematic Review and Meta-analysis JAMA Psychiatry, 2022.PMID 34935869
- [6]Elbogen EB, Johnson SC The intricate link between violence and mental disorder: results from the National Epidemiologic Survey on Alcohol and Related Conditions Arch Gen Psychiatry, 2009.PMID 19188537
- [7]Van Dorn R, Volavka J, Johnson N Mental disorder and violence: is there a relationship beyond substance use? Soc Psychiatry Psychiatr Epidemiol, 2012.PMID 21359532
- [8]Fazel S, Singh JP, Doll H, et al. Use of risk assessment instruments to predict violence and antisocial behaviour in 73 samples involving 24 827 people: systematic review and meta-analysis BMJ, 2012.PMID 22833604
- [9]Singh JP, Grann M, Fazel S A comparative study of violence risk assessment tools: a systematic review and metaregression analysis of 68 studies involving 25,980 participants Clin Psychol Rev, 2011.PMID 21255891
- [10]Yang M, Wong SC, Coid J The efficacy of violence prediction: a meta-analytic comparison of nine risk assessment tools Psychol Bull, 2010.PMID 20804235
- [11]Douglas KS, Guy LS, Hart SD Psychosis as a risk factor for violence to others: a meta-analysis Psychol Bull, 2009.PMID 19702378
- [12]Nielssen O, Large M Rates of homicide during the first episode of psychosis and after treatment: a systematic review and meta-analysis Schizophr Bull, 2010.PMID 18990713
- [13]Large MM, Nielssen O Violence in first-episode psychosis: a systematic review and meta-analysis Schizophr Res, 2011.PMID 21208783
- [14]McNiel DE, Eisner JP, Binder RL The relationship between command hallucinations and violence Psychiatr Serv, 2000.PMID 11013329
- [15]Ogloff JR, Daffern M The dynamic appraisal of situational aggression: an instrument to assess risk for imminent aggression in psychiatric inpatients Behav Sci Law, 2006.PMID 17171770
- [16]Abderhalden C, Needham I, Dassen T, et al. Structured risk assessment and violence in acute psychiatric wards: randomised controlled trial Br J Psychiatry, 2008.PMID 18700217
- [17]Buchanan A Risk of violence by psychiatric patients: beyond the "actuarial versus clinical" assessment debate Psychiatr Serv, 2008.PMID 18245161
- [18]Fazel S, Grann M The population impact of severe mental illness on violent crime Am J Psychiatry, 2006.PMID 16877653
- [19]Whiting D, Lichtenstein P, Fazel S Violence and mental disorders: a structured review of associations by individual diagnoses, risk factors, and risk assessment Lancet Psychiatry, 2021.PMID 33096045
- [20]Taylor PJ, Gunn J Homicides by people with mental illness: myth and reality Br J Psychiatry, 1999.PMID 10211145