Psych · Forensic psychiatry — fitness and criminal responsibility
Fitness to stand trial and criminal responsibility
Also known as Competence to stand trial · Competency to stand trial · Fitness to plead · Adjudicative competence · Unfit to stand trial · Insanity defence · Mental impairment defence · NGRI · NGMI · Criminal responsibility · Pritchard criteria · Presser criteria · Dusky standard · M'Naghten rules
Exam-exhaustive fellowship reference on fitness to stand trial / competence to stand trial / fitness to plead (Pritchard, Presser, Dusky principles), assessment structure and structured tools, restorability and report writing, and criminal responsibility / insanity / mental impairment defences (M'Naghten cognitive limb, ALI variants, jurisdiction-aware labels). Statutes are jurisdiction-specific; no invented section numbers. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
9 MCQs with explanations
Target exams
Red flags
Overview and definition
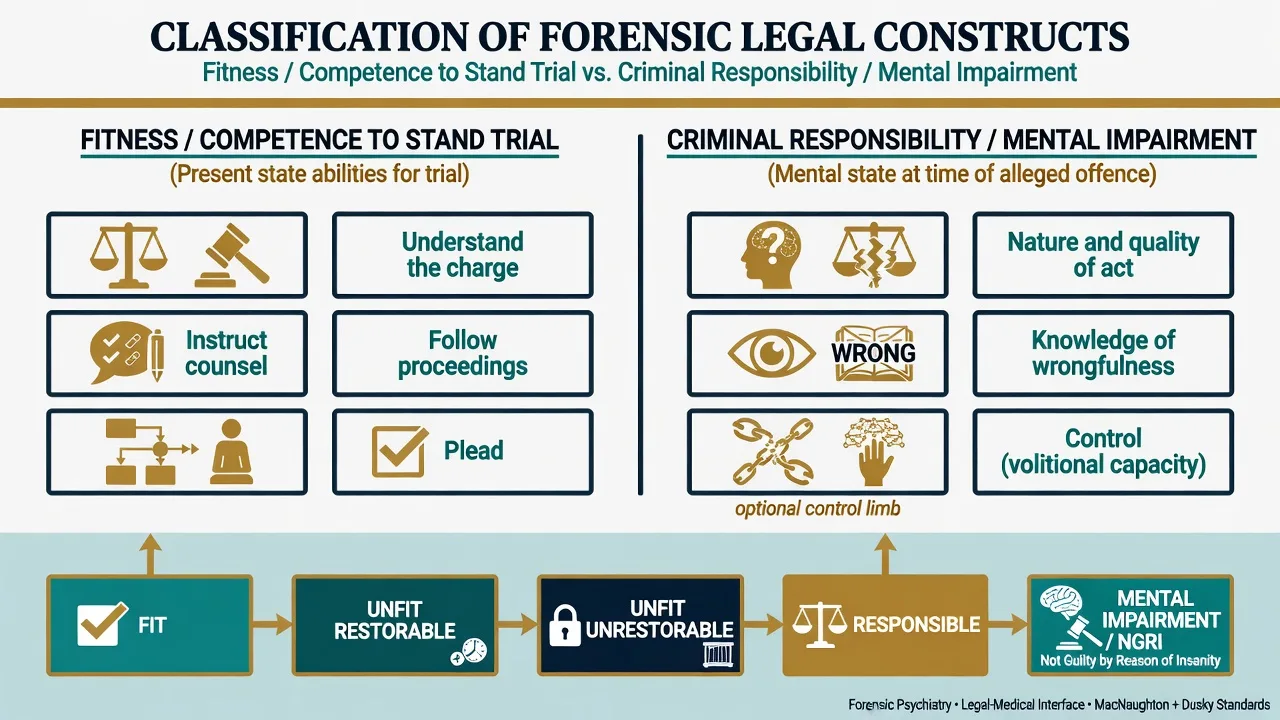
Fitness and criminal responsibility are the two core forensic interfaces every fellowship candidate must keep cleanly separated. Fitness to stand trial (Australia and New Zealand), fitness to plead (England and Wales), and competence / competency to stand trial (United States) all address adjudicative competence: can this defendant, now, understand the proceedings and assist counsel to a legally adequate degree?[1][2][17]
Criminal responsibility addresses a different time point: the alleged offence. The legal question is whether a mental condition at that time negated responsibility under the local test — often still discussed through the M’Naghten cognitive framework (nature and quality of the act; knowledge of wrongfulness), with some jurisdictions adding volitional or “mental impairment” language.[3][4][12][20]
These are legal constructs informed by psychiatry, not DSM diagnoses. Clinicians supply clinical data, functional analysis, and a reasoned opinion mapped to the legal standard; the court decides the ultimate issue according to local procedure.[1][2]
Classification
Fitness / competence constructs
| Construct (label) | Typical region | Core idea |
|---|---|---|
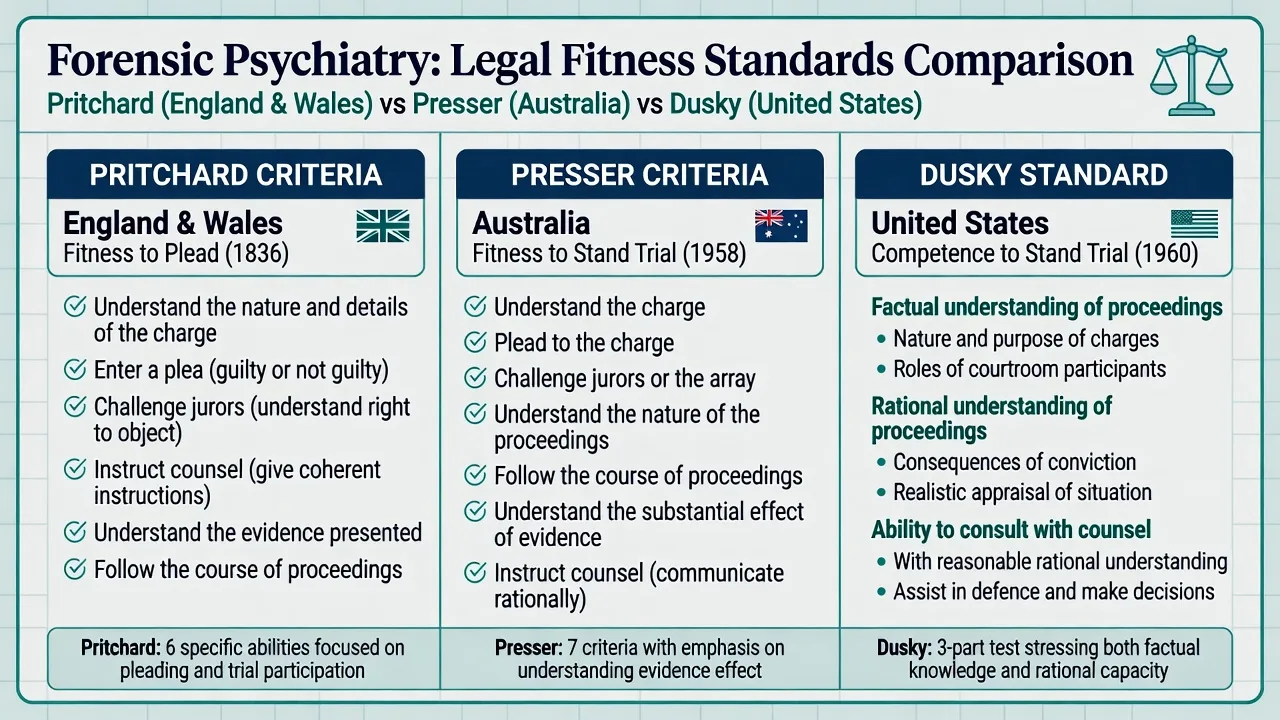
| Fitness to stand trial | Australia, New Zealand | Presser-style abilities to participate in trial |
| Fitness to plead | England and Wales | Pritchard-style abilities to plead and follow trial |
| Competence / competency to stand trial (CST) | United States | Dusky: factual + rational understanding + consult counsel |
| Adjudicative competence | Research literature | Umbrella research term (MacArthur program) |
Criminal responsibility constructs
| Construct (label) | Typical framing | Time focus |
|---|---|---|
| M’Naghten / McNaughton-type cognitive test | Nature/quality and/or wrongfulness | Offence |
| ALI / Model Penal Code “substantial capacity” | Appreciate wrongfulness and/or conform conduct | Offence |
| Mental impairment / NGMI-type defences | Statutory mental impairment criteria (ANZ and others) | Offence |
| NGRI / NCRMD-type special verdicts | Not guilty by reason of insanity / not criminally responsible | Offence + disposal |
Verdict and disposal labels are not interchangeable worldwide. In exams, state the principle, name the local label if known, and flag that statutory wording and post-verdict pathways differ by jurisdiction.[3][10]
Related but distinct constructs
- Present state
- Trial participation abilities
- Restorability is central if unfit
- Retrospective (offence time)
- Legal test limbs (cognitive ± control)
- Diagnosis + nexus required
- Treatment decision-specific
- Not a substitute for fitness
- Different legal framework
Epidemiology and risk context
Competence to stand trial evaluation is among the most frequently requested forensic psychiatric assessments in many systems, especially in the United States, reflecting both the prevalence of mental illness in justice settings and the constitutional importance of a fair trial.[1][2][17]
Quantitative comparative research synthesised by Nicholson and Kugler found that defendants found incompetent (unfit) differ systematically from those found competent: higher rates of psychotic disorder, more severe psychopathology, and greater intellectual impairment are over-represented among the unfit group.[6] The MacArthur adjudicative competence work similarly linked diagnosis and symptom burden to competence-related abilities.[18][19]
Australian practice literature emphasises special considerations in fitness assessment (cultural, communication, disability, and local legal framing) rather than transplanting US instrument culture wholesale.[10][11]
Pathophysiology / mechanisms of impairment
There is no single “fitness lesion.” Examiners want a mechanism map: which clinical process impairs which adjudicative ability?[1][19][23]
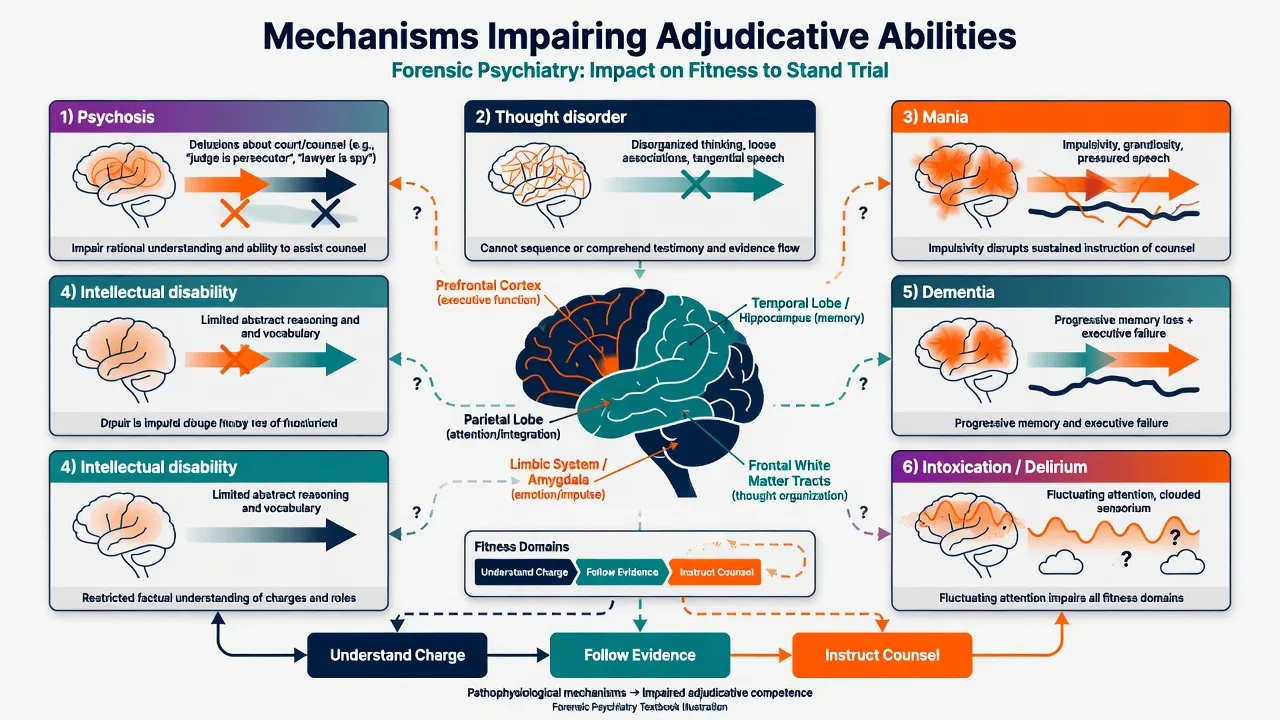
| Clinical driver | Typical fitness impact | Typical responsibility impact |
|---|---|---|
| Persecutory delusions about court/counsel | Rational understanding and assist-counsel collapse despite intact factual knowledge | May support wrongfulness or nature/quality limb if present at offence |
| Formal thought disorder | Cannot follow evidence or instruct coherently | May impair formation of intent/understanding at offence if severe |
| Mania | Impulsivity, grandiosity, inability to maintain working alliance with counsel | Grandiosity or impaired appreciation may be relevant if contemporaneous |
| Intellectual disability | Limited factual understanding; needs adapted interview and education | Cognitive impairment may be relevant; not automatic defence |
| Dementia / progressive NCD | Progressive unrestorability risk | Depends on state at offence; often separate from fitness now |
| Delirium / intoxication | Fluctuating fitness; treat and reassess | Self-induced intoxication doctrines often limit responsibility defences |
Rational understanding is the high-yield differentiator. A defendant may correctly list “judge, jury, prosecutor” yet believe the lawyer is part of a conspiracy — factual knowledge without rational application to their own case is classic unfitness/IST territory under Dusky-style reasoning and Presser/Pritchard practical application.[1][2][24]
For criminal responsibility, the mechanism question is retrospective: did a disease of the mind / mental impairment (legal phrasing varies) produce a defect of reason sufficient that the person did not know the nature and quality of the act, or did not know it was wrong — or, where the local test includes it, lacked substantial capacity to control conduct?[3][12][20]
Clinical presentation
Fitness referrals you will actually see
- Mute or near-mute defendant in cells or dock.
- Refuses to meet counsel; insists counsel is an enemy agent.
- Cannot state the charge after repeated plain-language explanation.
- Confuses judge with prosecutor; believes trial is a television show or religious tribunal.
- Pressured speech and flight of ideas prevent instruction of counsel.
- Profound cognitive impairment; answers are concrete, delayed, or echolalic.
- “I understand everything” with teach-back failure (pseudo-competence).
Criminal responsibility presentations
- Documented untreated psychosis around the offence with contemporaneous odd behaviour.
- Claimed amnesia for the act (amnesia alone is usually not unfitness and is a weak sole basis for insanity).
- Severe neuropsychiatric disease (epilepsy, encephalitis, dementia) with behavioural change around the material time.[21]
- Intoxication-related offences where defence counsel explore automatism or mental impairment pathways — often legally constrained if intoxication was self-induced.[22]
Differential diagnosis
The examiner wants discriminators, not a laundry list.[1][2][3]
| Look-alike | Discriminator |
|---|---|
| Unfit vs uncooperative but capable | Antagonism with intact teach-back and rational strategy ≠ unfitness |
| Unfit vs language/cultural barrier | Interpreter, cultural broker, court education first |
| Unfit vs educational ignorance of law | Teach roles and reassess; ignorance is not disease |
| Unfit vs refusal of counsel / pro se desire | Self-representation may require a higher practical standard in some places — still not automatic unfitness |
| Mental impairment defence vs fitness | Different time points; both can coexist or diverge |
| Mental impairment vs diminished responsibility / partial defences | Partial defences reduce liability; complete mental impairment/insanity is a different legal outcome where available |
| Insane vs sane automatism | Source of automatism (internal “disease of mind” vs external) is a legal categorisation with major disposal differences — jurisdiction-specific |
| Genuine illness vs malingered unfitness/insanity | Inconsistency, rare symptom combinations, surveillance, structured effort testing when indicated — never base solely on “does not look psychotic” |
Organic differentials always remain on the list: delirium, autoimmune encephalitis, acquired brain injury, dementia, aphasia, and substance intoxication/withdrawal can mimic or cause adjudicative impairment and must be considered when the presentation is acute or atypical.[1][21]
Clinical and bedside assessment
Fitness assessment structure
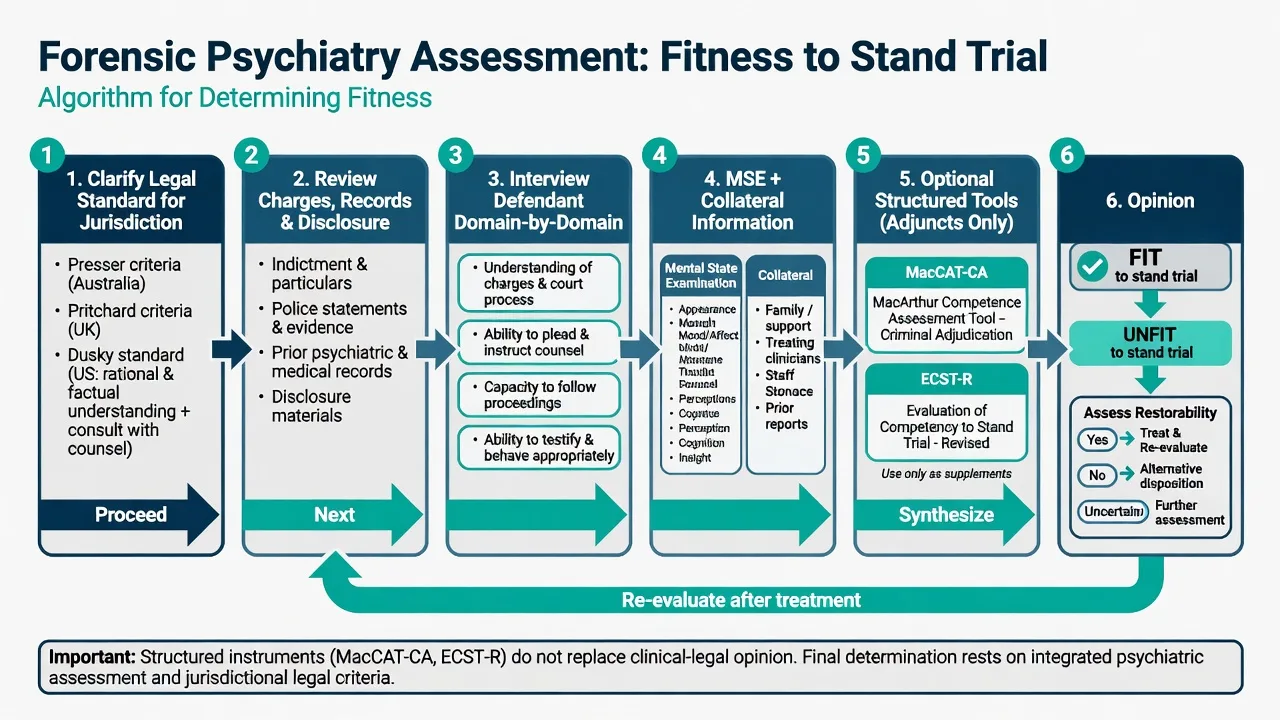
- Define the legal standard for the court you are advising (Presser / Pritchard / Dusky principles as appropriate). Do not invent local section numbers.[1][5][10]
- Know the case enough to assess understanding — charges, basic alleged facts, available disclosure, prior findings.
- Interview the defendant with plain language, teach-back, and non-leading probes of each ability domain.
- MSE with quoted content relevant to court-related delusions, thought form, cognition, and engagement.
- Collateral: counsel observations, custody staff, family, prior reports, medical records.
- Optional structured instruments (MacCAT-CA, ECST-R) as adjuncts.[7][8][9]
- Opinion mapped domain-by-domain to the legal test, plus restorability and recommendations.
Ability domains to probe (practical synthesis)
Across Presser, Pritchard, and Dusky, the functional core is similar even when wording differs.[1][2][5]
- Understand the charge and possible consequences.
- Enter a plea (and understand what pleas mean).
- Understand the nature of proceedings and key roles (judge, jury if any, prosecutor, defence).
- Follow the course of evidence.
- Challenge jurors / exercise procedural rights where applicable.
- Instruct counsel and maintain a working relationship.
- Rationally apply understanding to one’s own case (not merely recite roles).
FIT-NOW
Structured tools
The MacArthur program produced research instruments and the clinically used MacCAT-CA (understanding, reasoning, appreciation domains in a criminal adjudication frame). The ECST-R is another published competency measure. Critical reviews support their use as evidence-based adjuncts that structure enquiry and document reasoning — not as automated verdicts.[7][8][9][18]
Symptom measures correlate with competence-related abilities but do not replace the legal-functional analysis.[23]
Criminal responsibility assessment structure
- Clarify the exact legal test and burden framework for the jurisdiction (principles only in multi-jurisdiction answers).
- Reconstruct mental state at the material time using contemporaneous sources (police video, witness accounts, ED notes, prior admissions), not only the defendant’s current narrative.
- Establish diagnosis (or that no qualifying mental condition is supported), with organic differentials considered.[3][4][21]
- Test the nexus: how did symptoms at the time map onto nature/quality, wrongfulness, and (if applicable) control?
- Address intoxication, personality disorder, and malingering explicitly when raised.[3][22]
- Write a report that separates facts, clinical opinion, and legal-criteria analysis.
Investigations
Investigations serve differential diagnosis and documentation, not the legal verdict itself.[1][2]
| Domain | When useful |
|---|---|
| Cognitive screen / formal neuropsychology | Suspected ID, dementia, ABI, complex contested fitness |
| Metabolic panel, infection, imaging, EEG | Acute organic presentations, new cognitive change, seizures |
| Prior records and medication charts | Pattern of illness, adherence, prior fitness findings |
| Police/body-worn video, contemporaneous notes | Gold for responsibility reconstructions |
| Malingering / effort measures | When presentation is highly inconsistent — interpret cautiously |
IQ is not the fitness test. Australian data underline that assessor discipline and simplistic IQ thresholds can influence outcomes; the legal question remains functional adjudicative ability, not a number.[11]
Management — acute / court interface
When fitness is clearly impaired, prioritise fairness and clinical stabilisation before any empty trial ritual.[1][2]
- Advise the court that assessment (or further assessment) is required; support adjournment rather than an empty trial ritual.[1]
- Stabilise medical and psychiatric emergencies in custody (agitation, withdrawal, catatonia, medical differentials).[2]
- Start or optimise treatment of the driver of unfitness when clinically indicated (for example, antipsychotic treatment for psychosis-driven unfitness), within lawful custody/hospital frameworks of the jurisdiction.[2][14]
- Document risk to self/others in custody separately from the fitness opinion.[1]
If the person is fit, psychiatric treatment may still be urgently needed — fitness does not equal wellness.[1]
Management — definitive, restoration, and disposal
If fit
Trial proceeds. Continue clinical care. Do not confuse cooperation with health.[1][2]
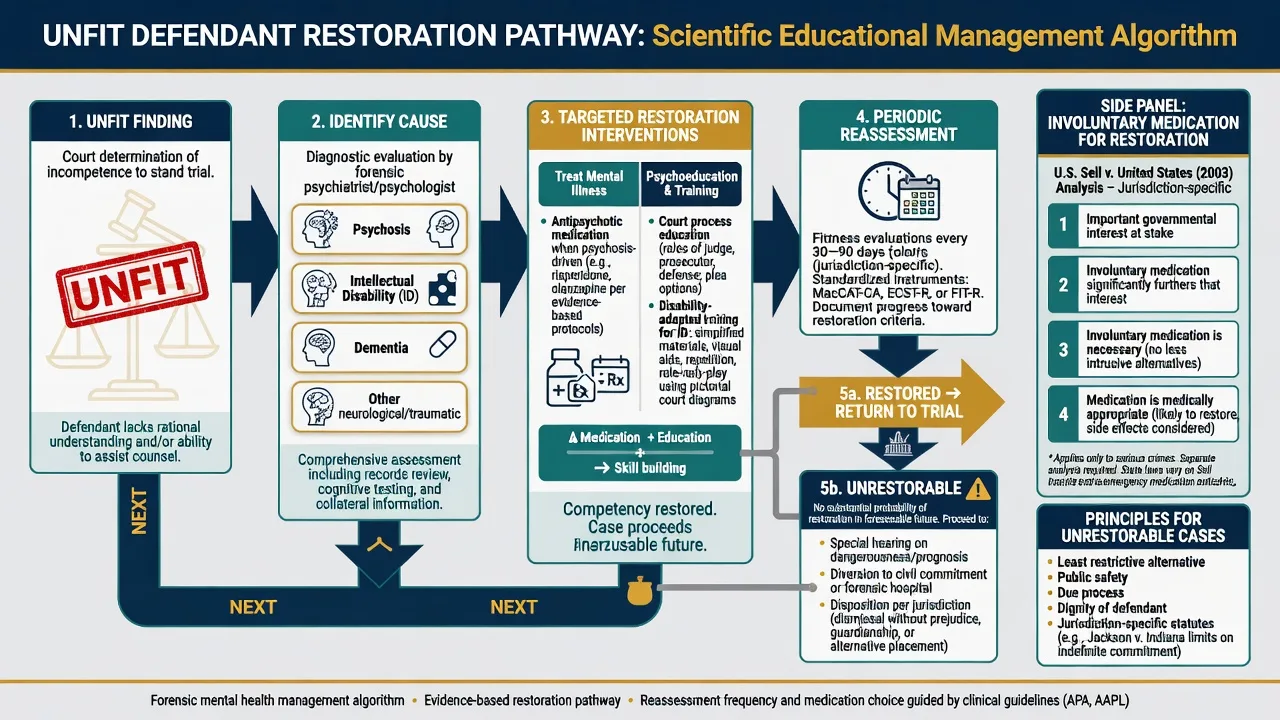
If unfit — restoration
Restoration is the clinical-legal project of returning the person to adjudicative competence where possible.[2][14]
| Driver of unfitness | Restoration focus |
|---|---|
| Psychosis | Antipsychotic treatment, reduce court-related delusions, improve organisation of thought |
| Mania | Mood stabilisation, sleep, reduced distractibility |
| Intellectual disability | Disability-adapted court education / training programs, simplified materials, practice with roles (documented programs exist in the US forensic literature) |
| Depression / mutism | Treat depression; address catatonic features if present |
| Dementia | Limited restorability if progressive; maximise sensory/communication supports; honest unrestorable opinions when appropriate |
Restorability opinion should address: likely / unlikely / uncertain; expected timeframe; barriers (treatment resistance, progressive disease, profound disability); and what interventions are planned.[14]
Involuntary medication to restore competence is highly jurisdiction-specific. In US federal doctrine, Sell-type analyses balance important government interests, likelihood of restoration, medical appropriateness, and less intrusive alternatives — discuss as principles, not as a universal protocol.[13][14] Comparative work on long-acting injectable versus oral antipsychotics in restoration settings is limited and should not be oversold as a universal superiority claim.[15]
If unrestorable
Local law provides alternative pathways (special hearings, diversion, limiting terms, hospital orders, or other dispositions). State principles: the criminal process cannot fairly continue in the ordinary way; clinical care and public protection still need planning; time limits on indefinite “restoration detention” exist in some systems as a fairness constraint.[2][14]
If mental impairment / NGRI-type finding
A successful defence is not automatic free release. Jurisdictions typically use hospital orders, supervision, or forensic review board models. Risk management, treatment, and graduated leave are clinical-legal continuums after the verdict.[3][4]
Report structure (exam-scoring gold)
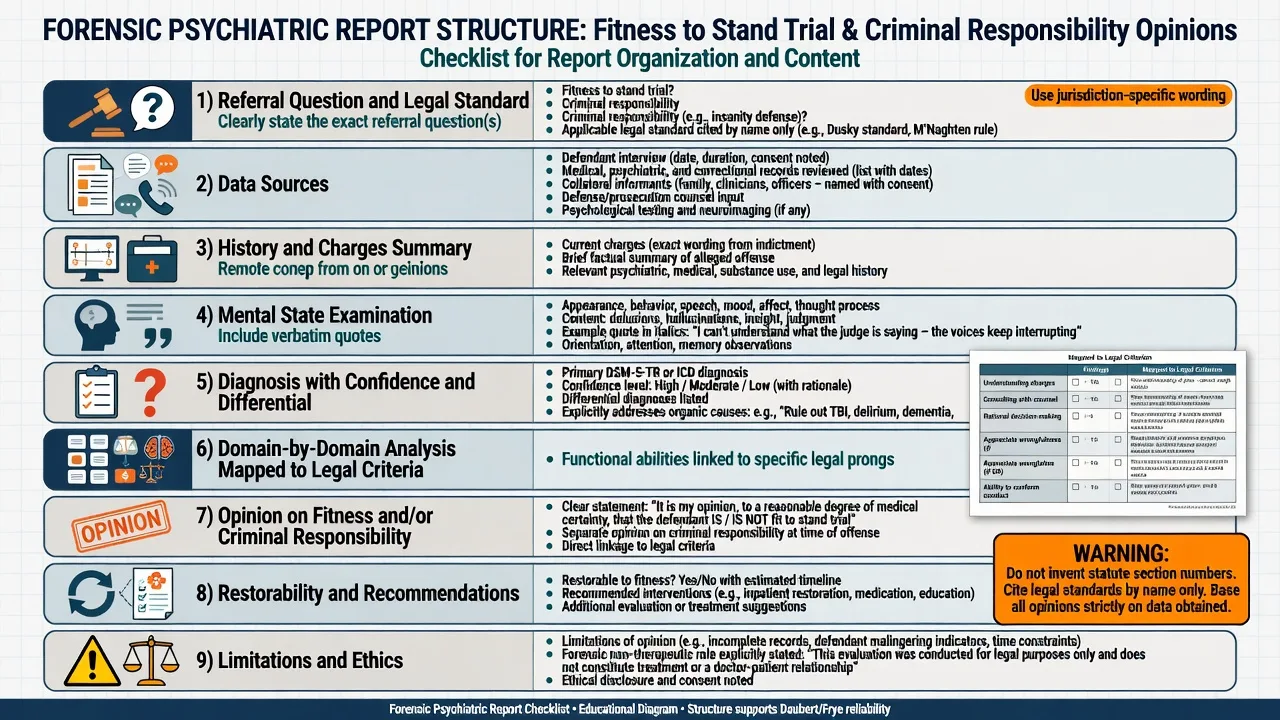
- Referral question and legal standard used.
- Sources of information and limits.
- Relevant history and charges (factual summary, not advocacy).
- Examination findings with quotations where material.
- Diagnosis and differentials (including organic).
- Domain-by-domain functional analysis.
- Opinion on fitness and/or criminal responsibility with reasoning.
- Restorability, treatment recommendations, risk issues if asked.
- Limitations (incomplete disclosure, single interview, cultural/language factors).
Specific subtypes and scenarios
Psychosis-driven unfitness
Highest yield. Target court-related delusions and thought disorder; reassess after treatment response.[6][19]
Intellectual disability
Do not equate IQ cut-offs with unfitness. Use adapted interviewing, check understanding after education, and consider specialised restoration training models.[11][16]
Amnesia for the offence
Usually does not by itself establish unfitness: the person may still understand proceedings and instruct counsel about other matters and strategy. Amnesia claims also require careful evaluation in responsibility analyses.[1][2]
Self-representation
Some systems scrutinise whether a higher practical capacity is needed to proceed without counsel. Basic fitness to stand trial with counsel is not identical to competence for complex self-representation — flag the distinction without inventing doctrine.[2]
M’Naghten-type cognitive tests
Classic multi-board pearl: disease of the mind → defect of reason → did not know nature and quality, or did not know it was wrong. This is a cognitive test; presence of psychosis alone is insufficient without the nexus.[12][3][20]
Volitional / ALI-type tests
Where available, add substantial capacity to conform conduct to the law. Many jurisdictions narrowed or removed pure control tests after policy controversies; know that local law controls.[3][20]
Intoxication and automatism
Self-induced intoxication often restricts mental-condition defences; involuntary intoxication and sane/insane automatism distinctions are jurisdiction-specific and examinable at principle level.[22]
Neuropsychiatric disorders
TBI, epilepsy, neurodegenerative disease, and autoimmune encephalitis can feature in both fitness and responsibility analyses; reconstruct timeline meticulously.[21]
Complications and pitfalls
[1] [2] [7] [10]Prognosis and disposition
Psychosis-related unfitness is often potentially restorable with treatment and court education, though timelines vary and treatment resistance is real.[14][15] Intellectual disability may improve functional court knowledge with training but not always to the legal threshold; progressive dementia often trends toward unrestorable.[16][14]
After mental impairment/NGRI-type findings, disposition is a long game of secure care, risk review, and gradual step-down under local law — not a single discharge decision.[3]
Special populations
| Population | Focus |
|---|---|
| Youth | Developmental immaturity can impair adjudicative abilities even without major mental illness; assess developmentally |
| Older adults | Dementia, sensory loss, delirium; fluctuating capacity for trial |
| Indigenous defendants | Communication style, cultural meaning of court, interpreter/cultural support — avoid bias equating difference with incapacity |
| Communication disability | Deafness, aphasia: maximise supports before unfitness |
| Women defendants | Competence-related abilities researched in MacArthur samples; still individualise |
| ABI / neurodevelopmental | Static cognitive limits vs treatable psychiatric comorbidity |
Evidence, guidelines, and regional differences
Use fitness to stand trial language and Presser principles as the classic common-law anchor taught in Australian forensic psychiatry, while applying the current statute and case law of the specific state/territory or New Zealand. Criminal responsibility is often framed as mental impairment (or local equivalent labels) rather than “insanity” alone. Special considerations in Australian fitness assessment and the misuse of crude IQ thresholds are live practice issues.[10][11]
Many common-law systems inherit M’Naghten-type cognitive language (including jurisdictions teaching “McNaughton rules” for exams). Always answer with principles + local label, never fabricated sections. AAPL guidelines are influential internationally but are not statute outside their context.[3][12][17][20]
Landmark practice anchors to name in viva (guideline and evidence anchors, not statute):[1][2][3]
- AAPL CST guideline (2007) and Practice Resource (2018).[1][2]
- AAPL insanity defence guidelines (2002; 2014).[3][4]
- MacArthur adjudicative competence research program.[18][19]
- Nicholson and Kugler quantitative review of competent vs incompetent defendants.[6]
- Evidence-based instrument reviews (MacCAT-CA, ECST-R).[7][8]
Exam pearls
PRITCHARD
- Fitness = now; responsibility = then.
- Pritchard / Presser / Dusky for multi-board coverage.[1][5][10]
- M’Naghten: nature/quality or wrongfulness — cognitive nexus required.[12]
- Diagnosis ≠ defence / ≠ unfitness.[3][6]
- Amnesia ≠ unfit by itself.[1]
- IQ ≠ fitness verdict.[11]
- Tools adjunctive; opinion is reasoned and criterion-linked.[7][8]
- Restorability is part of a complete unfitness opinion.[14]
- Never invent section numbers.[2][10]
Self-test: one stem, two questions
A defendant with schizophrenia believes his lawyer is transmitting thoughts for the prosecution. He correctly names the judge and jury. He is currently receiving no medication.[1][24]
- Fitness issue?
- Does this alone prove a mental impairment defence for an offence last year?[3]
Model. (1) Yes — rational understanding / ability to instruct counsel is likely impaired despite factual knowledge; assess fully and treat with restoration in mind.[1][24] (2) No — responsibility requires reconstruction of mental state at the offence, not today’s delusion alone.[3]
Fitness / CST
- Time: present state
- Question: can they participate fairly?
- Anchors: Presser / Pritchard / Dusky
- If impaired: restore or alternative process
Criminal responsibility
- Time: alleged offence
- Question: did mental condition meet the legal test then?
- Anchors: M'Naghten ± control / mental impairment
- If successful: special verdict + disposal pathway
Exam crimes
- Mixing fitness with responsibility
- Diagnosis without nexus
- Invented statute section numbers
- Instrument cut-score as verdict
“Fitness = now (trial process). Responsibility = then (offence). Diagnosis alone is never the legal test.”
References
- [1]Mossman D, Noffsinger SG, Ash P, et al. AAPL Practice Guideline for the forensic psychiatric evaluation of competence to stand trial J Am Acad Psychiatry Law, 2007.PMID 18083992
- [2]Wall BW, Ash P, Keram E, et al. AAPL Practice Resource for the Forensic Psychiatric Evaluation of Competence to Stand Trial J Am Acad Psychiatry Law, 2018.PMID 30602602
- [3]American Academy of Psychiatry and the Law AAPL Practice Guideline for forensic psychiatric evaluation of defendants raising the insanity defense J Am Acad Psychiatry Law, 2014.PMID 25492121
- [4]Giorgi-Guarnieri D, Janofsky J, Keram E, et al. AAPL practice guideline for forensic psychiatric evaluation of defendants raising the insanity defense J Am Acad Psychiatry Law, 2002.PMID 12099305
- [5]Mudathikundan F, Chao O, Forrester A Mental health and fitness to plead proposals in England and Wales Int J Law Psychiatry, 2014.PMID 24268448
- [6]Nicholson RA, Kugler KE Competent and incompetent criminal defendants: a quantitative review of comparative research Psychol Bull, 1991.PMID 2062978
- [7]Rogers R, Johansson-Love J Evaluating competency to stand trial with evidence-based practice J Am Acad Psychiatry Law, 2009.PMID 20018994
- [8]Anderson JL, Plantz J, Glocker S, et al. The MacCAT-CA and the ECST-R in Competency to Stand Trial Evaluations: A Critical Review and Practical Implications J Pers Assess, 2022.PMID 34878964
- [9]Pinals DA, Tillbrook CE, Mumley DL, et al. Practical application of the MacArthur competence assessment tool-criminal adjudication (MacCAT-CA) in a public sector forensic setting J Am Acad Psychiatry Law, 2006.PMID 16844797
- [10]Blake GA, Ogloff JRP, Antolak-Saper N Special considerations to the assessment of fitness to stand trial in Australia Psychiatr Psychol Law, 2023.PMID 37744651
- [11]Sakdalan JAE, Buchwald K, Visser S, et al. IQ thresholds and influence of the assessor's professional discipline on fitness to stand trial assessment outcomes in Australia Psychiatr Psychol Law, 2025.PMID 39882085
- [12]Diamond BL Isaac Ray and the trial of Daniel M'Naghten Am J Psychiatry, 1956.PMID 13292555
- [13]Gerbasi JB, Scott CL Sell v. U.S.: involuntary medication to restore trial competency--a workable standard? J Am Acad Psychiatry Law, 2004.PMID 15497635
- [14]Cochrane RE, Laxton KL, Mulay AL, et al. Guidelines for determining restorability of competency to stand trial and recommendations for involuntary treatment J Forensic Sci, 2021.PMID 34032278
- [15]Ghossoub E, Minchin S, Hayreh D, et al. Long-Acting Injectable versus Oral Antipsychotics for Restoration of Competency to Stand Trial J Am Acad Psychiatry Law, 2019.PMID 31533995
- [16]Wall BW, Krupp BH, Guilmette T Restoration of competency to stand trial: a training program for persons with mental retardation J Am Acad Psychiatry Law, 2003.PMID 12875497
- [17]Hoge SK Competence to stand trial: An overview Indian J Psychiatry, 2016.PMID 28216768
- [18]Hoge SK, Bonnie RJ, Poythress N, et al. The MacArthur adjudicative competence study: development and validation of a research instrument Law Hum Behav, 1997.PMID 9146101
- [19]Hoge SK, Poythress N, Bonnie RJ, et al. The MacArthur Adjudicative Competence Study: diagnosis, psychopathology, and competence-related abilities Behav Sci Law, 1997.PMID 9415960
- [20]Felthous AR Rational capacity and criminal responsibility in the USA Int J Law Psychiatry, 2022.PMID 35738073
- [21]Frierson RL, Joshi KG Mental health criminal defenses in persons with neuropsychiatric disorders Behav Sci Law, 2024.PMID 37966983
- [22]Glancy GD, Patel K, Heintzman M, et al. An International Comparison and Review of Self-Induced Intoxication Causing Automatism J Am Acad Psychiatry Law, 2023.PMID 37532277
- [23]Jacobs MS, Ryba NL, Zapf PA Competence-related abilities and psychiatric symptoms: an analysis of the underlying structure and correlates of the MacCAT-CA and the BPRS Law Hum Behav, 2008.PMID 17546483
- [24]Ragatz L, Vitacco MJ, Tross R, et al. Competency to Proceed to Trial Evaluations and Rational Understanding Int J Offender Ther Comp Criminol, 2015.PMID 25080435