Psych · Forensic psychiatry — arson and firesetting
Arson and fire-setting
Also known as Firesetting · Fire-setting · Deliberate firesetting · Pyromania · Arson mental disorder · Psychotic arson · Recidivist arson · Youth firesetting · Pathological fire-setting · Forensic arson assessment
Exam-exhaustive fellowship reference on deliberate firesetting, arson, and pyromania — terminology triad, DSM/ICD exclusions and rarity, NESARC epidemiology, strong psychosis association, multi-trajectory pathways, fire-specific assessment and specialist treatment, youth and gender variants, criminal-responsibility interface, and risk-management principles without invented statute section numbers. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
1 MCQ with explanations
Target exams
Red flags
Overview and definition
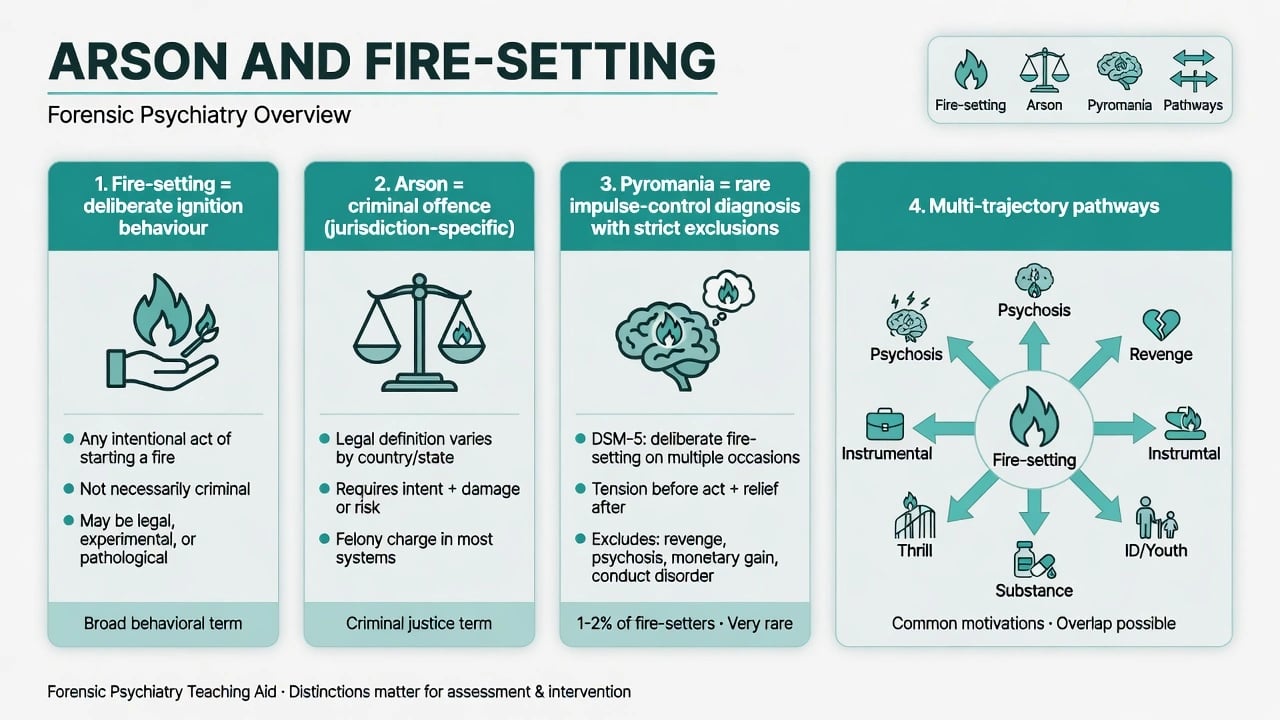
Deliberate fire use sits at a forensic interface of behaviour science, criminal law, and psychiatric diagnosis. Fellowship examiners punish the undergraduate habit of calling every arsonist a "pyromaniac." Hold three frames simultaneously.[1][11]
- Behavioural science — firesetting (preferred research term) means deliberate ignition regardless of legal outcome or diagnosis.[1][11]
- Criminal law — arson (and local equivalents) is an offence with jurisdiction-specific elements (intent, property type, endangerment). Statutes and labels are not universal — do not invent section numbers.[1]
- Nosology — pyromania (DSM-5-TR impulse-control disorder; related ICD-11 framing of fire-setting as a disorder of impulse control when criteria are met) requires repeated deliberate fire-setting with tension/arousal, fire fascination, pleasure/relief, and exclusion of profit, ideology, anger/revenge, crime concealment, impaired judgment from psychosis/mania/intoxication, and better explanation by conduct/antisocial patterns alone.[1][7]
Operational vocabulary:
- Index firesetting — the offence or incident under assessment.
- Fire interest / identification — cognitive-affective attraction to fire (dimensional, not diagnostic by itself).
- Instrumental vs expressive — gain/concealment versus emotion/communication pathways (can co-exist).
- Fire-specific treatment needs — attitudes, interest, offence-supportive thinking, and skills deficits beyond generic offender programmes.[8][12]
Classification — pathways, not one disease
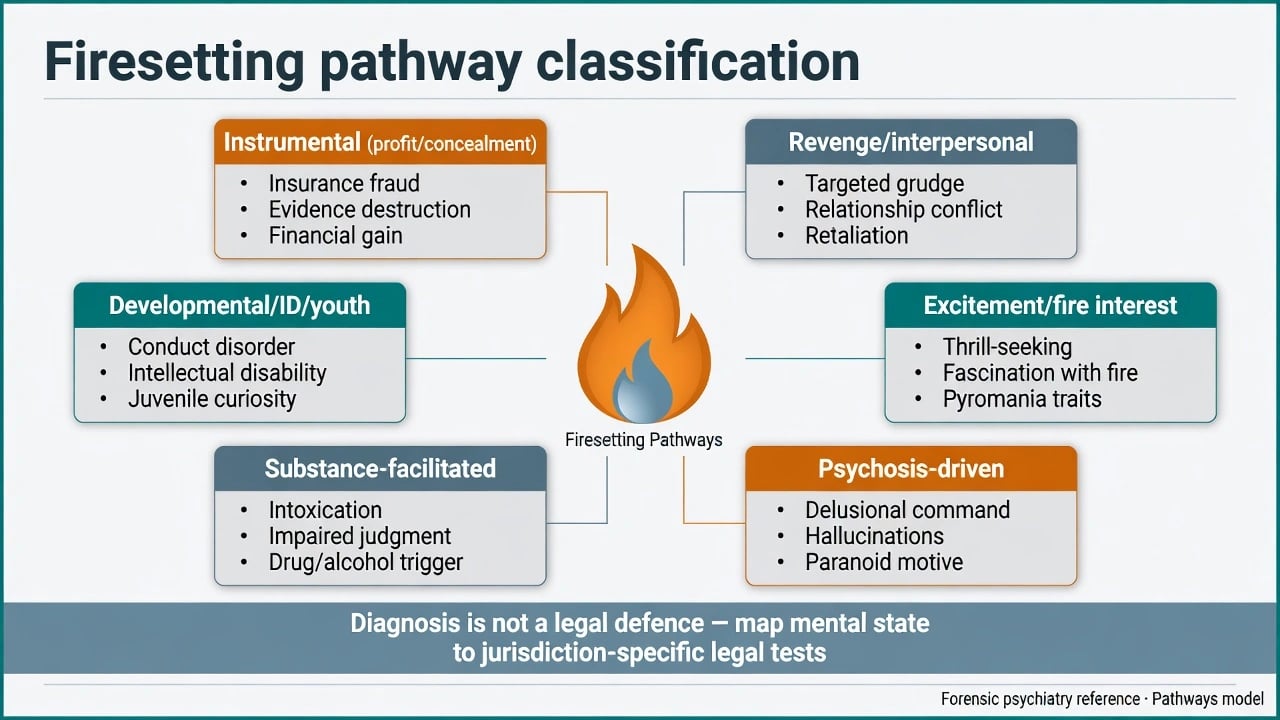
Examiner pathway set (adapt labels; motives often mixed):[1][8]
| Pathway | Typical drivers | Forensic notes |
|---|---|---|
| Instrumental | Insurance, profit, evidence destruction | Usually outside pure "mental condition" defence; still assess substances/illness co-factors |
| Revenge / interpersonal | Relationship conflict, grievance | High dynamic risk if access and anger persist |
| Excitement / fire interest | Thrill, fascination, reinforcement from fire | Overlaps fire-specific needs; pyromania only if full criteria and exclusions clear |
| Psychosis-driven | Persecutory/command content, disorganisation | Strong offence-class association with psychosis (Anwar); treat illness; reconstruct material time carefully |
| Substance-facilitated | Alcohol/stimulants impairing judgment | Facilitator more than sole "diagnosis"; jurisdiction limits on intoxication defences vary |
| Developmental / ID / youth | Curiosity, fireplay progression, communication via behaviour | Public-health and family intervention; capacity/suggestibility issues in ID |
| Pathway teaching table — multi-trajectory constructs, not exclusive DSM categories. [1][5][8] |
Multi-trajectory models of adult firesetting (M-TTAF-style teaching) emphasise developmental context, psychological vulnerabilities, fire-specific factors, and moderators rather than a single "fire bug type."[1][8][12]
Epidemiology and risk
Community surveys (NESARC analyses) place lifetime deliberate fire-setting in the order of about 1% of adults, with substantial psychiatric comorbidity among those who report it — not a rare curiosity only of secure hospitals.[2][3]
Among people charged with or convicted of arson/firesetting:
- Pyromania is rare when criteria are applied carefully (Lindberg consecutive Finnish male recidivist fire-setters).[4]
- Mental illness rates are elevated versus other offenders and community controls in Australian Victorian data (Ducat).[6]
- Schizophrenia and other psychoses show a particularly strong association with arson relative to many other crime types in Swedish national case-control work (Anwar, Långström, Grann, Fazel) — high-yield fellowship fact: arson is not "just another antisocial act" when psychosis is present, but absolute risk of arson for any given patient remains low.[5]
Public-health framing matters: deliberate firesetting causes deaths, injury, property loss, and community trauma far beyond the rarity of the pyromania label (Tyler et al., Lancet Public Health).[11]
Mechanisms
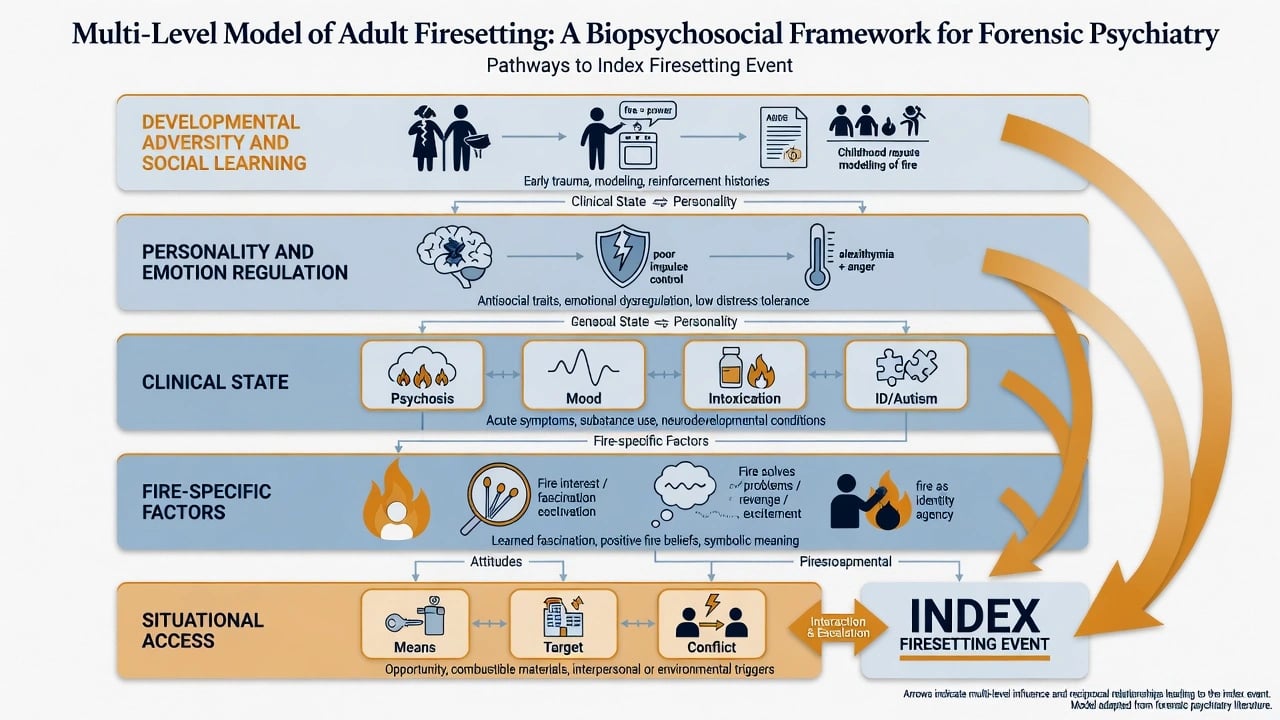
Integrate levels rather than hunting a single gene or "fire centre":
- Developmental — adversity, social learning, childhood fireplay.[14]
- Personality / regulation — antisocial traits, emotion dysregulation, low distress tolerance.[8]
- Clinical state — untreated psychosis, mania, severe depression with communication-by-fire, intoxication, ID/autism communication limits.[5][6]
- Fire-specific — interest, identification with fire, fire-supportive attitudes, scripts that "fire solves problems."[8][12]
- Situation — access to means, vulnerable targets, domestic conflict, institutional settings.
Clinical presentation
Pre-offence. Escalating fire interest or threats; childhood/adolescent fireplay; domestic grievance; untreated first-episode or relapsing psychosis; binge drinking or stimulant use; prior undetected small fires.[1][14]
Index characteristics to reconstruct. Target (own home, partner's property, institution, bush/vegetation, stranger commercial), planning vs impulsivity, accelerants, whether occupied, intent to harm persons vs property, self-harm/suicide by fire.[1][12]
Post-offence MSE. Ongoing psychotic content about the fire or victims; intoxication clearing; minimisation or proud fascination; depressive collapse and suicide risk (firesetting samples show elevated suicidal behaviour in classic Finnish work taught alongside Repo series — keep suicide on the checklist even when the index is property crime).[1]
Differential diagnosis
Discriminators, not laundry lists:
- Pyromania vs instrumental arson — external incentive and planning for gain defeat pyromania.[1][7]
- Psychosis-driven vs primary impulse-control — delusional nexus and exclusion criteria; psychosis association is real but not automatic for every arsonist.[5]
- Mania, intoxication, delirium, rare organic states — time-limited judgment impairment.[1]
- Conduct/ASPD opportunistic fire — broader antisocial repertoire without fire-specific affective drive meeting pyromania.[4]
- ID/autism-related behavioural communication — not "just badness"; assess adaptive function.[6]
- Self-immolation / suicidal fire use vs other-directed arson.
- Malingering of pyromania or psychosis after arrest — multi-source consistency testing.[15]
Assessment
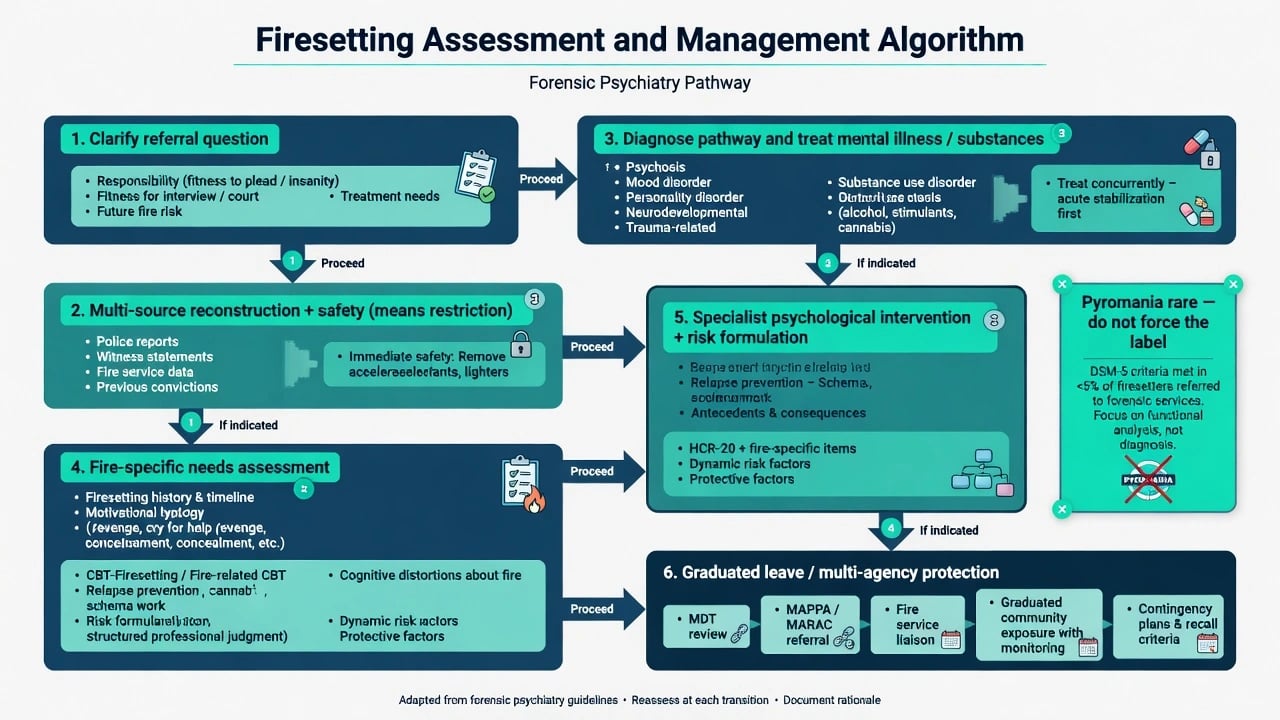
Clarify the referral question. Criminal responsibility at material time; fitness now; future firesetting/violence risk; treatment needs; programme suitability. These are different products.[1][15]
Multi-source reconstruction. Police brief, fire investigation summary, body-worn video if available, prior fires, childhood history, psychiatric notes, toxicology, collateral. Do not opine on responsibility from interview alone.[1][15]
Fire-specific domains (clinical teaching aligned with Four Factor Fire Scales principles and secure-setting needs tools such as SAFARI-style assessment): fire interest and identification; offence-supportive attitudes; emotional regulation; social competence; mental illness; substance use; situational triggers.[8][12]
Risk formulation. Scenario-based: who/what targets, when, with what means, under what clinical state. Pair general violence SPJ concepts with fire-specific factors. Risk instruments offer only moderate group-level accuracy for antisocial outcomes — humility required; scores do not decide past legal questions.[16]
Investigations
- Toxicology at arrest; medical review if delirium/organic differential plausible.[1]
- Cognitive/adaptive testing when ID suspected; developmental history for autism spectrum.
- Record search for prior firesetting, hospital/prison fire incidents, non-adherence, duration of untreated psychosis.
- Do not invent proprietary cut-offs for fire scales; state that tools structure clinical judgment.[12][16]
Acute management
- Safety first — remove lighters/matches/accelerant access in custody or hospital; observe for further ignition attempts and for suicide.[1]
- Medical/psychiatric stabilisation — treat intoxication/withdrawal; if acute psychosis drives the presentation, use ordinary acute antipsychotic pathways (for example oral or intramuscular antipsychotics per local rapid-tranquillisation and first-episode protocols, with ECG/metabolic baseline when feasible, monitoring for EPS and QTc) — agent choice is guided by acuity and prior response, not by a special "arson drug."[5]
- Interview timing — unreliable while floridly intoxicated or thought-disordered if the product is a responsibility opinion.[15]
- Court liaison — lawful placement pathways; principles only, no invented sections.
Definitive management
Treat the pathway, not the media label.
- Psychosis pathway — antipsychotic treatment to remission/relapse prevention; clozapine only by usual treatment-resistance criteria, not because of arson per se; adherence and dual-diagnosis work.[5]
- Affective/expressive pathway — treat mood disorder; skills for anger and interpersonal problem-solving.
- Substance pathway — integrated substance treatment; intoxication is often a facilitator.
- Pyromania (rare) — Grant clinical series document high comorbidity; pharmacotherapy literature is case-level (including experimental observations), not a robust first-line algorithm for arson generally — do not invent doses as if guideline-mandated for all firesetters.[7]
Specialist psychological intervention. Imprisoned firesetters differ from other prisoners and benefit from fire-specific programme content (Gannon). Specialist group therapy shows treatment effects on fire-related psychological factors in prisoner samples (FIPP-style evaluation). Mentally disordered offender programmes (FIP-MO) have been evaluated for male and female patients in secure care.[8][9][10][12]
Risk management and disposition. Graduated leave, environmental fire safety, multi-agency public protection principles, victim-access restrictions when revenge pathway, substance monitoring. Length of secure care follows residual risk formulation, not the word "arson" alone.[12][13]
Subtypes and scenarios
- Psychotic arson of a family home (high-yield Anwar + responsibility reconstruction).
- Instrumental insurance arson (diagnosis may be irrelevant to motive).
- Revenge after relationship breakdown.
- Youth fireplay progression (Lambie 10-year offending follow-up — broader antisocial outcomes matter).[14]
- Female firesetters (distinct psychopathology patterns in series).
- Intellectual disability community or institutional firesetting.
- Prison/hospital firesetting (means and contagion).
- Recidivist firesetting with substances — risk is heterogeneous; avoid automatic "kindling" fatalism without individual formulation.[13]
Complications and pitfalls
- Equating arson with pyromania.[1][4]
- Missing psychosis while chasing a "fire bug" stereotype.[5]
- Assuming mental illness explains all arson (instrumental motives exist).
- Assuming all firesetters are extreme recidivists (Brett challenges overstated dangerousness narratives).[13]
- Ignoring suicide risk after firesetting offences.
- Inventing statute numbers; writing "classic pyromaniac" without criteria.
- Using only generic violence tools without fire-specific needs.[12][16]
Prognosis and special populations
Recidivism is heterogeneous. Some index events are single expressive or first-episode psychotic crises that settle with treatment; others show repeated firesetting with personality and substance drivers. Youth firesetters require family-inclusive public-health responses, not only adult forensic labels.[13][14]
Women, people with ID, inpatients, and prisoners need pathway-adapted assessment. Cultural formulation and bias awareness apply as in all forensic work — name local protocols without fabricating them.[1][6][10]
Evidence, guidelines, and regional deltas
High-yield evidence map for viva recall (each row points to a verified reference):[1][2][4][5]
| Source | Exam use |
|---|---|
| Burton et al. JAAPL | Terminology triad and forensic expert role |
| Blanco / Vaughn NESARC | Community prevalence order and comorbidity |
| Lindberg | Pyromania rarity in recidivist arson |
| Anwar et al. | Psychosis–arson association strength |
| Ducat et al. | Australian mental illness rates among firesetters |
| Gannon / Tyler FIPP and FIP-MO | Specialist treatment evidence |
| Tyler Lancet Public Health / Psychiatry | Public-health and evidence-based assessment call |
| AAPL insanity guideline | Responsibility methodology principles |
| Fazel risk-instrument meta | Humility about predictive tools |
| Landmark map for exam navigation. [1][2][4][5][6][9][11][15][16] |
Exam pearls
FIRE-SET (exam checklist)
Pyromania versus psychosis-driven arson is the classic discriminator pair for MCQ stems.[1][5][7]
Legal-clinical interface (principles only)
- Responsibility — mental state at ignition mapped to local mental impairment / insanity limbs; diagnosis is never enough.[15]
- Fitness — present ability to understand proceedings and instruct counsel; reassess after treatment.
- Risk — future scenarios and management plan; instruments do not answer the past legal question.[16]
- Statutes, verdict names (NGRI/NGMI/mental impairment), and disposal pathways are jurisdiction-specific.
Bottom line for fellowship
Master the terminology triad, the rarity of pyromania, the strong psychosis–arson association, multi-trajectory formulation, fire-specific assessment and specialist psychological programmes, and the temporal triad of legal-clinical questions. Keep absolute-risk humility, restrict means, treat illness and substances, and never invent section numbers or force a pyromania label onto ordinary arson.[1][5][11][12]
References
- [1]Burton PR, McNiel DE, Binder RL Firesetting, arson, pyromania, and the forensic mental health expert J Am Acad Psychiatry Law, 2012.PMID 22960918
- [2]Blanco C, Alegría AA, Petry NM, et al. Prevalence and correlates of fire-setting in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) J Clin Psychiatry, 2010.PMID 20361899
- [3]Vaughn MG, Fu Q, Delisi M, et al. Prevalence and correlates of fire-setting in the United States: results from the National Epidemiological Survey on Alcohol and Related Conditions Compr Psychiatry, 2010.PMID 20399330
- [4]Lindberg N, Holi MM, Tani P, et al. Looking for pyromania: characteristics of a consecutive sample of Finnish male criminals with histories of recidivist fire-setting BMC Psychiatry, 2005.PMID 16351734
- [5]Anwar S, Långström N, Grann M, et al. Is arson the crime most strongly associated with psychosis? A national case-control study of arson risk in schizophrenia and other psychoses Schizophr Bull, 2011.PMID 19850668
- [6]Ducat L, Ogloff JR, McEwan T Mental illness and psychiatric treatment amongst firesetters, other offenders and the general community Aust N Z J Psychiatry, 2013.PMID 23739314
- [7]Grant JE, Won Kim S Clinical characteristics and psychiatric comorbidity of pyromania J Clin Psychiatry, 2007.PMID 18052565
- [8]Gannon TA, Ciardha CÓ, Barnoux MF, et al. Male imprisoned firesetters have different characteristics than other imprisoned offenders and require specialist treatment Psychiatry, 2013.PMID 24299093
- [9]Gannon TA, Alleyne E, Butler H, et al. Specialist group therapy for psychological factors associated with firesetting: Evidence of a treatment effect from a non-randomized trial with male prisoners Behav Res Ther, 2015.PMID 26248329
- [10]Tyler N, Gannon TA, Lockerbie L, et al. An evaluation of a specialist firesetting treatment programme for male and female mentally disordered offenders (the FIP-MO) Clin Psychol Psychother, 2018.PMID 29282790
- [11]Tyler N, Gannon TA, Ciardha CÓ, et al. Deliberate firesetting: an international public health issue Lancet Public Health, 2019.PMID 31376854
- [12]Tyler N, Gannon TA, Sambrooks K Arson assessment and treatment: the need for an evidence-based approach Lancet Psychiatry, 2019.PMID 31544760
- [13]Brett A 'Kindling theory' in arson: how dangerous are firesetters? Aust N Z J Psychiatry, 2004.PMID 15209833
- [14]Lambie I, Ioane J, Randell I, et al. Offending behaviours of child and adolescent firesetters over a 10-year follow-up J Child Psychol Psychiatry, 2013.PMID 23927002
- [15]American Academy of Psychiatry and the Law AAPL Practice Guideline for forensic psychiatric evaluation of defendants raising the insanity defense J Am Acad Psychiatry Law, 2014.PMID 25492121
- [16]Fazel S, Singh JP, Doll H, et al. Use of risk assessment instruments to predict violence and antisocial behaviour in 73 samples involving 24 827 people: systematic review and meta-analysis BMJ, 2012.PMID 22833604