Psych · Forensic psychiatry — duty to warn and third-party risk
Duty to warn and third-party risk
Also known as Tarasoff duty · Duty to protect · Duty to warn · Third-party violence risk disclosure · Confidentiality exceptions psychiatry · Protective disclosure · Tarasoff warning · Identifiable victim threat
Exam-exhaustive fellowship reference on Tarasoff principles, duty to warn versus duty to protect, limits of confidentiality when third parties are at serious risk, Appelbaum assessment-action-implementation model, protective options including treatment and containment, minimum necessary disclosure, documentation, alliance repair, and jurisdiction variation without inventing statutes. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
8 MCQs with explanations
Target exams
Red flags
Overview and definition
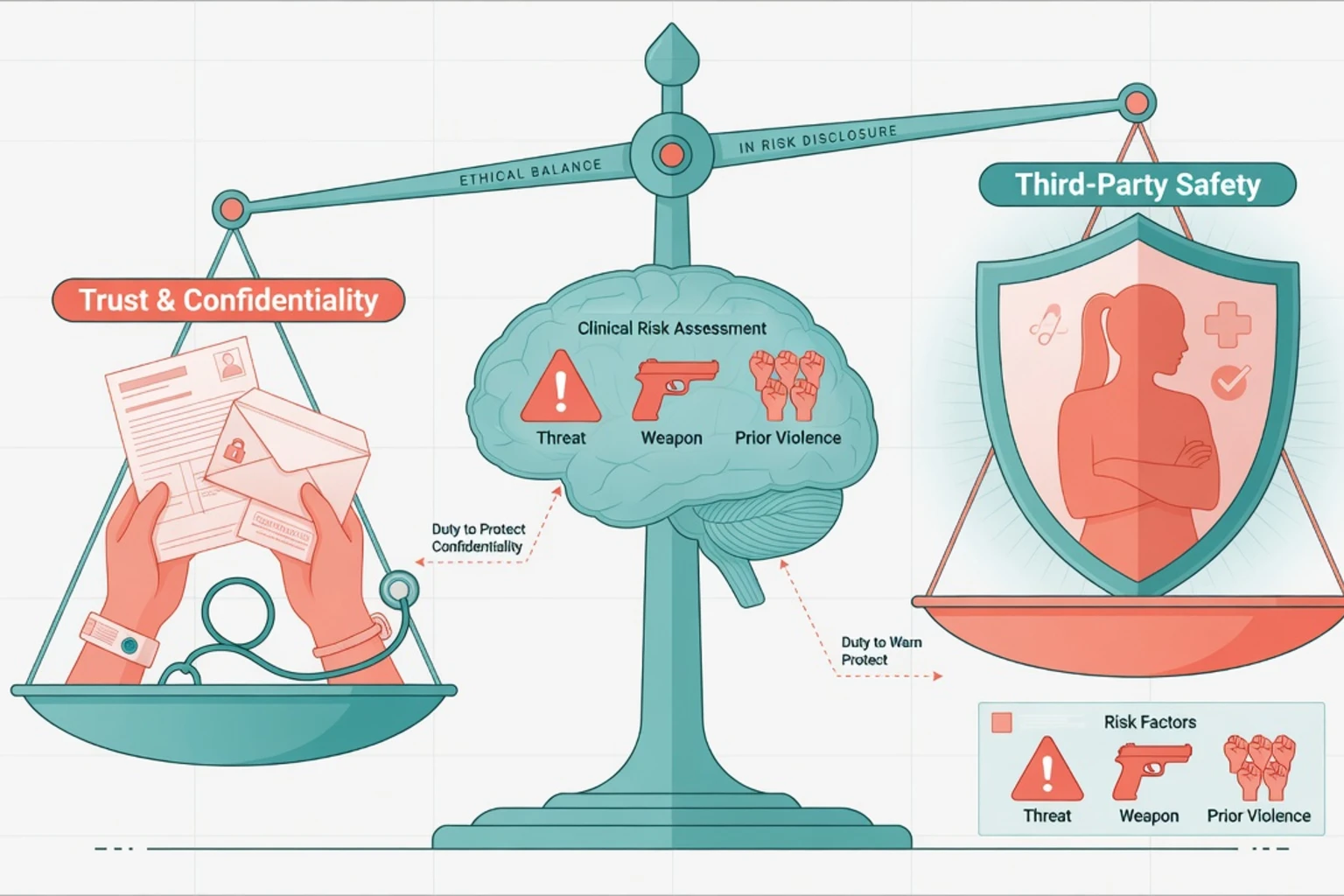
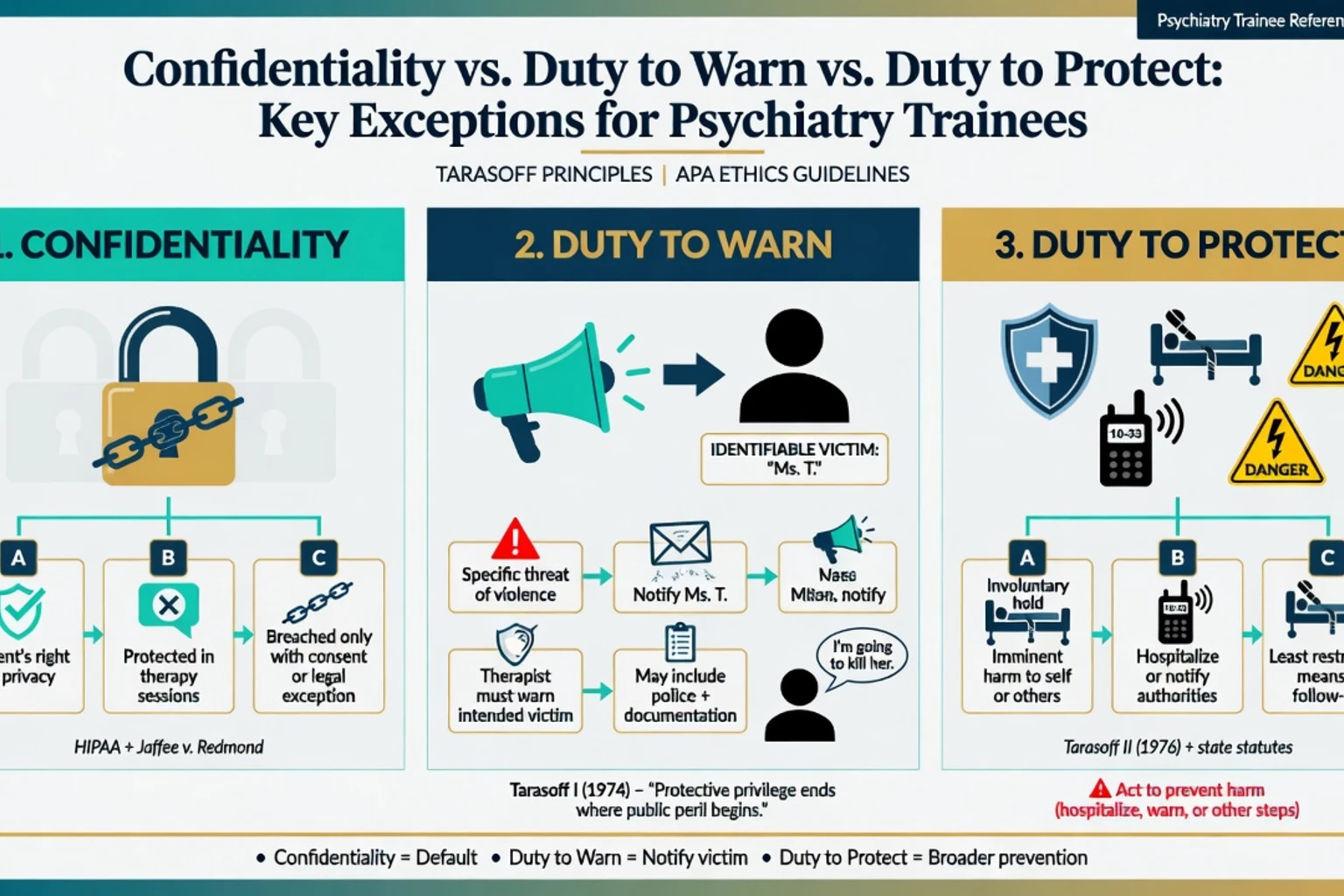
Confidentiality underpins psychiatric care: patients disclose dangerous thoughts because they expect restraint in further disclosure. That expectation has limits. Serious, foreseeable harm to others can create ethical and (in many places) legal pressure to protect non-patients — the classic third-party risk problem crystallised by Tarasoff v. Regents of the University of California.[2][3][13]
Duty to warn means notifying a potential victim (and often police) of a threat. Duty to protect is broader: take reasonable precautions to prevent harm. Warning is one option among several; hospitalisation, increased supervision, weapons restriction, and targeted treatment can discharge the protective obligation even when a direct warning is not the first or only step. California's own statutory and case trajectory illustrates that the exact label (warn vs protect) and required acts can shift over time within one jurisdiction.[1][5][6]
Jurisdiction caution (non-negotiable). US states differ: some codify mandatory duties, some permit disclosure, some case law finds no private duty to warn/protect in certain formulations (classic Texas discussion). Outside the US, candidates must not export California case names as if they are local statutes. Australia, New Zealand, UK nations, Canada, and India organise third-party protection through combinations of professional ethics (including RANZCP Code of Ethics rare-breach principles for safety of the patient or others), privacy legislation exceptions, mandatory reporting schemes (child protection and other local duties), mental health acts, and negligence doctrines. Teach principles; verify local law and organisational policy before acting; never invent section numbers in exams or practice notes.[7][8][11][12]
Classification — confidentiality, warn, protect

- Default: no disclosure without consent
- Builds alliance and accurate history
- Exceptions are narrow and justified
- Explain limits at intake
- Notify identifiable victim
- Often notify police as well
- Classic Tarasoff I language
- May be mandatory or permissive locally
- Broader Tarasoff II principle
- Warn, hospitalise, treat, contain
- Reasonable steps standard
- Document options considered
Related but distinct disclosure frameworks
Do not collapse every reporting duty into "Tarasoff". Related frameworks include child protection and elder abuse (often mandatory reporting), notifiable diseases and public health pathways, fitness-to-drive or firearms reporting, and infectious-disease partner notification (e.g. some HIV contexts) — each with distinct ethical-legal literature and thresholds; do not assume they are identical to interpersonal violence duties.[13][14][15]
Operational threat taxonomy
| Category | Typical features | Protective implication |
|---|---|---|
| Credible, specific, imminent | Named victim, plan, means, access, short time horizon | High acuity: contain now; disclosure often concurrent |
| Serious but not immediate | Clear intent, planned future act, victim known | Structured plan; may warn/protect under local rules |
| Non-specific anger | Diffuse rage, no target, no plan | Treat/risk-manage; disclosure usually not indicated |
| Fantasy / venting | Metaphorical language, no intent | Clarify meaning; do not over-disclose |
| Historical only | Past threat, current low dynamic risk | Review triggers; not automatic current disclosure |
Epidemiology and risk context
Tarasoff-type situations are low frequency, high consequence. Most patients with schizophrenia never commit serious interpersonal violence; relative risk is elevated in meta-analysis, especially with substance use and certain symptom patterns, but absolute risk remains low for most individuals. Prior violence remains a powerful historical marker; dynamic factors (active threats, intoxication, untreated psychosis, victim access) drive when protective action is urgent.[19][21][16]
Risk assessment tools offer only moderate group-level predictive accuracy and do not replace a decision about whether this patient, this target, and this context require protective disclosure or containment.[18][17]
System learning after rare tragedies (e.g. homicide inquiries involving psychiatric patients in New Zealand analyses) emphasises consistent method and communication failures more than a fantasy that every threat was "obvious" in retrospect.[20]
Mechanisms — ethics and clinical drivers
Ethical collision
- Autonomy / fidelity: respect privacy and keep promises of confidentiality.
- Non-maleficence / beneficence: prevent serious harm to identifiable others; also avoid unnecessary harm from over-disclosure.
- Justice: apply protective powers fairly without stigmatising whole diagnostic groups.
- Public trust: poorly handled breaches can deter help-seeking; well-handled, minimal, explained breaches can preserve both safety and longer-term engagement.[3][13][14]
Clinical pathways to third-party harm
Psychosis (persecutory delusions, command hallucinations, delusional jealousy), mania with grandiosity and disinhibition, intoxication or withdrawal, personality-driven revenge and stalking, and cognitive impairment with misidentification can all produce third-party risk — via different mechanisms. Pathway matters for which protective step works (antipsychotic and hospitalisation vs substance detox vs security measures vs domestic-violence multi-agency work).[19][21][16]
Clinical presentation
Classic exam stem. Outpatient in psychotherapy names a former partner, describes a plan, has access, and asks you to keep it secret. Or: inpatient on leave planning to attack a neighbour who "poisoned" him. Or: community patient fixated on a workplace supervisor with weapons talk.[1][6]
MSE signals. Hostility directed at a person; rehearsal language; calm certainty about killing; psychotic conviction that harm is justified; intoxication reducing control; lack of future orientation after the act.[1][16]
Collateral. Family reports stalking; police call about threats; victim messages the team; prior intimate-partner violence orders.[6][15]
Retraction. Patients often minimise once consequences appear. Retraction is data, not a magic wand — reassess intent, means, and access.[1][4][6]
Differential diagnosis of the disclosure decision
Discriminators include specific threat versus venting (who, what, when, how); identifiable victim versus society-at-large (general rage may not meet classic warn criteria, though hospitalisation may still be indicated); third-party violence versus suicide-only pathways; treating clinician versus forensic evaluator dual-role limits; and child or elder harm, which may trigger separate mandatory reporting even without a classic Tarasoff analysis.[13][14][15][1]
Assessment
Appelbaum three-part model (exam gold)
- Assess whether the patient poses a serious danger of violence.
- Select a reasonable course of action to protect potential victims.
- Implement that course and document reasoning, actions, and notifications.[1]
This model remains the cleanest viva structure decades after Tarasoff debates matured.[2][6]
Practical threat interview
- Content: exact words; identity of target; relationship; plan; timing; location; weapons; transportation; prior approaches to victim.
- Intent and inhibitors: wish vs intention; ambivalence; moral restraints; fear of consequences; protective relationships.
- Capacity for control: intoxication, impulsivity, command hallucinations, manic drive.
- Access: shared housing, school/work overlap, social media stalking, leave status.
- History: prior violence, breaches of orders, supervision failures.
- Collateral: family, other clinicians, police (within lawful channels), prior notes.
- Parallel suicide/self-harm assessment — dual risks commonly co-travel.[16][17][21]
Risk communication
Prefer scenarios ("If X and Y, then risk of assault on Z rises") over a lone "medium risk" label. SPJ-style communication improves actionability for teams and external partners.[22][17]
Informed limits at intake
Advise patients early that confidentiality has exceptions when there is serious risk of harm to self or others (worded per local policy and code). Surprise only at the moment of crisis worsens alliance rupture.[13][3]
Investigations and information gathering
- Records: prior threats, admissions, weapons mentions, DV history.
- Toxicology when substances drive disinhibition.
- Organic work-up if delirium, encephalitis, or new cognitive change is in differential.
- Lawful information-sharing with police/crisis services when imminence demands it.
- Do not delay obvious protective action solely to complete a perfect file review.[15][16]
Acute / emergency management
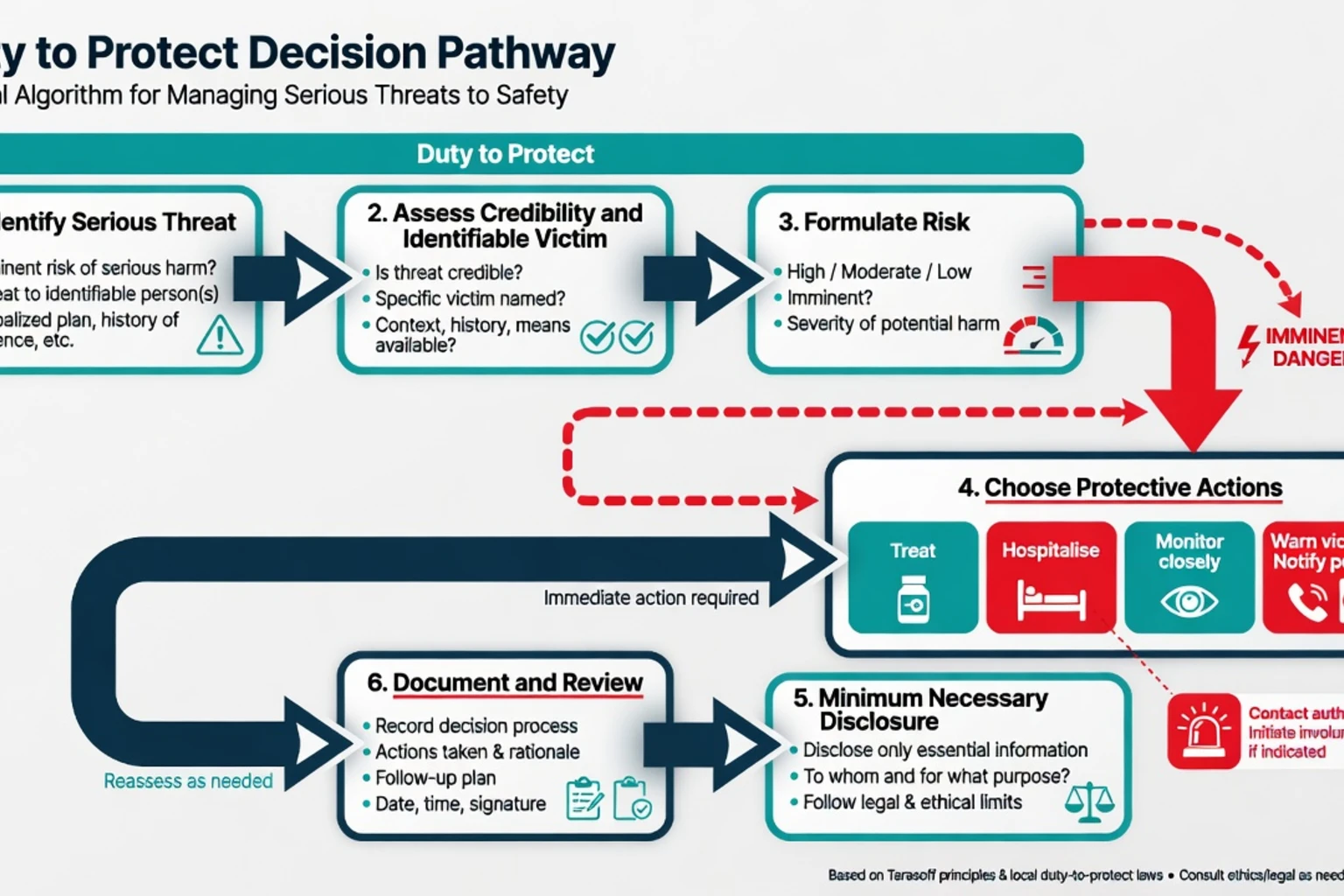
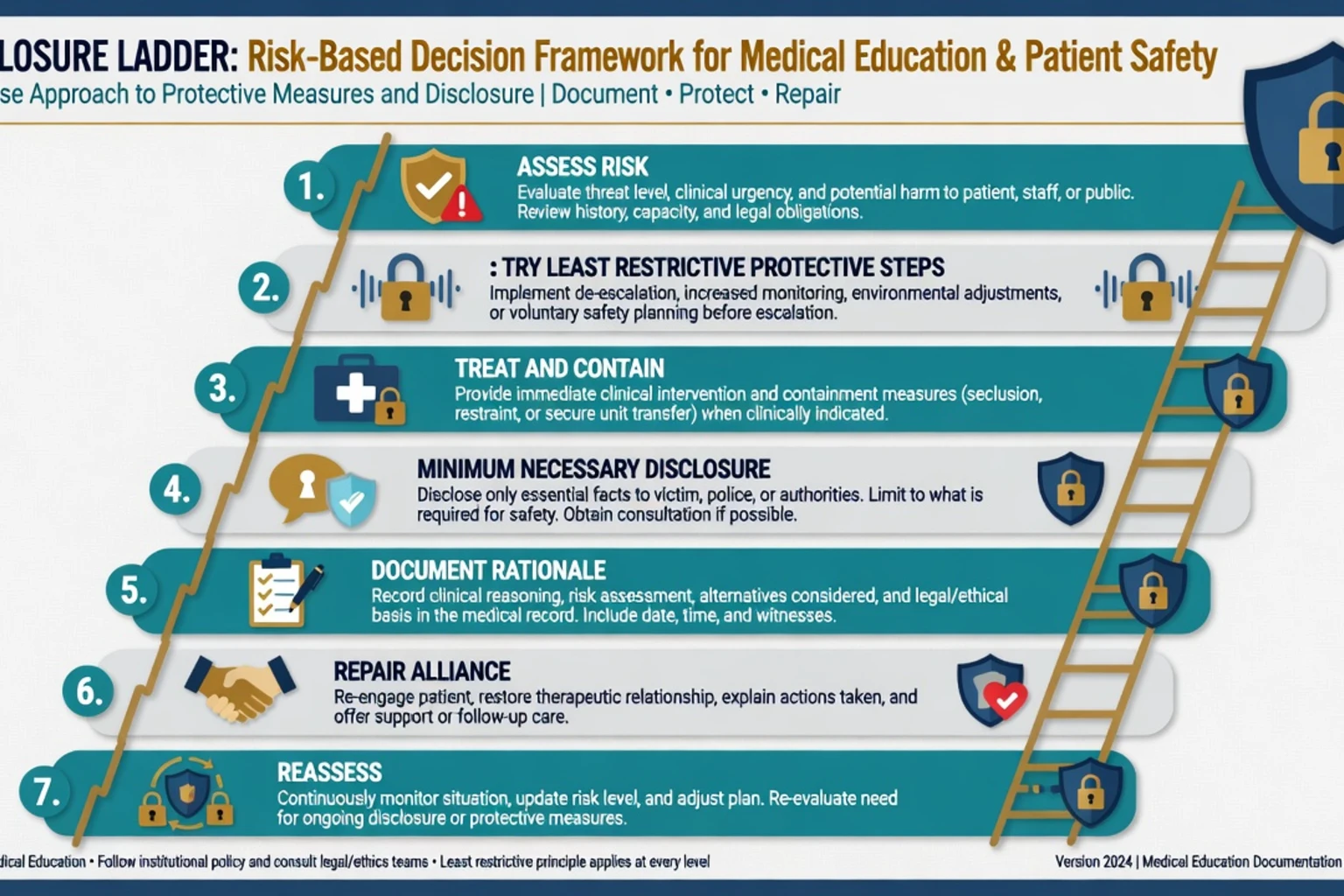
Immediate priorities: ensure safety of the interview setting and staff; prevent departure if imminence is high and lawful detention or observation options exist; reduce means (weapons, exit pathways) where possible; decide a protective package of treat plus contain with or without disclose; notify appropriate parties with minimum necessary information; and document contemporaneously.[1][6][15]
Hospitalisation. When mental illness is driving risk and community safety cannot be secured, seek voluntary admission first if safe; use local compulsory mental health powers when criteria met and less restrictive options fail. Do not invent section numbers — state criteria categories (mental disorder + risk + least restrictive alternative principles).[15][6]
Warning and police. When a reasonably identifiable victim is at serious risk and local law/ethics support or require disclosure, contact victim and/or police. Expect variable police responses; Guina and colleagues document law-enforcement experience with Tarasoff-type warnings and the need for clear, actionable communication.[4][10]
Definitive management and documentation
Protective options (often combined)
- Intensified outpatient contact and crisis plan
- Substance intervention and toxicology monitoring
- Medication optimisation (e.g. antipsychotic when psychosis-driven — choose agent/dose per clinical standards with monitoring; cite clinical context not Tarasoff itself for pharmacology)
- Restrict leave / increase observation in hospital
- Remove weapons access via lawful pathways
- Multi-agency public protection principles when community risk is sustained
- Warning victim; notifying police
- Temporary suspension of certain privileges (forensic leave) until risk reformulated[1][6][15]
Minimum necessary disclosure
Disclose what the recipient needs to stay safe: that a threat exists, nature/seriousness, who made it if required, and practical advice (e.g. contact police if approached). Avoid dumping psychotherapy process notes, sexual history, or irrelevant diagnoses.[4][13][14]
Effects of warning
Empirical work on Tarasoff warnings shows complex effects on victims and on the therapeutic relationship — warnings can be helpful for safety yet distressing; therapy may continue or rupture. Plan alliance repair: explain the legal/ethical duty, emphasise continued care, and separate the person from the dangerous act.[4]
Documentation checklist
Document exact threat language and time; assessment of credibility, means, access, and mental state; options considered (including less restrictive); legal or ethical basis consulted (policy, code, senior advice, local statute as verified); actions taken and times (who was called; what was said); plan for follow-up and escalation triggers; and supervision when complex. Unhelpful risk practices include vague labels without action, false precision, and failure to reassess after change — apply the same hygiene here.[17][22][1]
Subtypes and scenarios
- Inpatient threats to staff/patients — institutional security + clinical treat/contain; disclosure pathways internal and sometimes external.
- Public figure fixation — identifiability and "zone of danger" doctrines vary; protect steps still include treatment and law-enforcement liaison principles.
- Intimate partner violence / stalking — interface with DV services and local civil protection orders (local process; principles only).
- Forensic leave with named victim — victim access is a dynamic risk item; leave is a privilege contingent on safety planning.
- Substance-driven threats — reassess when sober; still protect during intoxication if imminence is high.
- Youth — parents/guardians, school safety, and child-protection frameworks may dominate.
- HIV/infectious third-party risk — related confidentiality literature; do not blindly map violence Tarasoff rules onto all infectious-disease scenarios.[13][14][15]
Complications and pitfalls
- Exporting California Tarasoff as universal statute
- Inventing section numbers
- Disclosing full records "to be safe"
- Warning without treating/containing when illness is driving risk
- Equating schizophrenia diagnosis with automatic third-party disclosure
- Ignoring weapons and victim access
- No documentation of alternatives considered
- Collapsing child-protection mandatory reporting into adult Tarasoff language without checking local law
- Over-relying on a single risk score for a disclosure decision
- Failing to reassess after retraction or after protective steps
Prognosis and disposition
Many acute threat crises settle with containment, treatment of driving illness, substance control, and practical separation from the target. Disposition spans intensive community support, voluntary admission, compulsory admission under local criteria, police involvement, and multi-agency plans. After disclosure, monitor alliance, reassess risk, and define step-down criteria (e.g. sustained absence of ideation, no access, stable treatment). Residual uncertainty is honest; zero-risk guarantees are not.[2][16][17]
Special populations
- Child and adolescent: mature-minor confidentiality vs parent notification; school threats; mandatory child-protection interfaces.
- Older adults: elder abuse reporting; cognitive impairment affecting intent language.
- Intellectual disability: concrete communication of threats; capacity supports; carer systems.
- Indigenous and culturally diverse communities: interpreters; culturally safe practice; still protect third parties when criteria met — culture is not a reason to ignore imminence.
- Custody/forensic: institutional threat protocols plus clinical duties; dual-agency communication.
- Perinatal: risk to partner or infant may engage child-protection as well as adult third-party analysis.
Evidence, guidelines, and regional deltas
Landmark US clinical literature: Appelbaum's practical model; Anfang and Appelbaum's multi-decade review; Soulier and colleagues on the duty-to-protect landscape; Johnson, Persad, and Sisti on interstate variation and training gaps; Binder and McNiel on real-world warnings; Knoll and Felthous clinical overviews; Guina and colleagues on police interface.[1][2][7][8][4][6][10][15]
Violence evidence (Fazel, Witt, Buchanan, Large, risk-instrument metas) informs how you assess risk quality — it does not write the legal duty for your postcode.[16][17][18][19][21]
Exam pearls
PROTECT third-party risk
- Confidentiality yields when essential to avert danger to others (Tarasoff policy principle).
- Diagnosis ≠ disclosure trigger; threat + clinical judgment + local duty does.
- Appelbaum: assess → choose action → implement/document.
- Minimum necessary information.
- Instruments moderate at group level — do not hide behind a score.
- Interstate and international variation is the point of multi-board exams — say so explicitly.
- Never invent jurisdiction statutes.
References
- [1]Appelbaum PS Tarasoff and the clinician: problems in fulfilling the duty to protect Am J Psychiatry, 1985.PMID 3976915
- [2]Anfang SA, Appelbaum PS Twenty years after Tarasoff: reviewing the duty to protect Harv Rev Psychiatry, 1996.PMID 9384976
- [3]Roth LH, Meisel A Dangerousness, confidentiality, and the duty to warn Am J Psychiatry, 1977.PMID 848576
- [4]Binder RL, McNiel DE Application of the Tarasoff ruling and its effect on the victim and the therapeutic relationship Psychiatr Serv, 1996.PMID 8916238
- [5]Weinstock R, Vari G, Leong GB, et al. Back to the past in California: a temporary retreat to a Tarasoff duty to warn J Am Acad Psychiatry Law, 2006.PMID 17185483
- [6]Knoll JL The psychiatrist's duty to protect CNS Spectr, 2015.PMID 25712614
- [7]Soulier MF, Maislen A, Beck JC Status of the psychiatric duty to protect, circa 2006 J Am Acad Psychiatry Law, 2010.PMID 21156904
- [8]Johnson R, Persad G, Sisti D The Tarasoff rule: the implications of interstate variation and gaps in professional training J Am Acad Psychiatry Law, 2014.PMID 25492073
- [9]Johnson R, Persad G, Sisti D The Tarasoff Rule: The Implications of Interstate Variation and Gaps in Professional Training Focus (Am Psychiatr Publ), 2019.PMID 32015727
- [10]Guina J, Dornfeld B, Pinals DA A 20-year follow-up survey of police officers' experience with Tarasoff warnings: How law enforcement reacts to clinicians' duty to protect Behav Sci Law, 2022.PMID 35195297
- [11]Scarano VR, Baily CM, Banfield JR The Texas Supreme Court speaks: mental health professionals have no duty to warn or protect third parties Tex Med, 2002.PMID 12448958
- [12]Boulos N, Mallela D, Felthous A Tarasoff in Missouri: The jurisprudence of a mental health provider's duty to warn and protect non-patients of potential risks from patients J Forensic Sci, 2023.PMID 37282852
- [13]Appel JM Trends in Confidentiality and Disclosure Focus (Am Psychiatr Publ), 2019.PMID 32047382
- [14]Bersoff DN Protecting victims of violent patients while protecting confidentiality Am Psychol, 2014.PMID 25046702
- [15]Felthous AR The clinician's duty to protect third parties Psychiatr Clin North Am, 1999.PMID 10083944
- [16]Buchanan A Risk of violence by psychiatric patients: beyond the "actuarial versus clinical" assessment debate Psychiatr Serv, 2008.PMID 18245161
- [17]Large MM, Ryan CJ, Nielssen OB Helpful and unhelpful risk assessment practices Psychiatr Serv, 2010.PMID 20439381
- [18]Fazel S, Singh JP, Doll H, et al. Use of risk assessment instruments to predict violence and antisocial behaviour in 73 samples involving 24 827 people: systematic review and meta-analysis BMJ, 2012.PMID 22833604
- [19]Fazel S, Gulati G, Linsell L, et al. Schizophrenia and violence: systematic review and meta-analysis PLoS Med, 2009.PMID 19668362
- [20]Simpson AI, Allnutt S, Chaplow D Inquiries into homicides and serious violence perpetrated by psychiatric patients in New Zealand: need for consistency of method and result analysis Aust N Z J Psychiatry, 2001.PMID 11437811
- [21]Witt K, van Dorn R, Fazel S Risk factors for violence in psychosis: systematic review and meta-regression analysis of 110 studies PLoS One, 2013.PMID 23418482
- [22]Storey JE, Watt KA, Hart SD An examination of violence risk communication in practice using a structured professional judgment framework Behav Sci Law, 2015.PMID 25615811