Psych · Forensic psychiatry — mental health law
Mental health law and involuntary treatment
Also known as Compulsory treatment · Civil commitment · Involuntary admission · Community treatment order · CTO · Outpatient commitment · Least restrictive care · Mental Health Act principles · Coercion in psychiatry
Exam-exhaustive fellowship reference on mental health law and involuntary treatment — principles of compulsory care, least restrictive alternative, capacity vs Mental Health Act frameworks, community treatment orders, human rights, perceived coercion, seclusion/restraint last resort, and jurisdiction-specific caution (do not invent section numbers). FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Mental health law structures when the state may authorise psychiatric assessment, detention, and treatment without the person's contemporaneous capacious consent. Clinicians must navigate three overlapping constructs: clinical need and risk, decision-making capacity, and statutory authority. Confusing them is the classic exam and practice failure.[9][17][21]
Involuntary (compulsory) treatment means care or detention under legal powers when valid informed consent is absent or overridden by statute. It includes emergency holds, compulsory inpatient admission, enforced medication under lawful authority, and community treatment orders (CTOs) / involuntary outpatient commitment. Voluntary status requires free agreement after adequate information; informal coercion (pressure, leverage, "sign or we section you") can make "voluntary" status ethically and legally fragile even when paperwork looks clean.[10][11]
Jurisdiction caution (non-negotiable). Mental Health Acts, capacity statutes, guardianship schemes, ages of majority, time limits, second-opinion rules, and tribunal names differ across Australian states and territories, New Zealand, UK nations, US states, and elsewhere. Examiners reward principles and local humility. Inventing section numbers is a fail.[13][14][21]
Classification — legal frameworks that examiners map
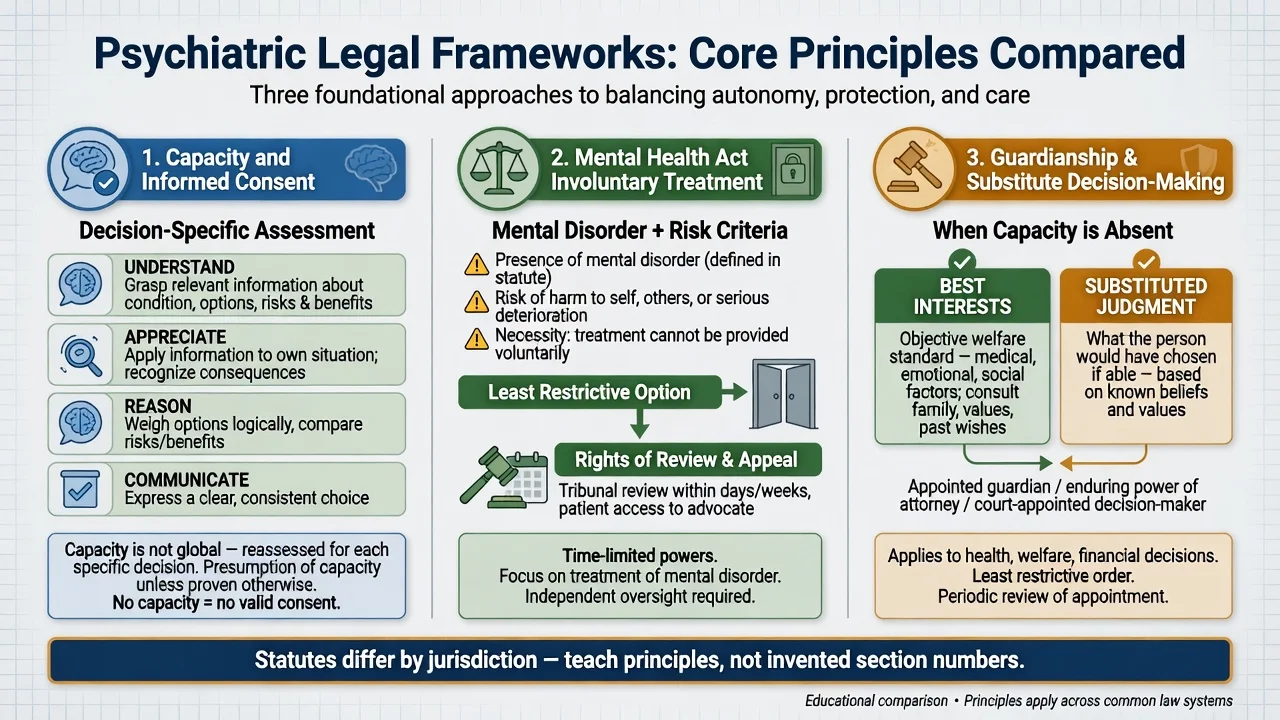
1. Capacity and informed consent framework
Capacity is decision-specific and time-specific. Classic functional abilities (Appelbaum/Grisso; MacCAT-T structure): understand relevant information; appreciate the situation and consequences; reason (use or weigh options); communicate a choice. Presumption of capacity; diagnosis alone is not incapacity. Medical and psychiatric inpatients both show substantial incapacity rates in landmark studies, with cognitive impairment, acute illness, psychosis, and poor insight as predictors.[15][16][17][18][19]
If capacity is present, respect informed consent or informed refusal — even of beneficial treatment — unless a separate statutory Mental Health Act pathway lawfully applies for psychiatric treatment under local criteria.[17][18]
2. Mental Health Act / civil commitment framework
Most civil commitment systems require some combination of: a defined mental disorder (or equivalent statutory concept); risk of harm to self or others and/or inability to meet basic needs / grave disability / need for treatment that cannot be delivered voluntarily; and application of the least restrictive option capable of achieving the lawful aim. Time limits, who may apply, second opinions, and review bodies are local. US civil commitment history shows evolution of dangerousness and grave-disability standards with large state variation.[13][14][21]
3. Guardianship / substitute decision-making
When capacity for a decision is lacking, substitute frameworks may authorise decisions using best interests and/or substituted judgment standards, often with different scope for medical, financial, and residential decisions. These pathways are not interchangeable with Mental Health Act detention powers; using the wrong pathway is a viva trap.[17][21]
Status taxonomy (operational)
- Capacious agreement
- Can leave (with process caveats)
- Watch for pressure/coercion
- Reassess if mental state changes
- Statutory detention
- Treatment under Act principles
- Rights: info, advocacy, review
- Revoke when criteria lapse
- Compulsory community conditions
- Recall/enforcement concepts
- Mixed outcome evidence
- Not a substitute for services
Epidemiology and patterns of compulsion
Compulsory admission rates and legal grounds vary widely across European and other systems — a reminder that "how we do it here" is not a natural law.[13][14]
Correlates of involuntary care commonly include psychosis, elevated risk, prior compulsory episodes, limited insight, and service-system factors. Ethnicity and social disadvantage associate with higher coercion in some settings; reflective practice and equity are clinical duties, not optional add-ons.[10][12]
Perceived coercion is not identical to legal status. Classic work shows pressure and process shape how coercive an admission feels — including among legally voluntary patients.[11] Qualitative work finds patients judge involuntary hospitalisation as "right" or "wrong" based on respect, necessity, fairness, and later benefit — process quality is part of outcome.[12]
CTO use intensity varies internationally. Meta-analytic work suggests observed benefits after CTOs can have an inverse relationship with how widely CTOs are used — supporting selective, not industrial, deployment.[5]
Pathophysiology and mechanisms — ethics and clinical drivers
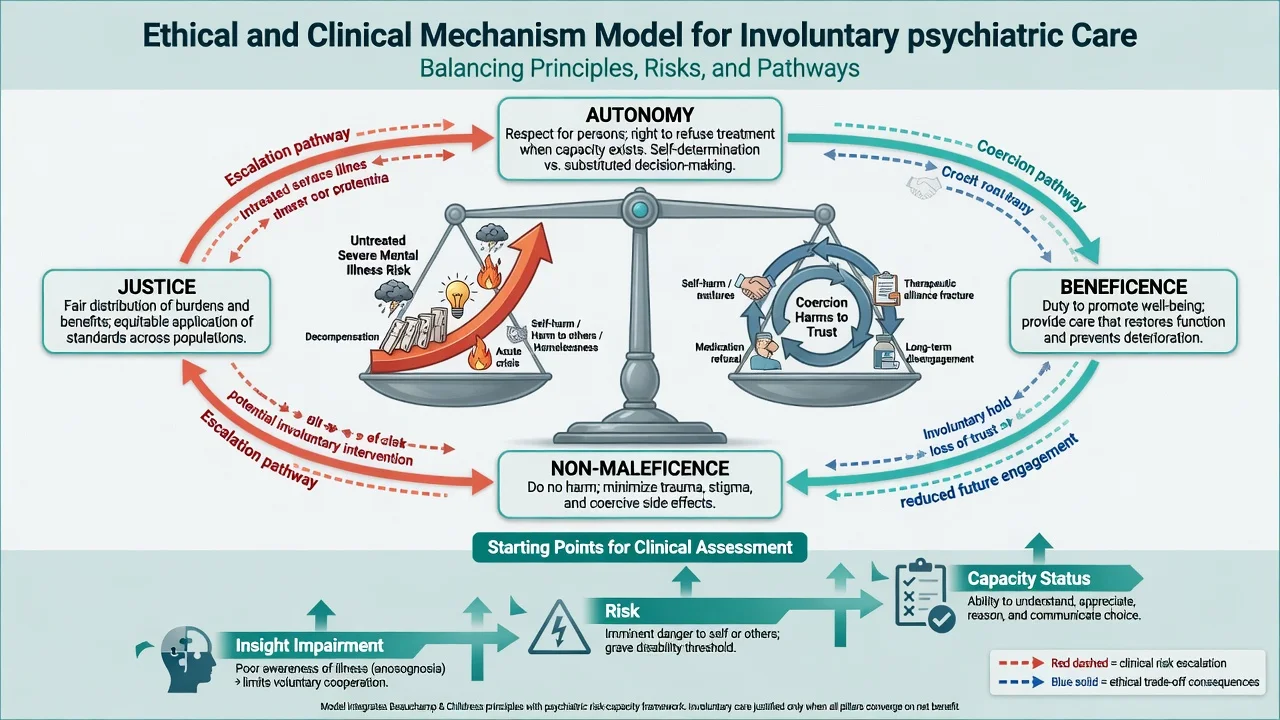
Compulsory powers sit at the collision of autonomy (self-determination when capacious), beneficence (treat illness and prevent deterioration), non-maleficence (avoid trauma of force and restrictive practices), and justice (fair application, non-discrimination, resource equity).[9][10]
Clinically, impaired insight, delusional appraisal of risk, manic grandiosity, severe depression with nihilism, and cognitive impairment can block voluntary engagement. Insight is related to but not identical with capacity: people may understand facts yet fail to appreciate their applicability, or may retain capacity for some decisions while lacking it for others.[17][18]
Coercion can be iatrogenic: eroding trust, reducing future help-seeking, and producing trauma — especially with seclusion/restraint, which systematic review links to significant adverse effects and requires last-resort use with safeguards.[10][20] Conversely, untreated severe mental illness can escalate suicide, violence, medical neglect, and social collapse. The clinical art is proportionate, time-limited intervention with continuous reassessment.[7][8]
Clinical presentation
Exam stems cluster around: untreated first-episode psychosis refusing admission with clear risk; mania demanding discharge from ED with financial ruin and sexual disinhibition risks; severe depression with active suicidal planning wanting to leave; relapsing schizophrenia on a CTO with non-attendance and early relapse signs; family insisting on "sectioning" when criteria are not met; "voluntary" patient who signed under threat and later says they were forced; older adult with dementia (Mental Health Act vs guardianship interface); personality disorder crisis where detention is requested for containment alone.[4][10]
Atypical and high-yield traps: quiet competent refusal of recommended care; fluctuating capacity after partial treatment; language barriers mistaken for lack of insight; cross-cultural explanatory models misread as delusion without interpreter and cultural formulation.[10][12][18]
Differential diagnosis of legal pathways
- Statutory mental disorder + risk tests
- Psychiatric treatment focus
- Detention/recall powers
- Tribunal/review rights
- Decision-specific functional test
- Consent or substitute decision
- General medical and psych decisions
- Not automatic detention
- Imminent serious harm
- Time-critical treatment
- Document common-law/statute basis
- Reassess as soon as safe
Also separate: forensic court orders vs civil orders; adult safeguarding vs psychiatric detention; substance intoxication alone vs primary mental illness meeting criteria; pure antisocial behaviour without qualifying mental disorder under local definitions.[9][21]
Clinical and bedside assessment
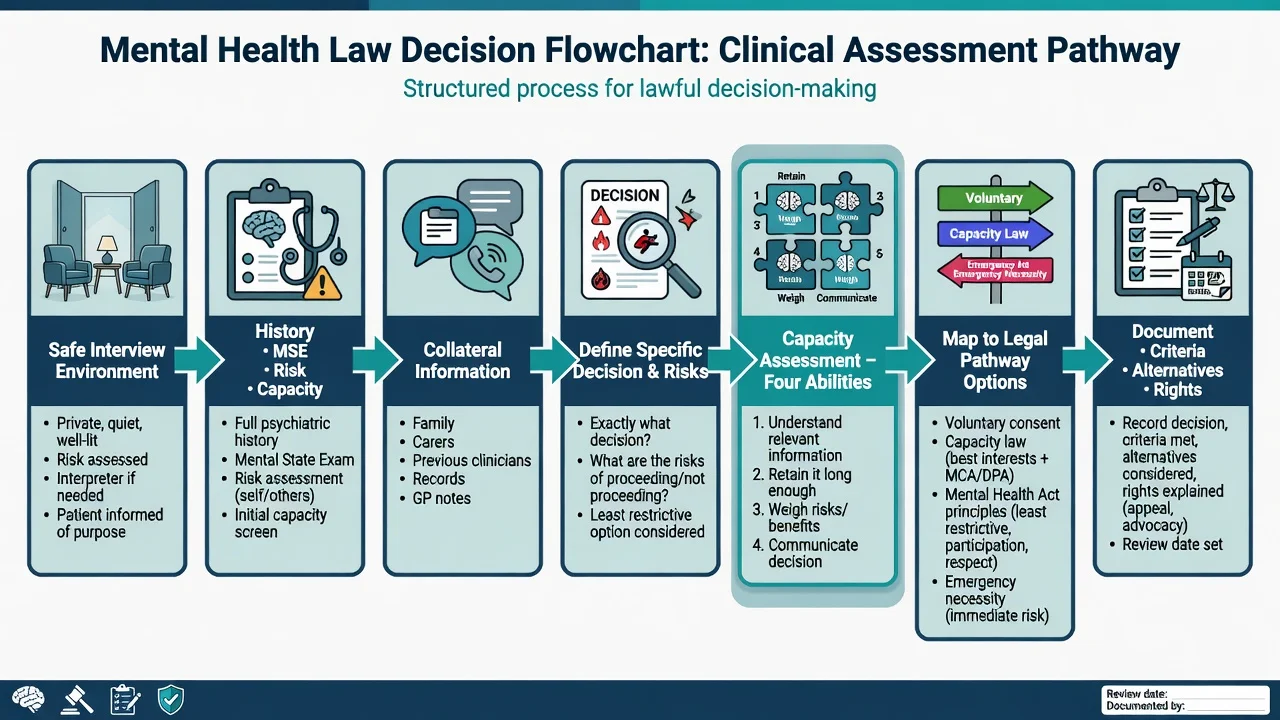
Structure the assessment
- Safety of the interview — environment, exits, security if needed, medical stability.
- Define the problem — what decision or legal question is being asked today?
- Mental disorder — nature, severity, course; organic differentials if indicated.
- Risk — suicide, self-neglect, violence, vulnerability, deterioration; scenarios not labels alone.
- Capacity for the specific decision — information given, teach-back, each ability probed.[19]
- Least restrictive options — what has been tried or is available now?
- Patient views, values, advance statements — and carer perspectives with confidentiality boundaries.
- Statutory pathway — apply local criteria honestly; do not stretch criteria for convenience.
- Rights process — information, advocacy, appeal/review routes under local law.
- Documentation and review date.
Capacity tools
The MacCAT-T operationalises understanding, appreciation, reasoning, and expressing a choice for treatment decisions. It structures the interview; it does not replace legal determination or Mental Health Act criteria.[19] Cognitive screens (MMSE/MoCA) are adjuncts only.
LAWFUL
Investigations
No blood test confers legal status. Investigate for organic contributors (delirium work-up, metabolic panel, substances, imaging/EEG when indicated) because treatable medical causes change both clinical and legal trajectories. Document the facts supporting criteria: quoted speech, collateral, observed behaviour, risk incidents, capacity findings per ability, alternatives considered, and who was informed of rights.[17][18]
Management — immediate (resuscitation of safety and process)
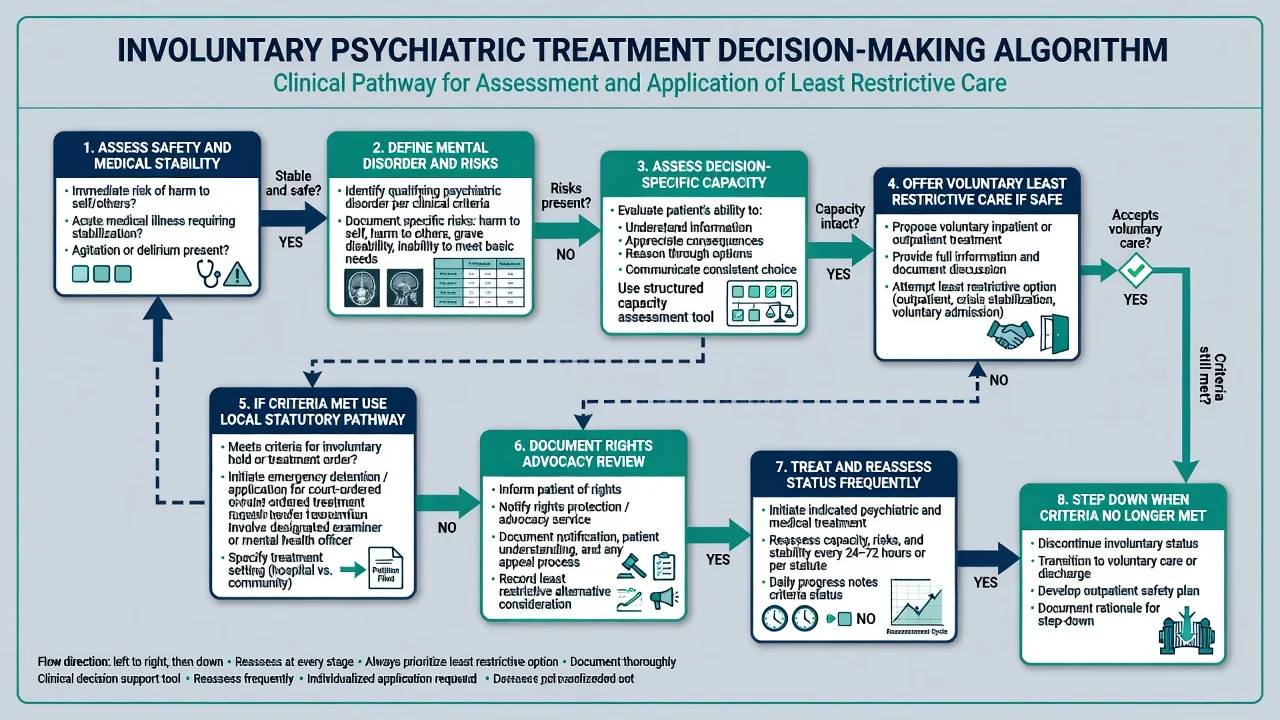
Immediate priorities: (1) medical and behavioural safety — ABC if needed, weapons, environment, de-escalation before restraint; (2) treat reversible drivers of agitation or incapacity where possible; (3) offer voluntary care if capacity and risk allow a safe voluntary pathway; (4) if not, apply the local emergency or compulsory pathway that actually fits — principles of necessity, proportionality, and least restriction; (5) explain (as far as possible) what is happening, why, and rights of review; (6) start clinical treatment promptly once authorised; (7) set a review time for mental state and legal status.[9][10][20]
Management — definitive and stepwise
Least restrictive ladder
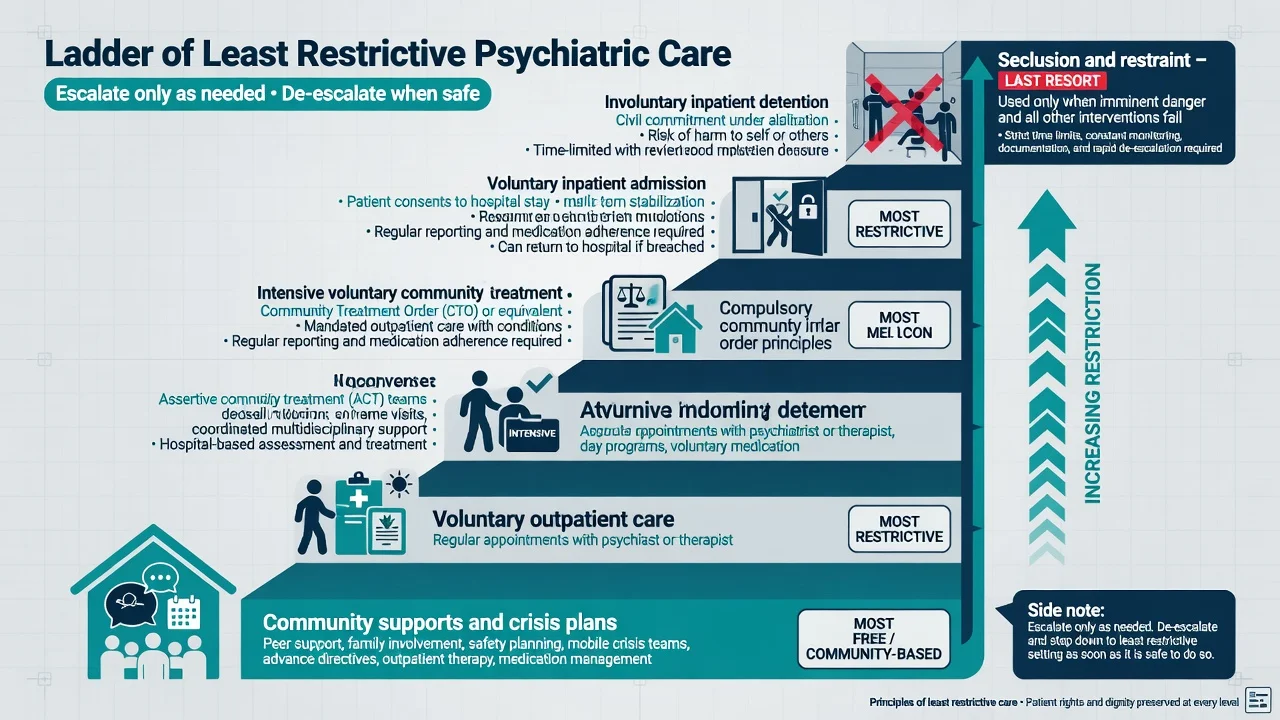
Think in ascending intrusiveness: crisis planning and community supports → voluntary outpatient → intensive voluntary community care (e.g. assertive outreach concepts) → compulsory community powers where available → voluntary inpatient → involuntary inpatient → seclusion/restraint as last resort. Always ask: what is the least restrictive setting that is still safe and lawful for this person today?[4][9][20]
Community treatment orders / outpatient commitment
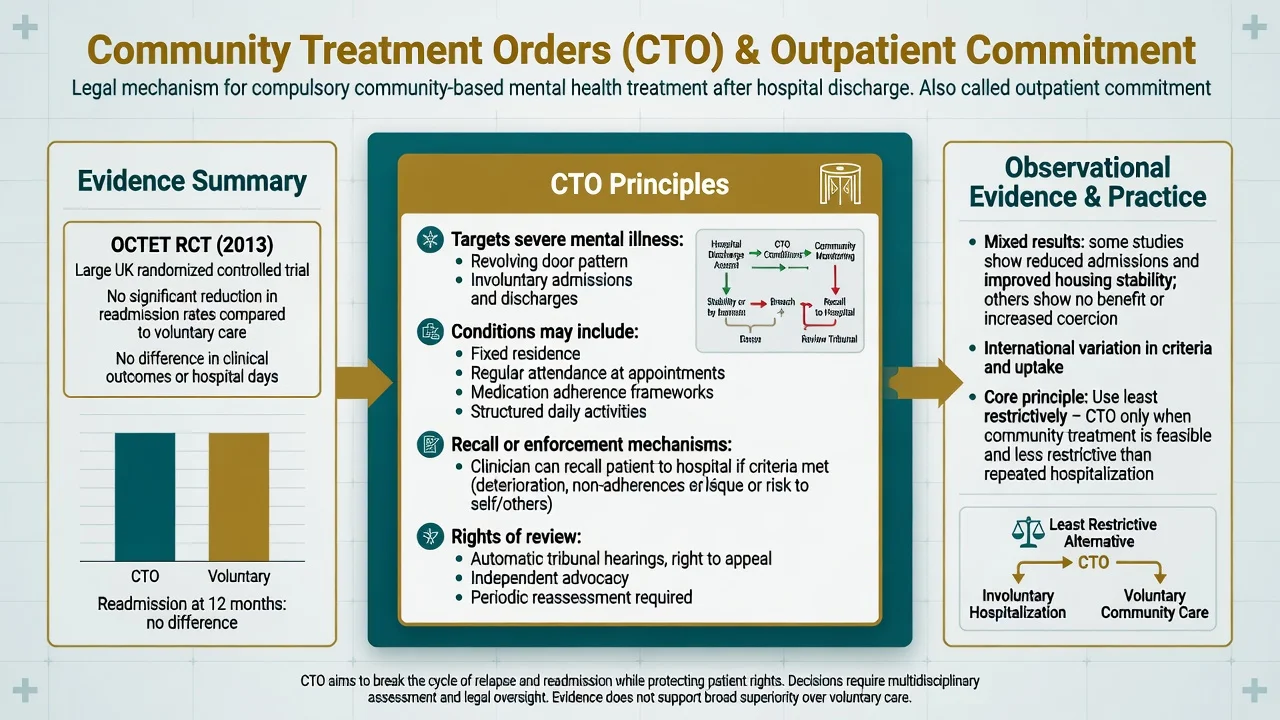
Concept. CTOs (and US outpatient commitment analogues) impose compulsory conditions in the community — often residence, attendance, and treatment adherence frameworks — with mechanisms to recall or enforce when criteria are met. Exact conditions and thresholds are statute-specific.[4][6]
Evidence (exam high-yield): OCTET (England) — RCT of CTOs versus leave under shorter-term powers in patients with psychosis showed no significant reduction in readmission over 12 months, with related follow-up and economic analyses not showing clear advantage;[1][23][24] Cochrane and systematic reviews — limited evidence that compulsory community treatment reduces service use or improves outcomes broadly;[2][3][4] US RCTs (e.g. North Carolina) — some benefit on hospital recidivism when outpatient commitment was sustained and paired with intensive services;[6] use intensity — benefits may inverse with high population rates of CTO use, so select carefully.[5]
Clinical use principles: consider for revolving-door severe mental illness where voluntary engagement has repeatedly failed and community compulsion is less restrictive than repeated detention; pair with real services; review and discharge from order when criteria fade; never use as punishment or resource shortcut.[4][5]
Inpatient compulsory care
Outcomes of involuntary versus voluntary admission are heterogeneous; symptom improvement can occur under both pathways, and multi-centre observational data show symptom change after coerced admission is complex and not uniformly negative or positive.[7][8] Focus on: lawful criteria; dignity; information; advocacy; therapeutic engagement; physical health; early leave planning; and status review as mental state improves — many regain capacity after treatment and should be re-consented.[22]
Restrictive practices
Seclusion and restraint: last resort for imminent harm when alternatives fail; continuous observation; shortest duration; post-event debrief for patient and staff; governance review. Harms are well documented in systematic review.[20]
Specific subtypes and scenarios
| Scenario | High-yield principle |
|---|---|
| ED short hold | Emergency safety + rapid full assessment; do not convert into de facto long detention without authority |
| FEP refusal | High clinical stakes; least restrictive still applies; early treatment windows matter |
| CTO breach | Assess risk and criteria now; recall is not automatic vengeance — document current tests |
| Dementia / older adult | Capacity + guardianship interface often primary; MH Act not a default nursing-home tool |
| Youth | Age thresholds and parental consent rules are local; developmental capacity principles |
| Intellectual disability | Supported decision-making first; dual diagnosis assessment |
| Personality disorder crisis | Detention criteria still require statutory mental disorder/risk tests — not "containment on demand" |
| Forensic dual status | Criminal justice orders vs civil MH powers — clarify which regime applies |
| Cross-cultural | Interpreters; cultural formulation; equity awareness regarding compulsion rates |
Complications and pitfalls
- Inventing section numbers.
- Equating disagreement with incapacity or with dangerousness.
- Using compulsion for social problems without mental disorder criteria.
- Skipping voluntary options that were feasible.
- Ignoring rights communication.
- CTO as paperwork without services.
- Seclusion as culture rather than exception.[20]
- Not revoking when better.
- Mistaking language/cultural barriers for lack of insight.
- Failing to repair the therapeutic alliance after coercion.[10][12]
Prognosis and disposition
Many compulsory episodes are temporary. Plan for recovery of capacity and return to voluntary status; document step-down criteria.[22] Disposition options: revoke and continue voluntary care; step down to CTO only if criteria and least-restrictive test support it; maintain inpatient compulsion if risks and statutory tests persist; involve community teams early. Alliance repair — explaining what happened, inviting narrative, shared crisis planning — is part of disposition quality.[8][12]
Special populations
Children/adolescents: jurisdiction-specific age and parental frameworks; developmental capacity. Older adults: delirium and dementia change capacity and pathway choice. Pregnancy: maternal capacity and risk principles; do not invent special universal sections. Indigenous and ethnic minority patients: higher compulsion rates in some systems demand structural humility, cultural safety, and bias checks. Language barriers: professional interpreters are required for valid process and capacity assessment.[10][14][17]
Evidence, guidelines, and regional differences
Landmark evidence
| Source | Take-home |
|---|---|
| OCTET Burns 2013 | CTO did not reduce 12-month readmission vs leave-based powers in English psychosis sample[1] |
| Kisely Cochrane 2017 | Limited evidence compulsory community treatment improves major outcomes[2] |
| Maughan 2014; Rugkåsa 2016 | Systematic international evidence mixed; no strong general effect on service use[3][4] |
| Kisely 2023 | Benefits inverse to CTO use rates — selective use matter[5] |
| Swartz 1999 | US outpatient commitment benefits under sustained order + services conditions in RCT analyses[6] |
| Kallert reviews | Involuntary vs voluntary outcomes diverse; coercion is multi-dimensional[7][8][9] |
| Newton-Howes 2011 | Correlates and themes of coercion in care[10] |
| Lidz 1995; Katsakou 2012 | Perceived coercion and patient moral appraisal of detention process[11][12] |
| Zinkler 2002; Dressing 2004 | European detention rate and legal variation[13][14] |
| Capacity series | Raymont medical; Cairns/Okai/Owen psychiatric capacity epidemiology and insight links[15][16][17][18] |
| Chieze 2019 | Seclusion/restraint adverse effects systematic review[20] |
Regional deltas (principles only)
Australian state and territory Mental Health Acts and New Zealand legislation differ in definitions, CTO design, time limits, and tribunal structures. Emphasise least restrictive care, rights, and clinical governance — always verify the local Act and forms you are practising under. Do not transpose NSW/VIC/QLD/NZ sections across borders.[4][13][14]
Exam pearls
- Capacity ≠ insight ≠ Mental Health Act criteria — assess each construct.[18]
- OCTET is the high-yield negative CTO trial; do not claim CTOs "proven to stop readmission" universally.[1]
- Least restrictive must list concrete alternatives you considered.
- Perceived coercion can be high in voluntary patients — process matters.[11]
- Document who/what/when/why for criteria and the review date.
- Seclusion/restraint: last resort; know harms evidence.[20]
- Many regain capacity — re-consent and step down.[22]
- Family demand ≠ statutory criteria.
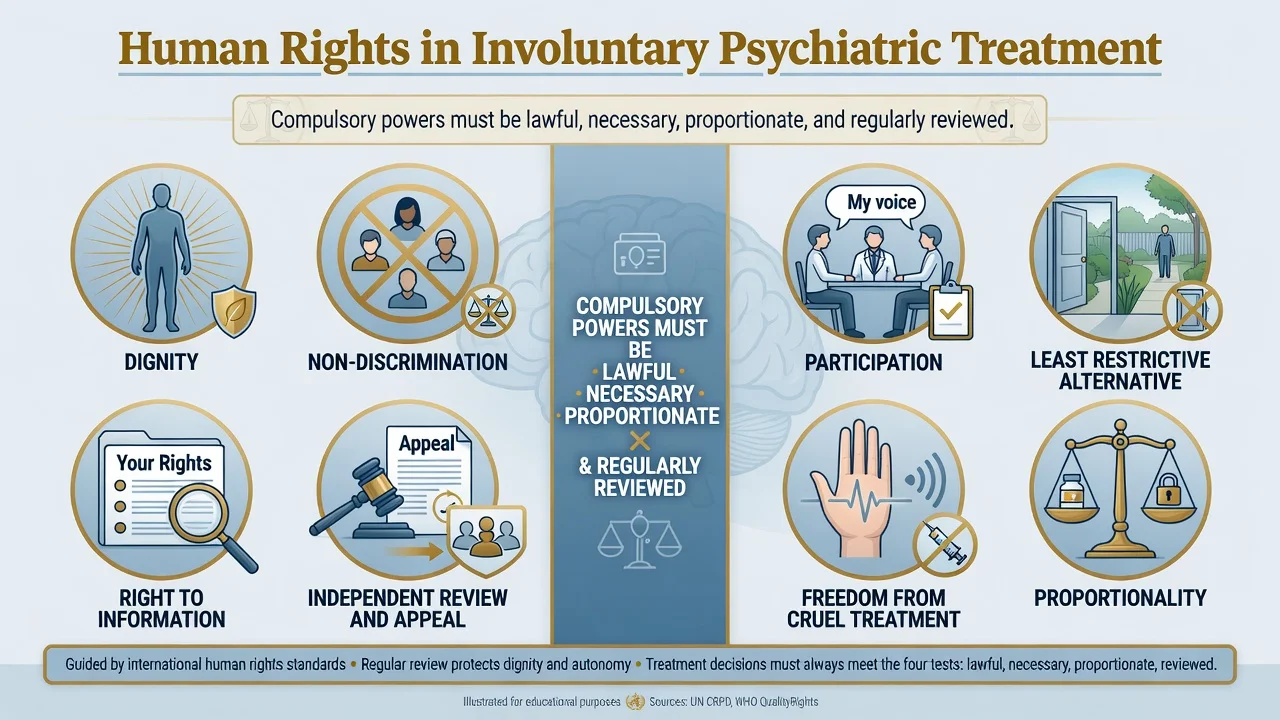
- Human rights frame: lawful, necessary, proportionate, regularly reviewed.
Self-test: CTO viva opener
Q. A consultant asks: "Why not put everyone with relapsing schizophrenia on a CTO at discharge?"
A. Because compulsion requires individual statutory criteria and least restrictive justification; RCTs (OCTET) and Cochrane-level reviews do not support broad superiority for reducing readmission; high-volume use may dilute benefit; CTOs without intensive services are empty force; rights and stigma costs are real. Select for revolving-door cases where community compulsion is safer than repeated detention and pair with genuine care.[1][2][4][5]
References
- [1]Burns T, Rugkåsa J, Molodynski A, et al. Community treatment orders for patients with psychosis (OCTET): a randomised controlled trial Lancet, 2013.PMID 23537605
- [2]Kisely SR, Campbell LA, O'Reilly R Compulsory community and involuntary outpatient treatment for people with severe mental disorders Cochrane Database Syst Rev, 2017.PMID 28303578
- [3]Maughan D, Molodynski A, Rugkåsa J, et al. A systematic review of the effect of community treatment orders on service use Soc Psychiatry Psychiatr Epidemiol, 2014.PMID 24136002
- [4]Rugkåsa J Effectiveness of Community Treatment Orders: The International Evidence Can J Psychiatry, 2016.PMID 27582449
- [5]Kisely S, McMahon L, Siskind D Benefits following community treatment orders have an inverse relationship with rates of use: meta-analysis and meta-regression BJPsych Open, 2023.PMID 37056174
- [6]Swartz MS, Swanson JW, Wagner HR, et al. Can involuntary outpatient commitment reduce hospital recidivism?: Findings from a randomized trial with severely mentally ill individuals Am J Psychiatry, 1999.PMID 10588412
- [7]Kallert TW, Glöckner M, Schützwohl M Involuntary vs. voluntary hospital admission. A systematic literature review on outcome diversity Eur Arch Psychiatry Clin Neurosci, 2008.PMID 18080170
- [8]Kallert TW, Katsakou C, Adamowski T, et al. Coerced hospital admission and symptom change--a prospective observational multi-centre study PLoS One, 2011.PMID 22140543
- [9]Kallert TW Coercion in psychiatry Curr Opin Psychiatry, 2008.PMID 18650692
- [10]Newton-Howes G, Mullen R Coercion in psychiatric care: systematic review of correlates and themes Psychiatr Serv, 2011.PMID 21532070
- [11]Lidz CW, Hoge SK, Gardner W, et al. Perceived coercion in mental hospital admission. Pressures and process Arch Gen Psychiatry, 1995.PMID 7492255
- [12]Katsakou C, Rose D, Amos T, et al. Psychiatric patients' views on why their involuntary hospitalisation was right or wrong: a qualitative study Soc Psychiatry Psychiatr Epidemiol, 2012.PMID 21863281
- [13]Zinkler M, Priebe S Detention of the mentally ill in Europe--a review Acta Psychiatr Scand, 2002.PMID 12100342
- [14]Dressing H, Salize HJ Compulsory admission of mentally ill patients in European Union Member States Soc Psychiatry Psychiatr Epidemiol, 2004.PMID 15669660
- [15]Raymont V, Bingley W, Buchanan A, et al. Prevalence of mental incapacity in medical inpatients and associated risk factors: cross-sectional study Lancet, 2004.PMID 15488217
- [16]Cairns R, Maddock C, Buchanan A, et al. Prevalence and predictors of mental incapacity in psychiatric in-patients Br J Psychiatry, 2005.PMID 16199799
- [17]Okai D, Owen G, McGuire H, et al. Mental capacity in psychiatric patients: Systematic review Br J Psychiatry, 2007.PMID 17906238
- [18]Owen GS, David AS, Richardson G, et al. Mental capacity, diagnosis and insight in psychiatric in-patients: a cross-sectional study Psychol Med, 2009.PMID 18940026
- [19]Grisso T, Appelbaum PS, Hill-Fotouhi C The MacCAT-T: a clinical tool to assess patients' capacities to make treatment decisions Psychiatr Serv, 1997.PMID 9355168
- [20]Chieze M, Hurst S, Kaiser S, et al. Effects of Seclusion and Restraint in Adult Psychiatry: A Systematic Review Front Psychiatry, 2019.PMID 31404294
- [21]Anfang SA, Appelbaum PS Civil commitment--the American experience Isr J Psychiatry Relat Sci, 2006.PMID 17294986
- [22]Owen GS, Ster IC, David AS, et al. Regaining mental capacity for treatment decisions following psychiatric admission: a clinico-ethical study Psychol Med, 2011.PMID 20346192
- [23]Simon J, Mayer S, Łaszewska A, et al. Cost and quality-of-life impacts of community treatment orders (CTOs) for patients with psychosis: economic evaluation of the OCTET trial Soc Psychiatry Psychiatr Epidemiol, 2021.PMID 32719905
- [24]Vergunst F, Rugkåsa J, Koshiaris C, et al. Community treatment orders and social outcomes for patients with psychosis: a 48-month follow-up study Soc Psychiatry Psychiatr Epidemiol, 2017.PMID 28900690