Psych · Forensic psychiatry — female offenders
Female offenders
Also known as Women offenders · Women prisoners mental health · Female forensic patients · Gender-responsive corrections · Women in secure care · Maternal filicide · Women who offend · Female criminal justice pathways
Exam-exhaustive fellowship reference on female offenders — gendered pathways, trauma and dual diagnosis burden, PTSD and self-harm, risk-tool caveats, gender-responsive care, women's secure pathways, and filicide/infanticide psychiatric interfaces. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Overview and definition
For exam purposes, female offenders means women and girls who contact criminal justice as alleged or convicted offenders — community sentences, courts, custody, and forensic hospitals. The clinical syllabus is not "women commit less crime, so risk is trivial." It is: lower base rates of serious violence than men do not cancel individual risk, while mental health morbidity, self-harm, trauma, parenting, and dual diagnosis dominate day-to-day care.[3][4][1]
This topic is distinct from general prison mental health (shared reception and equivalence principles still apply), general forensic risk tools (add female validation caveats), and general homicide (emphasise filicide/infanticide). The depth here is sex-specific pathways, service design, and formulation.[3][11][13]
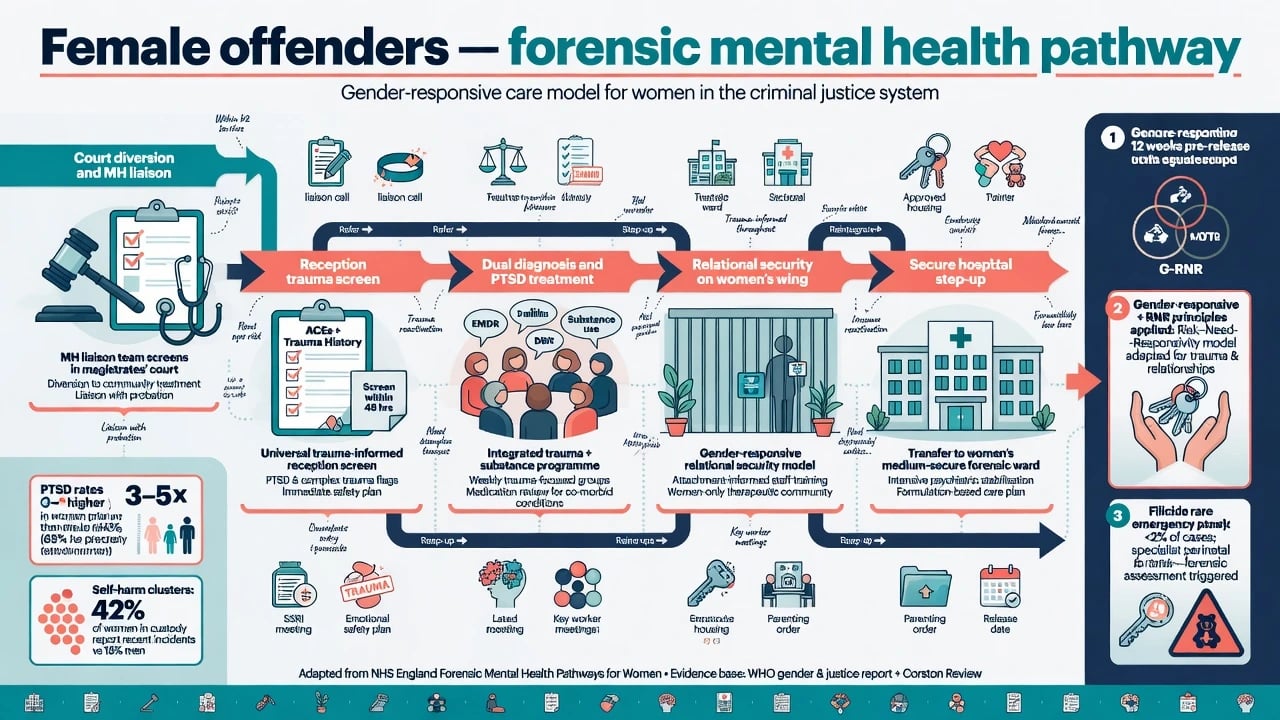
Gendered pathways (trauma → substance use → survival crime / relational conflict) sit alongside standard Risk–Need–Responsivity (RNR) logic: address criminogenic needs, but deliver care in ways that respond to trauma, relationships, caregiving, and economic marginalisation.[10][3]
Epidemiology — what every registrar must quote
Women remain a minority of sentenced prisoners and high-secure patients in most systems, but their share of custody has risen in many jurisdictions, and psychiatric need is dense.[3][4]
Classic US jail work by Teplin and colleagues found that the large majority of incarcerated women met criteria for one or more lifetime psychiatric disorders, with substantial current morbidity — order-of-magnitude higher than community female rates for several diagnoses.[1] Abram and colleagues further documented high comorbidity of severe psychiatric disorders and substance use disorders among women in jail — dual diagnosis is ordinary, not exceptional.[2]
Across prison meta-analyses, severe mental illness remains elevated versus community rates for both sexes; sex-stratified teaching points for exams emphasise that women show particularly high depression, PTSD, and self-harm burdens relative to men in custody.[4][3][5][7]
PTSD. Baranyi and colleagues' review of PTSD in prisoners reported higher point-prevalence ranges among female than male prisoner samples (female ranges commonly cited in the mid-teens to high-thirties percent across studies, with wide heterogeneity).[5] Single-site work in incarcerated women has reported PTSD meeting diagnostic criteria in a large fraction of samples and linked symptom severity to clinical need — treat trauma as a core diagnosis, not a soft add-on.[6]
Self-harm. Large epidemiological work in English and Welsh prisons shows self-harm is common, clusters, associates with later suicide, and occurs at higher rates among women prisoners — never reframe as pure attention-seeking without assessment.[7] Suicide risk factors in prison (Zhong meta-analysis) still guide formulation: prior self-harm, psychiatric morbidity, ideation, isolation, and custodial stressors.[8]
Post-release. Pratt and colleagues showed extreme suicide risk in the early weeks after release for recently released prisoners — women's transition plans must include scripts, appointments, housing, substance treatment, and often child-contact and safety-from-abuser planning.[9]
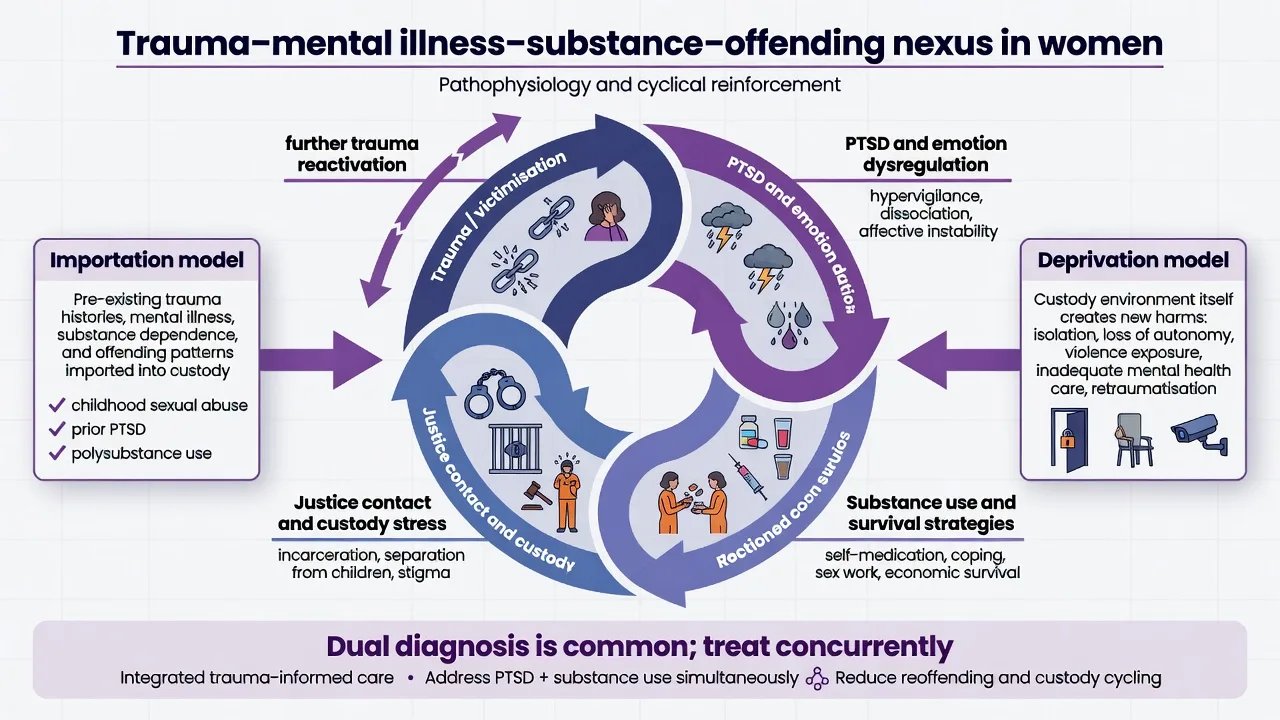
Pathophysiology and mechanisms — pathways, not stereotypes
Importation explains much: women often enter custody already carrying childhood abuse, sexual violence, intimate-partner violence (IPV), poverty, interrupted schooling, and prior mental health or substance treatment gaps.[1][6]
Deprivation adds custody-specific harms: separation from children, strip-searching and body searches that re-trigger trauma, bullying, isolation, legal uncertainty on remand, and medication discontinuity.[3][7]
Mechanistic exam frame for MEQs:
- Trauma and coercive control → PTSD/complex PTSD, shame, dissociation, emotion dysregulation.
- Self-medication with alcohol, opioids, stimulants → dependence and acquisitive offending.
- Relational conflict and reactive aggression (sometimes after prolonged victimisation) → violent charges that still need risk management, not automatic exoneration.
- Primary SMI (psychosis, bipolar) can drive rare high-harm offences — do not force every case into a pure trauma narrative.[3][5][2]
Personality pathology patterns differ in base rates: borderline traits and self-harm are enriched in many women's secure samples; classic male-pattern lifelong antisociality is less modal — but antisocial and psychopathic traits still occur and matter for risk.[11][14]
Classification and clinical subtypes examiners use
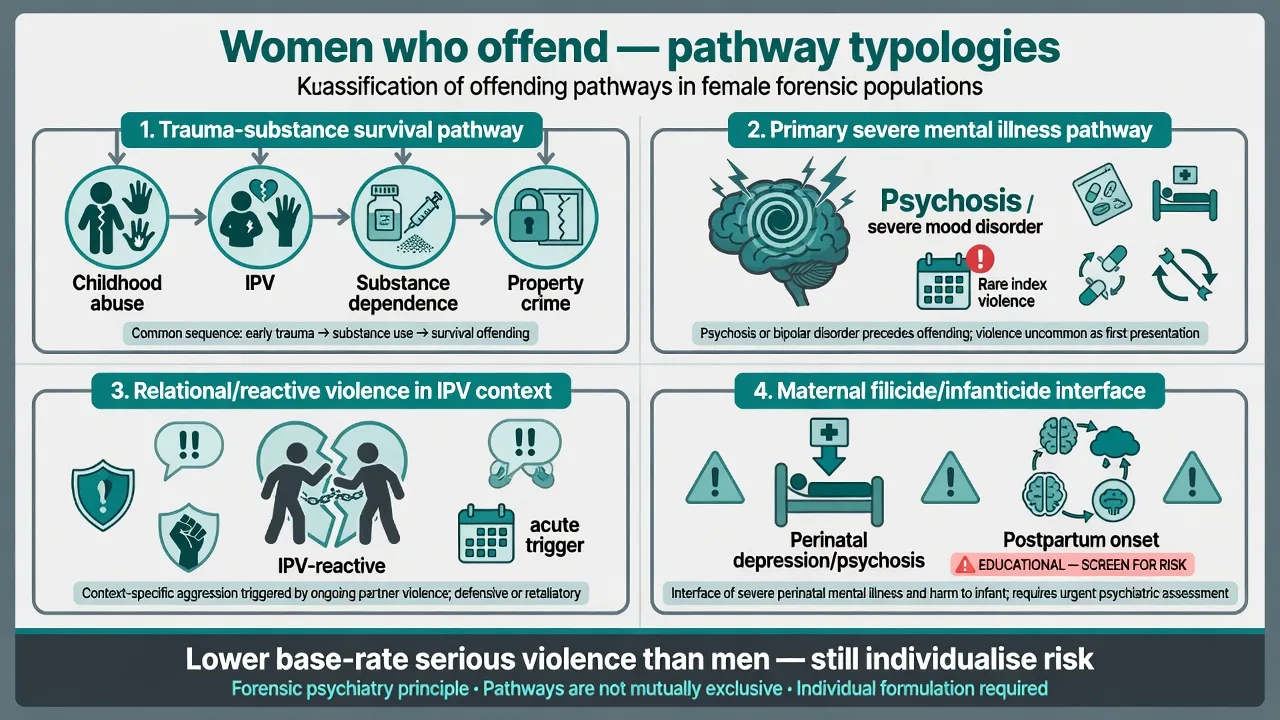
Think in pathway typologies rather than a single female offender type — trauma–substance survival crime, primary SMI index offences, relational/IPV-context violence, maternal filicide/infanticide interfaces, and institutional self-harm trajectories are overlapping frames for formulation, not mutually exclusive boxes.[10][11][15][7]
| Pathway pattern | Clinical anchors | Care emphasis |
|---|---|---|
| Trauma–substance–survival crime | PTSD, SUD, theft/fraud, sex-work related charges | Gender-responsive SUD + trauma therapy |
| Primary SMI index pathway | Psychosis/mood + offence | Treat SMI; hospital when needed |
| Relational/IPV-context violence | Victimisation + reactive violence | Safety, trauma, risk to partner/children |
| Maternal filicide/infanticide | Depression, psychosis, neonaticide contexts | Perinatal psychiatry + legal principles |
| Institutional self-harm trajectory | High self-harm, BPD traits, custody stress | DBT-informed, least restrictive |
Clinical presentation and MSE
Reception and early remand. High rates of distress, self-harm ideation, untreated depression/PTSD, stimulant crash or opioid withdrawal, and acute parenting crisis (children removed or at risk).[1][7][8]
Women's prison mid-sentence. Self-harm clusters, relational conflict, trauma reactivation after visits or court outcomes, emerging or relapsing psychosis if medicines interrupted.[7][3]
Secure hospital. Complex formulations: index offence + SMI + trauma + personality traits + substance history; need for relational security and careful mixed-sex risk management where estates are not single-sex.[11][12]
MSE language for exams. Quote affect, trauma-related hypervigilance, dissociation, command hallucinations if present, suicidal content, homicidal content toward named others, insight, and attachment to children as both protective and risk-relevant. Explain limits of confidentiality at the outset of forensic contact.[6][11][8]
Differential diagnosis
Work differentials actively given high base rates:
- Trauma-related flashbacks/dissociation vs primary psychosis.
- Substance-induced mood/psychosis vs primary bipolar/schizophrenia spectrum.
- Adaptive anger after abuse vs instrumental antisocial violence.
- Personality disorder labels used to withhold antidepressants, trauma therapy, or antipsychotics — a classic pitfall.
- Organic: TBI from IPV, seizure, infection, Wernicke in alcohol dependence.
- Malingering for placement is possible but last after full assessment — false negatives are high-stakes given self-harm and suicide risk.[2][5][8][3]
Assessment structure
Trauma-informed forensic interview
- Presenting legal context and current symptoms.
- Developmental trauma, sexual violence, IPV, trafficking, and child-protection history.
- Psychiatric and self-harm history; prior custody and hospital admissions.
- Substances: onset linked to trauma is common — still diagnose and treat the SUD.
- Parenting status, pregnancy, custody of children, mother–infant unit needs.
- Risk triad: suicide/self-harm, violence/harm to others, vulnerability/victimisation.
- Protective factors: therapeutic alliance, sobriety supports, safe housing, non-abusive relationships, cultural supports.
- Collateral: community notes, child protection, family (safely), prior prison health.[1][6][8]
Risk tools — gender caveats (high-yield)
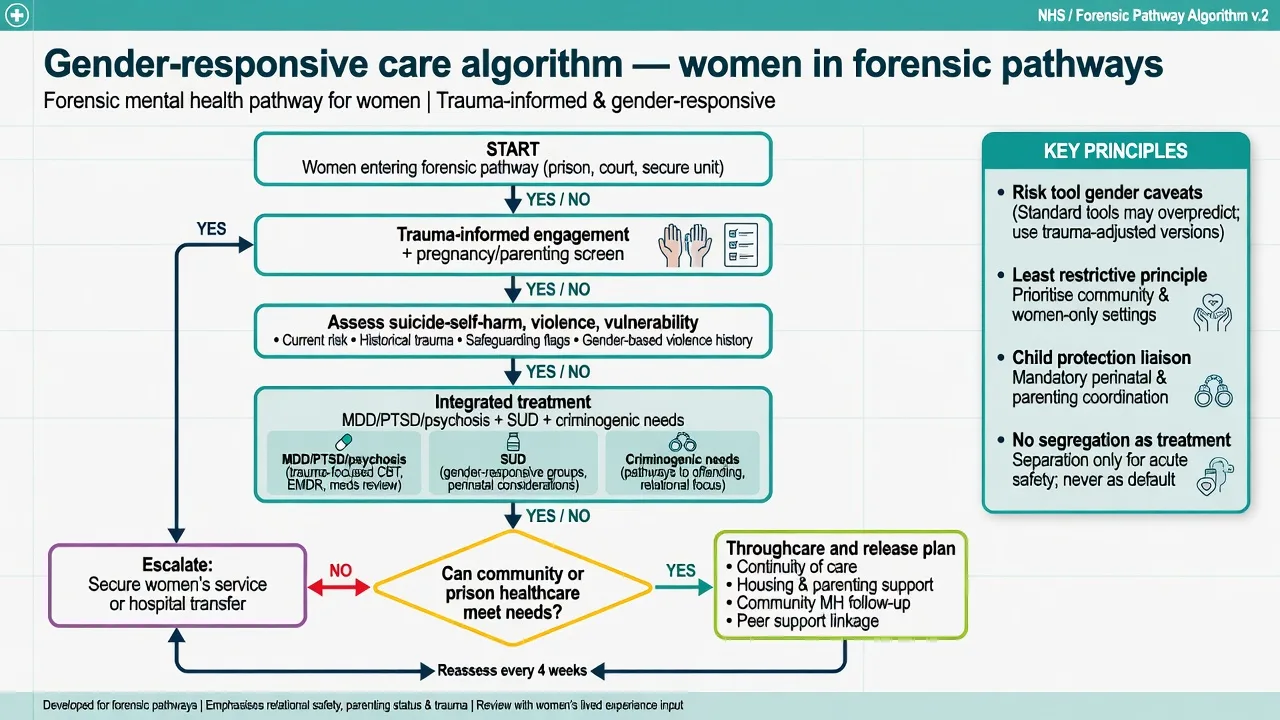
Structured professional judgment (e.g. HCR-20 conceptual domains) and actuarial instruments remain useful frameworks, but instruments developed and validated mainly in male samples need gender-aware interpretation. Coid and colleagues compared predictive accuracy of structured tools across sexes and highlighted gender differences in performance — do not assume identical AUCs or cut-points transfer without thought.[13] National Trajectory Project analyses (Nicholls et al.) examine whether gender-specific forensic services are essential — women NCRMD/forensic populations show both shared and sex-patterned clinical needs; service design should reflect trauma, psychosocial function, and offence profiles rather than cloning male high-secure models uncritically.[14]
Exam answer: use structured frameworks, document dynamic factors (substance craving, active psychosis, recent self-harm, return to abusive partner, child-access conflict), and never replace formulation with a single male-normed score.[13][14][8]
Investigations
Pregnancy test when relevant; BBV/STI screens as indicated; UDS; baseline metabolic panel and ECG before QT-prolonging agents; TFTs/B12/folate as indicated; imaging/EEG if organic red flags or significant head injury from IPV.[3]
Acute management
- Self-harm/suicide crisis: enhanced or constant observation as indicated; ligature-aware environment; trauma-informed engagement; urgent psychiatry; hospital transfer if needs exceed prison capacity. Isolation is not treatment.[7][8][3]
- Withdrawal and medicine continuity: same clinical standards as general prison mental health — alcohol/benzo protocols, OAT continuity where policy allows, restart psychotropics promptly.[3]
- Perinatal emergency: severe depression, postpartum psychosis, or denial-of-pregnancy contexts require emergency perinatal psychiatry pathways and safeguarding — rare filicide risk is not theoretical in these syndromes.[16][15]
Definitive management — gender-responsive and evidence-linked
Gender-responsive principles
Gender-responsive care addresses trauma, relationships, parenting, economic marginalisation, and substance use together. Messina and colleagues' randomised experimental study of gender-responsive substance abuse treatment for women in prison found signals of improved post-release outcomes versus standard care in that pilot RCT — use as evidence that delivery model matters, not as a universal programme brand to invent locally.[10]
Integrated clinical package
- Treat diagnoses: MDD, PTSD/complex PTSD, psychosis, bipolar, anxiety — with community-equivalent medicines and monitoring under custody constraints.[3][6]
- Treat SUD concurrently (not "substances first, psychiatry later").[2][10]
- Psychological therapies: trauma-focused CBT or EMDR when indicated and skilled; DBT skills for emotion dysregulation and self-harm; motivational interviewing for SUD; mentalization-informed work where personality pathology dominates relational risk.
- Criminogenic needs (RNR): antisocial peers, substance use, unstable housing, unemployment, criminal attitudes — delivered in trauma-aware groups when possible.[10][3]
- Parenting and child contact: care plans that ignore children fail women and children; coordinate with child protection ethically.
- Throughcare: scripts, appointments, OAT, housing, safety from abusers, crisis contacts — target Pratt's post-release suicide window.[9]
Secure hospital pathways for women
Bartlett and colleagues characterised pathways of care for women in secure hospitals — who goes where (low vs medium security; NHS vs independent) is driven by clinical need, risk, and system capacity, and care pathways are poorly understood without deliberate mapping. Exam stance: place at the least restrictive security level that safely meets need; avoid both under-securing high-harm risk and over-securing trauma-driven distress without violence risk.[11]
Mezey and colleagues examined safety of women in mixed-sex versus single-sex medium secure units — sexual safety, harassment, and feeling unsafe are material clinical issues in mixed estates; relational security and placement decisions are part of treatment, not mere logistics.[12]
- Trauma-informed frame
- Parenting and economic needs
- Relational security
- Evidence signal from GR substance programmes
- Targets criminogenic needs
- Risk principle still valid
- May miss trauma drivers
- Best combined with GR delivery
- When risk/need exceeds prison
- Least restrictive security
- Map women's pathways
- Mixed-sex safety issues
Psychopharmacology principles (custody-adapted)
Prefer evidence-based agents for the disorder; supervise administration; monitor QTc and metabolic risk; plan labs for mood stabilisers and clozapine; use LAIs when clinically indicated and consented or lawfully authorised. Avoid abrupt cessation at reception. Exact doses follow the primary disorder monographs and local formulary — examiners want continuity, monitoring, and dual diagnosis logic, not invented prison-specific milligram tables.[3]
Filicide and infanticide — high-stakes rare interface
Filicide (killing of a child by a parent) and related infanticide/neonaticide pathways are rare but exam-critical. Bourget and colleagues' review of maternal and paternal filicide delineates typologies and mental illness associations used in forensic teaching (including altruistic, acutely psychotic, accidental/fatal maltreatment, unwanted child, and spouse-revenge conceptual clusters — apply carefully as frameworks, not rigid boxes).[15]
Postpartum psychosis carries risks of suicide and, rarely, filicide; Brockington's review of suicide and filicide in postpartum psychosis is a core citation for perinatal forensic viva answers. Emergency treatment of postpartum psychosis, safeguarding of the infant, and specialist mother-and-baby pathways are clinical priorities; legal defences such as infanticide offences (where they exist) are jurisdiction-specific — state principles only, never invent sections.[16][15]
Assessment of alleged maternal child homicide always includes full psychiatric history, perinatal timeline, psychosis/depression screen, substance use, partner violence, and child-protection chronology — with meticulous documentation for court if commissioned.[15][16]
Complications and pitfalls
- Assuming women are "always low risk."
- Applying male-normed risk scores without clinical override.[13]
- Using segregation, strip-searching, or restraint without trauma-informed safeguards.
- Ignoring child protection and parenting in the care plan.
- Pathologising survival behaviours while missing treatable PTSD/MDD/SUD.[6][2]
- Dismissing self-harm as manipulative.[7]
- Inventing Mental Health Act or infanticide statute numbers across jurisdictions.
Prognosis and disposition
Many women serve relatively short sentences and can reintegrate when housing, substance treatment, trauma care, and safety from abusers are secured. Recidivism risk tracks untreated SUD, homelessness, coercive relationships, and untreated SMI more than offence labels alone.[10][3][9]
Disposition ladder: community diversion and treatment courts (where available) → women's prison healthcare/in-reach → low/medium secure women's services → high secure (rare) → step-down with throughcare. Match security to risk and need using women's pathway evidence, not male high-secure defaults.[11][14]
Special populations
- Adolescent girls: high trauma and self-harm; youth justice interface.
- Perinatal women: pregnancy testing, mother-and-baby units, postpartum psychosis pathways.[16]
- Indigenous women: over-incarceration; cultural safety mandatory in ANZ/Canadian vivas.
- Intellectual disability: vulnerability, suggestibility, adapted communication.
- Older women: depression, cognition, physical multimorbidity.
- Trans women and gender-diverse people in custody: placement safety and continuity of care (local policy; principles of vulnerability assessment).
Regional deltas
State/territory prison health partnerships deliver women's custodial care; Indigenous over-representation is a core viva theme. Secure women's services and mother-and-baby arrangements vary by jurisdiction. Infanticide and mental impairment defences are statute-specific — cite principles, not invented sections. RANZCP forensic faculty positions emphasise trauma-informed and least-restrictive care.[3][11]
Women's minority share of custody is widespread; trauma and dual diagnosis burdens recur across high- and middle-income systems. Apply equivalence of care, reception suicide/self-harm screens, and concurrent dual diagnosis treatment within local resource limits.[3][4][5]
Exam pearls
- Quote high psychiatric morbidity in incarcerated women (Teplin-class) and SMI+SUD comorbidity (Abram).[1][2]
- Name higher PTSD ranges in women prisoners (Baranyi) and higher self-harm (Hawton).[5][7]
- Frame gendered pathways + RNR, not pathways instead of RNR.[10]
- Risk tools need gender-aware use (Coid; Nicholls service-design questions).[13][14]
- Secure pathways for women are a mapped problem (Bartlett); mixed-sex safety is clinical (Mezey).[11][12]
- Filicide frameworks (Bourget) and postpartum psychosis suicide/filicide risk (Brockington) for perinatal forensic stems.[15][16]
- Post-release suicide window still applies (Pratt).[9]
- Never invent statute numbers.
Related topics
Cross-links: prison mental health; risk assessment in forensic settings; homicide and mental disorder; deliberate self-harm and risk assessment; complex PTSD and trauma-informed care; substance use disorders. Female offenders sits at their sex-specific intersection without replacing those monographs.[3]
References
- [1]Teplin LA, Abram KM, McClelland GM Prevalence of psychiatric disorders among incarcerated women. I. Pretrial jail detainees Arch Gen Psychiatry, 1996.PMID 8639033
- [2]Abram KM, Teplin LA, McClelland GM Comorbidity of severe psychiatric disorders and substance use disorders among women in jail Am J Psychiatry, 2003.PMID 12727711
- [3]Fazel S, Hayes AJ, Bartellas K, et al. Mental health of prisoners: prevalence, adverse outcomes, and interventions Lancet Psychiatry, 2016.PMID 27426440
- [4]Fazel S, Seewald K Severe mental illness in 33,588 prisoners worldwide: systematic review and meta-regression analysis Br J Psychiatry, 2012.PMID 22550330
- [5]Baranyi G, Cassidy M, Fazel S, et al. Prevalence of Posttraumatic Stress Disorder in Prisoners Epidemiol Rev, 2018.PMID 29596582
- [6]Harner HM, Budescu M, Gillihan SJ, et al. Posttraumatic stress disorder in incarcerated women: A call for evidence-based treatment Psychol Trauma, 2015.PMID 25793594
- [7]Hawton K, Linsell L, Adeniji T, et al. Self-harm in prisons in England and Wales: an epidemiological study of prevalence, risk factors, clustering, and subsequent suicide Lancet, 2014.PMID 24351319
- [8]Zhong S, Senior M, Yu R, et al. Risk factors for suicide in prisons: a systematic review and meta-analysis Lancet Public Health, 2021.PMID 33577780
- [9]Pratt D, Piper M, Appleby L, et al. Suicide in recently released prisoners: a population-based cohort study Lancet, 2006.PMID 16829295
- [10]Messina N, Grella CE, Cartier J, Torres S A randomized experimental study of gender-responsive substance abuse treatment for women in prison J Subst Abuse Treat, 2010.PMID 20015605
- [11]Bartlett A, Somers N, Fiander M, Harty MA Pathways of care of women in secure hospitals: which women go where and why Br J Psychiatry, 2014.PMID 25104832
- [12]Mezey G, Hassell Y, Bartlett A Safety of women in mixed-sex and single-sex medium secure units: staff and patient perceptions Br J Psychiatry, 2005.PMID 16319412
- [13]Coid J, Yang M, Ullrich S, et al. Gender differences in structured risk assessment: comparing the accuracy of five instruments J Consult Clin Psychol, 2009.PMID 19309193
- [14]Nicholls TL, Crocker AG, Seto MC, et al. The national trajectory project of individuals found not criminally responsible on account of mental disorder. Part 5: how essential are gender-specific forensic psychiatric services? Can J Psychiatry, 2015.PMID 25886689
- [15]Bourget D, Grace J, Whitehurst L A review of maternal and paternal filicide J Am Acad Psychiatry Law, 2007.PMID 17389348
- [16]Brockington I Suicide and filicide in postpartum psychosis Arch Womens Ment Health, 2017.PMID 27778148