Psych · Forensic psychiatry — expert evidence
Expert evidence and forensic report writing
Also known as Expert evidence psychiatry · Forensic report writing · Psychiatric expert witness · Medico-legal report psychiatry · Forensic mental health assessment report · Expert testimony psychiatry · Independent medical examination report psychiatry · Court report forensic psychiatry
Exam-exhaustive fellowship reference on psychiatric expert evidence and forensic report writing: expert vs fact/treating roles, dual-role ethics, forensic assessment method (AAPL), structured report architecture, oral testimony and cross-examination, bias and reliability, ultimate-issue limits, and admissibility principles (Frye/Daubert-type teaching). Jurisdiction principles only — no invented statute section numbers. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Psychiatric expert evidence is the application of specialised psychiatric knowledge, skills, and methods to legal questions beyond ordinary experience — fitness, criminal responsibility, capacity, disability, risk, and related civil or criminal issues.[1][11] The expert is not a second advocate. In teaching and professional standards, the expert assists the trier of fact with transparent reasoning under an impartiality frame that many jurisdictions encode as a duty to the court or tribunal (exact wording is local).[8][9][11]
This topic is about the expert process and product: roles, ethics, assessment method, report architecture, testimony craft, bias, and quality. Substantive legal tests (Banks v Goodfellow principles, Dusky/Presser/Pritchard, M'Naghten-type limbs) live in sister forensic topics; here you learn how to write and defend expert work about them.[1][3]
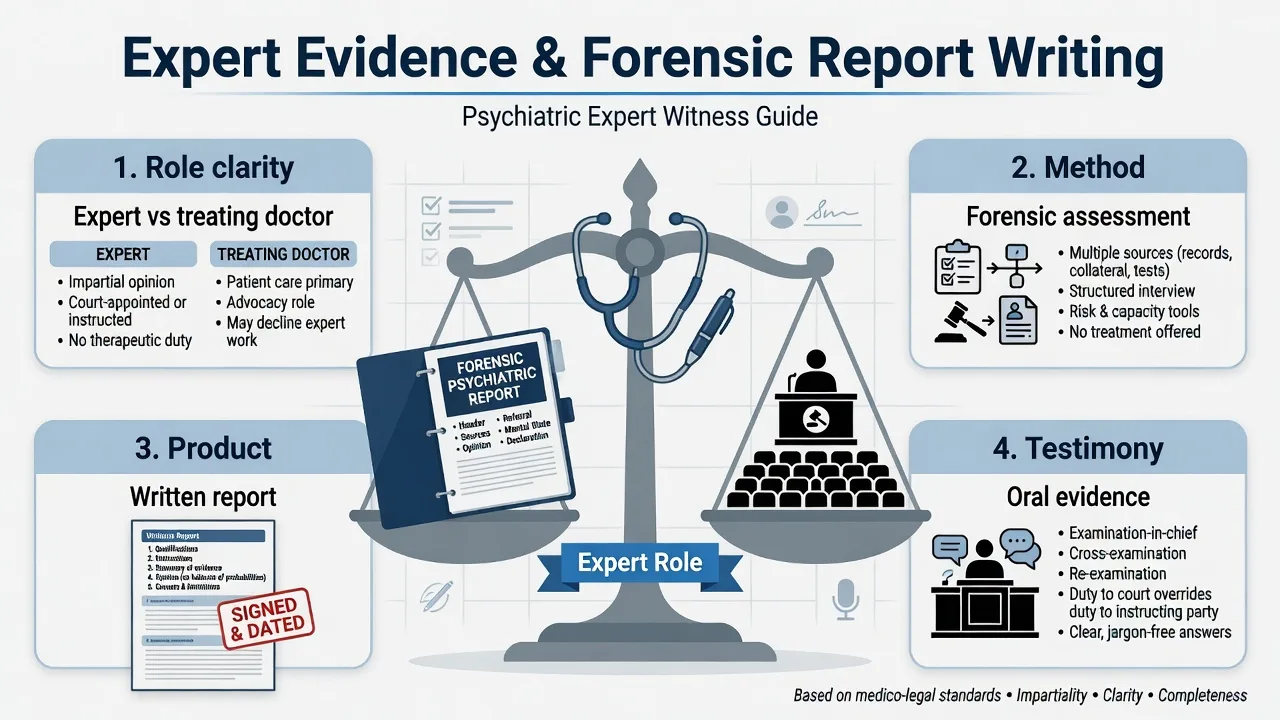
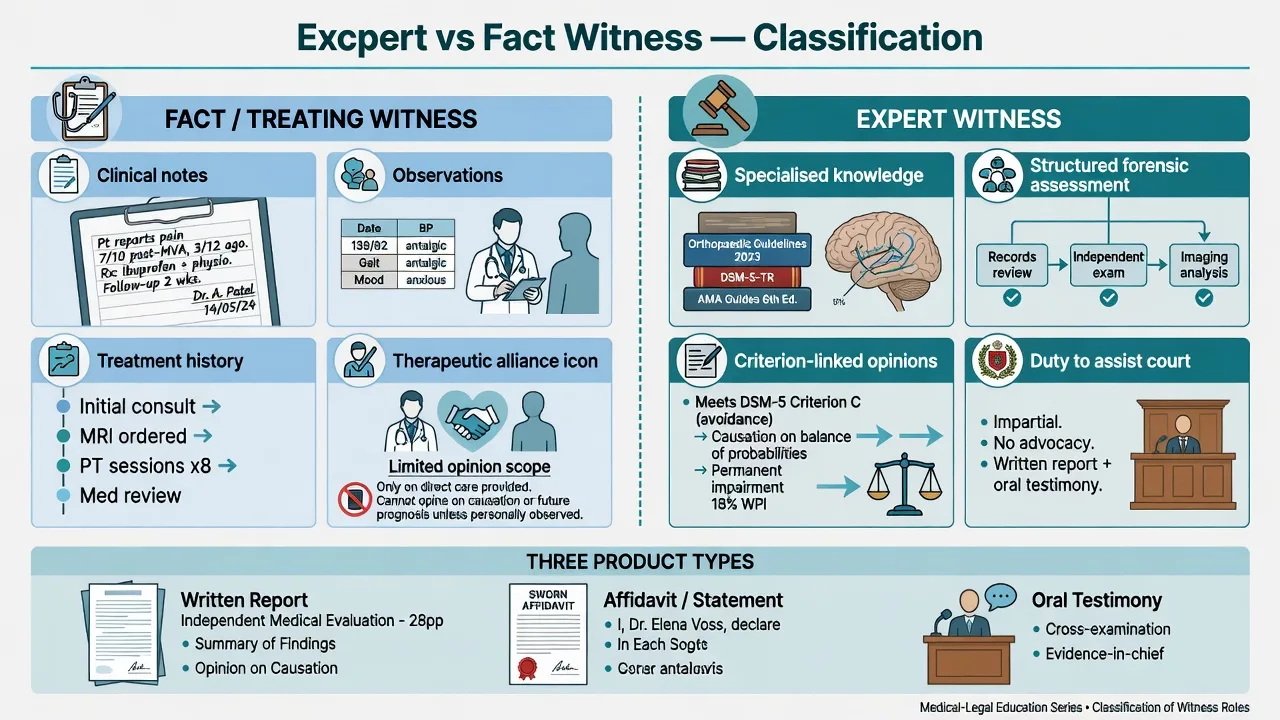
Expert vs fact (treating) witness
| Role | Typical content | Ethics frame |
|---|---|---|
| Fact / treating witness | What was observed, diagnosed, treated; contemporaneous notes | Therapeutic alliance; confidentiality defaults to clinical rules |
| Expert witness | Opinion answering legal referral questions using specialised methods | Non-therapeutic forensic role; disclosure of limits; impartiality |
| Hybrid risk | Treating doctor asked for “expert” opinion on contested ultimate questions | Dual-role conflict — disclose, limit, or decline |
A treating clinician may be a necessary fact witness. That is not the same as being a neutral contested expert on ultimate forensic questions. Fellowship answers that conflate the two fail ethics stations.[7][10]
Classification of expert products
Products include the comprehensive written forensic report, shorter affidavits/statements of evidence, oral testimony (evidence-in-chief, cross-examination, re-examination), and sometimes consulting (non-testifying) expert work for counsel. Disclosure duties and privilege for consulting experts are jurisdiction-specific — state principles, do not invent rules.[1][3][12]
Retention models also differ: party-retained independent medical examination (IME), court/tribunal-appointed expert, and joint experts or concurrent evidence processes where used. Neutrality expectations rise as the process becomes more court-centred, but allegiance bias risk exists whenever one side pays.[15][17]
Epidemiology and system context
Expert psychiatric evidence is high-volume across criminal, civil, family, and administrative systems. Quality problems are not rare: incomplete source lists, weak mapping to legal criteria, and overconfident wording appear in report audits and practice literature.[3][4]
Inter-expert disagreement is empirically common even when experts review serious-crime or psychiatric-injury materials — courts must not assume psychiatric consensus, and experts must not pretend to certainty the literature does not support.[15][16] Adversarial retention can systematically tilt opinions toward the retaining side; this is a documented bias risk, not a courtroom insult.[17]
Mechanisms of expert error (not pathophysiology)
Examiners want a failure-mode map, not neurochemistry.[5][17]
| Mechanism | How it contaminates expert work |
|---|---|
| Allegiance / hired-gun pressure | Selective emphasis, underplaying contrary data |
| Dual-role alliance | Softened risk, incomplete disclosure, advocacy tone |
| Anchoring on incomplete brief | Missing records never sought; one narrative freezes |
| Confirmation bias | Interview probes only support the early hypothesis |
| Instrument over-call | Cut-score becomes pseudo-legal verdict |
| Overconfidence language | “Certainly insane / totally disabled” without data strength |
| Ultimate-issue creep | Expert substitutes for judge/jury on the legal conclusion |
Wettstein’s conceptualisation of the report as a constructed narrative performance is a warning, not an invitation to invent: structure and transparency are the antidote to uncontrolled subjectivity.[5]
Clinical and courtroom “presentations”
Referral stems include solicitor letters of instruction, court orders for assessment, insurer IMEs, fitness or criminal-responsibility briefs, civil capacity requests, and risk opinions for leave or release.[1][18] Evaluees may be genuine, guarded, coached, culturally mismatched, or acutely unwell. Counsel may pressure for rubber-stamped certainty, selective file selection, or late changes to questions.[17][18]
In court, direct examination builds a teachable narrative; cross-examination attacks methodology, missing data, bias, and prior inconsistent statements. Preparation is part of the clinical-legal method, not theatre training alone.[12]
Differential that examiners care about
- Answers defined legal questions
- Transparent sources and limits
- Duty framed to decision-maker
- Alliance-based clinical advocacy risk
- Often incomplete legal criteria mapping
- May be fact evidence, not neutral expert work
- Opinion without method or data trail
- Vulnerable under reliability challenges
- Opposite of AAPL-style structured assessment
Other discriminators: court-appointed vs party-retained experts; consulting vs testifying roles; strong opinion with thin data vs honest uncertainty; genuine specialty expertise vs overreach; and clinical probability statements vs restricted ultimate legal conclusions.[14][17]
Assessment: forensic method before writing
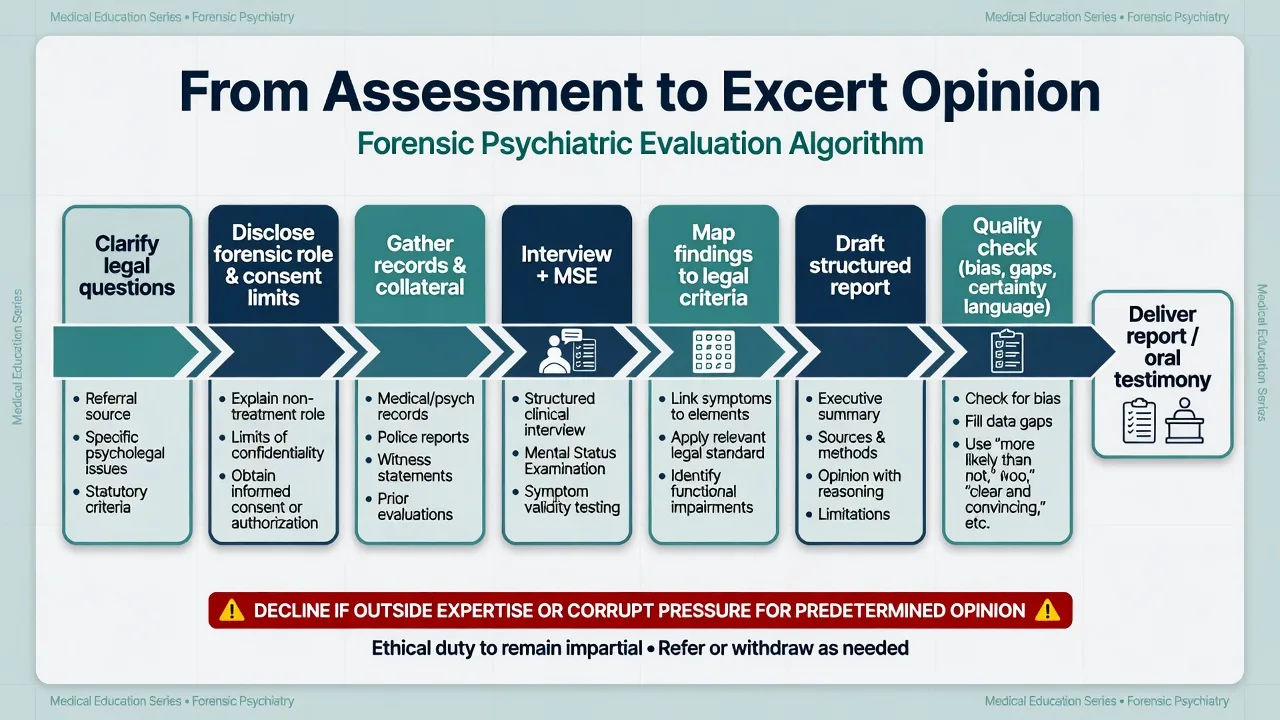
Universal expert method
- Clarify the referral questions and the applicable legal standard (principles + local naming only).[1][2]
- Identify who retains you and whether you can act as independent expert without dual-role conflict.[7][10]
- Disclose the forensic (usually non-therapeutic) role and confidentiality limits to the evaluee; document consent/notification appropriate to the process.[1][8]
- Gather sources — contemporaneous records first; list gaps explicitly.[1][3]
- Interview + MSE with probes mapped to legal abilities or functional domains at issue.[1]
- Use structured tools as adjuncts when indicated and within competence — never as automatic legal verdicts.[1][13]
- Formulate alternatives, validity issues, and confidence bounds.[3][5]
- Opine line-by-line to each question; stop at the edge of expertise and of the brief.[4][14]
The AAPL Practice Guideline for the Forensic Assessment is the major international teaching scaffold for evaluation process, role, and documentation standards; secondary teaching summaries restate its practical thrust for clinicians.[1][2]
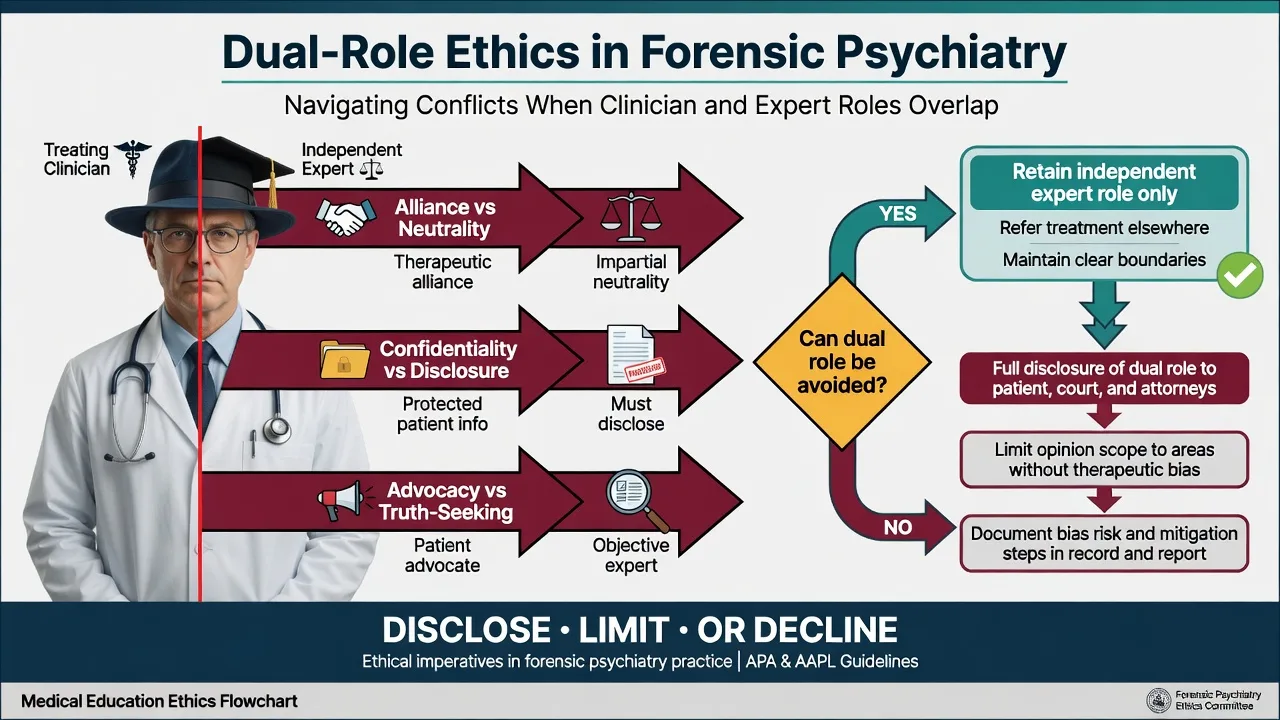
Dual-role ethics (non-negotiable)
Strasburger and colleagues’ classic “two hats” analysis remains core: simultaneous psychotherapist and expert roles create conflicts among alliance, confidentiality, and truth-seeking.[7] Appelbaum’s forensic ethics work reframes the forensic role around truth-seeking and respect for persons rather than a pure beneficence frame borrowed from treatment, and later papers translate those principles into practice decisions (accept/decline, disclosure, scope control).[8][9][10]
Admissibility principles (teaching frames, not invented statutes)
Multi-board exams expect named concepts, not fake section numbers. General acceptance (Frye-type teaching) concerns methods accepted in the relevant field. Reliability / scientific validity factors (Daubert-type teaching in US-influenced materials) include testability, peer review, error rates, standards, and general acceptance — applied to the method, not as a universal statute you invent. Local rules of evidence and expert codes of conduct control actual admission of evidence.[13]
Glancy and Saini discuss the confluence of evidence-based practice and Daubert-type reliability thinking for forensic psychiatry — useful for defending methods, not for inventing local law.[13]
Investigations and source hierarchy
Record review is the expert’s primary “investigation.” Prioritise contemporaneous treating notes, custody/medical charts, police materials, prior expert reports, workplace or school files, and validated collateral. Neuropsychology and formal validity assessment may be essential in disability, TBI, and contested effort scenarios — request them when the legal question turns on cognition or response style and you lack that competence yourself.[1][3]
Never invent data. Material contradictory information belongs in the report with reasoned weighting, not silent deletion.[4][6]
Acute issues during expert work
Clinical safety does not stop because the brief is forensic. Suicidality, violence risk, delirium, or safeguarding crises trigger local clinical and reporting duties while you document interaction with the forensic process.[1] If the brief is ethically impossible (outside expertise; dual-role unmanageable; pressure for a predetermined opinion; insufficient time/records for a safe opinion), decline, limit, or seek adjournment rather than guess.[10][17]
Definitive product: the forensic report
Report writing is a core forensic competency. Practice literature surveys report approaches (including forensic mental health assessment framing) and emphasises structure, transparency, and linkage of data to opinions.[3][4] Ethical dilemmas often crystallise in the written product — what is disclosed, what is omitted, how strongly claims are worded.[6]
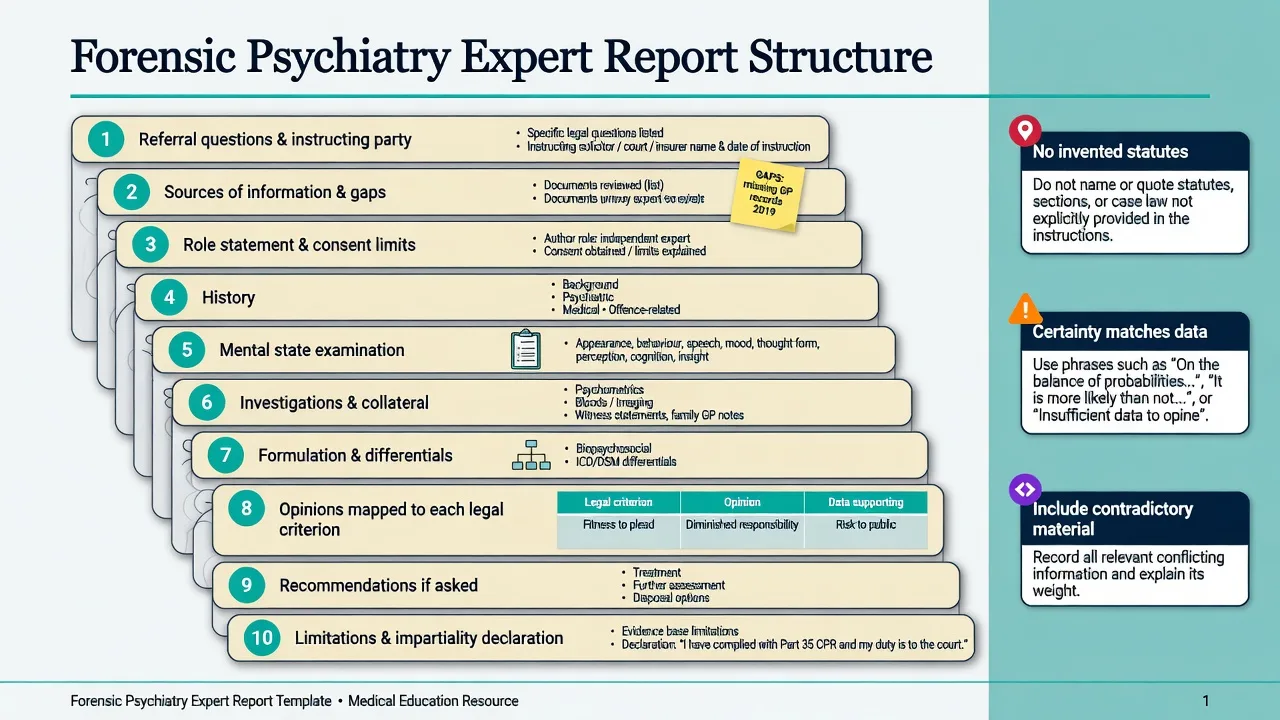
Recommended architecture (adapt to local form requirements)
- Referral questions and instructing party / appointment basis
- Sources of information and material gaps
- Role statement, consent/notification, confidentiality limits
- History relevant to the legal questions (not a free-form novel)
- Mental state examination with carefully quoted content where material
- Investigations / collateral / tools and their limits
- Formulation, differentials, validity issues
- Opinions mapped to each question/criterion
- Recommendations only if asked and within role
- Limitations, confidence language, and any required impartiality/truth declaration
Opinion quality standards
- Answer the questions asked — and say when you cannot.
- Separate diagnosis from legal conclusion. Diagnosis informs, it does not equal, fitness, insanity, incapacity, or disability.
- Certainty language matches data strength — avoid false precision.
- Ultimate issue: some systems restrict or regulate expert conclusions on the final legal question; know the principle and local practice without inventing rules. Provide the psychiatric data the decision-maker needs either way.[14]
- No invented statutes, form codes, or universal percentage tables.
Samuels’ Australasian medico-legal practice notes reinforce practical quality control: brief quality, boundaries, and professional systems that keep reports defensible.[18]
Oral testimony and cross-examination
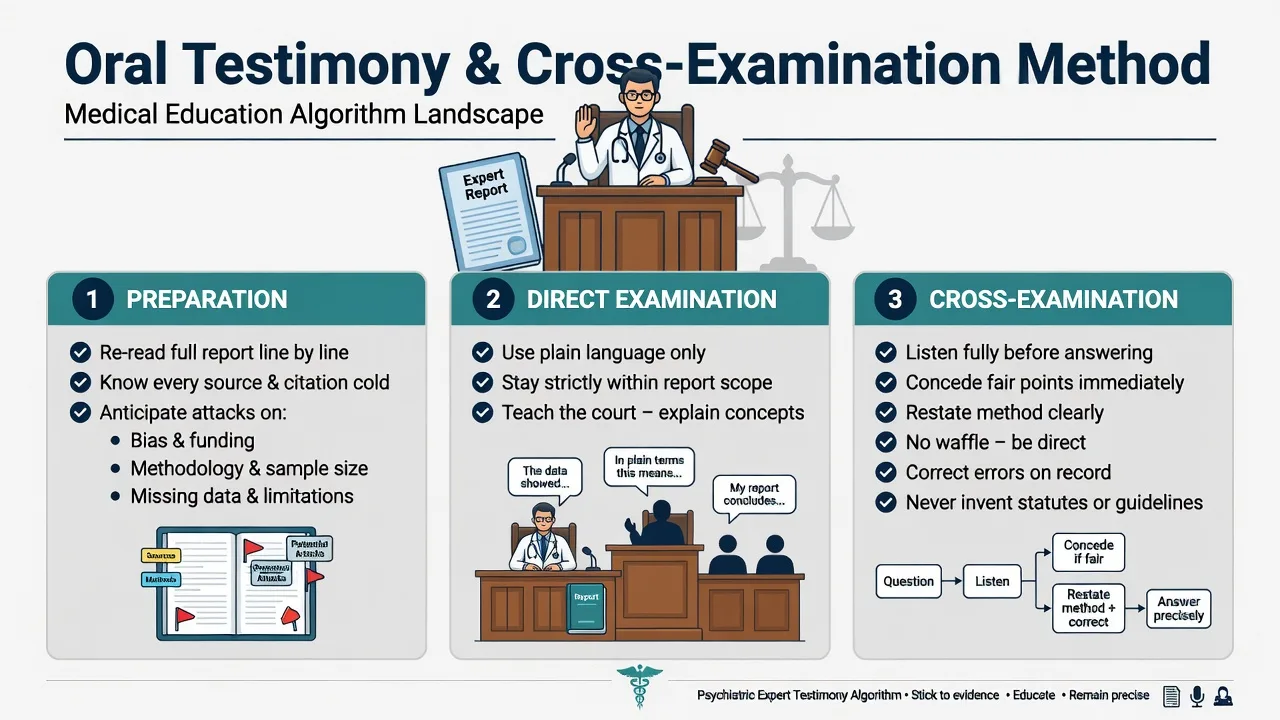
Gutheil’s practical teaching on presenting forensic psychiatric evidence emphasises truthfulness under oath, preparation, and disciplined communication.[12] Under cross-examination: listen to the full question; answer what is asked; concede fair methodological limits; restate how you reached the opinion; correct errors immediately; avoid the expert waffle (evasive non-answers that destroy credibility).[12]
Subtypes and high-yield scenarios
| Scenario | Examiner focus |
|---|---|
| Criminal fitness / responsibility report | Domain-by-domain criteria mapping; restorability if unfit; no invented sections |
| Civil capacity / disability IME | Role ethics; function not diagnosis alone; validity |
| Treating doctor subpoenaed | Fact scope; resist conversion into undeclared independent expert |
| Court-appointed expert | Heightened impartiality expectations; still document method |
| Joint experts / concurrent evidence | Professional disagreement without pejorative theatre |
| Thin brief + urgent court date | State missing data; seek more time; do not guess |
| Tele-forensic evaluation | Method suitability and local admissibility concerns — principles |
| Tribunal affidavit | Shorter form still needs sources, opinions, limits |
Complications and pitfalls
Classic failures: dual-role silence; advocacy masquerading as science; omission of contradictory records; instrument worship; ultimate-issue overreach; pejorative personal attacks on opposing experts; and inventing law.[6][7][14][17] Inter-expert disagreement is expected in complex cases — the professional response is transparent method, not louder certainty.[15][16]
Prognosis and disposition of expert work
A defensible report survives cross-examination and professional scrutiny; a weak one may be preferred by one party briefly and destroyed later. Opinions can change with new material — issue a clear supplemental report rather than silent drift. Release and confidentiality of the finished product follow local process rules (court, tribunal, insurer, counsel).[3][18] Reckless expert evidence risks judicial criticism and regulatory attention — principles of professional accountability, not invented penalty schedules.
Special populations
Valid expert data require communication competence: interpreters, cultural safety (including Indigenous contexts), developmental expertise for children/youth, and recognition of fluctuating cognition in older adults with timed documentation. Custody and secure settings constrain privacy and access — document environmental limits on assessment quality rather than pretending the interview was ideal.[1][11]
Evidence, guidelines, and regional deltas
| Source | Use in exams |
|---|---|
| AAPL Forensic Assessment Guideline (Glancy 2015) | Core process scaffold |
| Appelbaum forensic ethics series | Dual-role / truth-seeking frame |
| Strasburger “two hats” | Dual-role classic |
| Young / Appelbaum KL / Wettstein / Weinstock | Report craft and ethics nexus |
| Large et al.; Forrester | Reliability and bias realism |
| Glancy and Saini Daubert–EBP | Method reliability teaching |
| Buchanan ultimate issue | Limits of legal conclusion-giving |
| Chaplow (ANZ); Samuels practice notes | Regional teaching anchors |
Exam pearls
Classic stem patterns
- Treating psychiatrist asked by family lawyer for a full contested parenting/capacity expert report — dual-role management.
- Insurer demands “total permanent disability” certificate after a single interview with a thin file — structure, validity, decline rubber stamp.
- Cross-examination: “Doctor, you always work for the defence, don’t you?” — allegiance bias acknowledgement without collapse.
- Report missing contradictory admission notes — ethics of omission.
- Expert asked “Is the defendant insane under section X?” — ultimate-issue and invented-section traps.
REPORT — expert product checklist
References
- [1]Glancy GD, Ash P, Bath EP, et al. AAPL Practice Guideline for the Forensic Assessment J Am Acad Psychiatry Law, 2015.PMID 26054704
- [2]Vasile M, Hamalian G, Wortzel HS New Guidelines for Forensic Assessment J Psychiatr Pract, 2016.PMID 27138081
- [3]Young G Psychiatric/ psychological forensic report writing Int J Law Psychiatry, 2016.PMID 28029436
- [4]Appelbaum KL Commentary: the art of forensic report writing J Am Acad Psychiatry Law, 2010.PMID 20305073
- [5]Wettstein RM Commentary: conceptualizing the forensic psychiatry report J Am Acad Psychiatry Law, 2010.PMID 20305074
- [6]Weinstock R Commentary: The forensic report--an inevitable nexus for resolving ethics dilemmas J Am Acad Psychiatry Law, 2013.PMID 24051589
- [7]Strasburger LH, Gutheil TG, Brodsky A On wearing two hats: role conflict in serving as both psychotherapist and expert witness Am J Psychiatry, 1997.PMID 9090330
- [8]Appelbaum PS The parable of the forensic psychiatrist: ethics and the problem of doing harm Int J Law Psychiatry, 1990.PMID 2286491
- [9]Appelbaum PS A theory of ethics for forensic psychiatry J Am Acad Psychiatry Law, 1997.PMID 9323651
- [10]Appelbaum PS Ethics and forensic psychiatry: translating principles into practice J Am Acad Psychiatry Law, 2008.PMID 18583695
- [11]Chaplow DG, Peters JL, Kydd RR The expert witness in forensic psychiatry Aust N Z J Psychiatry, 1992.PMID 1476528
- [12]Gutheil TG The presentation of forensic psychiatric evidence in court Isr J Psychiatry Relat Sci, 2000.PMID 10994298
- [13]Glancy GD, Saini M The confluence of evidence-based practice and Daubert within the fields of forensic psychiatry and the law J Am Acad Psychiatry Law, 2009.PMID 20018992
- [14]Buchanan A Psychiatric evidence on the ultimate issue J Am Acad Psychiatry Law, 2006.PMID 16585229
- [15]Large MM, Nielssen O Factors associated with agreement between experts in evidence about psychiatric injury J Am Acad Psychiatry Law, 2008.PMID 19092070
- [16]Large M, Nielssen O, Elliott G The reliability of evidence about psychiatric diagnosis after serious crime: Part I. Agreement between experts J Am Acad Psychiatry Law, 2010.PMID 21156911
- [17]Forrester A Clinical and scientific expert witness bias: Sources and expression Med Sci Law, 2020.PMID 32272871
- [18]Samuels AH Civil Forensic Psychiatry - part 3: practical aspects of managing a medico-legal practice Australas Psychiatry, 2018.PMID 29457467