Psych · Forensic psychiatry — morbid jealousy and erotomania
Morbid jealousy and erotomania
Also known as Pathological jealousy · Delusional jealousy · Othello syndrome · Jealous type delusional disorder · Erotomania · de Clérambault syndrome · Erotomanic delusional disorder · Psychotic jealousy · Morbid jealousy forensic · Love delusion stalking
Exam-exhaustive fellowship reference on morbid (pathological/delusional) jealousy including Othello syndrome and erotomania (de Clérambault): DSM-5-TR/ICD-11 mapping, primary versus secondary causes, partner and third-party risk, stalking interface, assessment, pharmacotherapy and psychological management, organic and alcohol pathways, and forensic report principles. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Overview and definition
Fellowship exams pair these syndromes because they are monothematic delusional presentations with high interpersonal risk, classic forensic interfaces, and frequent secondary causes that general adult and C-L psychiatrists must recognise. Mullen's work frames jealousy as a human passion that becomes pathological when it dominates, resists contrary evidence, and organises behaviour around accusation, surveillance, and control.[1][2]
Operational vocabulary (exam precision):
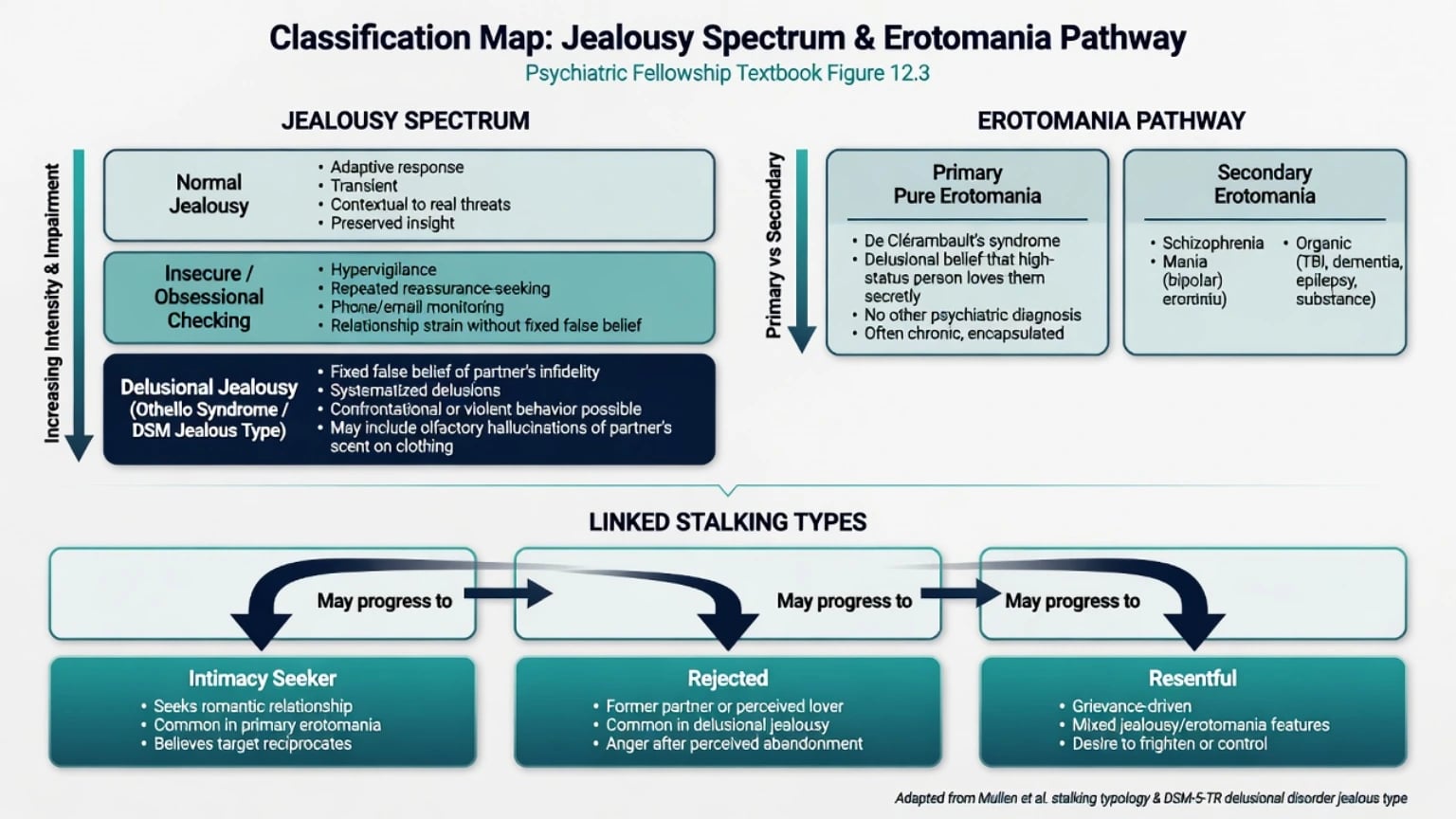
- Normal / reactive jealousy — proportionate, revisable concern about a real or plausible threat to a valued bond.
- Obsessional / insecure jealousy — repetitive checking and doubt with partial insight; may resemble OCD phenomenology.
- Morbid / pathological jealousy — umbrella clinical term for jealousy that is excessive, unjustified, or delusional and functionally destructive.[1]
- Delusional jealousy / Othello syndrome — fixed false belief of partner infidelity; may be primary delusional disorder or secondary.[4][15]
- Erotomania / de Clérambault syndrome — delusional belief of being loved, classically by a person of higher status who cannot openly declare love; primary or secondary.[7][8]
- Pathological extensions of love — Mullen and Pathé's clinical framing linking erotomania, morbid infatuation, and related pursuit behaviours to stalking risk.[3]
These labels organise clinical and forensic teaching. They are not automatic legal verdicts and are not synonyms for all intimate-partner violence.[1][3][16]
Classification — DSM/ICD and spectrum thinking
DSM-5-TR / ICD-11 anchors
When primary and meeting duration and exclusion rules, use delusional disorder jealous type (central theme that the spouse or lover is unfaithful) or erotomanic type (central theme that another person is in love with the individual). ICD-11 persistent delusional disorder language captures monothematic delusions without forcing a schizophrenia diagnosis when other criterion A domains are absent. Always state primary versus secondary: secondary presentations (alcohol-related, dementia-associated Othello, Parkinson agonist-related jealousy, schizophrenia or mania with love/jealousy content) change the treatment hierarchy.[4][7][15]
Stalking interface (typology, not a diagnosis)
Mullen and colleagues' stalker study and later risk work remain FRANZCP-relevant. Erotomanic and morbidly infatuated patients often sit in intimacy-seeking pathways; post-relationship rejected stalkers (with or without frank delusion) contribute substantially to violence risk in stalking research; resentful and predatory types complete the teaching set.[10][11][12] Zona's forensic comparison of erotomanic and obsessional subjects underlines that forensic samples are enriched and not population base rates.[9]
| Construct | Core belief | Typical risk focus | Classic trap |
|---|---|---|---|
| Delusional jealousy | Partner is unfaithful | Partner, alleged rival, children | Couples therapy into the delusion |
| Erotomania | Other loves me | Object of love, rivals, sometimes self | Treating as harmless romance |
| Rejected stalker | Relationship must resume / grievance | Ex-partner | Assuming psychosis is required for danger |
| Secondary Othello | Same as jealousy | As above plus medical fragility | Missing alcohol, dementia, agonists |
Epidemiology and risk
Community jealousy is common and dimensional — a New Zealand community study by Mullen and Martin documented frequent jealousy experiences without equating them to delusional disorder.[2] Delusional jealousy is uncommon overall but enriched among people with certain psychiatric disorders, alcohol-use problems, and forensic series; Soyka and Schmidt's prevalence work across psychiatric disorders is a standard citation for examiners who want numbers-with-humility rather than invented percentages.[4]
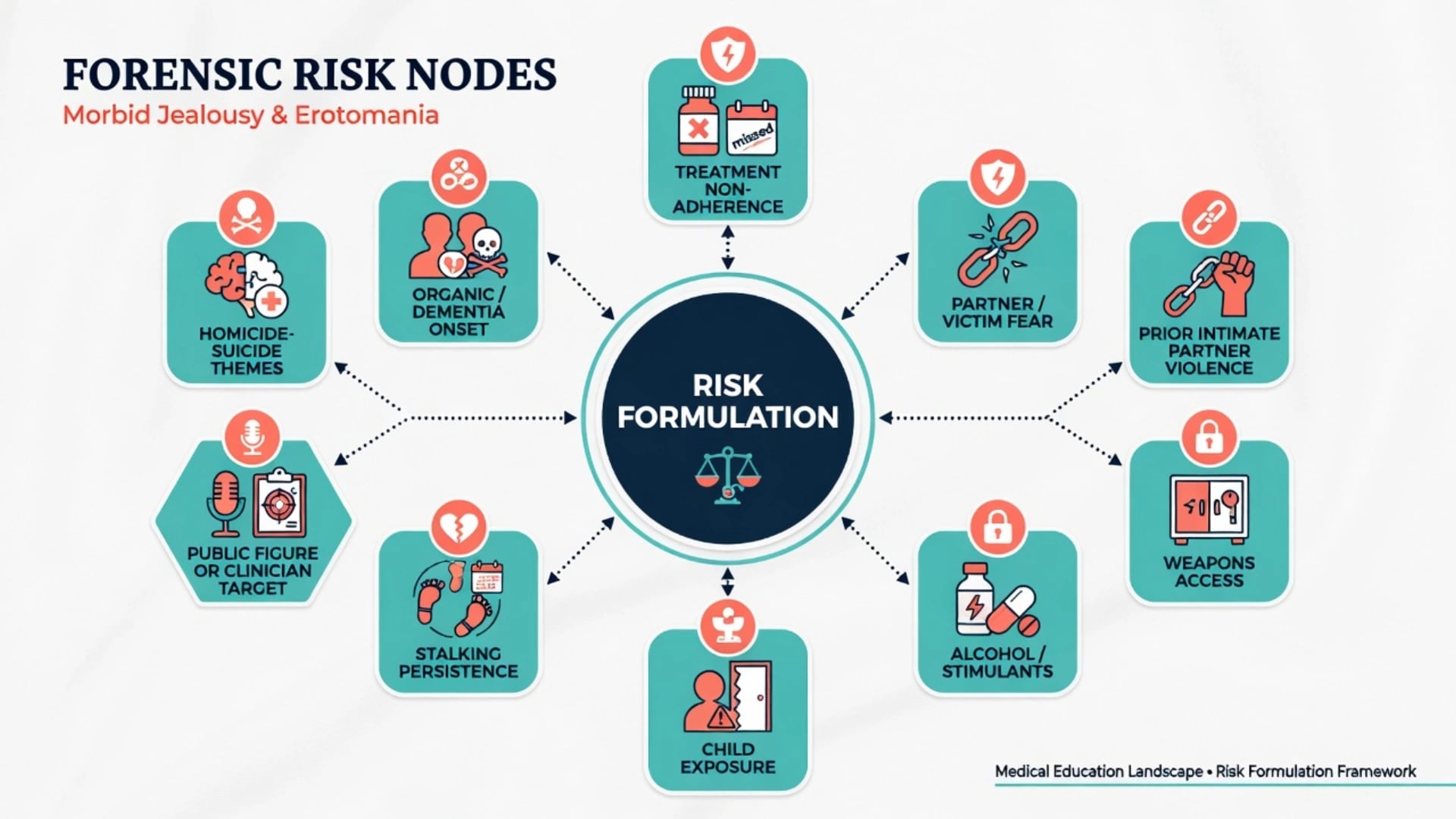
Violence and domestic homicide context. Delusional jealousy is associated with high rates of partner-directed aggression and stalking behaviours in clinical-forensic series; Silva and colleagues documented dangerousness and stalking behaviour among persons with delusional jealousy.[5][6] Domestic homicide population work shows mental illness at the offence in a minority of cases overall — jealousy themes matter clinically, but most domestic homicide is not reducible to a single delusional diagnosis.[16] In stalking research, violence associates with prior intimacy, threats, and related dynamic factors more than with a pure erotomanic label alone; still assess every case for approach, weapons, and grievance.[11][12]
Pathophysiology and mechanisms
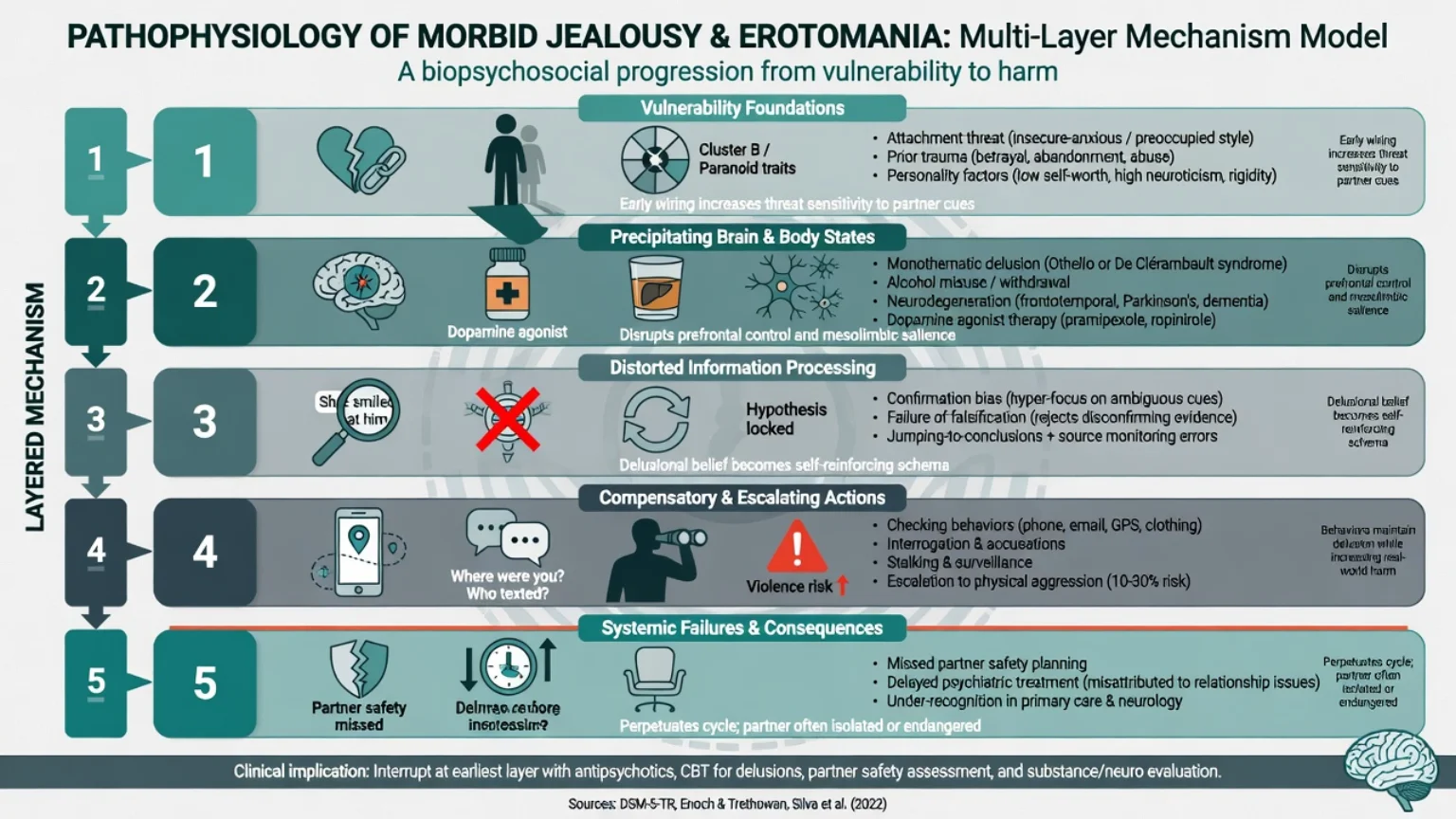
- Dispositional — attachment insecurity, prior betrayal trauma, paranoid personality traits, developmental adversity.
- Clinical state — monothematic delusion; alcohol intoxication/dependence; neurodegeneration; dopamine-agonist effects; mood or schizophrenia-spectrum illness.[4][15]
- Cognitive — confirmatory bias, inability to use disconfirming evidence, rumination, misreading of neutral cues as "proof".[1]
- Behavioural — checking rituals, interrogation, restriction of partner's autonomy, following, digital surveillance, assaults when challenged.[5][6]
- Relational/system — partner isolation, missed victim disclosure, delayed treatment, fragmented multi-agency response to stalking.[11]
Relational and system contexts shape how pathological jealousy unfolds and is disclosed, without shifting blame onto victims — partner isolation and delayed help-seeking are classic amplifiers of harm.[1][5] Erotomania's conceptual history (Segal; later Kennedy clinical course work) emphasises primary pure forms versus secondary symptomatic erotomania with different prognoses.[7][8]
Clinical presentation
Morbid and delusional jealousy
History from the partner often outranks the patient's narrative: repeated accusations, midnight interrogations, demands to "confess", inspection of phones and clothing, odometer checks, social media surveillance, forbidding contact with friends, and violence if the partner asserts independence. The patient may present self as the injured party. Discriminators of delusional quality include impossibility or extreme fixity of the infidelity belief, organised delusional work-up that never falsifies the hypothesis, and lack of insight.[1][5]
Erotomania
The patient describes secret signals, telepathic messages, or media references proving that a celebrity, clinician, teacher, or stranger loves them. External obstacles or a "test" explain the absence of open reciprocation. Behaviour ranges from letters and gifts to loitering, workplace approaches, litigation, and confrontation of perceived rivals. Clinical course series show chronicity is common and treatment response variable; secondary forms track the parent illness.[8][9]
MSE and risk language (viva-ready)
Document: affect (jealous rage, elation, despair), thought content (exact delusional wording), insight/judgment, substance state, suicidal ideation (including extended suicide themes), homicidal ideation toward partner/rival/object of love, and plans/means. Always ask about children as witnesses or secondary targets.[5][11]
Differential diagnosis
- Fixed infidelity belief
- Poor insight
- Checking that never settles
- Partner risk primary
- Intrusions + doubt
- Some insight possible
- Ego-dystonic elements
- CBT/ERP-informed options
- Being loved delusion
- Higher-status object classic
- Approach behaviours
- Clinician target risk
- Control without frank delusion
- Instrumental patterns
- Safety still first
- Do not force psychosis label
Also separate schizophrenia/schizoaffective multi-domain psychosis, manic erotomanic content, substance-induced states, dementia-related Othello, Parkinson agonist-related jealousy, and malingered delusion after arrest (late hypothesis after multi-source inconsistency).[4][7][15]
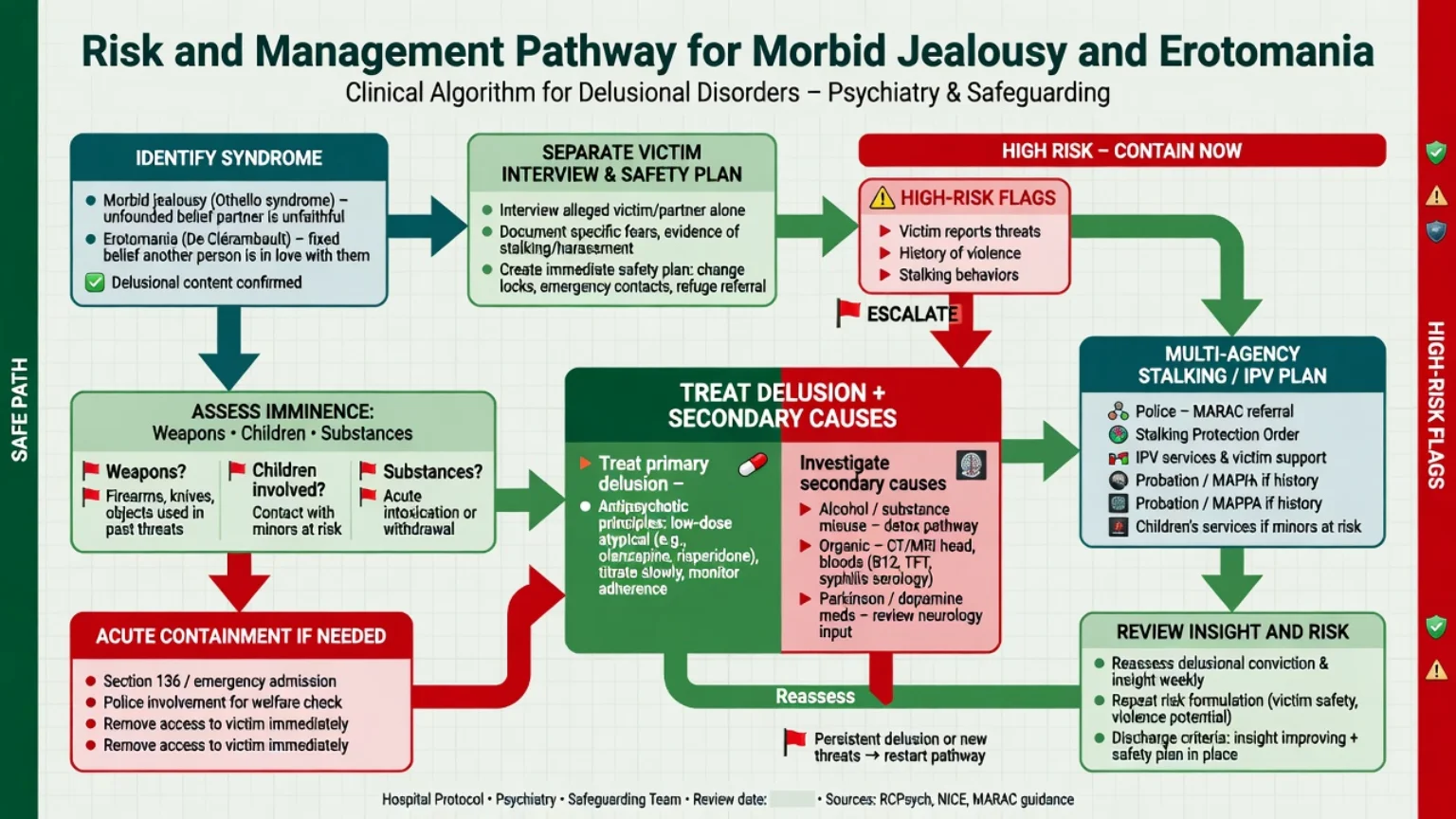
Assessment
Bedside structure
- Clarify the belief — jealousy versus erotomania versus mixed content; quote the patient.
- Separate interviews — patient and partner/alleged object; protect the partner from retaliatory questioning.
- Behaviour inventory — checking, stalking acts, digital abuse, property damage, sexual coercion, assaults.
- Risk — prior IPV, weapons, intoxication, child protection thresholds, homicide-suicide talk, breach of orders.
- Secondary causes — alcohol, stimulants, cognitive decline, Parkinson medications, other medical red flags.[4][11][15]
- Legal frame — capacity and compulsory treatment principles as jurisdiction-specific; third-party risk duties as principles only — do not invent statute section numbers.
- If court-commissioned — multi-source reconstruction of mental state at any index offence; diagnosis is not a defence.
Investigations
Baseline metabolic panel and ECG when starting antipsychotics; urine drug screen and alcohol history; cognitive screening and neuroimaging when late-onset, focal signs, or dementia suspected; review dopamine agonists with neurology in Parkinson disease; pregnancy test when relevant.[13][14][15]
Acute management (safety first)
- Imminent assault risk: emergency services, secure environment, consider inpatient care under lawful frameworks.
- Acute agitation: de-escalation first; rapid tranquillisation principles as for other acute behavioural disturbance if needed (agent selection, route, monitoring per local acute protocol — not a unique "jealousy cocktail").
- Iatrogenic Othello: urgent neurology liaison to reduce or change dopamine agonists when clinically appropriate.[15]
- Alcohol withdrawal: treat as medical priority; delusion may partially shift with abstinence but do not assume automatic resolution.[4]
- Clinician-directed erotomania: dual clinician review, clear written boundaries, security notification pathways, avoid mixed messages.[3][11]
Definitive management
Pharmacotherapy for primary delusional disorder
Evidence is limited relative to schizophrenia trials; practice is informed by delusional-disorder treatment reviews and historical case series. Antipsychotics are first-line for primary jealous or erotomanic delusional disorder. Historical literature includes successful pimozide case series in pure erotomania; modern practice usually prefers better-tolerated second-generation agents with metabolic and ECG monitoring as indicated.[13][14]
Illustrative adult oral options (individualise; start low in older/organic patients):
- Risperidone oral typically 1–2 mg daily initially, titrate toward approximately 2–6 mg daily in divided or once-daily dosing as tolerated; monitor EPS, prolactin, weight, glucose/lipids; ECG if cardiac risk.[13][14]
- Olanzapine oral typically 5 mg at night initially, common effective range around 5–20 mg daily; monitor weight, glucose, lipids, sedation.[13][14]
- Aripiprazole oral typically 5–10 mg daily initially, often 10–15 mg daily; monitor akathisia, impulse-control behavioural changes (relevant if Parkinson comorbidity).[13][14]
- Historical pimozide appears in classic pure-erotomania reports; if ever considered, specialist-level ECG/QT monitoring and interaction review are mandatory — many services avoid it as first-line given safer alternatives.[14]
Adherence is often poor because insight is limited; long-acting injectables may be considered after oral tolerability when risk and non-adherence are high — same monitoring principles as schizophrenia care.[13]
Psychological and social interventions
- Do not collude with the delusion; gently challenge only when rapport and safety allow.
- Behavioural and CBT-informed approaches may help non-delusional or residual obsessional jealousy (checking rituals, intolerance of uncertainty) when insight is partial and safety allows; they do not replace victim protection when delusion and violence risk are active.[1]
- CBT techniques adapted for delusions (engagement, peripheral questioning, behavioural experiments when safe) may help residual conviction; evidence remains modest for pure delusional disorder.[13]
- Alcohol treatment, housing stability, and reduction of unstructured contact with the victim are often more risk-reducing than medication alone.[4][11]
- Victim advocacy, protection-order pathways, and multi-agency stalking management follow local law — name principles, not invented sections.[11]
Regional deltas
ANZ (RANZCP-facing): integrate general adult care with forensic liaison when IPV/stalking risk is high; Indigenous and rural access barriers affect disclosure and protection planning. UK: NICE psychosis and domestic-abuse interfaces; multi-agency public protection principles for high-risk stalking. US (ABPN): Tarasoff-type third-party risk duties are jurisdiction-specific; document risk reasoning without inventing a universal statute number. Everywhere: victim safety and non-collusion are constant.[5][11]
Subtypes and high-yield scenarios
- Middle-aged man, alcohol dependence, delusional jealousy, partner facial injuries — treat alcohol + delusion + safety.[4][5]
- Alzheimer disease with new Othello accusations against spouse-carer — organic pathway, carer support, cautious pharmacology.[15]
- Parkinson disease on dopamine agonist with new jealous delusion — medication review with neurology.[15]
- Primary erotomania toward a treating psychiatrist — boundary and security plan.[3][8]
- Secondary erotomania in schizophrenia — treat parent psychosis; risk still real.[7][8]
- Rejected stalker after break-up without frank delusion — high violence yield in stalking data; do not wait for psychosis to act on safety.[10][12]
- Jealousy themes in domestic homicide or homicide-suicide review teaching — mental illness minority overall; still screen for delusion and depression.[16]
Complications and pitfalls
- Missing partner fear or child exposure.
- Debating "proof of infidelity" as if it were marital counselling.
- Ignoring alcohol and organic disease.
- Assuming erotomania is benign.
- Equating either diagnosis with insanity/mental-impairment after an assault.
- Unlawful confidentiality breach versus paralysis when serious third-party risk is clear — use lawful local pathways.
- Inventing Mental Health Act or duty-to-warn section numbers in exams.[5][11][16]
Prognosis and disposition
Primary delusional disorders are often chronic; partial behavioural control and risk reduction are realistic goals even when conviction softens incompletely.[8][13] Alcohol-linked cases may improve with sustained abstinence plus treatment of residual delusion.[4] Organic Othello tracks the neurology. Disposition ladder: community care with victim safety plan → voluntary or compulsory inpatient care when risk uncontainable → forensic pathways after serious offending. Stalking persistence and violence risk reviews guide monitoring intensity over time.[11][12]
Special populations
- Older adults / dementia: Othello syndrome is a recognised neuropsychiatric association; carer safety is central.[15]
- Parkinson / dopamine agonists: iatrogenic pathway; do not start by adding high-dose antipsychotics without medication review.[15]
- Women and same-sex relationships: do not teach male-only stereotypes; assess all dyads.[16]
- Clinician and public-figure targets: Pathé/Mullen clinical stalking lessons apply.[3][10]
- CALD / Indigenous: interpreters, family structure, and shame barriers; safety planning must be culturally safe without minimising risk.[11]
Evidence and guidelines
Core scientific spine: Mullen on jealousy pathology and community prevalence; Mullen and Pathé on pathological extensions of love; Soyka on prevalence of delusional jealousy; Silva on dangerousness and stalking in delusional jealousy; Segal and Kennedy on erotomania concept and course; Zona forensic comparison; Mullen stalker study and stalking risk management papers; McEwan on violence in stalking; Manschreck and González-Rodríguez on delusional-disorder treatment history; Cipriani on Othello and dementia; Oram on mental illness in domestic homicide as population context.[1][3][4][5][8][10][13][16]
There is no single RANZCP "morbid jealousy guideline"; practice is synthesised from psychosis care standards, domestic-abuse/IPV guidance, and forensic risk principles informed by the stalking and delusional-disorder evidence base above.[11][13][16]
Exam pearls
JEALOUS-E risk scan
Mastery means holding clinical monothematic delusion, victim safety, secondary medical causes, and legal-time-point humility in one formulation — the same discipline that separates fellowship answers from undergraduate overviews.[1][5][11][16]
References
- [1]Mullen PE Jealousy: the pathology of passion Br J Psychiatry, 1991.PMID 1801774
- [2]Mullen PE, Martin J Jealousy: a community study Br J Psychiatry, 1994.PMID 8137108
- [3]Mullen PE, Pathé M The pathological extensions of love Br J Psychiatry, 1994.PMID 7866676
- [4]Soyka M, Schmidt P Prevalence of delusional jealousy in psychiatric disorders J Forensic Sci, 2011.PMID 21265838
- [5]Silva AJ, Ferrari MM, Leong GB, et al. The dangerousness of persons with delusional jealousy J Am Acad Psychiatry Law, 1998.PMID 9894217
- [6]Silva JA, Derecho DV, Leong GB, et al. Stalking behavior in delusional jealousy J Forensic Sci, 2000.PMID 10641922
- [7]Segal JH Erotomania revisited: from Kraepelin to DSM-III-R Am J Psychiatry, 1989.PMID 2675641
- [8]Kennedy N, McDonough M, Kelly B, et al. Erotomania revisited: clinical course and treatment Compr Psychiatry, 2002.PMID 11788912
- [9]Zona MA, Sharma KK, Lane J A comparative study of erotomanic and obsessional subjects in a forensic sample J Forensic Sci, 1993.PMID 8355005
- [10]Mullen PE, Pathé M, Purcell R, et al. Study of stalkers Am J Psychiatry, 1999.PMID 10450267
- [11]Mullen PE, Mackenzie R, Ogloff JR, et al. Assessing and managing the risks in the stalking situation J Am Acad Psychiatry Law, 2006.PMID 17185471
- [12]McEwan TE, Mullen PE, MacKenzie RD, et al. Violence in stalking situations Psychol Med, 2009.PMID 19215627
- [13]Manschreck TC, Khan NL Recent advances in the treatment of delusional disorder Can J Psychiatry, 2006.PMID 16989110
- [14]González-Rodríguez A, Monreal JA, Natividad M, et al. Seventy Years of Treating Delusional Disorder with Antipsychotics: A Historical Perspective Biomedicines, 2022.PMID 36552037
- [15]Cipriani G, Vedovello M, Nuti A, et al. Dangerous passion: Othello syndrome and dementia Psychiatry Clin Neurosci, 2012.PMID 23066764
- [16]Oram S, Flynn SM, Shaw J, et al. Mental illness and domestic homicide: a population-based descriptive study Psychiatr Serv, 2013.PMID 23820784