Psych · Forensic psychiatry — fabricated or induced illness
Fabricated or induced illness (Munchausen by proxy)
Also known as Munchausen syndrome by proxy · Munchausen by proxy · Fabricated or induced illness · FII · Factitious disorder imposed on another · FDIA · Medical child abuse · Caregiver-fabricated illness · Perplexing presentations · Illness induction syndrome
Exam-exhaustive fellowship reference on fabricated or induced illness (FII), medical child abuse, caregiver-fabricated illness, and factitious disorder imposed on another (FDIA): terminology map from Meadow MSBP through RCPCH and AAP frameworks, epidemiology, perpetrator psychopathology, recognition red flags, multi-agency safeguarding, covert surveillance ethics principles, differential diagnosis, forensic assessment, child and caregiver management, and court interfaces without invented statute numbers. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
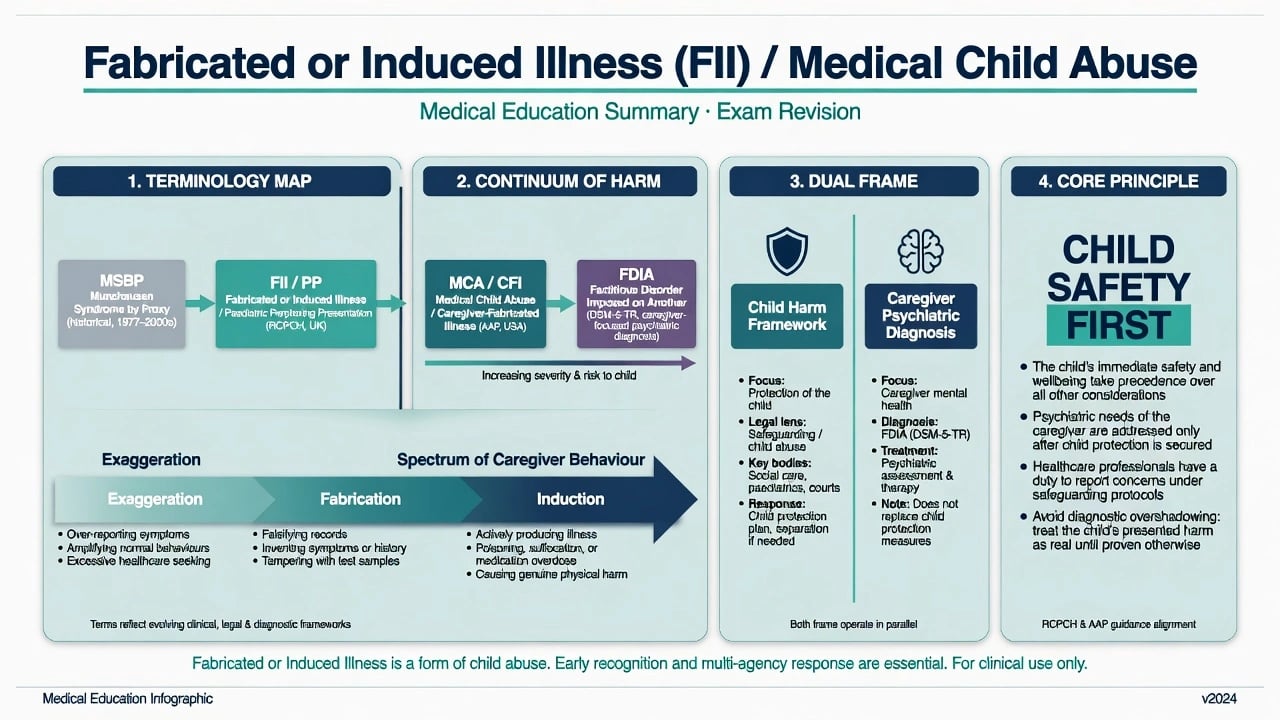
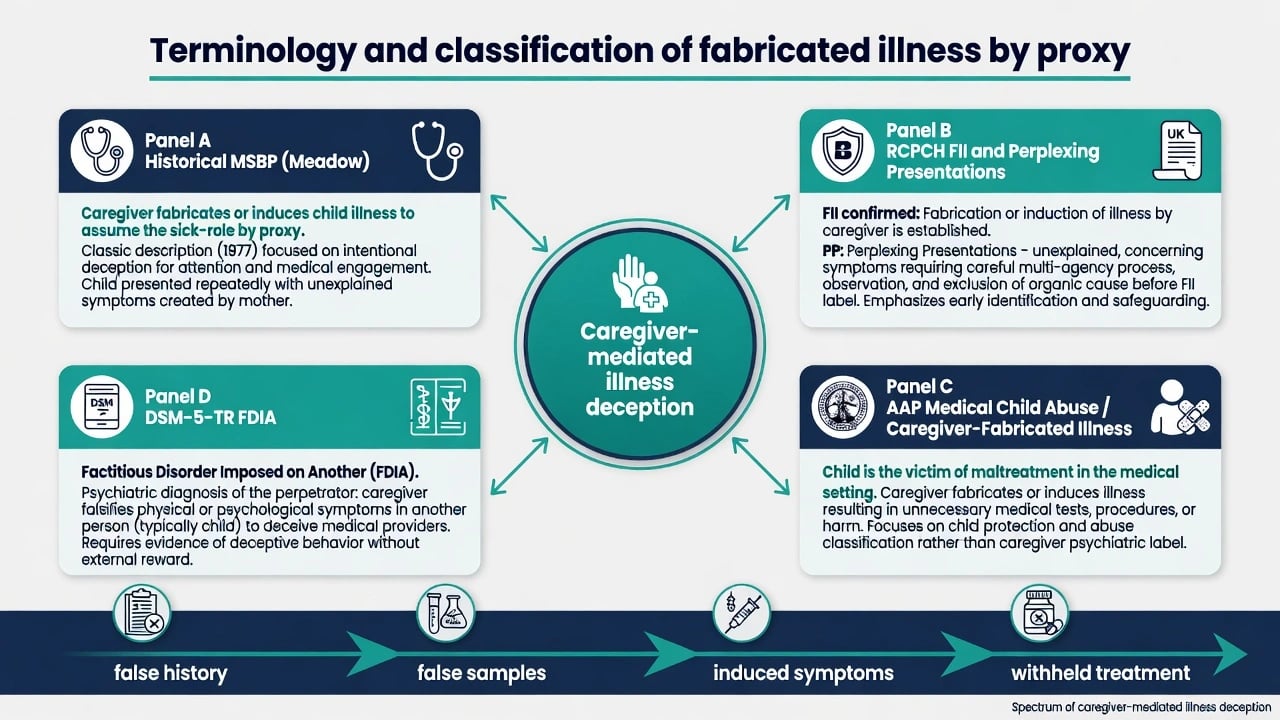
Meadow's 1977 Lancet description named Munchausen syndrome by proxy for caregivers who created or invented illness in a child, situating the problem in the hinterland of child abuse rather than as a curiosity of adult factitious behaviour alone.[1] Subsequent definitional work emphasised describing illness falsification behaviours and harm to the child, not a single glamorous syndrome label.[13][20]
Fellowship candidates must hold two simultaneous frames that keep child protection and caregiver psychiatry separate.[4][11][12][16]
- Child protection / paediatric frame — the child is a victim of maltreatment occurring through the medical system (unnecessary tests, procedures, induction of pathology).[11][12]
- Psychiatric frame — the caregiver may meet criteria for factitious disorder imposed on another when illness is falsified in another person and deception is intentional, without the external incentives that define malingering.[16]
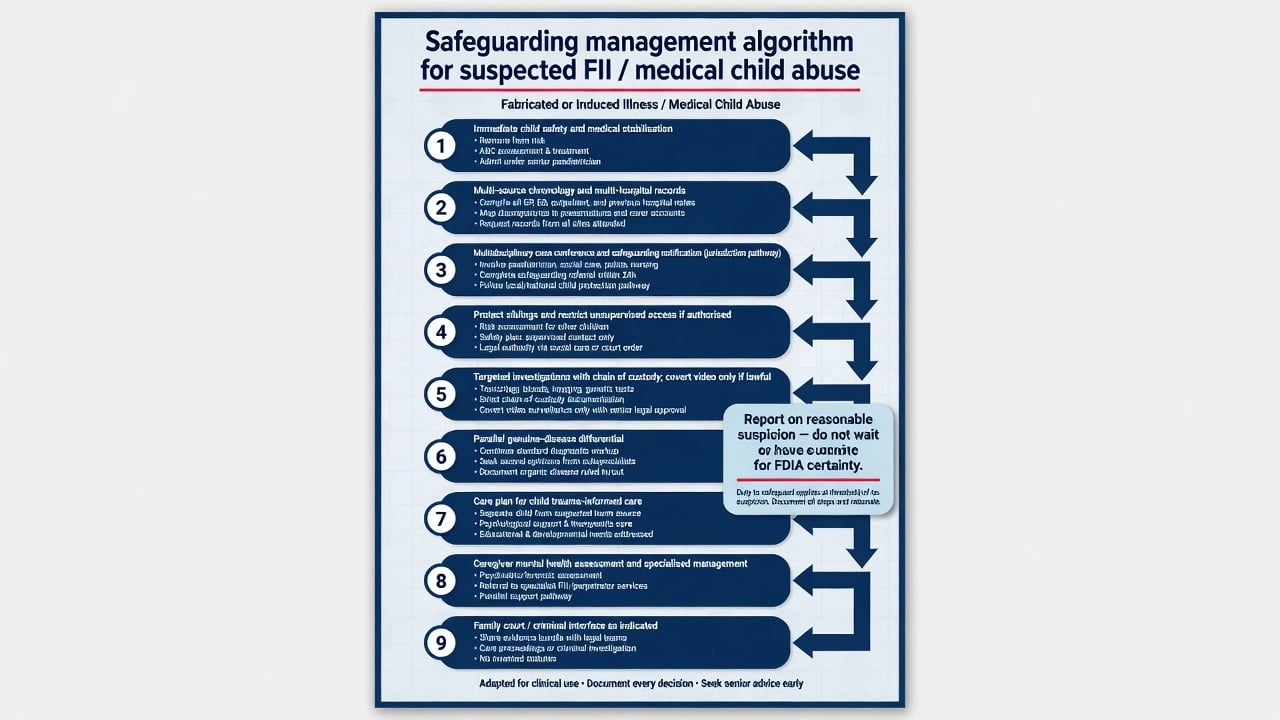
A diagnosis of FDIA in the caregiver is not required before safeguarding action. Report and protect on reasonable suspicion of maltreatment; psychiatric labels follow multi-source evaluation.[4][18]
Classification and terminology
| Framework | Core idea | Exam use |
|---|---|---|
| Historical MSBP (Meadow) | Caregiver fabricates/induces child illness; sick-role by proxy | Legacy exam language; know limits and controversy |
| RCPCH FII / PP | Confirmed fabrication or induction (FII); perplexing presentations needing careful process (PP) | UK/ANZ teaching; process before premature FII label |
| AAP MCA / CFI | Child is victim of maltreatment in a medical setting | US ABPN-facing; child-centred wording |
| DSM-5-TR FDIA | Psychiatric diagnosis of perpetrator who falsifies illness in another | Caregiver formulation; not a child diagnosis |
| Continuum | Exaggeration → fabrication → induction | Severity and lethality climb with induction |
Continuum of caregiver behaviour
Caregiver behaviour is usefully mapped on a severity continuum rather than as a single binary label: exaggeration (amplifying real symptoms or excessive healthcare seeking without frank invention), fabrication (false history, false records, contaminated samples, invented seizures or allergies), and induction (actively producing illness by poisoning, suffocation, interference with lines or devices, or withholding essential treatment).[2][3][4]
Induction carries the highest acute lethality (especially non-accidental poisoning and suffocation) and must drive urgent protection even when psychiatric diagnosis remains open.[2][3][5]
Epidemiology and risk
True population incidence is low and under-ascertained. British Isles surveillance of MSBP, non-accidental poisoning, and non-accidental suffocation produced small annual case counts with high severity among confirmed cases — use as order-of-magnitude teaching that rarity does not mean triviality.[5]
Literature syntheses (Rosenberg; Sheridan) catalogued methods of harm, victim ages (often young children), predominance of female caregiver perpetrators in published series, and non-trivial mortality — exact percentages vary by inclusion criteria, so examiners reward pattern knowledge over memorised pseudo-precision.[2][3]
Yates and Bass systematically reviewed 796 perpetrators of medical child abuse: predominantly mothers/female caregivers, with elevated rates of healthcare-related occupation or training in many series, substantial psychiatric comorbidity, and heterogeneous methods spanning fabrication and induction.[10][19]
Risk concentrators (exam list)
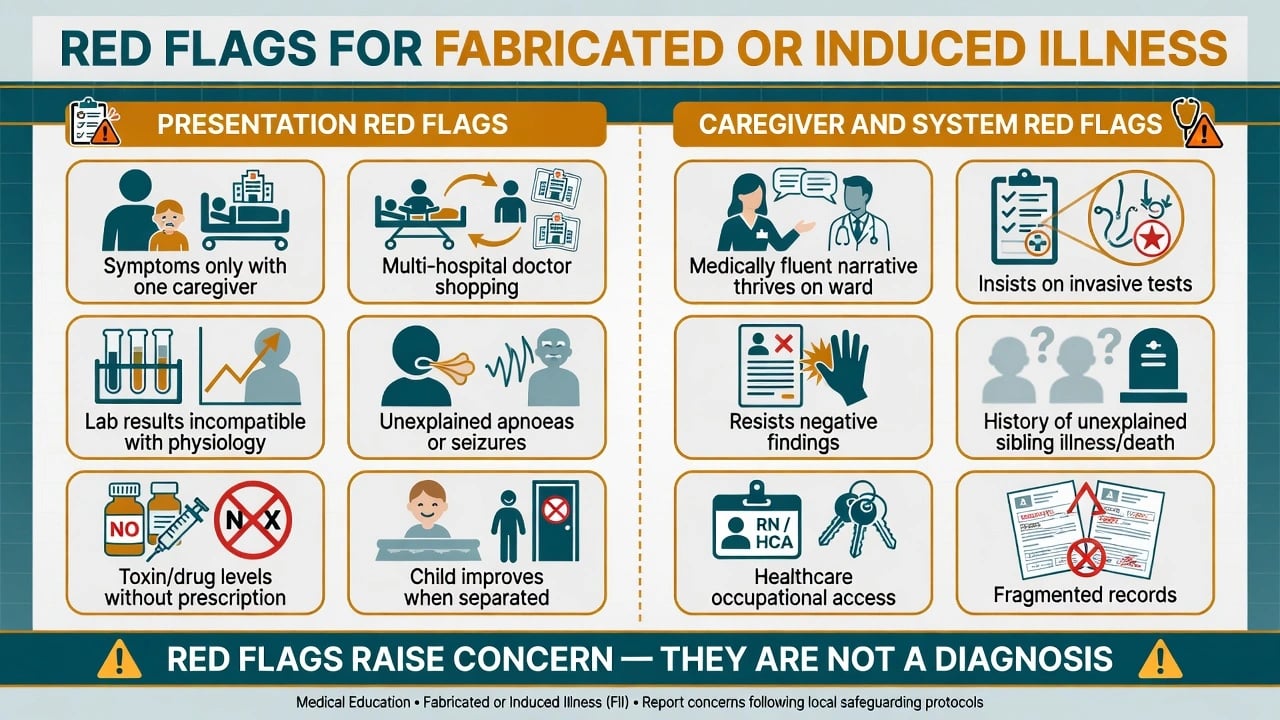
- Young age of the child (infants and toddlers — highest induction lethality).
- Multi-specialty chronic "diagnostic odyssey" without coherent organic synthesis.
- Symptoms or events only when one caregiver has access.
- Sibling history of unexplained illness or death.
- Caregiver thrives in the medical environment; doctor-shops; demands invasive tests.
- Healthcare literacy or occupational access to means (medicines, devices).[3][4][10]
Pathophysiology and mechanisms
Caregiver mechanisms
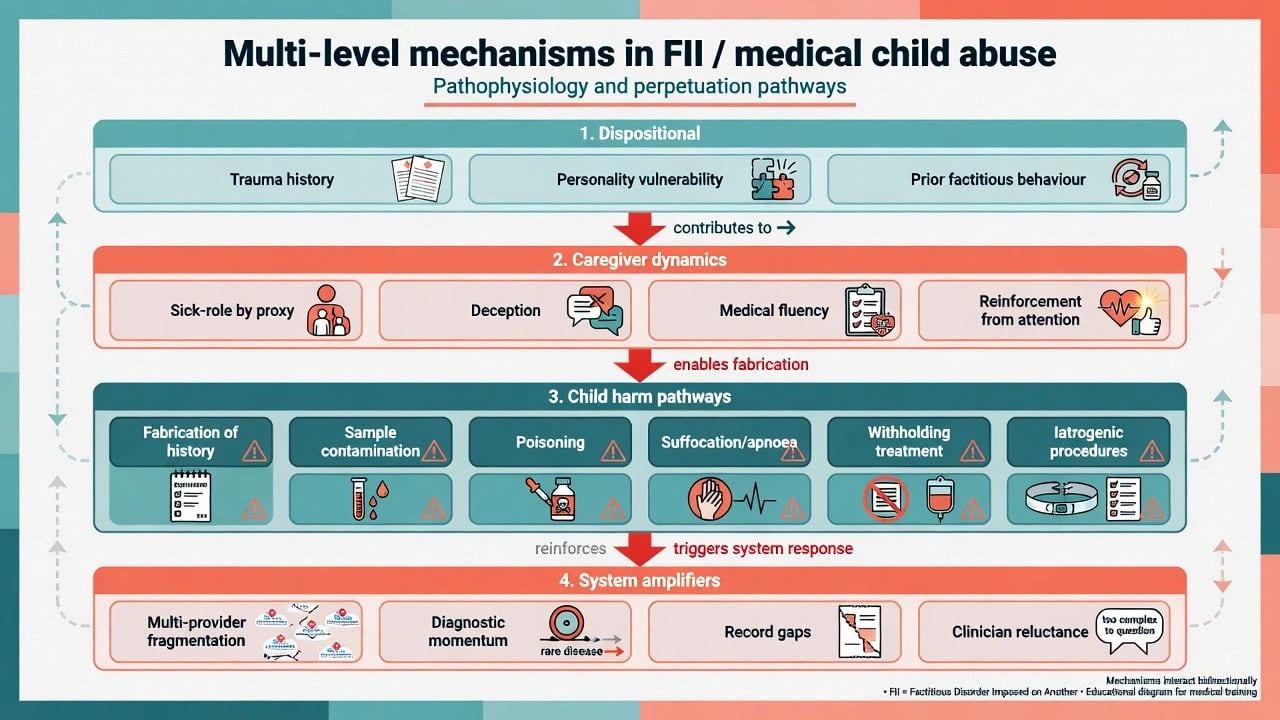
Perpetrator series show high rates of personality disorder, histories of factitious or somatising behaviour in the caregiver themselves, depression/anxiety, and deceptive illness behaviour — not a uniform "attention-seeking mother" caricature.[7][9][10] Bass and Jones' case series of FII perpetrators documented substantial Axis I and personality psychopathology and prior deceptive medical behaviour, supporting structured psychiatric assessment once child safety is secured.[9]
Psychological drivers are heterogeneous and should be formulated case by case rather than reduced to a single slogan.[7][9][14][16]
- Need for the sick-role by proxy and medical attention.
- Trauma and attachment pathology shaping caregiving identity.
- Factitious dynamics continuous with self-directed factitious disorder.
- Occasional external incentives (benefits, custody, immigration) that shift the formulation toward malingering by proxy rather than pure FDIA — both can harm the child and both need safeguarding.[14][16]
System mechanisms
Fragmented multi-provider care, incomplete electronic records, diagnostic momentum ("rare disease" framing), and clinician reluctance to suspect caregivers create a web of deceit in which iatrogenic harm accumulates.[2][4] The medical system can become an unwitting instrument of abuse through repeated investigations and procedures.[11][12]
Child harm pathways
Direct induction (toxin, airway obstruction), fabrication leading to unnecessary surgery or immunosuppression, developmental disruption, and later collusion or own illness falsification in older children are all described pathways.[3][8]
Clinical presentation
Classic stems
- Recurrent unexplained apnoeas or "seizures" only in one caregiver's presence; normal investigations when observed by staff.
- Blood in samples that does not match clinical bleeding; glucose/insulin patterns of exogenous insulin; unexplained drug levels.
- Chronic multi-system illness with normal objective findings and escalating invasive requests.
- Fabricated food allergy, immunodeficiency, or epilepsy careers across hospitals.
- Child improves markedly during periods of supervised separation.[2][3][4]
Caregiver interpersonal pattern (soft signs)
Medically fluent narrative; unusually calm or conversely crisis-amplifying during events; strong alliances with some staff and hostility to sceptics; thrives on ward social role; resists discharge or negative results. Soft signs support concern; they never alone prove FII.[4][14]
Differential diagnosis
- Keep open until multi-specialty synthesis
- False accusation risk is real
- Parallel workup with safeguarding
- Unexplained concerning symptoms
- No confirmed fabrication yet
- RCPCH process-oriented approach
- No intentional deception
- Fear-driven help-seeking
- Supportive education, not criminalisation
- External incentive primary
- Still child harm
- Different psychiatric label, same protection
Also include paediatric somatic symptom / functional presentations with honest reporting, iatrogenic complexity, non-accidental injury and neglect without illness fabrication, adolescent self-directed factitious disorder, and cultural care practices misread without interpreters.[4][17][18]
Meadow's own later writing stressed boundaries of what is and is not MSBP — over-extension of the label damages families and the concept.[20] Contemporary Australian guidance similarly emphasises careful process and multi-agency caution.[18]
Assessment
Principles
- Protect the child first — safety plan and lawful reporting thresholds beat diagnostic elegance.[4][18]
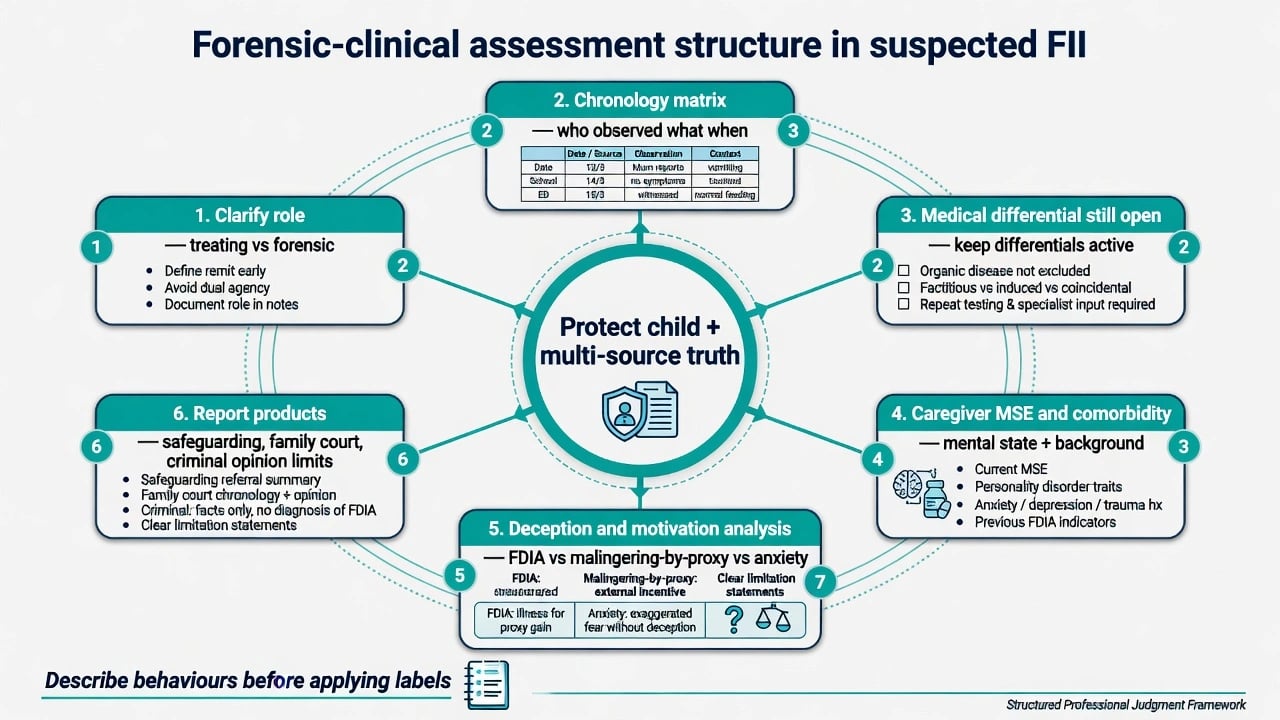
- Clarify your role — treating paediatric/psychiatry team versus independent forensic expert; avoid covert dual agency.[14]
- Multi-source chronology — every hospital, GP, pharmacy, school attendance, growth chart, sibling records.[14][16]
- Symptom–observer matrix — who saw what, when, alone with whom.
- Interview the child alone when developmentally appropriate; avoid coercive confession focus.
- Caregiver MSE without premature courtroom accusation in the ward corridor.
- Describe behaviours before applying MSBP/FII/FDIA labels.[13][14]
Forensic assessment of illness falsification draws on multi-source data, analysis of deception, differential motivation (FDIA vs malingering by proxy vs anxiety), and clear report products for child protection or court — not detective work that exceeds legal authority.[14][16]
Investigations
- Targeted toxicology, drug levels, and metabolic tests when induction is plausible — with chain of custody.
- Video-EEG or observed monitoring for alleged seizures/apnoeas.
- Pharmacy reconciliation and prescription forensics (principles).
- Covert video surveillance only under lawfully authorised multi-agency protocols with senior governance — never freelance by a junior clinician. Ethical and legal thresholds are high and jurisdiction-specific.[4][12]
- Separation observations when safely authorised may show improvement; supportive, not sole proof.[4]
- Continue appropriate organic workups in parallel — false dichotomies harm children with real disease.[17][18]
Acute management
Immediate priorities follow a child-safety and multi-agency sequence rather than a psychiatric label-first pathway.[4][11][18]
- Medical stabilisation of the child (airway, toxin, seizure, hypoglycaemia pathways as indicated).
- Stop ongoing induction opportunity — restrict unsupervised caregiver access if authorised under local safeguarding.
- Notify child-protection / multi-agency hub per local mandatory reporting principles (do not invent section numbers).
- Protect siblings and other dependents.
- Single senior voice for the team to reduce splitting and leakage of plan to the caregiver before safety is secured.
- Document contemporaneously.[4][6][11][18]
There is no specific psychotropic antidote for FII. Treat acute medical complications of induction using standard paediatric emergency protocols, and manage any concurrent caregiver mental illness with ordinary agent, dose, route, and monitoring standards for that condition rather than a special FII regimen.[4][15][16]
Definitive management
Child
- Paediatric leadership; reverse unnecessary treatments when safe.
- Trauma-informed psychological care; developmental catch-up.
- Carefully planned communication/disclosure as age-appropriate.
- Long-term monitoring for psychological sequelae after fabricated illness — follow-up series document ongoing emotional and behavioural difficulties in many victims even when physical recovery occurs.[8]
Caregiver
- Assess and treat co-morbid mental illness (depression, anxiety, PTSD, psychosis if present).
- Specialised psychological approaches to factitious dynamics are described; engagement is often poor and prognosis for cessation of deception is guarded, especially with entrenched personality pathology.[15][16]
- Do not offer false reassurance that "therapy will fix risk" without structural child-protection controls.
Multi-agency and legal interfaces
- Health, statutory child protection, police, education, and legal services share information under local lawful frameworks.
- Family court / care proceedings: psychiatry may opine on caregiver mental state, parenting capacity, risk of recurrence, and treatability — not the ultimate legal finding of abuse alone.[6][14]
- Criminal pathway when assault, poisoning, or homicide is alleged: fitness, mental state at material time, and disposal principles are separate products (see criminal forensic topics); do not invent offence-section numbers.[16]
Placement and further-abuse risk literature after confirmed MSBP/poisoning/suffocation cases shows that unsupervised return without major change in dynamics is high-risk; supervised or alternative care plans are often required.[6]
Subtypes and scenarios
| Scenario | High-yield points |
|---|---|
| History/record fabrication only | Still harmful via procedures; multi-hospital chronology key |
| Sample contamination | Chain of custody; lab liaison |
| Poisoning | Insulin, anticonvulsants, salt, sedatives, laxatives — toxicology emergency |
| Suffocation / induced apnoea | ALTE/BRUE differential; highest lethality concern |
| Withholding treatment | Deterioration of real illness used as induction |
| Disability / special-education fabrication | Educational and benefits interfaces (definitional literature) |
| Adult dependent FDIA | Elderly or disability-care victims — same dual-frame logic |
| Healthcare-professional caregiver | Access and fluency amplify risk — not a stereotype alone |
Complications and pitfalls
- Delayed recognition → cumulative iatrogenic harm.
- False positive FII accusation of anxious parents of complex/autistic children — dual risk of under- and over-call; process and multi-source evidence protect both child and family justice.[17][18]
- Premature confrontation without safety plan → flight, escalation, evidence destruction.
- Equating FDIA diagnosis with court proof standard.
- Covert video without lawful authority.
- Ignoring male or non-mother perpetrators.
- Single-clinician crusade without multi-agency governance.
- Inventing mandatory-reporting statute numbers in exams or reports.[4][12][14]
Prognosis and disposition
Physical recovery of the child is often good if induction stops early; psychological sequelae are common in follow-up series.[8] Further abuse risk remains substantial if the child returns to the same dynamics without structural change; placement decisions must be risk-led.[6] Perpetrator prognosis for ending deception is guarded when personality and factitious pathology dominate; better when a treatable major mental illness is the main driver and insight/engagement exist.[9][15]
Disposition products: child safety plan, sibling protection, graded or supervised contact only with explicit risk management, caregiver treatment pathway, and clear multi-agency review points.[6][16]
Special populations
- Infants/toddlers — highest lethality from induction.
- Children with disability/complex care — harder differential; higher opportunity for interference with devices/medicines.
- Adolescents — possible collusion or transition to self-directed factitious behaviour.[8]
- Healthcare-trained caregivers — series flag occupational over-representation; individualise, do not profile alone.[10]
- Cultural and Indigenous contexts — trauma-informed safeguarding without racist over-call or under-protection; use interpreters.
- Adults with disability / older adults as FDIA victims in care settings.[16][19]
Evidence and guidelines
- Landmark description: Meadow 1977.[1]
- Literature reviews: Rosenberg 1987; Sheridan 2003.[2][3]
- Epidemiology and outcomes: McClure 1996; Davis 1998; Bools victim follow-up and psychopathology.[5][6][7][8]
- Modern clinical reviews: Bass and Glaser 2014 Lancet FII; Yates and Bass 2017 perpetrators; Abdurrachid 2022 FDIA perpetrator review.[4][10][19]
- AAP: Stirling 2007 Beyond MSBP; Flaherty 2013 caregiver-fabricated illness clinical report.[11][12]
- Forensic/treatment: APSAC definitional position; Sanders and Bursch forensic assessment and psychological treatment; Bursch evaluation/management of FDIA.[13][14][15][16]
- Regional practice: RCPCH PP/FII guidance (reviewed Wear and Li 2022); Australian practitioner guide (Tully 2021).[17][18]
- NICE / RANZCP / APA: use child-maltreatment and safeguarding principles and local college child-protection position statements at system level — name principles, not fabricated section numbers.
Exam pearls
FII SAFE
References
- [1]Meadow R Munchausen syndrome by proxy. The hinterland of child abuse Lancet, 1977.PMID 69945
- [2]Rosenberg DA Web of deceit: a literature review of Munchausen syndrome by proxy Child Abuse Negl, 1987.PMID 3322516
- [3]Sheridan MS The deceit continues: an updated literature review of Munchausen Syndrome by Proxy Child Abuse Negl, 2003.PMID 12686328
- [4]Bass C, Glaser D Early recognition and management of fabricated or induced illness in children Lancet, 2014.PMID 24612863
- [5]McClure RJ, Davis PM, Meadow SR, et al. Epidemiology of Munchausen syndrome by proxy, non-accidental poisoning, and non-accidental suffocation Arch Dis Child, 1996.PMID 8813872
- [6]Davis P, McClure RJ, Rolfe K, et al. Procedures, placement, and risks of further abuse after Munchausen syndrome by proxy, non-accidental poisoning, and non-accidental suffocation Arch Dis Child, 1998.PMID 9613350
- [7]Bools C, Neale B, Meadow R Munchausen syndrome by proxy: a study of psychopathology Child Abuse Negl, 1994.PMID 8000908
- [8]Bools CN, Neale BA, Meadow SR Follow up of victims of fabricated illness (Munchausen syndrome by proxy) Arch Dis Child, 1993.PMID 8285772
- [9]Bass C, Jones D Psychopathology of perpetrators of fabricated or induced illness in children: case series Br J Psychiatry, 2011.PMID 21804147
- [10]Yates G, Bass C The perpetrators of medical child abuse (Munchausen Syndrome by Proxy) - A systematic review of 796 cases Child Abuse Negl, 2017.PMID 28750264
- [11]Flaherty EG, Macmillan HL, Committee on Child Abuse and Neglect Caregiver-fabricated illness in a child: a manifestation of child maltreatment Pediatrics, 2013.PMID 23979088
- [12]Stirling J, American Academy of Pediatrics Committee on Child Abuse and Neglect Beyond Munchausen syndrome by proxy: identification and treatment of child abuse in a medical setting Pediatrics, 2007.PMID 17473106
- [13]Ayoub CC, Alexander R, Beck D, et al. Position paper: definitional issues in Munchausen by proxy Child Maltreat, 2002.PMID 12020066
- [14]Sanders MJ, Bursch B Forensic assessment of illness falsification, Munchausen by proxy, and factitious disorder, NOS Child Maltreat, 2002.PMID 12020067
- [15]Sanders MJ, Bursch B Psychological Treatment of Factitious Disorder Imposed on Another/Munchausen by Proxy Abuse J Clin Psychol Med Settings, 2020.PMID 31089919
- [16]Bursch B, Emerson ND, Sanders MJ Evaluation and Management of Factitious Disorder Imposed on Another Psychiatr Clin North Am, 2021.PMID 31612305
- [17]Wear KR, Li S Guideline review: RCPCH perplexing presentations, fabricated or induced illness in children guidance 2021 Arch Dis Child Educ Pract Ed, 2022.PMID 34728544
- [18]Tully J, Hopkins O, Smith A, et al. Fabricated or induced illness in children: A guide for Australian health-care practitioners J Paediatr Child Health, 2021.PMID 34310788
- [19]Abdurrachid N, Gama Marques J Munchausen syndrome by proxy (MSBP): a review regarding perpetrators of factitious disorder imposed on another (FDIA) CNS Spectr, 2022.PMID 32772954
- [20]Meadow R What is, and what is not, 'Munchausen syndrome by proxy'? Arch Dis Child, 1995.PMID 7618944