Psych · Forensic psychiatry — homicide
Homicide and mental disorder
Also known as Psychotic homicide · Abnormal homicide · Homicide due to mental disorder · First-episode psychosis homicide · Filicide mental illness · Homicide-suicide · Schizophrenia homicide · Mental impairment homicide · NGRI homicide · Forensic homicide assessment
Exam-exhaustive fellowship reference on homicide and mental disorder — absolute vs relative risk, myth versus epidemiology, first-episode untreated psychosis concentration, substances and personality pathways, domestic/filicide/homicide-suicide subtypes, criminal responsibility interface, post-homicide forensic assessment, secure pathway and multi-agency public protection principles. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
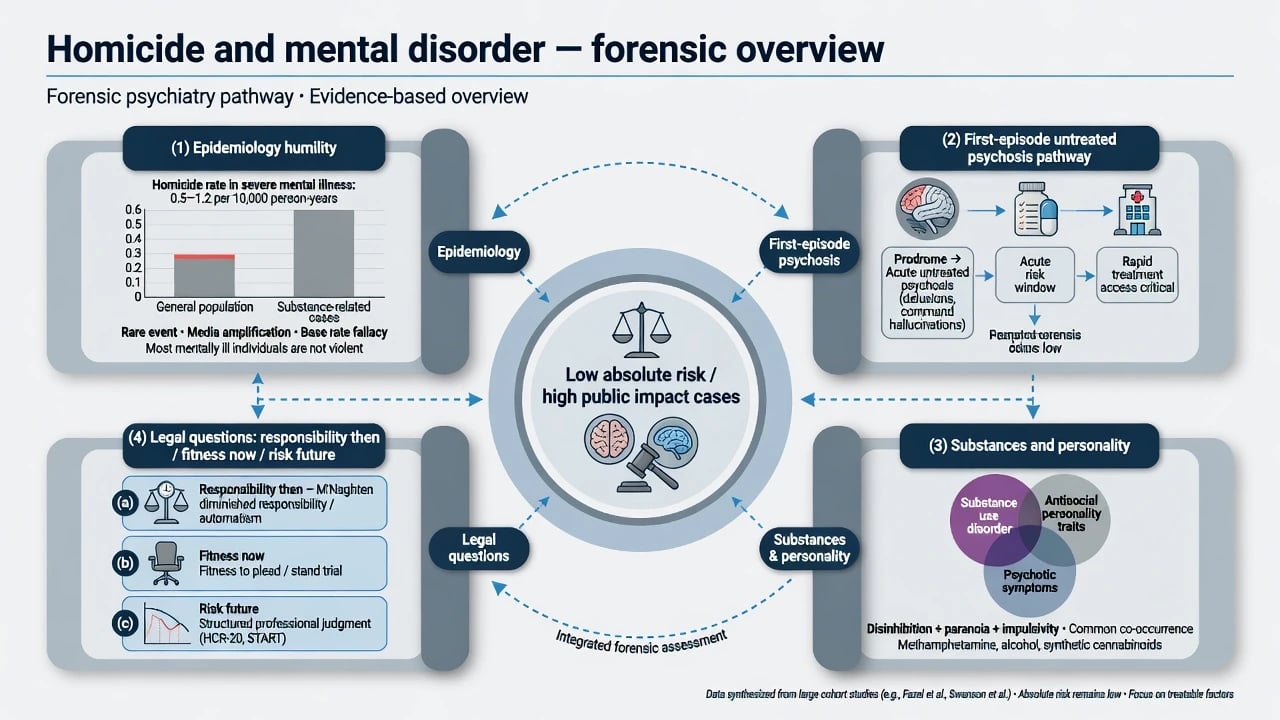
Homicide is a legal category of unlawful killing (murder, manslaughter, and local equivalents). "Homicide due to mental disorder" and related research labels (abnormal homicide, patient homicide) are epidemiological constructs, not DSM-5-TR or ICD-11 diagnoses. Fellowship examiners test whether you can hold three simultaneous frames that keep absolute-risk humility, clinical pathway science, and legal time points separate.[1][2][17]
- Population science — absolute risk is low; media narratives often overstate community-care failure.[1][2]
- Clinical pathway science — untreated psychosis (especially first episode), substances, and prior violence concentrate risk far more than a diagnosis label alone.[5][9][10]
- Legal-clinical interface — mental state at the offence (responsibility / mental impairment / insanity), now (fitness), and future (risk and public protection) are different questions.[17]
Operational vocabulary for exams (research labels, not legal verdicts):
- Relative risk — elevated odds compared with general population (can be real and still compatible with rare absolute events).
- Absolute risk — probability that a given patient will kill (usually very low).
- Patient homicide — perpetrator in recent contact with mental health services (definitions vary by study).
- Psychotic homicide — homicide during active psychotic illness (research label).
- Index offence reconstruction — multi-source recovery of mental state at the material time. These research labels organise national inquiry teaching and forensic reports; they are not substitutes for legal verdicts or DSM/ICD diagnoses.[2][3][5]
Classification — pathways, not one disease
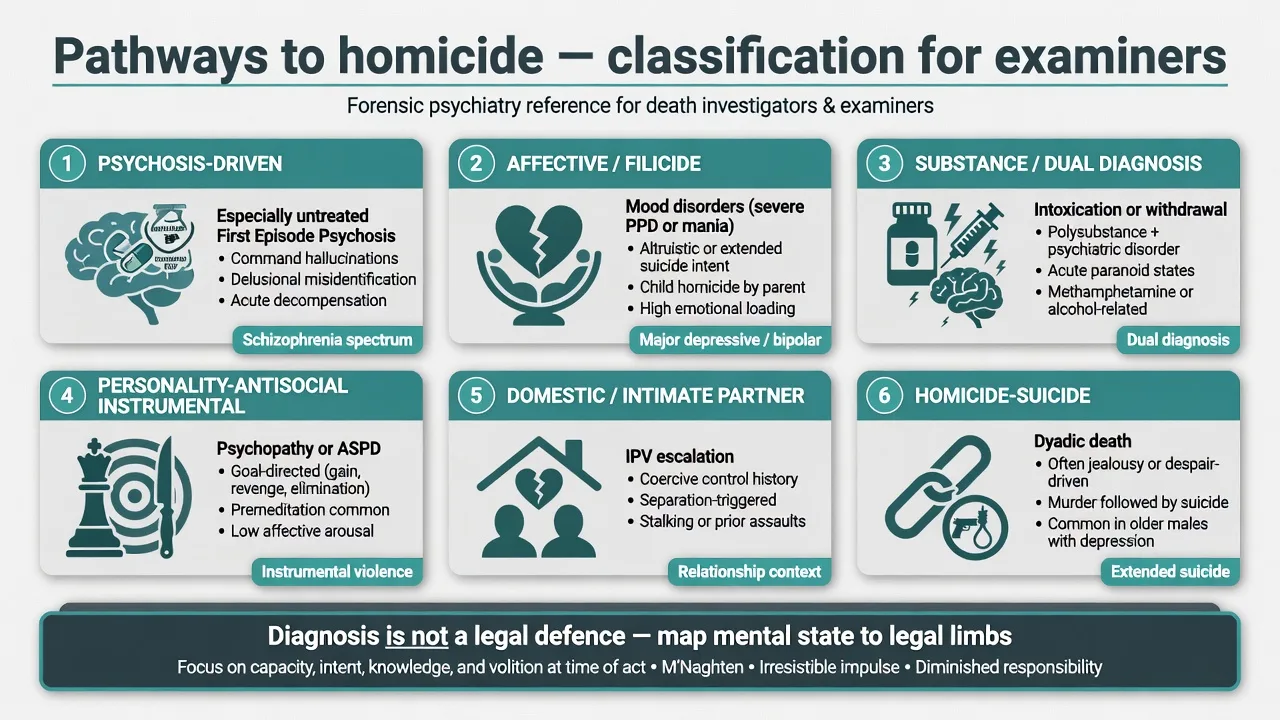
| Pathway | Clinical core | Exam traps |
|---|---|---|
| Psychosis-driven | Untreated FEP or relapsed psychosis with persecutory/threat content | Assuming all schizophrenia homicide is stranger and treated |
| Affective / filicide | Severe depression, mania, altruistic or extended-suicide themes | Ignoring maternal vs paternal pattern differences |
| Substance / dual diagnosis | Intoxication, stimulant paranoia, alcohol disinhibition | Blaming illness alone when substances dominate timeline |
| Personality-antisocial | Instrumental, planned, gain or status | Calling every antisocial homicide a mental-illness defence |
| Domestic / IPV | Escalating intimate-partner violence with or without SMI | Missing non-psychotic domestic drivers |
| Homicide-suicide | Dyadic death; depression, jealousy, despair | Treating only the homicide half of the risk picture |
Epidemiology — myth versus evidence
Absolute and relative risk
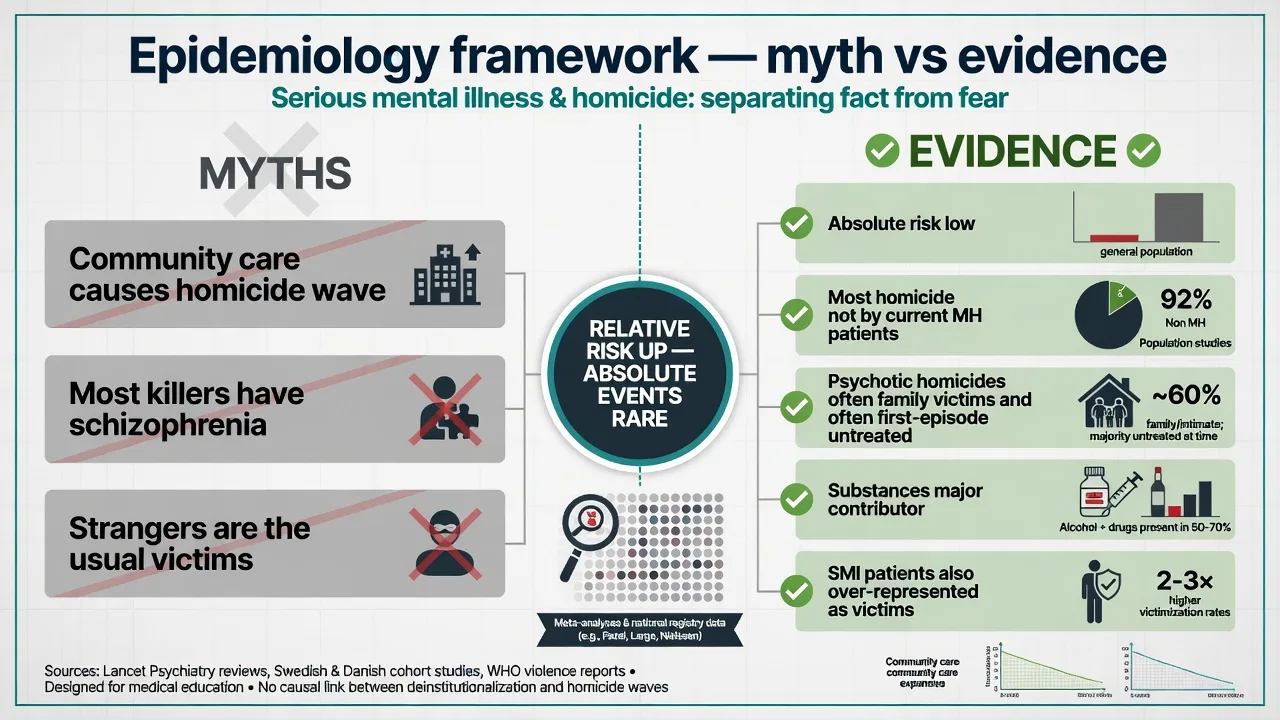
Schizophrenia spectrum disorders elevate relative odds of violence and, in some datasets, homicide, yet absolute homicide risk remains low and most people with schizophrenia are never violent.[7][8][18] Finnish forensic data illustrated large odds ratios for schizophrenia and especially antisocial personality disorder for homicidal behaviour, while affective and anxiety disorders did not show comparable elevation — useful for viva discrimination, not for predicting any individual.[7]
Population-impact work shows severe mental illness accounts for a minority share of violent crime overall; public-protection policy that focuses only on "the mentally ill" will miss most violence.[21]
National clinical surveys (England and Wales teaching core)
In a large national clinical survey of people convicted of homicide, about one-third had a lifetime mental disorder diagnosis; schizophrenia lifetime was around five percent of perpetrators, and symptoms of mental illness at the offence were present in a smaller subset. Most perpetrators had not been under recent specialist care.[3] Among perpetrators with schizophrenia, clinical features and service-contact patterns are highly examinable (illness duration, substances, prior violence, family victims).[4]
Taylor and Gunn's classic "myth and reality" argument remains viva gold: high-profile killings are used to claim community care has failed, yet the epidemiology does not support a simple narrative that deinstitutionalisation caused a homicide wave by people with mental illness.[1] A fifty-year England and Wales analysis of homicide due to mental disorder showed rate patterns that diverged from total homicide trends after the mid-1970s — candidates should cite the direction of argument (not invent yearly counts).[2]
Longer-term trend work continues to track rates and court outcomes (hospital orders vs imprisonment) for mentally disordered homicide offenders — disposal patterns shift with law, service design, and clinical practice, not with diagnosis alone.[16]
First-episode concentration
Among people who kill during psychotic illness, meta-analysis shows a large proportion of homicides occur during the first episode of psychosis before treatment (pooled estimate about two-fifths in the Nielssen and Large meta-analysis).[5] Duration of untreated psychosis associates with the proportion of psychotic homicides occurring before treatment — early detection is a prevention theme, not a promise of zero risk.[6] Australian (NSW) series of homicide during psychotic illness reinforce the same clinical message for FRANZCP candidates: untreated psychosis and family victims are high-yield patterns.[22]
Substances, strangers, gender, victims
Alcohol or drug misuse contributes to a substantial share of homicides in national series — dual diagnosis is not a side note.[10] Stranger homicide by people with psychotic illness is real but over-emphasised relative to family and acquaintance victims; media salience is not base-rate teaching.[11] Gender analyses show female perpetrators more often kill family members and have higher recorded rates of mental illness than male perpetrators in population descriptive work.[23] Domestic homicide analyses similarly find mental illness at the offence in a minority, with important subtype variation.[14]
People with mental illness are also over-represented as victims of homicide — victimology is an examiner discriminator against one-sided "dangerous patient" framing.[15]
Pathophysiology and mechanisms
Multi-level model
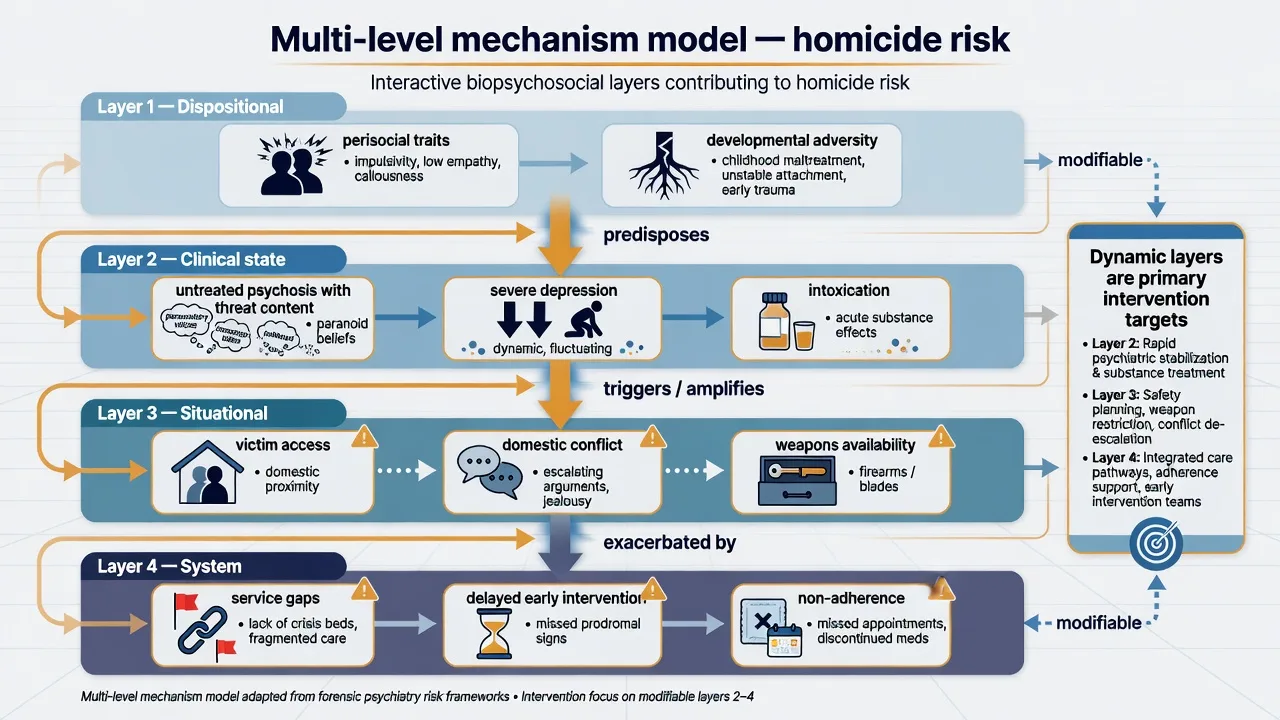
- Dispositional — antisocial traits, impulsivity, developmental adversity, prior violence history.
- Clinical state — untreated psychosis with threat/control-override or persecutory content; severe depression (filicide, homicide-suicide); mania; intoxication/withdrawal.
- Situational — access to a known victim (often family or partner), weapons, acute conflict, domestic breakdown.
- System — delayed FEP treatment, non-adherence, fragmented dual-diagnosis care, weak multi-agency information sharing.[5][9][18]
Psychosis and delusion content
Meta-analytic work supports psychosis as a risk factor for violence to others with modest average effect sizes and substantial heterogeneity — content, substances, and treatment status matter.[18] In untreated schizophrenia, emergence of persecutory delusions associates with violence more than the schizophrenia label alone.[19] MacArthur Violence Risk Assessment Study data showed that delusions as a broad class were not a simple universal driver of violence after discharge; examiners reward nuanced discussion of threat content, substance use, and prior violence rather than "delusions cause homicide" slogans.[20] Meta-regression of violence risk factors in psychosis repeatedly highlights prior violence, substance misuse, non-adherence, and hostility/impulsivity domains as concentrators.[9]
Prevention mechanism (exam pearl)
If a large share of psychotic homicide clusters before first treatment, then reducing duration of untreated psychosis, improving early detection of FEP, and engaging dual-diagnosis care are structural prevention strategies with a clearer logic than fear-based detention of all people with schizophrenia.[5][6]
Clinical presentation
Pre-offence patterns examiners use
- Young adult with emerging untreated psychosis, family noticing fearfulness, sleep loss, persecutory talk, and social withdrawal — then a sudden lethal assault on a parent or co-resident.[5][22]
- Known schizophrenia with non-adherence, stimulant or alcohol relapse, rising hostility, and loss of contact with services.[4][9]
- Intimate-partner escalation with jealousy, depression, or substance use; sometimes without any psychotic illness.[14]
- Maternal severe depression or psychosis with altruistic or extended-suicide themes toward children.[12]
- Homicide-suicide pathway with severe depression, domestic breakdown, or morbid jealousy themes.[13]
Post-offence presentations
Custody or secure hospital: residual psychosis, clearing intoxication, claimed amnesia, profound guilt and suicide risk, or organised denial. Immediate priorities are safety (including suicide prevention after homicide), medical stabilisation, and lawful information-gathering for later forensic opinion — not a rushed ultimate-issue verdict on day one.[17]
Differential diagnosis of the "homicide picture"
- Threat/persecutory content
- Often family victim
- FEP untreated high yield
- Treat illness urgently
- Timeline to intoxication
- Stimulant paranoia
- Reassess when sober
- SUD is risk treatment
- Planning and gain
- Personality history
- Limited mental-impairment role
- RNR / security focus
Also separate severe depression / filicide / homicide-suicide, morbid jealousy (dedicated topic), organic states (delirium, encephalitis, TBI), and malingered psychosis after arrest. Malingering is a late hypothesis after multi-source inconsistency analysis, not a default when a defence is raised.[12][13][17]
Assessment after homicide
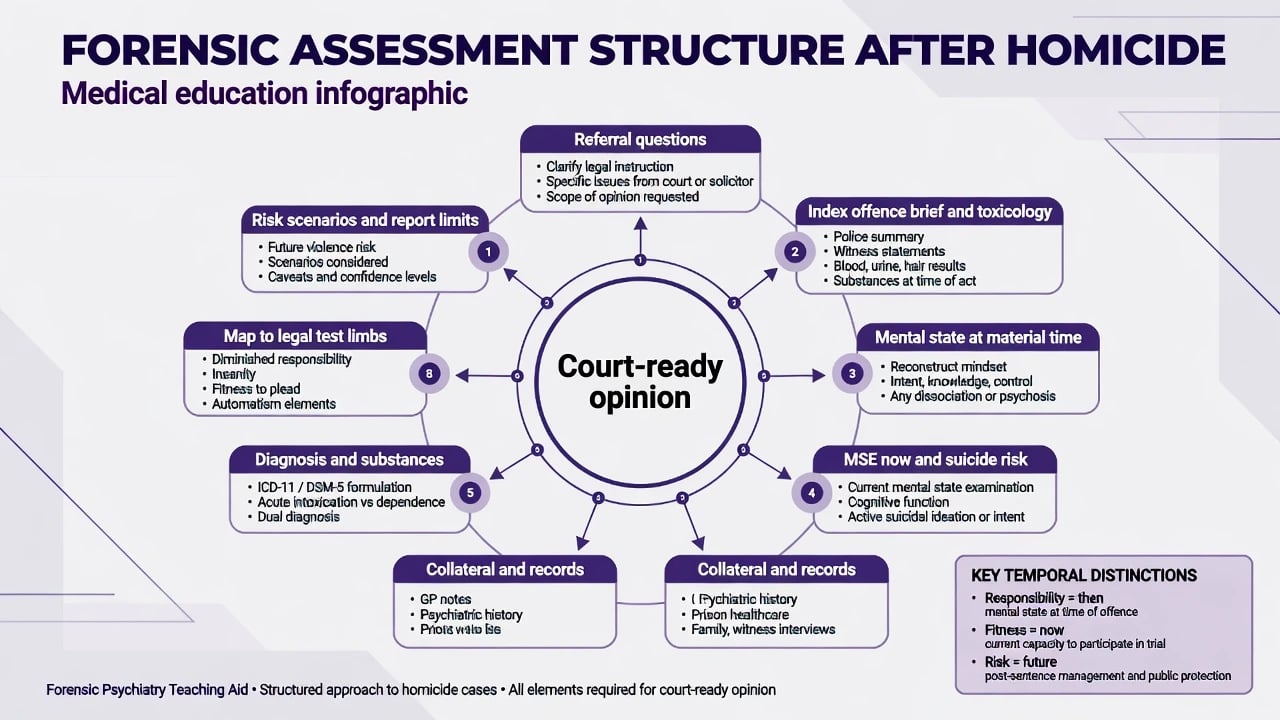
Separate the legal questions
Keep three products distinct in every report: responsibility for the offence, present fitness for trial, and future risk for leave or public protection.[17]
| Question | Time point | Product |
|---|---|---|
| Criminal responsibility / mental impairment / insanity | Then (offence) | Opinion mapped to legal limbs |
| Fitness / competence / fitness to plead | Now (trial) | Present adjudicative abilities |
| Future violence risk | Future scenarios | Formulation, scenarios, management plan |
| Disposal / secure care recommendation | After verdict / under local law | Jurisdiction-specific principles only |
| Never invent statute section numbers. Name that verdict labels (NGRI, NGMI, mental impairment, diminished responsibility) and burdens of proof are jurisdiction-specific.[17] |
Multi-source reconstruction
Minimum data set for a defensible responsibility opinion:
- Police brief, witness accounts, body-worn video where available.
- Toxicology and medical findings at arrest.
- Prior psychiatric notes, medication adherence, FEP timeline / DUP.
- Collateral from family and custody staff.
- MSE with quoted content about beliefs, wrongfulness, and planning.
- Substance timeline independent of self-report alone.[17][22]
Future risk after the index
Even after a completed homicide, secure care, leave, and eventual community supervision require SPJ-style formulation (who might be harmed, under what circumstances, what prevents it). Risk instruments offer only moderate group-level accuracy and never replace scenarios and a plan.[24]
Investigations
- Toxicology — essential for substance pathway discrimination.[10]
- Medical / organic screen when delirium, encephalitis, seizure disorder, or head injury is plausible.
- Cognitive testing / formal ID assessment when intellectual disability or dementia is in play.
- Structured violence risk tools (HCR-20-style SPJ concepts) for future risk management — not as a substitute for reconstructing past intent.[24]
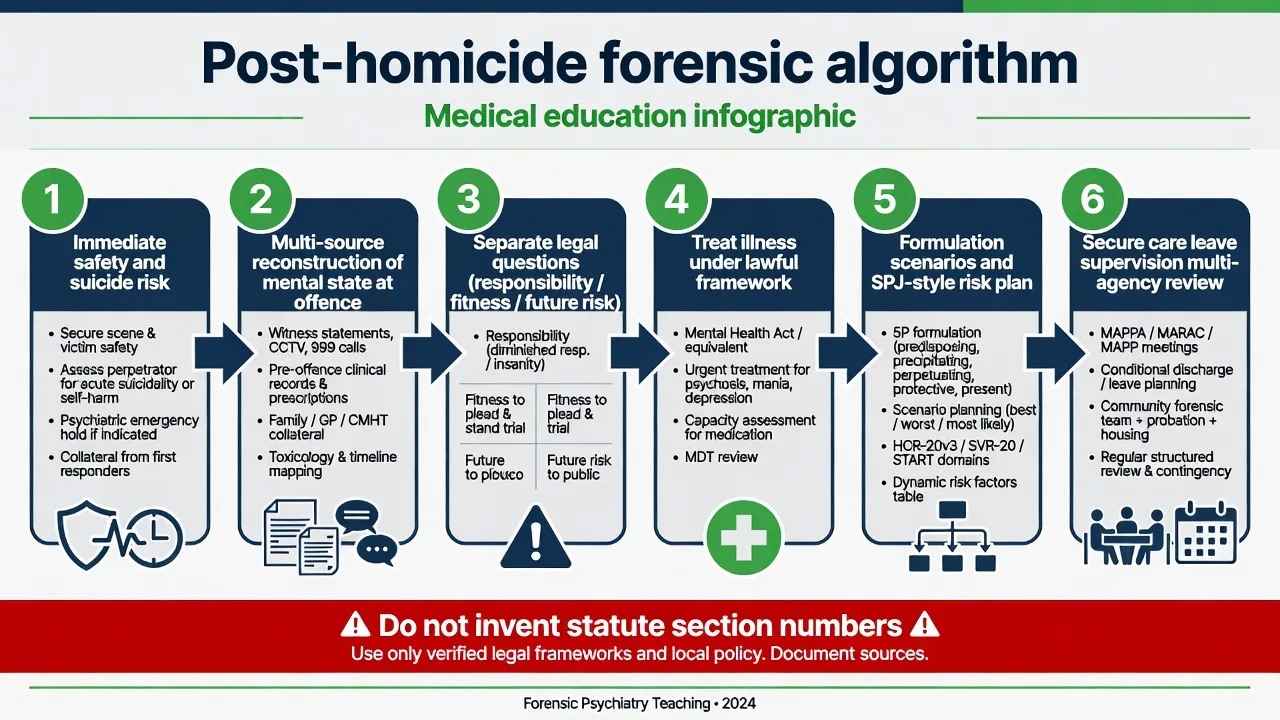
Acute management
Immediate priorities after alleged homicide:
- Safety of co-detainees, staff, and the person (high suicide risk).
- Treat acute psychosis, severe agitation, withdrawal, and medical complications under the lawful custody/hospital framework of the jurisdiction (principles only).
- Avoid detailed forensic interviews while delirious or heavily intoxicated if reliability will collapse.
- Court liaison for assessment pathways without forcing empty process when obviously unfit.[17]
Antipsychotic choice and dosing follow ordinary acute-psychosis standards for the clinical picture; document agent, dose, route, and monitoring, and avoid inventing a special "homicide dose." Treat substances concurrently because substance misuse is a major contributor in homicide series and a core dynamic risk concentrator in psychosis.[9][10][17]
Definitive management and legal-clinical pathway
Criminal responsibility analysis (principles)
AAPL-style insanity/mental-impairment evaluation methodology (portable principles): clarify the legal test; obtain multi-source data; establish presence of a mental condition at the material time; analyse nexus to knowledge of nature/quality, wrongfulness, and (where local law allows) control; address substances, malingering, and alternative explanations; write limitations clearly.[17]
If mental impairment / NGRI / NGMI pathway
Secure hospital or forensic pathway principles apply. This is not automatic community release. Treatment of psychosis, substance programmes, graded leave, victim-related conditions, and multi-agency public protection frameworks (MAPPA-like principles in the UK; local forensic/community partnerships in ANZ) structure long-term care. Disposal and review rights are jurisdiction-specific.[16][17]
If convicted and imprisoned
Prison mental health care, suicide prevention, and sentence-plan risk work continue. Recidivist homicide is uncommon but over-represented in some mentally abnormal offender subgroups in Finnish series — residual risk management remains mandatory.[7]
Prevention and public mental health
- Early intervention in psychosis and reduced DUP.[5][6]
- Integrated dual-diagnosis care.[9][10]
- Domestic-violence and filicide-aware perinatal/parenting pathways.[12][14]
- Continuity after discharge and adherence support for known psychosis.[4][9]
- Honest public communication: absolute risk low; treatable risk factors exist; stigma-based policy is bad epidemiology.[1][21]
Subtypes and high-yield scenarios
First-episode psychotic homicide
Often family victim, untreated illness, limited prior service contact. Criminal-responsibility analysis focuses on contemporaneous psychotic content and knowledge of wrongfulness/nature; prevention teaching focuses on FEP systems.[5][22]
Relapsed treated schizophrenia
Non-adherence, substances, and service disengagement dominate. Future-risk work targets adherence, dual diagnosis, and supervision intensity.[4][9]
Stranger homicide and psychosis
Rare relative to family victims; high media salience. Still requires full multi-source analysis — rarity does not equal impossibility.[11]
Filicide
National series: mental illness is not present in most filicides overall, but mothers more often have mental disorder and symptoms at offence than fathers; affective illness is prominent; a subset have schizophrenia/delusional disorders. Service monitoring of severely ill parents is a prevention theme without pathologising all parental homicide.[12]
Homicide-suicide
National consecutive case series link mental disorder (especially depression and some personality/relationship pathology) to a substantial share of homicide-suicide events; clinical prevention includes depression treatment, domestic-violence pathways, and lethal-means awareness in high-conflict dyads.[13]
Domestic homicide
Approximately one in ten convicted homicide perpetrators in England and Wales teaching series have symptoms of mental illness at the time of homicide overall; domestic contexts need both mental-health and domestic-violence frameworks.[14]
Complications and pitfalls
- Inflating absolute risk from relative-risk headlines.[1][8]
- Equating diagnosis with legal insanity.[17]
- Ignoring substances and prior violence.[9][10]
- Over-focusing on stranger risk while missing family victims and FEP untreated pathways.[5][11]
- Mixing fitness (now) with responsibility (then).[17]
- Inventing statute section numbers or universal form codes.
- Under-calling suicide risk after homicide.
- Forgetting patients with mental illness as victims of homicide.[15]
- Using a single actuarial score as destiny for leave or release.[24]
Prognosis and disposition
Psychotic homicide is often a single catastrophic pathway rather than a serial pattern, but residual violence risk still requires structured management. Homicide recidivism risk is higher in some mentally abnormal offender groups than in ordinary homicide samples in Finnish data, yet remains a rare absolute event — manage scenarios, do not promise zero risk.[7] Court outcomes (hospital vs prison) for mentally disordered homicide offenders have shifted over decades; know that trends exist and that local law governs disposal.[16]
Special populations
- Women — higher relative rates of recorded mental illness among female homicide perpetrators; family victims more common.[23]
- Parents — filicide-specific mental-illness patterns; perinatal and child-protection interface.[12]
- Youth — conduct, substance, and developmental pathways often dominate over classic late-onset psychosis teaching cases.
- Older adults — depression, cognitive disorders, carer stress, homicide-suicide dyads.[13]
- SMI as victims — elevated homicide victimisation risk; safety planning is bidirectional.[15]
- Cultural / Indigenous defendants — interpreter, cultural formulation, bias awareness; local protocols; no invented universal procedure.
Evidence and guidelines
Core evidence set for this topic:
- Myth vs reality and long-run mental-disorder homicide rates.[1][2]
- NCISH-linked national clinical surveys of mental disorder, schizophrenia, substances, domestic homicide, filicide, homicide-suicide, and long-term court outcome trends.[3][4][10][12][13][14][16]
- FEP concentration and DUP association.[5][6][22]
- Diagnostic ORs, schizophrenia-violence metas, psychosis-violence metas, and risk-factor metas.[7][8][9][18]
- Delusion content nuance (Keers; MacArthur).[19][20]
- Population impact of SMI on violent crime.[21]
- AAPL insanity evaluation methodology for responsibility opinions.[17]
- Risk-instrument performance humility for future risk.[24]
RANZCP / NICE / APA do not publish a single "homicide guideline"; examiners expect synthesis of forensic epidemiology, early-intervention psychosis standards, dual-diagnosis care, domestic-violence pathways, and jurisdiction-specific mental impairment law by principle, anchored to national inquiry series and AAPL-style evaluation methodology.[1][3][5][17]
Exam pearls
HOMICIDE-MD exam grid
References
- [1]Taylor PJ, Gunn J Homicides by people with mental illness: myth and reality Br J Psychiatry, 1999.PMID 10211145
- [2]Large M, Smith G, Swinson N, et al. Homicide due to mental disorder in England and Wales over 50 years Br J Psychiatry, 2008.PMID 18669997
- [3]Shaw J, Hunt IM, Flynn S, et al. Rates of mental disorder in people convicted of homicide. National clinical survey Br J Psychiatry, 2006.PMID 16449701
- [4]Meehan J, Flynn S, Hunt IM, et al. Perpetrators of homicide with schizophrenia: a national clinical survey in England and Wales Psychiatr Serv, 2006.PMID 17085616
- [5]Nielssen O, Large M Rates of homicide during the first episode of psychosis and after treatment: a systematic review and meta-analysis Schizophr Bull, 2010.PMID 18990713
- [6]Large M, Nielssen O Evidence for a relationship between the duration of untreated psychosis and the proportion of psychotic homicides prior to treatment Soc Psychiatry Psychiatr Epidemiol, 2008.PMID 17960314
- [7]Eronen M, Hakola P, Tiihonen J Mental disorders and homicidal behavior in Finland Arch Gen Psychiatry, 1996.PMID 8639032
- [8]Fazel S, Gulati G, Linsell L, et al. Schizophrenia and violence: systematic review and meta-analysis PLoS Med, 2009.PMID 19668362
- [9]Witt K, van Dorn R, Fazel S Risk factors for violence in psychosis: systematic review and meta-regression analysis of 110 studies PLoS One, 2013.PMID 23418482
- [10]Shaw J, Hunt IM, Flynn S, et al. The role of alcohol and drugs in homicides in England and Wales Br J Psychiatry, 2006.PMID 16869841
- [11]Nielssen O, Bourget D, Laajasalo T, et al. Homicide of strangers by people with a psychotic illness Schizophr Bull, 2011.PMID 19822580
- [12]Flynn SM, Shaw JJ, Abel KM Filicide: mental illness in those who kill their children PLoS One, 2013.PMID 23593128
- [13]Flynn S, Gask L, Appleby L, et al. Homicide-suicide and the role of mental disorder: a national consecutive case series Soc Psychiatry Psychiatr Epidemiol, 2016.PMID 27086087
- [14]Oram S, Flynn SM, Shaw J, et al. Mental illness and domestic homicide: a population-based descriptive study J Interpers Violence, 2013.PMID 23820784
- [15]Rodway C, Flynn S, While D, et al. Patients with mental illness as victims of homicide: a national consecutive case series Lancet Psychiatry, 2014.PMID 26360576
- [16]Flynn S, Ibrahim S, Kapur N, et al. Mental disorder in people convicted of homicide: long-term national trends in rates and court outcome Br J Psychiatry, 2021.PMID 32624025
- [17]American Academy of Psychiatry and the Law AAPL Practice Guideline for forensic psychiatric evaluation of defendants raising the insanity defense J Am Acad Psychiatry Law, 2014.PMID 25492121
- [18]Douglas KS, Guy LS, Hart SD Psychosis as a risk factor for violence to others: a meta-analysis Psychol Bull, 2009.PMID 19702378
- [19]Keers R, Ullrich S, Destavola BL, et al. Association of violence with emergence of persecutory delusions in untreated schizophrenia Am J Psychiatry, 2014.PMID 24220644
- [20]Appelbaum PS, Robbins PC, Monahan J Violence and delusions: data from the MacArthur Violence Risk Assessment Study Am J Psychiatry, 2000.PMID 10739415
- [21]Fazel S, Grann M The population impact of severe mental illness on violent crime Am J Psychiatry, 2006.PMID 16877653
- [22]Nielssen OB, Westmore BD, Large MM, et al. Homicide during psychotic illness in New South Wales between 1993 and 2002 Med J Aust, 2007.PMID 17371211
- [23]Flynn S, Abel KM, While D, et al. Mental illness, gender and homicide: a population-based descriptive study Psychiatry Res, 2011.PMID 20724002
- [24]Fazel S, Singh JP, Doll H, et al. Use of risk assessment instruments to predict violence and antisocial behaviour in 73 samples involving 24 827 people: systematic review and meta-analysis BMJ, 2012.PMID 22833604