Psych · Forensic psychiatry — prison mental health
Prison mental health
Also known as Custodial mental health · Jail psychiatry · Correctional mental health · Prison psychiatry · In-reach mental health · Reception screening prison · Prison suicide · Segregation mental health · Equivalence of care prison
Exam-exhaustive fellowship reference on prison mental health — prevalence of SMI and SUD, reception screening, suicide and self-harm, dual diagnosis, segregation harms, equivalence of care, transfer pathways, and release transition risk. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Prison (custodial) mental health is the detection, assessment, treatment, and care coordination of mental illness, substance use, self-harm, and vulnerability inside prisons, jails, and remand centres. It is clinical healthcare under security constraints — not a sub-branch of punishment.[3][18]
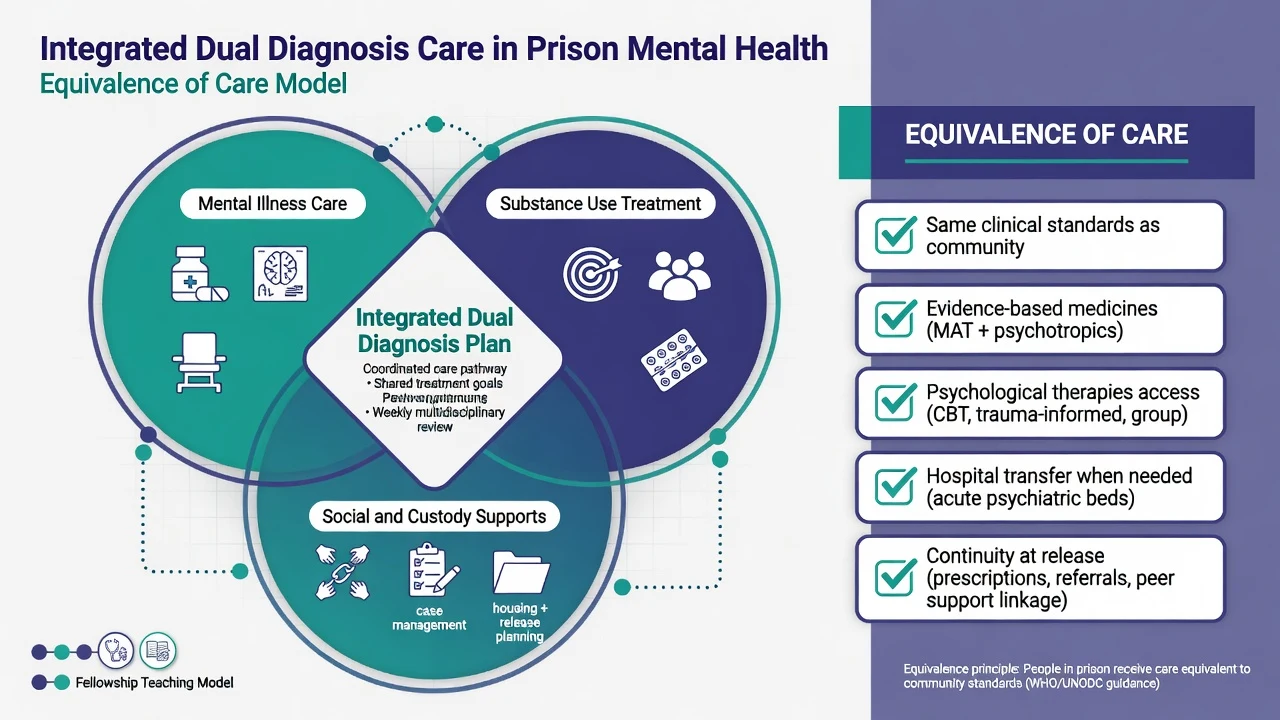
Equivalence of care is the governing maxim for exams and ethics: people in custody retain the right to mental healthcare of a standard comparable to that available in the community, adapted to the secure setting. Equivalence does not mean identical buildings; it means evidence-based assessment, medicines, psychological therapies, and timely transfer when prison healthcare cannot meet need.[3][18]
Operational map (custody vocabulary):
- Reception — first hours after arrival; peak window for missed withdrawal, suicide, and untreated psychosis.
- Remand — unsentenced custody; uncertainty and first-night risk.
- In-reach — specialist mental health teams delivering care inside prison.
- Healthcare wing / inpatient unit — higher clinical intensity within the prison estate.
- Transfer — move to external psychiatric hospital when needs exceed prison capacity (lawful pathways are jurisdiction-specific — do not invent section numbers).
- Segregation / solitary / separate confinement — highly restricted isolation; a risk amplifier, not a treatment modality.[3][15][16]
This topic is distinct from forensic risk assessment for leave/release court reports (HCR-20-style SPJ), fitness to stand trial, and civil Mental Health Act principles — though all three interfaces appear at the prison gate. The depth here is custodial healthcare delivery from reception to release.[3][18]
Epidemiology — why every registrar must know the base rates
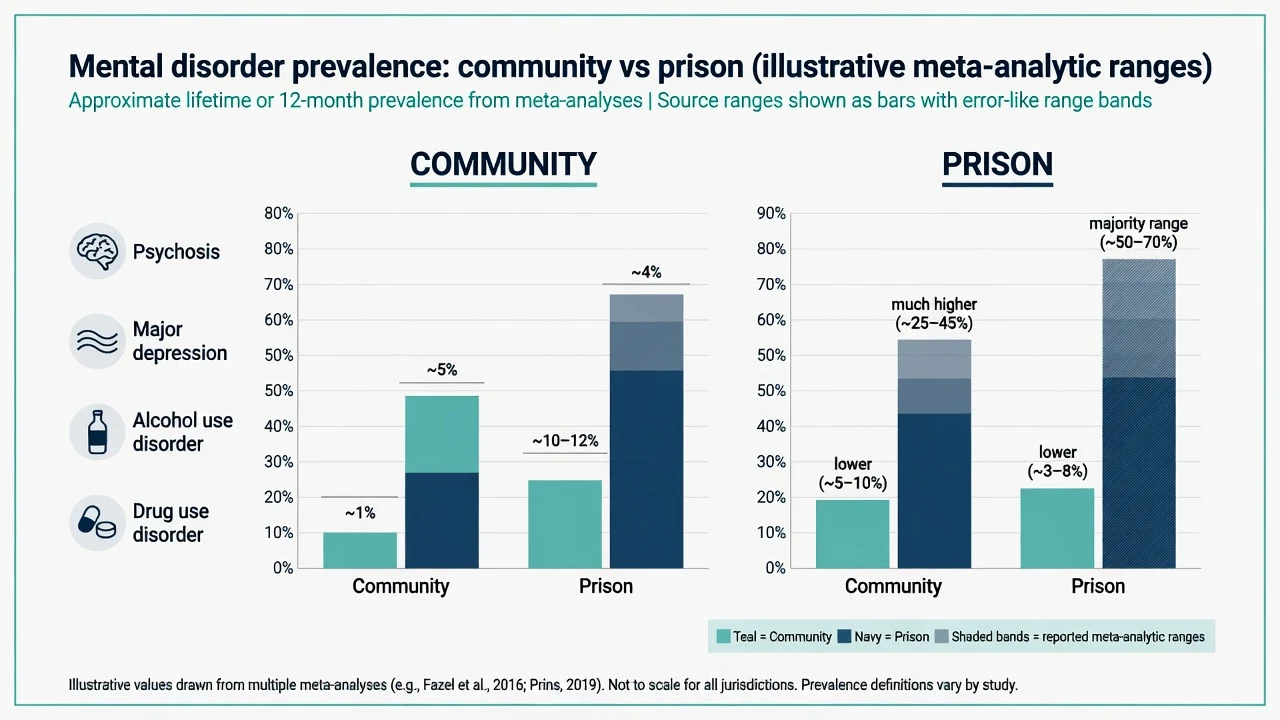
Large systematic reviews place psychotic illness in about 3–4% of prisoners and major depression around 10–12% — several-fold community rates. The 2002 Fazel and Danesh synthesis of 62 surveys (~23,000 prisoners) established the modern base-rate picture; Fazel and Seewald (2012) updated severe mental illness estimates across 33,588 prisoners worldwide.[1][2]
Substance use disorders are the modal comorbidity. Systematic review data show very high prevalence of alcohol and drug abuse/dependence among prisoners compared with the general population — dual diagnosis is ordinary, not exotic.[4][3]
LMIC prison systems also show elevated severe mental illness and SUD in meta-analysis (Baranyi et al.), so the problem is global, not only high-income estate design.[5]
Physical multimorbidity, infectious disease, and disrupted community care amplify psychiatric risk and complicate medicines (e.g. QTc, hepatic disease, opioid agonist therapy continuity).[18]
*Exact SUD proportions vary widely by country, sex, and definition; exam answer emphasises markedly elevated rates versus community, not a single universal percentage.[4]
Prospective work shows mental health needs change during imprisonment — screening once at reception is necessary but not sufficient; re-presentation and mid-sentence deterioration are expected.[12]
Pathophysiology and mechanisms — importation and deprivation
Two complementary models explain high morbidity:
- Importation — people enter custody already carrying high rates of SMI, SUD, trauma, personality disorder, and social disadvantage.
- Deprivation — custody stressors (isolation, bullying, overcrowding, loss of supports, legal uncertainty, substance withdrawal, medication discontinuity) precipitate or worsen illness and self-harm.[3][12]
Segregation multiplies deprivation: reduced stimulation, limited human contact, and uncertainty associate with anxiety, depression, perceptual disturbance, worsening psychosis, self-harm risk, and broader health harms in observational and meta-analytic work.[15][16][17]
Reception screening — the high-yield exam algorithm
Reception is a medical and psychiatric triage, not a paperwork ritual. Aims within hours of arrival:
- Detect active suicide risk and recent self-harm.
- Detect psychosis spectrum symptoms and severe mood disturbance.
- Detect withdrawal risk (alcohol, benzodiazepines, opioids) and intoxication.
- Secure medication continuity (antipsychotics including LAIs, mood stabilisers, antidepressants, opioid agonist therapy where policy allows).
- Identify vulnerability (intellectual disability, trauma, language, Indigenous status, first custody).[3][13][14]
Structured symptom screens at prison entry can capture the spectrum of psychosis clinical stages; self-harm history and recent ideation have predictive value for subsequent self-harm risk after entry — use them, then clinical judgment and observation, not a single checkbox as the whole plan.[13][14]
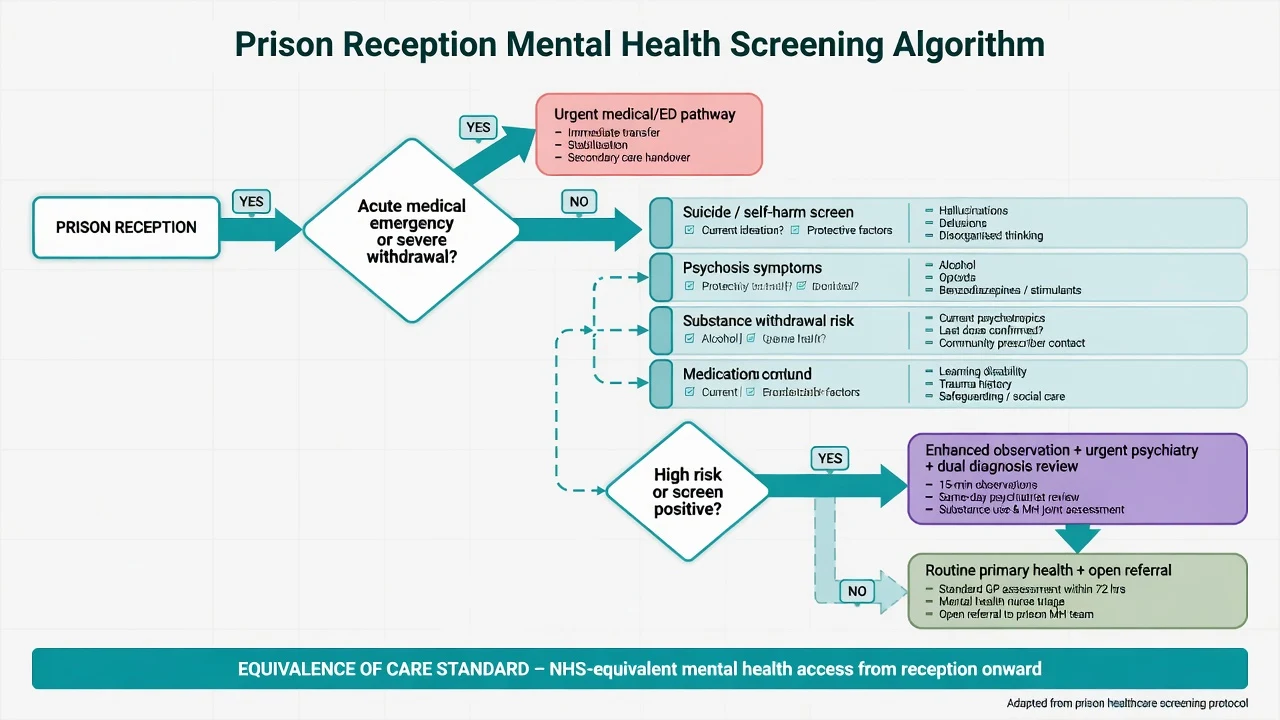
Acute medical priorities at the gate
- Alcohol / benzodiazepine withdrawal — CIWA-style protocols, thiamine, supervised benzodiazepine detoxification per local medical protocol; risk of seizures and delirium tremens.
- Opioid withdrawal — symptomatic care; maintain or initiate opioid agonist treatment according to local prison health policy; abrupt cessation of community methadone/buprenorphine is a safety failure.
- Stimulant crash / intoxication — medical observation; assess for psychosis and suicide after acute phase.
- Missed psychotropics — verify community scripts, last LAI date, and restart promptly when clinically indicated.
Exact drug doses and detox schedules are protocol- and jurisdiction-specific; examiners want the pathway and hazards, not invented national dose tables. Continuity of community medicines and safe withdrawal management are core prison-health safety tasks.[3][18]
Suicide and self-harm — the dominant safety syllabus
Suicide is a leading cause of death in custody in many systems; ecological data across countries show substantial prison suicide burdens.[9][10]
Risk factors for suicide in prison (Zhong et al. systematic review and meta-analysis) include, among others, suicidal ideation, prior self-harm/attempts, psychiatric diagnosis/treatment need, single-cell occupancy, and occupancy-related factors — communicate as a profile, not a prediction score that replaces clinical judgment.[8]
National clinical survey data (Shaw et al.) emphasise recent contact with mental health services, history of self-harm, and the need for active prevention systems rather than post-hoc blame.[10]
Self-harm is common, often clustered in time and place, and associated with later suicide. Hawton and colleagues mapped prevalence, risk factors, clustering, and subsequent suicide in English and Welsh prisons — treat self-harm as a clinical signal, never only a discipline event.[6]
Meta-analysis of self-harm risk factors in prison (Favril et al.) consolidates psychiatric morbidity, prior self-harm, and custodial stressors as key domains for assessment and prevention planning.[7]
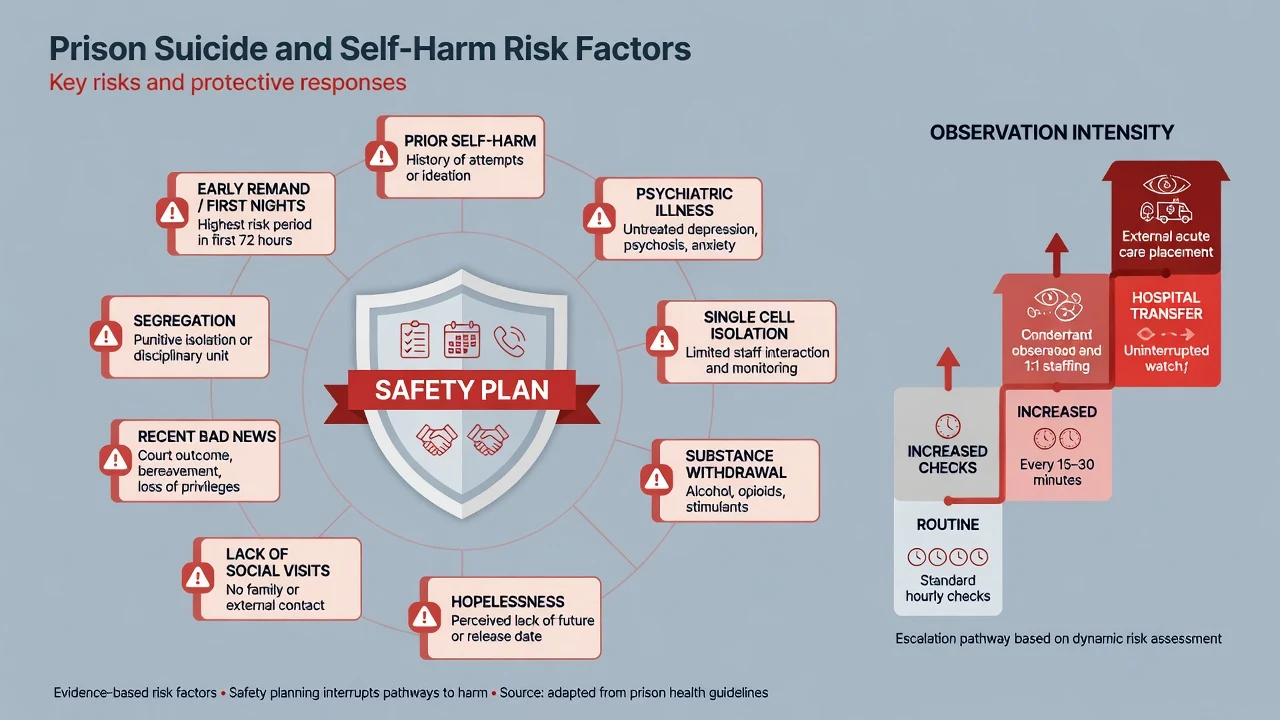
Observation and environment (principles)
Observation intensity steps from routine checks through increased checks and constant/1:1 observation to hospital transfer when needs exceed prison capacity. Match intensity to dynamic risk and review after court outcomes, bullying, or clinical change. Environmental prevention (ligature reduction, safer cells, meaningful activity, social contact) works with clinical care — neither replaces the other. Isolation used as a substitute for care is an exam pitfall.[8][10][3]
Post-release suicide — the forgotten peak
Pratt and colleagues showed markedly elevated suicide rates among recently released prisoners, especially early after release. Exam pearl: prevention does not end at the gate — discharge planning (scripts, appointment, housing, OAT continuity, crisis plan, family contact) is suicide prevention.[11]
Dual diagnosis and substance use
Substance use disorders are so common that any prison mental health formulation that ignores alcohol, opioids, stimulants, and benzodiazepines is incomplete.[4][3]
Integrated dual diagnosis care (not sequential "fix substances first, then psychiatry") is the service model examiners expect: shared goals, concurrent treatment of psychosis/mood and SUD, and custody/social supports in one plan.[3]
Psychopharmacology in custody (exam-level principles)
Prefer agents with established evidence for the disorder; account for diversion risk, QTc, metabolic monitoring, and supervised administration. Long-acting injectable antipsychotics can aid adherence when clinically indicated and consented (or lawfully authorised under local framework). Mood stabilisers and clozapine need laboratory pathways — lack of labs is a system design problem, not a reason to abandon evidence-based care without transfer. Avoid abrupt cessation of community psychotropics at reception. Benzodiazepines: short-term protocolised detox only; chronic diversion risk is real. Do not invent prison formulary rules; local pharmacy policy constrains choice while the clinical standard remains equivalence.[3][18][4]
Segregation and solitary confinement
Segregation (solitary / separate confinement / "the hole") is associated with adverse psychological effects and mortality signals in systematic review and meta-analysis, and with high rates of psychological distress in large survey work.[15][16]
Physical health harms also accumulate in isolation settings.[17]
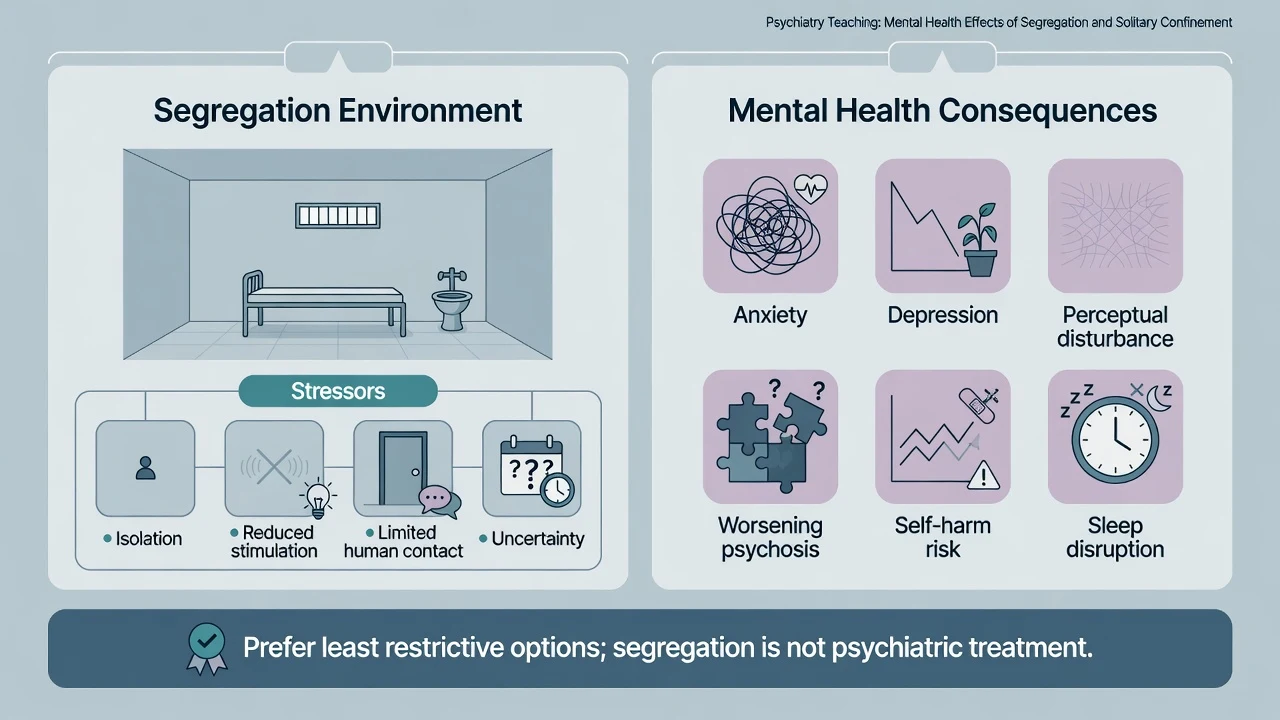
Exam stance: do not recommend segregation as treatment for psychosis, self-harm, or personality disorder crises. If custody places someone in segregation for security reasons, mental health services must increase, not decrease, monitoring and advocacy for step-down. Document deterioration clearly; push for least restrictive alternatives and hospital transfer when indicated.[15][16][3]
Assessment structure (custody-adapted)
Custody-adapted assessment covers: context (remand vs sentenced); history (psychiatric, self-harm, substances, trauma, LAI/OAT); MSE with quoted risk content; risk triad (suicide/self-harm, violence, vulnerability); capacity/legal status (jurisdiction-specific principles only); collateral; and formulation (importation + deprivation, dual diagnosis, protective factors). Structure around high base-rate morbidity and dynamic custody stressors rather than a single checklist score.[3][8][7][4]
- Pre-existing SMI/SUD/trauma
- Social disadvantage
- Interrupted community care
- Explains high base rates
- Isolation and bullying
- Withdrawal and stress
- Legal uncertainty
- Explains mid-sentence change
- Reception screen
- In-reach + dual diagnosis
- Avoid segregation-as-care
- Release transition plan
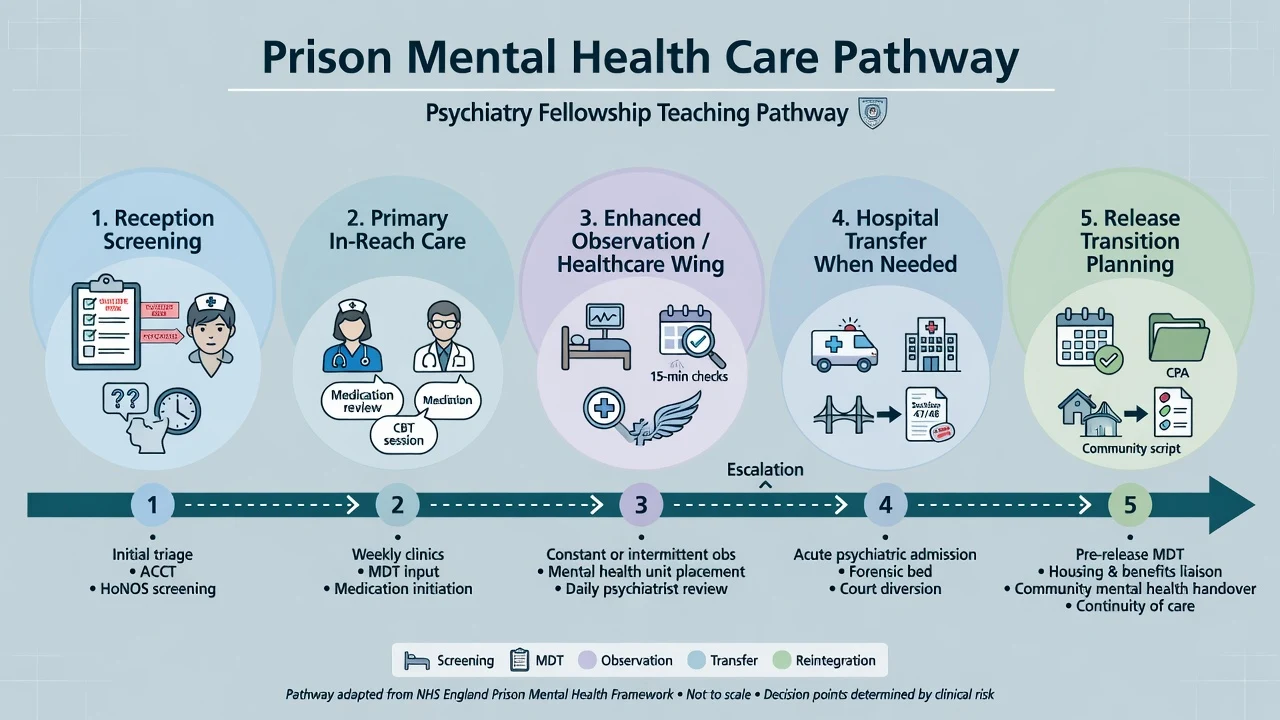
Definitive management and service model
Stepped custodial care
- Primary healthcare — screening, common mental disorders, physical comorbidity, first-line medicines.
- Specialist in-reach — psychiatry, psychology, dual-diagnosis workers, nursing.
- Enhanced observation / healthcare wing — higher acuity within prison.
- External hospital transfer — when needs exceed prison capacity (acute psychosis with high risk, complex detox, need for intensive psychiatric nursing).
- Release and throughcare — appointments, scripts, OAT, housing liaison, crisis contacts — target the post-release suicide window.[3][11]
Self-harm care pathway
Psychosocial assessment after every significant episode; treat underlying depression/psychosis/PTSD/SUD; collaborative safety plan; environmental modifications; avoid purely punitive responses that increase isolation.[6][7]
Psychological therapies
Access should approximate community standards under equivalence: CBT for depression/anxiety/psychosis coping, trauma-informed approaches where skilled, group programmes where safe. Security logistics are barriers to manage, not reasons to abandon therapy altogether.[3]
Multi-agency work
Shared risk with custody officers, health, psychology, and (where relevant) parole/probation. Share need-to-know risk information lawfully; do not dump entire clinical files into the wing office. Confidentiality limits must be explained to the patient at the outset of care. Joint systems for self-harm review and observation are part of effective prevention after epidemiological work showing clustering and service-contact gaps before suicide.[6][10][3]
Differential diagnosis and pitfalls
Differential pitfalls in custody include situational distress versus major depression; primary psychosis versus substance-induced psychosis; withdrawal delirium mis-sent to segregation; personality disorder labels used to withhold treatment for comorbid MDD/PTSD; and organic causes (head injury, seizure, infection, Wernicke) framed as pure behaviour. High SMI and SUD base rates mean these differentials must be worked actively. Malingering for placement is possible but last — false negatives at reception are high-stakes given early-custody suicide risk.[2][4][3][8][10]
Special populations
Special populations needing adapted pathways within the same equivalence and suicide-prevention standards include women (higher depression/PTSD/self-harm in many samples; perinatal care; trauma-informed defaults), youth, older prisoners (depression, cognition, frailty), Indigenous peoples (over-representation; cultural safety), intellectual disability/ABI (vulnerability and adapted communication), and transgender prisoners (placement safety and care continuity). Sex-specific and trauma-related morbidity patterns are emphasised in prison mental health overviews.[3][6][18]
Equivalence of care and prison health governance sit with state/territory health–justice partnerships; Indigenous over-incarceration and cultural assessment are core viva themes. Compulsory treatment and hospital transfer pathways are jurisdiction-specific — cite principles, not invented sections.[3]
Overcrowding and limited in-reach capacity are common realities in many systems including LMICs; meta-analytic work still shows elevated SMI and SUD. Apply equivalence principles and prioritise reception suicide/withdrawal risk and urgent psychosis pathways when resources allow.[5][2]
Prognosis and disposition
Many people improve with treatment, structure, and substance abstinence; others deteriorate under isolation, bullying, or untreated illness. Disposition is a clinical intensity ladder, not a moral ranking. Successful step-down and safer release associate with engagement, substance control, stable aftercare, and reduced acute risk — mirror community forensic logic without requiring full HCR-20 for every wing review.[3][12]
Exam pearls
- Quote psychosis ~3–4% and depression ~10–12% from meta-analyses as order-of-magnitude anchors.[1][2]
- Name SUD as modal comorbidity.[4]
- First nights / early remand and first weeks post-release are suicide peaks.[8][11]
- Self-harm clusters and predicts later suicide risk — assess every episode.[6]
- Segregation is not treatment.[15][16]
- Equivalence of care is the ethical and exam maxim.[3][18]
- Never invent Mental Health Act or prison regulation section numbers across jurisdictions.
- Dual diagnosis = concurrent care, not sequential gatekeeping.
Related topics
Cross-links for board study (each is a separate MedVellum topic): risk assessment in forensic settings; mental health law and involuntary treatment; fitness to stand trial and criminal responsibility; deliberate self-harm and risk assessment; substance use disorders. Prison mental health sits at their custodial intersection without replacing those monographs.[3]
References
- [1]Fazel S, Danesh J Serious mental disorder in 23000 prisoners: a systematic review of 62 surveys Lancet, 2002.PMID 11867106
- [2]Fazel S, Seewald K Severe mental illness in 33,588 prisoners worldwide: systematic review and meta-regression analysis Br J Psychiatry, 2012.PMID 22550330
- [3]Fazel S, Hayes AJ, Bartellas K, et al. Mental health of prisoners: prevalence, adverse outcomes, and interventions Lancet Psychiatry, 2016.PMID 27426440
- [4]Fazel S, Bains P, Doll H Substance abuse and dependence in prisoners: a systematic review Addiction, 2006.PMID 16445547
- [5]Baranyi G, Scholl C, Fazel S, et al. Severe mental illness and substance use disorders in prisoners in low-income and middle-income countries: a systematic review and meta-analysis of prevalence studies Lancet Glob Health, 2019.PMID 30879509
- [6]Hawton K, Linsell L, Adeniji T, et al. Self-harm in prisons in England and Wales: an epidemiological study of prevalence, risk factors, clustering, and subsequent suicide Lancet, 2014.PMID 24351319
- [7]Favril L, Yu R, Hawton K, Fazel S Risk factors for self-harm in prison: a systematic review and meta-analysis Lancet Psychiatry, 2020.PMID 32711709
- [8]Zhong S, Senior M, Yu R, et al. Risk factors for suicide in prisons: a systematic review and meta-analysis Lancet Public Health, 2021.PMID 33577780
- [9]Fazel S, Grann M, Kling B, Hawton K Prison suicide in 12 countries: an ecological study of 861 suicides during 2003-2007 Soc Psychiatry Psychiatr Epidemiol, 2011.PMID 20140663
- [10]Shaw J, Baker D, Hunt IM, et al. Suicide by prisoners. National clinical survey Br J Psychiatry, 2004.PMID 14990526
- [11]Pratt D, Piper M, Appleby L, et al. Suicide in recently released prisoners: a population-based cohort study Lancet, 2006.PMID 16829295
- [12]Hassan L, Birmingham L, Harty MA, et al. Prospective cohort study of mental health during imprisonment Br J Psychiatry, 2011.PMID 21200075
- [13]Yee N, Browne C, Chemjong P, et al. The full spectrum of clinical stages of psychosis at prison entry: prevalence and concurrent validity of symptom screening Soc Psychiatry Psychiatr Epidemiol, 2025.PMID 39080008
- [14]Browne C, Chemjong P, Korobanova D, et al. Self-harm risk screening on prison entry: assessing the predictive validity of self-harm history and recent ideation in men and women Int J Prison Health, 2023.PMID 36422644
- [15]Luigi M, Dellazizzo L, Giguère CÉ, et al. Shedding Light on "the Hole": A Systematic Review and Meta-Analysis on Adverse Psychological Effects and Mortality Following Solitary Confinement in Correctional Settings Front Psychiatry, 2020.PMID 32973582
- [16]Reiter K, Ventura J, Lovell D, et al. Psychological Distress in Solitary Confinement: Symptoms, Severity, and Prevalence in the United States, 2017-2018 Am J Public Health, 2020.PMID 31967876
- [17]Strong JD, Reiter K, Gonzalez G, et al. The body in isolation: The physical health impacts of incarceration in solitary confinement PLoS One, 2020.PMID 33035215
- [18]Fazel S, Baillargeon J The health of prisoners Lancet, 2011.PMID 21093904