Psych · Forensic psychiatry — civil
Civil forensic psychiatry
Also known as Civil forensic psychiatry · Medico-legal psychiatry civil · Testamentary capacity · Financial capacity · Psychiatric disability evaluation · Independent medical examination psychiatry · Fitness for work psychiatry · Fitness for duty psychiatry · Personal injury psychiatry · Guardianship assessment psychiatry
Exam-exhaustive fellowship reference on civil forensic psychiatry: testamentary and financial capacity (Banks v Goodfellow principles; functional domains), guardianship and substitute decision-making principles, personal-injury and psychiatric disability evaluation (AAPL disability guideline), fitness for work/duty, symptom validity, dual-role ethics, and civil report structure. Jurisdiction principles only — no invented statute section numbers. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
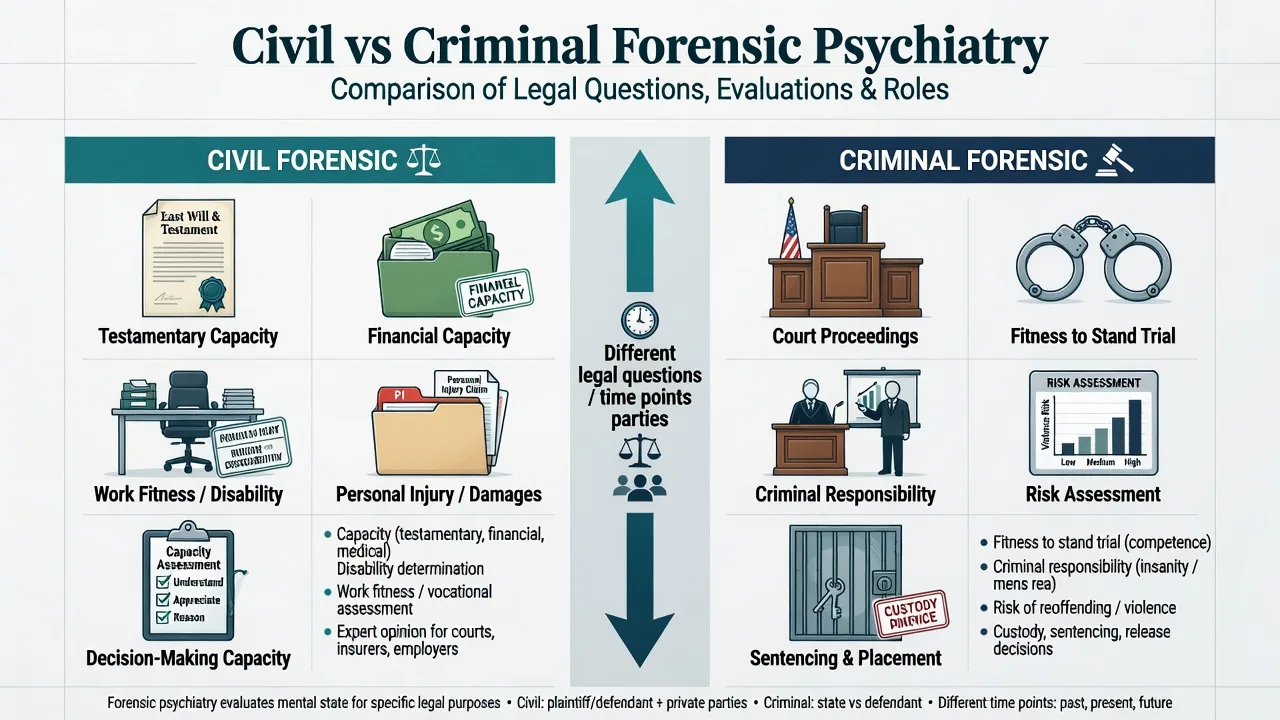
Civil forensic psychiatry is the psychiatric contribution to civil legal processes: wills and estates, financial management and contracts, guardianship and enduring powers, personal injury and workers-compensation claims, insurance disability, and occupational fitness assessments.[1][2][6] It is distinct from criminal forensic work (fitness to stand trial, criminal responsibility, violence risk in justice settings), though the same doctor may do both and the same illness can raise both civil and criminal questions in different briefs.[1][6]
The clinician’s product is usually an expert opinion for a court, tribunal, insurer, employer, or lawyer — not a treatment plan. Role clarity, neutrality, source transparency, and criterion-linked opinions are the professional core.[3][6]
Classification of civil domains
| Domain | Core legal question (principle) | Typical product |
|---|---|---|
| Testamentary capacity | Could the person make a valid will at the material time? | Concurrent or retrospective capacity opinion |
| Financial / contractual capacity | Can the person manage money / enter this transaction? | Functional capacity opinion |
| Guardianship / substitute decisions | Is substitute decision-making needed for defined domains? | Domain-specific capacity + supports |
| Treatment capacity (civil interface) | Can the person decide on this treatment now? | Decision-specific capacity (MacCAT-T adjunct) |
| Personal injury / psychiatric disability | Diagnosis, causation, impairment, function | IME / expert report |
| Fitness for work / duty | Can this person safely/effectively do this job? | Fitness opinion ± restrictions |
| Family-law interface | Parenting capacity / risk to children (high-level) | Jurisdiction-specific; do not invent statutes |
Statutes, tribunal procedures, impairment schedules, and workers-compensation schemes are jurisdiction-specific. In exams and reports, state principles, name the local framework if known, and do not invent section numbers or universal percentage tables.[1][4][5]
Epidemiology and system context
Ageing populations drive rising demand for testamentary and financial capacity work; dementia is the dominant clinical driver of financial incapacity in the evidence base.[11][13] Personal-injury and disability evaluations are among the commonest civil psychiatric requests; reliability of psychiatric work-disability ratings is imperfect, which is why structured methods and transparent reasoning matter.[4][17]
Undue-influence risk clusters around older adults who are isolated, dependent, cognitively impaired, or subject to sudden will changes favouring a new caregiver or relative.[15]
Mechanisms: how illness impairs civil function
There is no single “civil capacity lesion.” Examiners want a mechanism map from syndrome to functional legal ability.[7][11][13]
| Clinical process | Testamentary impact | Financial / work impact |
|---|---|---|
| Amnestic dementia | May lose property inventory and beneficiary awareness | Bill-paying and asset tracking fail early |
| Frontotemporal / dysexecutive syndromes | Impulsive gifts; poor appreciation of claims | High scam/risk behaviour; overestimation of ability |
| Delirium | Fluctuating capacity; deathbed wills high risk | Acute mismanagement; reassess after recovery |
| Psychosis | Delusions may “poison” dispositions | Paranoid financial decisions; work disruption |
| Severe depression | Apathy, nihilism, undervaluation of self/estate | Reduced work capacity; may retain formal capacity |
| TBI / neurocognitive injury | Variable; often needs neuropsychology | Personal-injury core scenario |
Unwise ≠ incapacitated. A person may make a bad investment or an eccentric will and still meet capacity criteria if functional abilities are intact and not delusionally distorted.[7][21]
Clinical presentation and referral stems
Common stems include contested wills after death (retrospective testamentary opinion); living patients with mild cognitive impairment wanting a new will; bank or family concern about financial exploitation; independent medical examination (IME) after motor-vehicle collision for PTSD/depression; insurer requests for long-term psychiatric disability status; and employer requests for fitness for duty in safety-sensitive roles.[2][4][9]
Civil evaluees may arrive with incomplete records, attorney framing, secondary gain pressures, or genuine severe illness. Structure protects against both advocacy bias and cynical under-recognition of illness.[3][6][19]
Differential that examiners care about
- Fails functional legal criteria for this decision
- Time- and decision-specific
- May be reversible if cause treatable
- Meets criteria despite poor choice
- Autonomy preserved
- Do not substitute best interests for capacity
- External coercion/manipulation of will
- May coexist with capacity or incapacity
- Different legal theory from pure incapacity
Other discriminators include psychiatric injury related to an incident versus coincidental primary psychiatric illness (causation analysis); impairment (clinical loss) versus disability (functional/work impact) versus job-specific fitness; malingering or invalid responding versus genuine disorder with reduced effort secondary to pain, depression, or fatigue (validity tools inform but do not replace clinical-legal reasoning); and delirium versus dementia in end-of-life will changes.[4][5][16][18][19][22]
Assessment
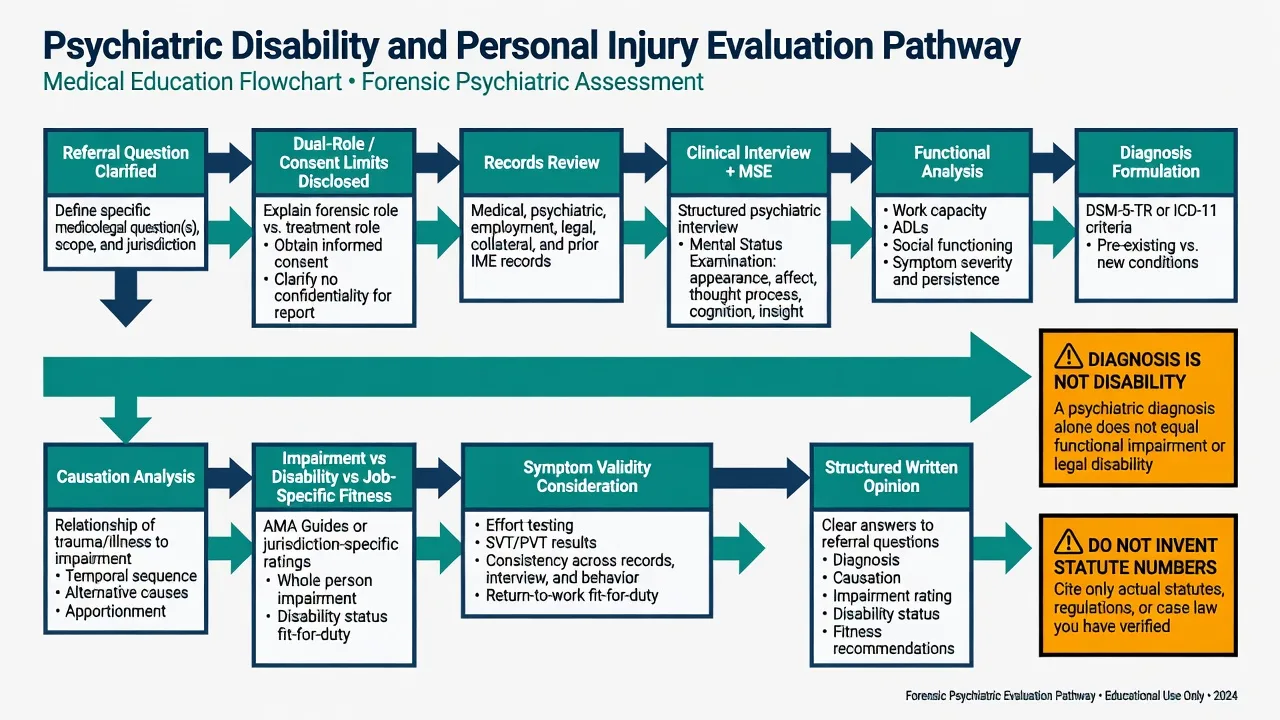
Universal civil forensic method
- Clarify the referral questions and the applicable legal standard for that jurisdiction (principles + local naming).[1][6]
- Identify the client (court, insurer, lawyer, employer) and explain limits of confidentiality and the non-therapeutic forensic role.[3][6]
- Gather sources: contemporaneous treating notes, imaging/labs when relevant, workplace files, prior claims, collateral, draft wills, bank/financial records as appropriate.[6][9]
- Interview + MSE with teach-back on the specific decision domains.[11][14]
- Functional analysis mapped to legal criteria (not diagnosis checklists alone).[4][21]
- Validity consideration when self-report drives disability/injury claims.[19]
- Opinion linked line-by-line to criteria; state limitations.[3][6]
Testamentary capacity
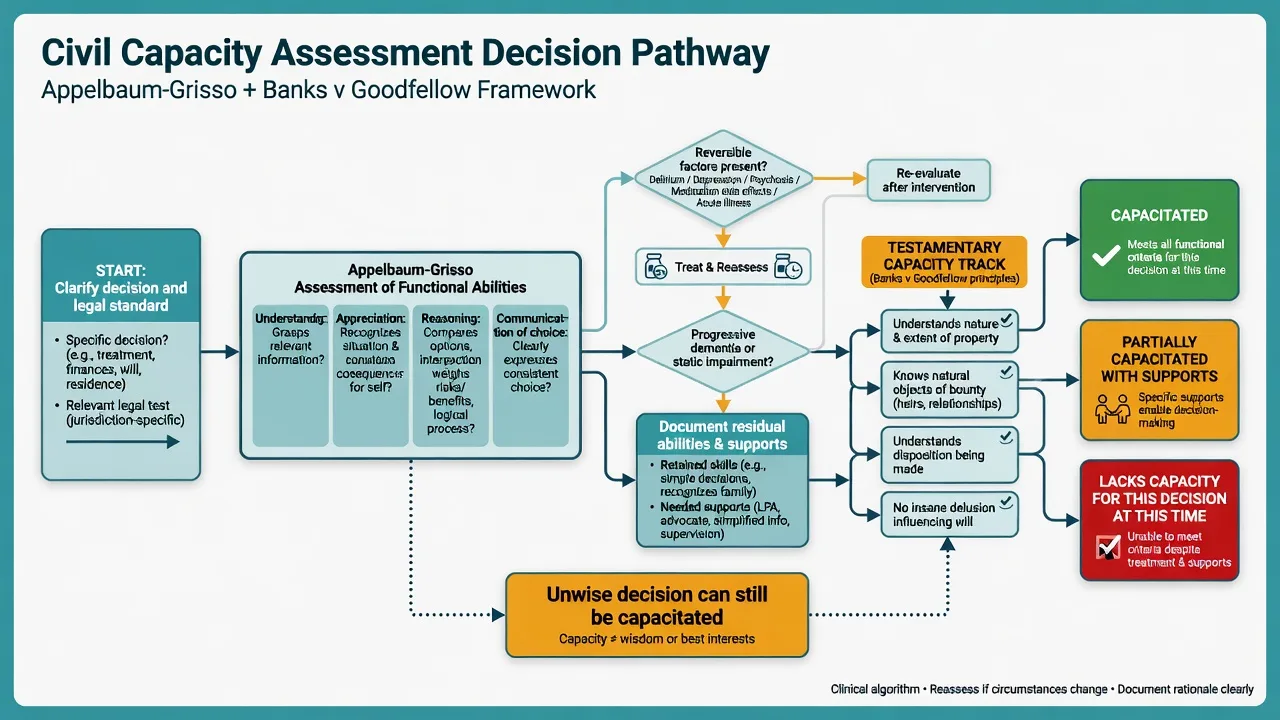
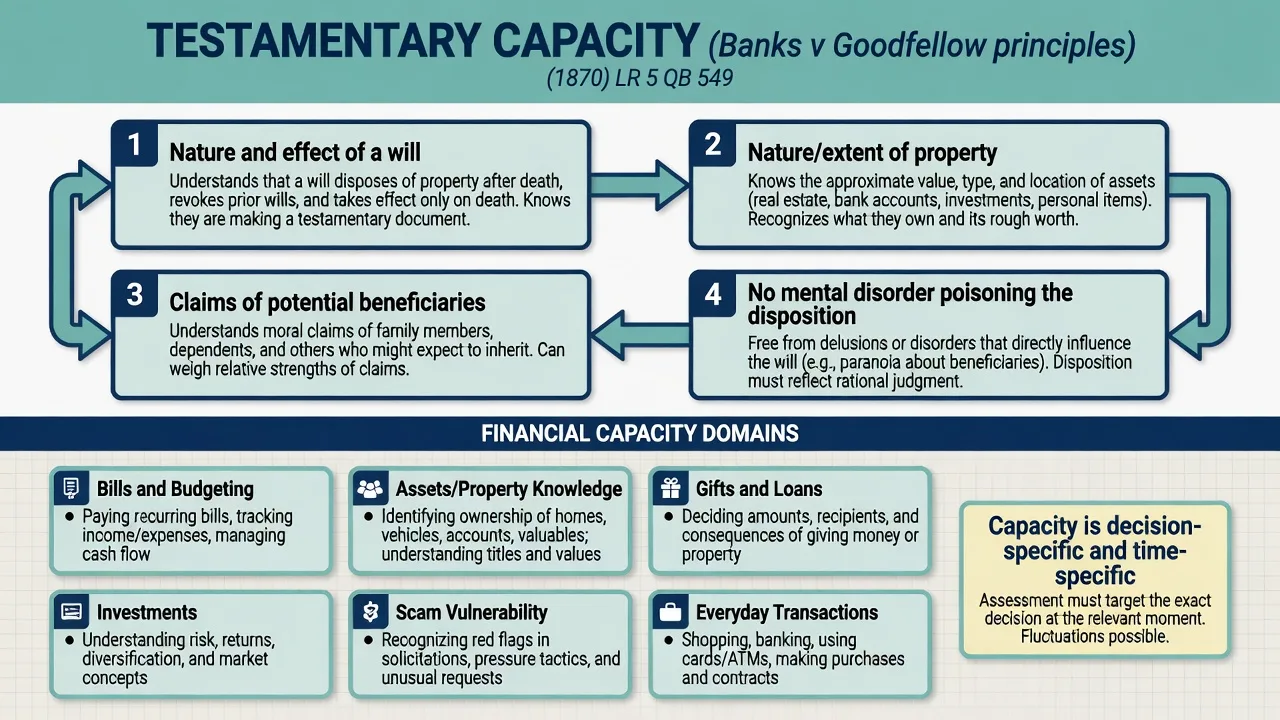
The classic common-law teaching framework is Banks v Goodfellow principles (recite cleanly in viva): (1) understand the nature and effect of a will; (2) understand the nature and extent of property (in broad terms); (3) comprehend and appreciate the claims of those who might expect to benefit; (4) not be affected by a disorder of mind that poisons the affections or influences the disposition (delusional distortion of the gift).[7][8][10][14]
Local statutory language may refine or restate these principles; do not invent local section numbers as if universal.[7][8]
Concurrent assessment (person alive, will being made now) allows interview, teach-back, and collateral. Retrospective assessment (will already made; capacity challenged after death) depends on reconstruction: contemporaneous medical notes, draft wills, solicitor observations, financial behaviour, timeline of cognitive change — Shulman and colleagues emphasise the expert’s structured historical method rather than speculative certainty.[9][14]
Deathbed wills require active exclusion of delirium and documentation of lucid intervals if claimed; fluctuation is the trap.[16]
Undue influence is a related but distinct construct: susceptibility (illness, dependence), opportunity, and unnatural transactions are clinical risk markers, not a legal verdict you invent.[12][15]
Financial capacity
Assess domain-by-domain: everyday transactions, bills/budgeting, asset knowledge, gifts/loans, investments, and vulnerability to scams/exploitation.[11][13] Dementia systematically erodes financial skills; executive and frontotemporal presentations may show risky behaviour with partial factual knowledge.[13] Instruments exist as adjuncts under a functional approach; they do not replace criterion-linked clinical opinion.[11]
Guardianship and substitute decision-making
Guardianship and related civil protective frameworks (enduring powers of attorney, supported decision-making) are jurisdiction-specific. Fellowship standard: assess domain-specific abilities (personal care, residence, finances, medical decisions), residual strengths, less-restrictive supports, and risks of harm/exploitation — not a global “incompetent” stamp based on diagnosis alone.[10][11]
Treatment capacity (civil interface)
For treatment decisions, the Appelbaum–Grisso functional abilities — understanding, appreciation, reasoning, expressing a choice — remain the research-backed teaching frame; MacCAT-T is a clinical tool, not a court verdict machine.[20][21] This is related to, but not identical with, testamentary or financial capacity.
Personal injury and psychiatric disability
AAPL guidance structures disability evaluation around clarifying the legal/insurance questions, comprehensive history and MSE, diagnosis, functional impairment, causation reasoning, and work capacity where asked — with explicit attention to role ethics and limits of expertise.[4][5] Personal-injury neuropsychiatric cases need timeline reconstruction, alternative causes, comorbidity, and often neuropsychology collaboration.[18]
Causation language is jurisdiction-specific (e.g. material contribution, but-for, aggravation of pre-existing illness). State clinical relationships carefully; do not invent local tort formulae as universal law.[4][18]
Work-disability psychiatric ratings show limited reproducibility when unstructured; improve reliability with defined functional criteria and transparent reasoning.[17]
Symptom and performance validity
In civil disability and injury contexts, structured validity assessment is a professional expectation when self-report is material. AACN consensus updates principles for effort, response bias, and malingering assessment in neuropsychological practice; psychiatric experts should know when to request formal testing and how to interpret patterns, not single cut-scores.[19] Tools such as SIRS/SIRS-2 are one class of structured interviews for feigned psychopathology — admissibility and use require training and context; they are not automatic “liar detectors.”[22]
Fitness for work and fitness for duty
Separate impairment (clinical findings), disability (activity/role limitation), and fitness for a specific job (match residual function to essential job demands and safety risks). Ask for a job demands analysis. Opinions may include fit / unfit / fit with restrictions / temporary unfitness with review date. Safety-sensitive roles (transport, weapons, healthcare procedures) raise public-protection stakes; still avoid inventing occupational statutes.[2][4][5]
Investigations and adjuncts
Useful adjuncts include cognitive screening and formal neuropsychology when capacity or injury claims turn on cognition or effort; medical work-up for delirium and metabolic, infectious, or neurological differentials; imaging/EEG when organic disease is plausible (supportive, not dispositive of legal capacity); collateral from family, solicitor, workplace, and treating teams; and financial records and will drafts in estate cases.[6][9][12][18]
Acute issues during civil assessment
For fluctuating capacity (delirium, mania), stabilise and reassess when feasible rather than freezing a single ambiguous snapshot as eternal truth.[16]
Definitive product: the civil forensic report
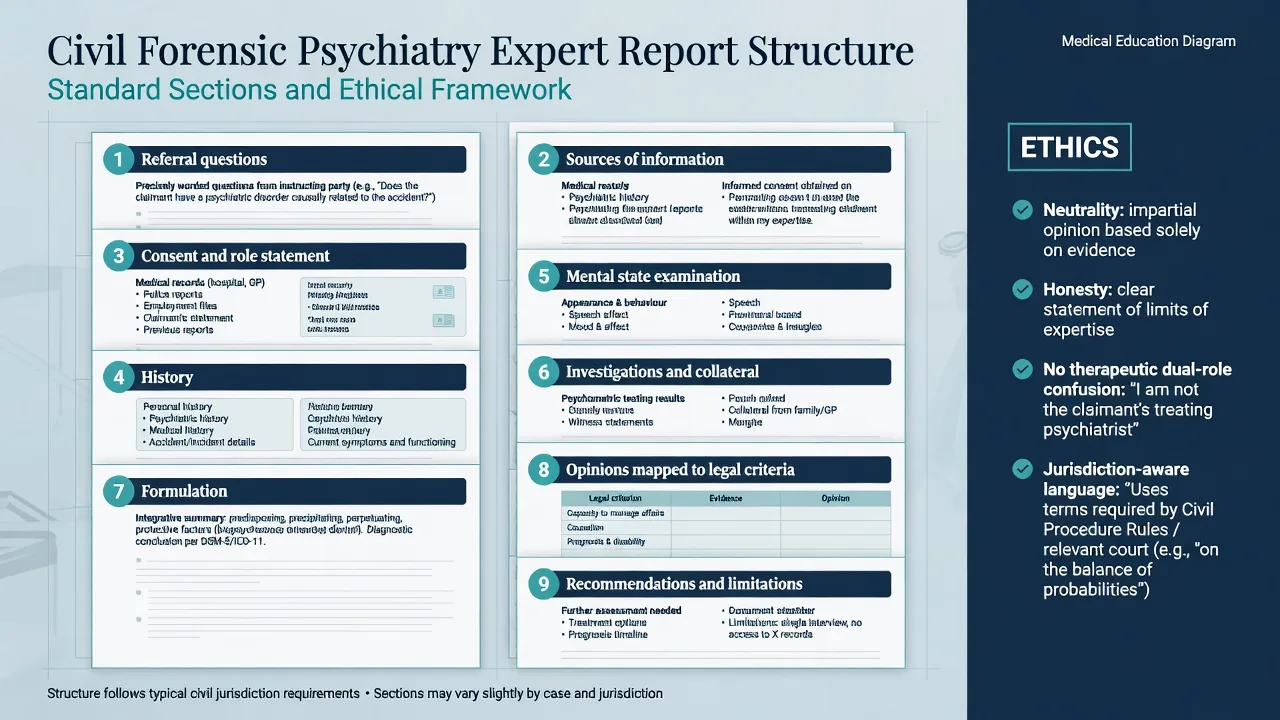
Recommended report structure (adapt to local court/tribunal expectations): referral questions and instructing party; sources of information (and gaps); role statement and consent/limits of confidentiality; history (psychiatric, medical, occupational, incident, legal); mental state examination with quoted material content; investigations and collateral; formulation including differential and validity issues; opinions mapped to each legal criterion / referral question; recommendations (treatment only if appropriate to brief), prognosis, and reassessment interval; and limitations plus any local declaration of truthfulness/impartiality.[3][4][6]
Practical practice issues
Samuels’ Australasian series emphasises overview, specific civil issues, and the practicalities of medico-legal practice (brief quality, fees, boundaries, quality control) — useful FRANZCP-region framing without replacing primary legal advice.[1][2][3]
Subtypes and high-yield scenarios
| Scenario | Examiner focus |
|---|---|
| Mild dementia + new will | Domain testing; document residual capacity; contemporaneous notes gold standard |
| Retrospective contested will | Reconstruction method; avoid false certainty; name missing data |
| Deathbed will | Delirium first; lucid interval documentation |
| Suspected undue influence | Risk factors; capacity still assessed separately |
| PTSD after collision | Diagnosis thresholds; causation; function; validity |
| Long-term depression disability claim | Course, treatment adequacy, function, secondary gain without pejorative over-call |
| Safety-sensitive fitness for duty | Job demands, risk, restrictions, review |
| Intellectual disability + finances | Supported decision-making; adaptive skills not IQ alone |
Complications and pitfalls
- Diagnosis = incapacity / disability fallacy
- Invented statutes and “standard” whole-person impairment percentages stated as universal law
- Dual-role blur (treating doctor as undeclared advocate-expert)
- Hired-gun bias and selective data use
- Ignoring validity assessment in high-stakes self-report claims
- Instrument cut-score justice
- Retrospective speculation without records
- Confusing impairment, disability, and job fitness
- Answering questions not asked; refusing to answer questions that were asked
- Ethnocentric capacity judgements without interpreter/cultural formulation
Prognosis and disposition
Capacity may recover with treatment of depression, psychosis, or delirium; progressive neurodegenerative disease often predicts declining financial and complex decision capacity.[13][16][21] Work disability trajectories depend on diagnosis, comorbidity, workplace factors, treatment access, and sometimes litigation context.[4][17] State reassessment intervals for fluctuating or treatment-responsive conditions. Report release pathways and confidentiality rules are jurisdiction-specific.[3][6]
Special populations
- Older adults: dementia spectrum, polypharmacy, delirium, undue influence, deathbed wills
- Intellectual disability: adaptive function, supported decision-making, avoid IQ cut-off myths
- Cultural/linguistic diversity: use skilled interpreters; property and kinship concepts may be culturally structured
- Indigenous contexts: culturally safe assessment; avoid imposing majority-culture “rationality” templates without understanding
- Neuropsychiatric injury: TBI, stroke, FTD — collaborate with neurology/neuropsychology
Evidence and guidelines
| Anchor | Use in exams |
|---|---|
| AAPL Psychiatric Disability Guideline/Resource (Gold 2008; Anfang 2018) | Structure of disability/IME opinions |
| AAPL Forensic Assessment Guideline (Glancy 2015) | General forensic method and ethics of assessment |
| Samuels civil forensic Parts 1–3 (2018) | ANZ overview, specific issues, practice logistics |
| Testamentary capacity reviews (Aravind 2024; Jakubek/Shulman 2025) | Modern synthesis of TC methods |
| Shulman/Peisah IPG literature | Concurrent/retrospective TC; undue influence; delirium |
| Appelbaum–Grisso / MacCAT-T | Functional civil/treatment capacity abilities |
| AACN 2021 validity consensus | Effort/response bias principles |
| Kunz 2019 | Work-disability rating reliability caution |
Regional notes
ANZ (FRANZCP primary): Use Samuels’ civil forensic series as a regional teaching scaffold; apply local guardianship, succession, workers-compensation, and civil procedure frameworks by principle without inventing section numbers. Banks v Goodfellow principles remain common viva language for wills across common-law teaching.[1][2][7]
UK/MRCPsych: Mental capacity frameworks for decisions (treatment, welfare, property) are statutory and jurisdiction-specific (England and Wales frameworks differ from Scotland/NI). Testamentary capacity remains heavily common-law influenced in teaching. State principles; do not invent Act sections in global answers.[7][21]
US/ABPN: AAPL disability and forensic assessment guidelines are high-yield. Disability systems (SSDI, workers’ compensation, tort) differ by forum. Fitness for duty common in occupational contexts.[4][5][6]
India/MD-DNB/NEET-SS: Civil capacity, certification, and disability contexts are statute- and board-specific; answer with functional principles and local naming only when known.[1][10]
Exam pearls
CIVIL-CAP (civil capacity checklist)
Self-check
If you can only remember five lines for the exam: civil ≠ criminal (different questions, parties, products); capacity is functional, decision- and time-specific (diagnosis alone never decides); Banks v Goodfellow principles for wills and Appelbaum–Grisso abilities for many civil decisions; disability/IME needs diagnosis + function + causation + validity + job fit when asked; structured report, clean ethics, and no invented statutes.[1][4][7][21]
References
- [1]Samuels AH Civil forensic psychiatry - Part 1: an overview Australas Psychiatry, 2018.PMID 29400548
- [2]Samuels AH Civil forensic psychiatry - Part 2: specific issues Australas Psychiatry, 2018.PMID 29457475
- [3]Samuels AH Civil Forensic Psychiatry - part 3: practical aspects of managing a medico-legal practice Australas Psychiatry, 2018.PMID 29457467
- [4]Gold LH, Anfang SA, Drukteinis AM, et al. AAPL Practice Guideline for the Forensic Evaluation of Psychiatric Disability J Am Acad Psychiatry Law, 2008.PMID 19092058
- [5]Anfang SA, Gold LH, Meyer DJ AAPL Practice Resource for the Forensic Evaluation of Psychiatric Disability J Am Acad Psychiatry Law, 2018.PMID 29752290
- [6]Glancy GD, Ash P, Bath EP, et al. AAPL Practice Guideline for the Forensic Assessment J Am Acad Psychiatry Law, 2015.PMID 26054704
- [7]Aravind H, Taylor M, Gill N Evaluation of testamentary capacity: A systematic review Int J Law Psychiatry, 2024.PMID 38422563
- [8]Jakubek A, Montag T, Hull IM, et al. The Medico-Legal Approach to the Assessment of Testamentary Capacity: A Systematic Review Am J Geriatr Psychiatry, 2025.PMID 39690101
- [9]Shulman K, Herrmann N, Peglar H, et al. The Role of the Medical Expert in the Retrospective Assessment of Testamentary Capacity Can J Psychiatry, 2021.PMID 32233933
- [10]Roof JG Testamentary capacity and guardianship assessments Psychiatr Clin North Am, 2012.PMID 23107570
- [11]Sousa LB, Simões MR, Firmino H, et al. Financial and testamentary capacity evaluations: procedures and assessment instruments underneath a functional approach Int Psychogeriatr, 2014.PMID 24229806
- [12]Mart EG Neuropsychological Assessment of Testamentary Capacity and Undue Influence Arch Clin Neuropsychol, 2016.PMID 27480988
- [13]Sudo FK, Laks J Financial capacity in dementia: a systematic review Aging Ment Health, 2017.PMID 27647045
- [14]Shulman KI, Peisah C, Jacoby R, et al. Contemporaneous assessment of testamentary capacity Int Psychogeriatr, 2009.PMID 19323871
- [15]Peisah C, Finkel S, Shulman K, et al. The wills of older people: risk factors for undue influence Int Psychogeriatr, 2009.PMID 19040788
- [16]Liptzin B, Peisah C, Shulman K, et al. Testamentary capacity and delirium Int Psychogeriatr, 2010.PMID 20594383
- [17]Kunz R, von Allmen DY, Marelli R, et al. The reproducibility of psychiatric evaluations of work disability: two reliability and agreement studies BMC Psychiatry, 2019.PMID 31266488
- [18]Ciccone JR, Fisher J, Jones JCW Forensic neuropsychiatric evaluation of a personal injury case Behav Sci Law, 2024.PMID 38145476
- [19]Sweet JJ, Heilbronner RL, Morgan JE, et al. American Academy of Clinical Neuropsychology (AACN) 2021 consensus statement on validity assessment Clin Neuropsychol, 2021.PMID 33823750
- [20]Grisso T, Appelbaum PS, Hill-Fotouhi C The MacCAT-T: a clinical tool to assess patients' capacities to make treatment decisions Psychiatr Serv, 1997.PMID 9355168
- [21]Grisso T, Appelbaum PS Comparison of standards for assessing patients' capacities to make treatment decisions Am J Psychiatry, 1995.PMID 7793439
- [22]Wygant DB, Tylicki JL, Disney LF, et al. Structured Interview of Reported Symptoms-2nd Edition (SIRS-2): Use and Admissibility in Forensic Mental Health Assessment J Pers Assess, 2022.PMID 34871131