Psych · Forensic psychiatry — risk assessment
Risk assessment in forensic settings
Also known as Forensic violence risk assessment · HCR-20 forensic · Structured professional judgement forensic · Actuarial risk assessment forensic · VRAG · Static-99R · SAPROF protective factors · Forensic risk formulation · Secure hospital risk assessment · Release risk assessment
Exam-exhaustive fellowship reference on risk assessment in forensic settings — UCJ vs actuarial vs SPJ; HCR-20 conceptual domains; formulation and scenarios; protective factors (SAPROF concepts); institutional vs community horizons; light sexual-offending pointer; RNR; multi-agency public protection principles; forensic report structure. Distinct from emergency violence-risk imminence. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Risk assessment in forensic settings answers legal-clinical questions that general emergency risk work only touches lightly: what security level, when is leave safe, can this person step down or be released, what should a court or tribunal hear, and how should multi-agency supervision be designed. The product is a defensible opinion that links evidence-based risk factors to concrete scenarios and a risk management plan.[4][5][8][15]
This topic is distinct from emergency violence-risk assessment. The emergency monograph centres imminence tools (DASA/BVC), ED threats, and same-day safety. Forensic practice still uses imminence tools on secure wards, but the examiner depth here is SPJ manuals and domains, actuarial adjuncts, protective factors, institutional vs community horizons, a light sexual-offending pointer, RNR, and report structure.[1][16][17]
Operational terms (forensic risk vocabulary):
- Risk — likelihood × nature/severity × imminence × victims/targets under specified circumstances.
- Formulation — narrative of drivers, scenarios, and preventable pathways.
- Prediction — probabilistic estimate with moderate group-level accuracy only.
- Static factors — relatively fixed history (prior violence, age at first violence, chronic traits).
- Dynamic factors — changeable clinical and situational drivers (symptoms, substances, insight, access).
- Protective factors — strengths and buffers that support desistance and safer management.[1][2][3][9][10]
Classification — three approaches and the SPJ core
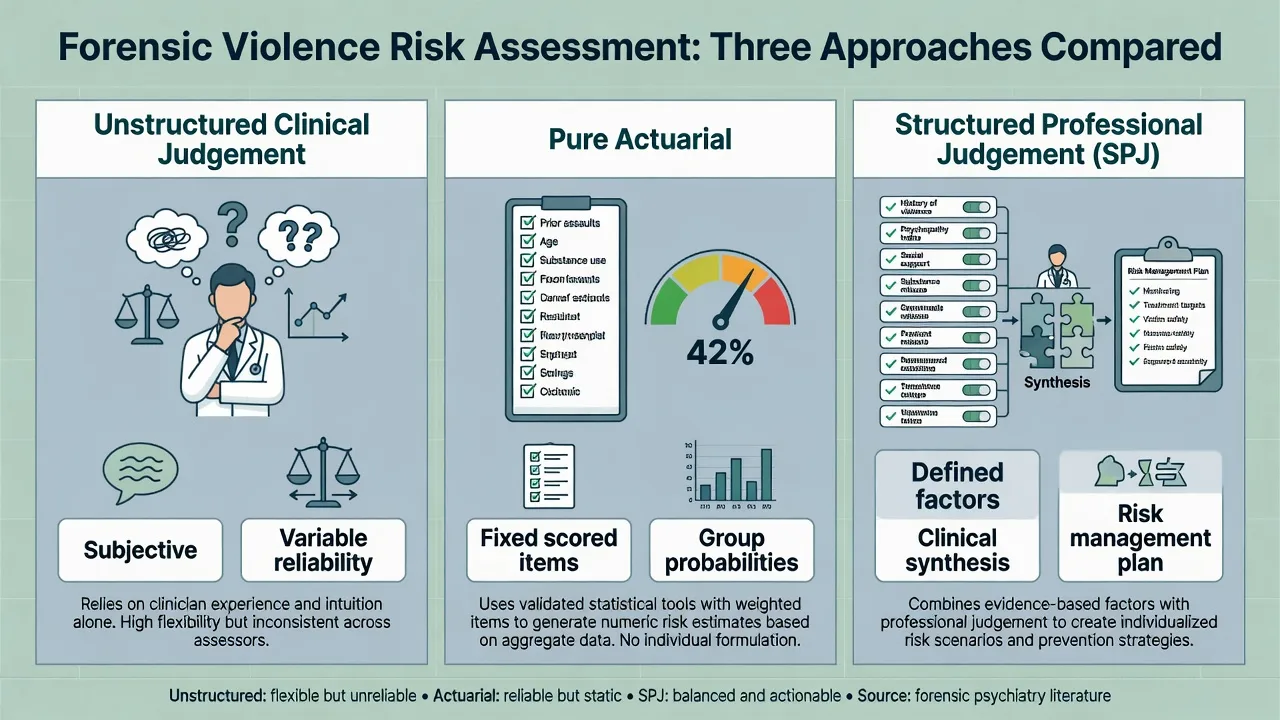
Unstructured clinical judgement (UCJ)
Clinician-only appraisal without a fixed item set. Flexible for unusual cases, but reliability and transparency are poor — historically the weakest predictive performance in comparative work. Examiners still expect you to know its limits and not romanticise "gut feel" for high-stakes leave or release decisions.[3][4]
Pure actuarial tools
Fixed items scored with algorithms (class examples: VRAG / VRAG-R for general violence risk; Static-99R for sexual recidivism). Strengths: transparent scoring, group-level ranking, research base. Limits: often static-heavy, sample-bound, weak for individual certainty, and incomplete as a treatment plan without formulation.[1][12][13]
Structured professional judgement (SPJ)
Defined risk factors (manualised domains) assessed by a trained clinician, integrated with case-specific information into a risk formulation, scenarios, and risk management plan. The prototype in forensic teaching is the HCR-20 family (currently V3 in many services). SPJ is not "a score with a fancy name" — the professional judgement and management plan are the point.[7][8][15]
- No fixed item set
- Flexible for rare cases
- Low transparency
- Historically weakest reliability
- Fixed scored items
- Group probabilities
- Transparent algorithm
- Thin as sole management plan
- Manualised domains
- Clinical synthesis
- Scenarios + plan
- HCR-20-style prototype
HCR-20-style domains (conceptual)
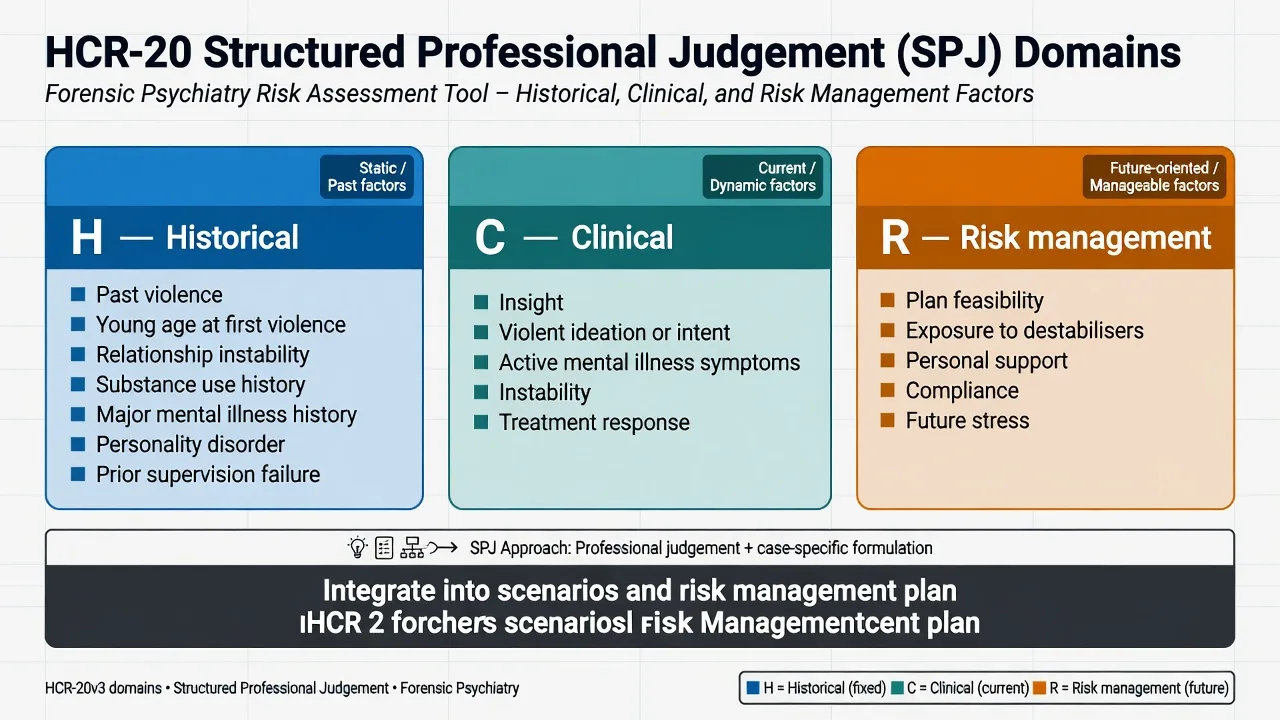
Teach and examine the three-band structure used across HCR-20 versions:
- Historical — past violence and related long-term vulnerabilities (prior violence, young age at first violence, relationship instability, employment problems, substance-use history, major mental illness history, personality disorder, traumatic experiences, prior supervision failure — as conceptual domains, not a photocopy of proprietary item text).
- Clinical — current insight, violent ideation/intent/plans, active symptoms of major mental illness, instability, treatment or supervision response.
- Risk management — feasibility of future plans, exposure to destabilisers, personal support, treatment/supervision compliance, stress/coping in the anticipated living situation.[7][8]
Empirical work supports predictive validity of HCR-20 V3 in mentally disordered offender and civil samples, while critical reflections warn about legal misuse, false precision, and cultural equity issues — cite both utility and limits in viva.[7][8]
Factor types for formulation
| Type | Examples in forensic work | Exam use |
|---|---|---|
| Static | Prior convictions for violence, age at first violence, long-standing antisocial traits | Sets baseline; slow to change |
| Dynamic stable | Entrenched attitudes, chronic substance pattern, personality style | Medium-term therapy and RNR targets |
| Dynamic acute | Relapse of psychosis, intoxication, leave stress, acute rejection | Drive today's observation and leave decisions |
| Protective | Coping, motivation, prosocial network, professional care, stable housing | SAPROF-style strengths; guide desistance plans |
Epidemiology and base-rate humility
Meta-analyses of violence and antisocial risk instruments across tens of thousands of participants show moderate group-level predictive accuracy. Tools help rank relative risk; they do not identify individuals who will reoffend with high certainty in a short window.[1][2][3]
Schizophrenia spectrum disorders elevate relative odds of violence perpetration versus the general population, yet most people with schizophrenia are never violent; absolute risk remains low for many patients, and substances and prior violence concentrate risk more than diagnosis alone.[18][19]
Sexual recidivism base rates are often lower than public stereotype implies; Static-99R and related tools map score bands to observed sexual recidivism rates in large samples — communicate rates with humility and avoid equating "elevated relative risk" with inevitability.[11][12]
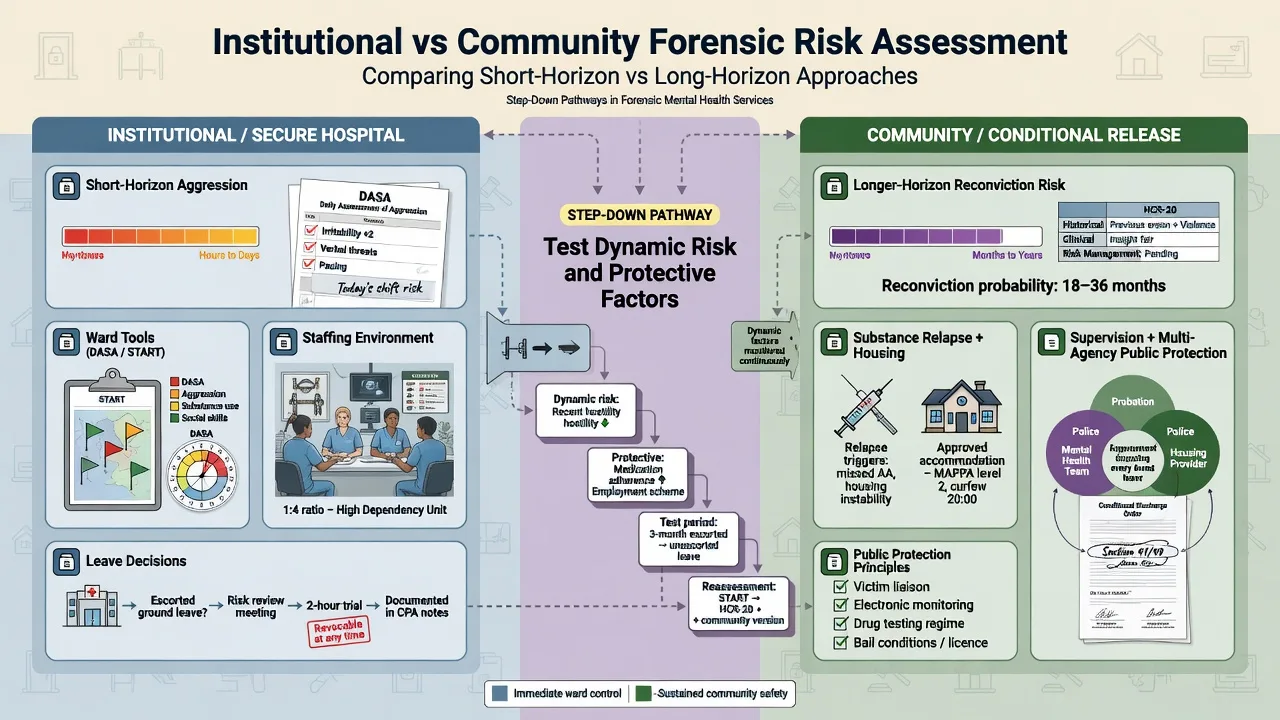
Institutional aggression and community reconviction are different outcomes. A tool validated for community reconviction may under- or over-perform for ward assaults; choose and interpret tools by the decision you are making.[16][17]
Pathophysiology and mechanisms — multi-level model
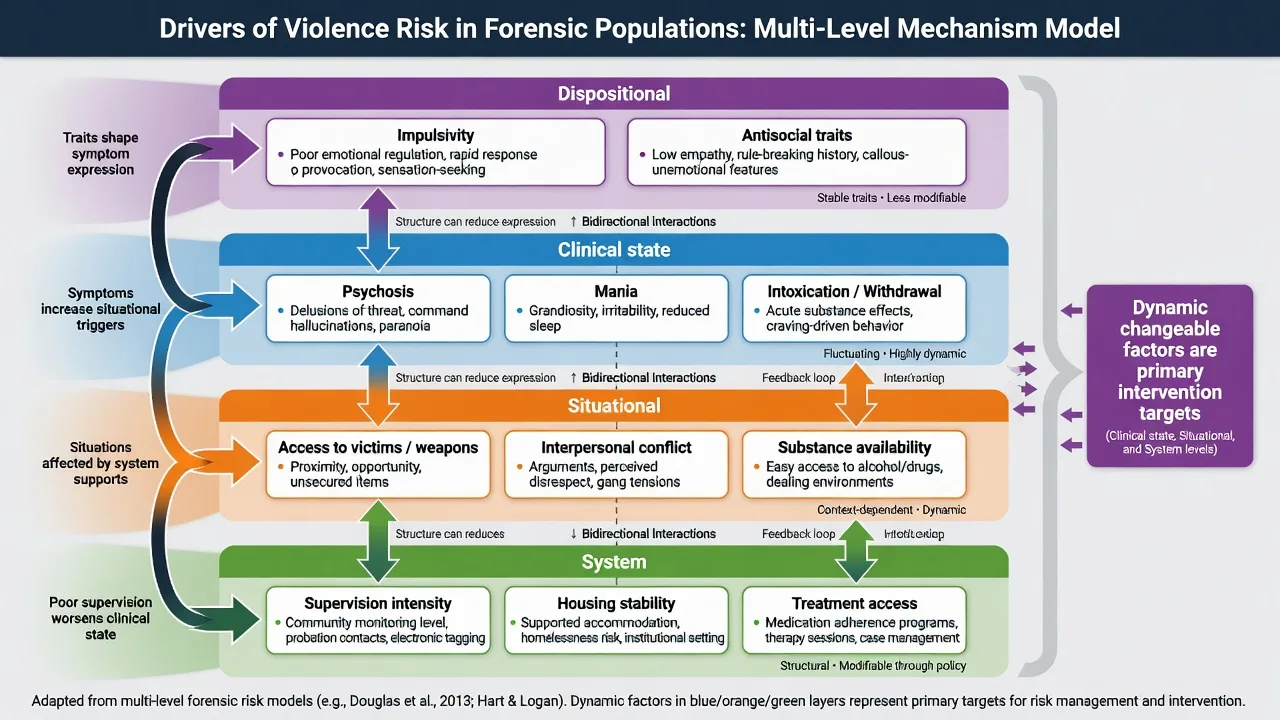
A viva-ready multi-level model:
- Dispositional — impulsivity, antisocial or psychopathic traits, cognitive style, developmental adversity.
- Clinical state — active psychosis (including threat/control-override content), mania, severe affective dysregulation, intoxication/withdrawal, cognitive impairment.
- Situational — access to victims and weapons, interpersonal conflict, substance availability, crowding and staff interaction on wards.
- System — supervision intensity, housing stability, treatment quality, multi-agency information sharing.[4][18]
Risk-Need-Responsivity (RNR)
RNR remains the dominant organisational logic for forensic intervention intensity:
- Risk — match intensity of service to risk level (more intensive for higher risk).
- Need — target criminogenic needs (antisocial attitudes, substance use, impulsivity, criminal peers, family/marital problems, education/employment, leisure) plus treat mental illness as both clinical care and risk management.
- Responsivity — deliver interventions in a style the person can use (cognitive ability, culture, engagement barriers).[14]
Real-world community supervision studies show incomplete but meaningful application of RNR tools; examiners reward linking formulation to actionable needs, not inventory worship.[14]
Protective and desistance processes
Improvements in dynamic risk and protective factors during forensic inpatient treatment predict lower community recidivism after discharge — protective work is not soft decoration; it is evidence-linked risk management.[9]
Clinical presentation in forensic pathways
Typical examiner stems:
- Secure hospital admission after an index offence with psychosis or personality disorder.
- Multidisciplinary review for leave or security step-down.
- Conditional discharge / community forensic follow-up with substance relapse.
- Court or tribunal report on future risk and recommendations.
- Parole-style or multi-agency public protection review.
- Institutional aggression surge on a forensic ward.
- Sexual offence history with upcoming release or victim-related stressor.[8][17]
Atypical patterns: high static actuarial band but strong current protective factors and full treatment response; low static score with fixated threat and means; quiet instrumental planning without florid psychosis; concurrent victimisation and perpetration risk in the same patient.[5][18]
Differential diagnosis of the "risk picture"
- TCO / command content
- Often reactive defensive
- Treat illness urgently
- High yield when untreated
- Intoxication timeline
- Relapse before leave
- SUD is risk treatment
- Reassess when sober
- Planning and gain
- Personality history
- RNR / criminogenic needs
- Security and supervision
Always consider organic contributors (TBI, epilepsy-related aggression, delirium, encephalitis) and concurrent vulnerability (self-harm, exploitation). Malingering for placement is a late hypothesis after thorough multi-source assessment.[18]
Clinical and multi-source assessment
Forensic assessment is file-heavy. Core sources:
- Index offence brief, victim statements (where lawful), police summary.
- Prior convictions and institutional behaviour records.
- Psychiatric, substance, and personality history.
- MSE with quoted threats, targets, and insight.
- Collateral (family, keyworkers, probation/corrections where lawful).
- Prior risk instruments and their dates — revalidate, do not copy blindly.
- Parallel suicide and vulnerability risk.[4][15]
Interview structure mirrors emergency risk work but with deeper historical and future risk-management detail: what will housing, substances, relationships, and supervision look like after leave or release?[8]
Legal status, capacity for specific decisions, and least-restrictive security are jurisdiction-specific. State principles (necessity, proportionality, review rights); do not invent section numbers for ANZ/UK/US statutes in exams unless the stem supplies them.[5]
Investigations and tools — match tool to horizon
Imminent / short-term institutional tools
DASA and related shift-level tools flag near-term aggression risk on wards and should change staffing and observation today.[16]
START (Short-Term Assessment of Risk and Treatability) concepts support multi-outcome short-term risk and strength appraisal in forensic and correctional settings; critical START factors can be used as care targets, not only scores.[17][20]
Intermediate / long-term SPJ
HCR-20 V3 (conceptual use with training): structure Historical, Clinical, and Risk management information into scenarios and a plan for leave, release, and supervision decisions.[7][8]
Actuarial adjuncts
VRAG / VRAG-R class tools provide group-level ranking for general violence risk; revisions and cross-validation studies support continued research use with acknowledged limits in new samples.[13]
Sexual risk (light pointer)
For sexual offending pathways, static actuarial tools (Static-99R class) have the strongest evidence base among sexual recidivism instruments; meta-analyses show moderate accuracy overall, with static tools generally outperforming unstructured approaches. Score bands map to observed sexual recidivism rates — always pair with dynamic and protective assessment for management, not static scores alone.[10][11][12]
Psychopathy constructs
PCL-class psychopathy measures inform personality risk traits (callousness, shallow affect, behavioural lifestyle) relevant to instrumental violence and treatment responsivity. They are not a diagnosis that dooms the person; integrate into formulation and RNR responsivity planning.[3]
Management — immediate safety (forensic ward / leave crisis)
Immediate priorities mirror emergency care inside secure settings:
- Environment, staffing, observation level, weapon search, separate potential victims.
- Treat acute psychosis, mania, intoxication, akathisia, pain, and delirium.
- De-escalation before seclusion/restraint; least restrictive force.
- Suspend leave if dynamic risk has spiked (substance relapse, new threats, rising institutional scores).
- Multi-agency notification principles when a named community victim is at imminent risk (jurisdiction-specific pathways).[16][18][20]
Management — definitive: formulation to plan
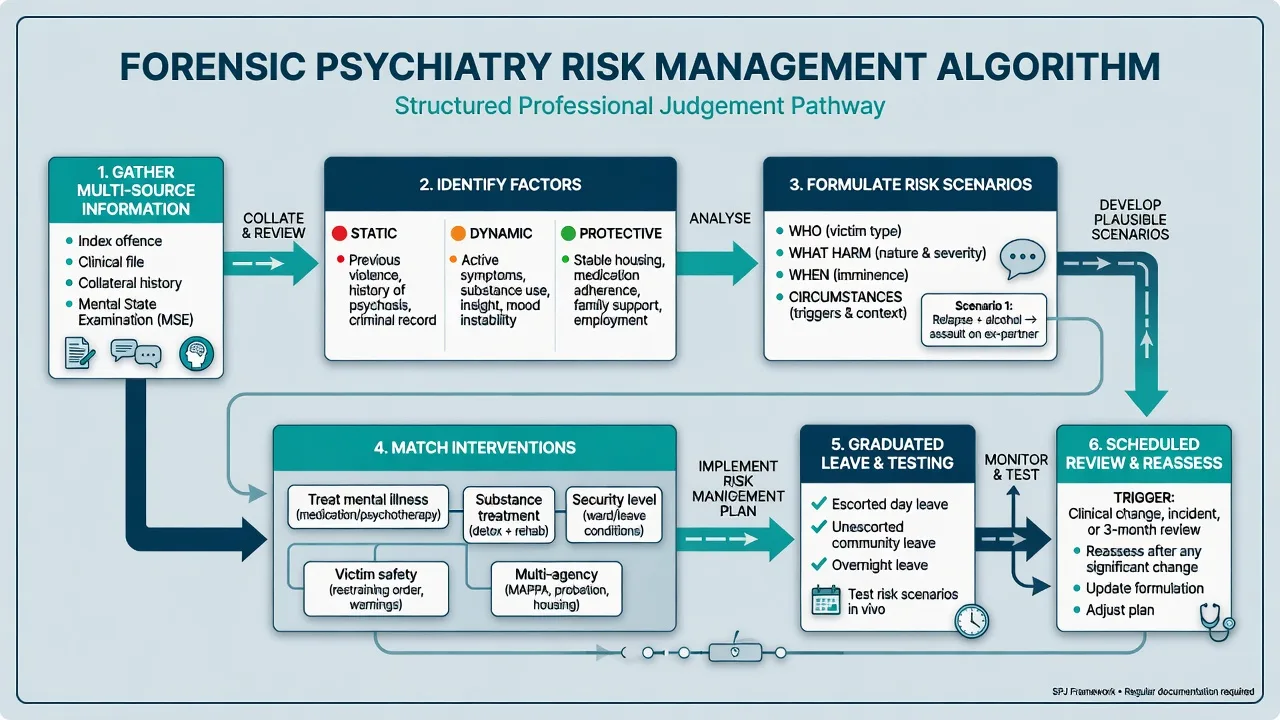
Scenario planning (exam gold)
Write risk scenarios in plain language:
- Who is at risk (named person, staff class, intimate partner, public)?
- What harm (assault, sexual offence, arson, stalking)?
- When (hours after leave, after substance use, after relationship rupture)?
- Under what circumstances (non-adherence, homelessness, unsupervised contact)?
- What prevents it (medication adherence, abstinence monitoring, supervised leave, no-contact conditions, housing, therapy)?[4][15]
Protective factors in the plan
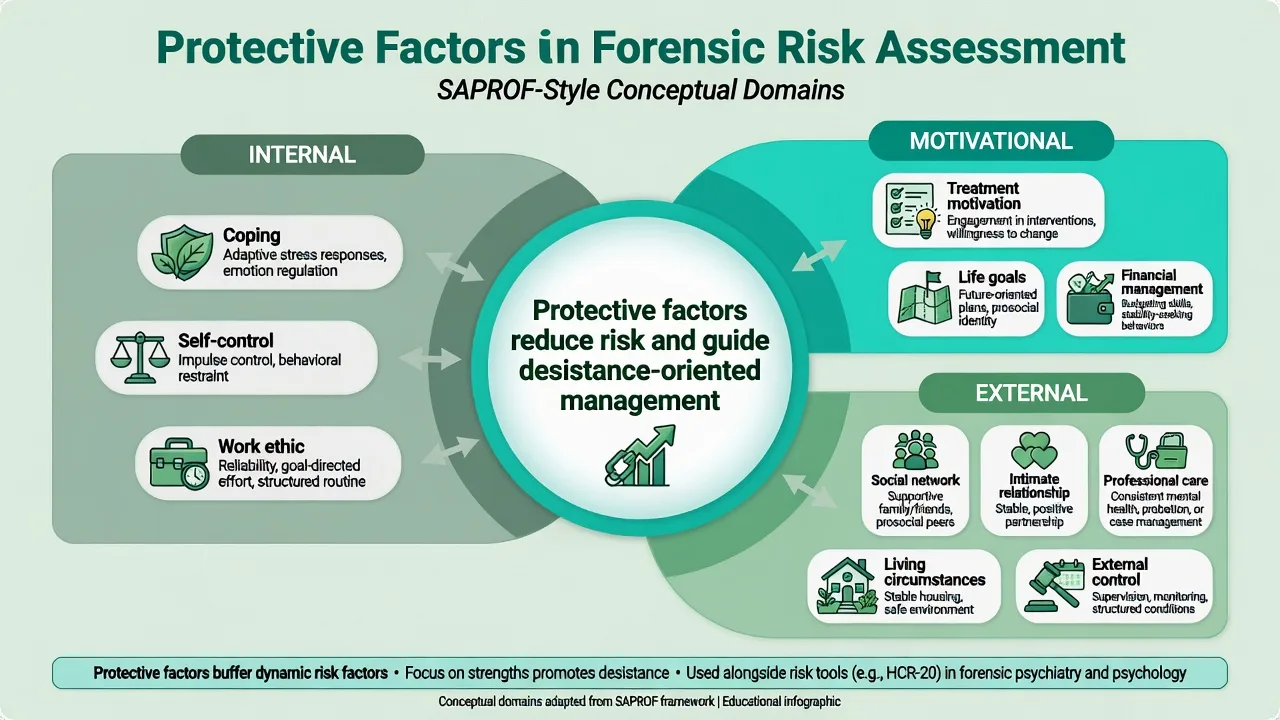
Assess and build protective factors: coping, self-control, work or structured activity, treatment motivation, life goals, social network, intimate relationship quality, professional care continuity, living circumstances, and appropriate external control. Improvements in protective factors during forensic treatment associate with reduced post-discharge recidivism.[9][10]
Security, leave, and step-down
Graduated leave tests dynamic risk and protective factors under increasing freedom. Contingency plans must specify what happens if substances reappear, insight collapses, or a victim is approached. Step-down decisions are dynamic-factor decisions dressed as administrative ones.[8][9]
Multi-agency public protection (principles)
Many jurisdictions use multi-agency frameworks (MAPPA-like in the UK; local forensic/community partnerships in ANZ) to share information and coordinate supervision for higher-risk sexual and violent offenders. Know the principle (proportionate multi-agency planning for public protection) without inventing local statutory section numbers.[8]
Review triggers
Reassess after clinical change, substance relapse, leave or release, relationship rupture, non-adherence, new threats, victim contact, or change in housing/supervision. Stale risk reports are a patient-safety and professional-standards failure.[5][15]
Specific subtypes and scenarios
Institutional aggression
Use short-horizon tools (DASA/START-style), environmental controls, staffing, and acute clinical treatment. HCR Clinical items often spike before leave decisions are safe.[16][17][20]
Community forensic / conditional release
Longer-horizon SPJ, substance monitoring, housing, social supports, multi-agency information sharing, and clear recall pathways if dynamic risk escalates.[8][9]
Sexual offending pathway (pointer)
Use Static-99R-class static ranking, pair with dynamic sexual risk and SAPROF-style protective assessment for sexually violent pathways, and manage victim access and supervision conditions. Do not generalise a general violence tool to sexual recidivism without justification.[10][11][12]
Personality disorder / high psychopathy traits without psychosis
Emphasise instrumental risk, RNR criminogenic needs, boundaries, and supervision; antipsychotic treatment is not a risk solution if there is no psychosis. Responsivity adaptations matter.[14]
Intellectual disability and youth interfaces
Adapted tools and base rates apply (e.g. youth-oriented SPJ such as SAVRY in youth services). Do not apply adult norms blindly; seek specialist forensic ID/youth input.[2]
Complications and pitfalls
Classic failures:
- Ignoring protective factors and writing only risk lists.
- Confusing imminence tools with long-horizon instruments.
- Incomplete index offence and file review before court opinion.
- Stigmatising language that equates mental illness with permanent dangerousness.
- Inventing statute section numbers or over-claiming legal expertise outside training.
- Cultural and equity bias concerns with tools in Indigenous and minority populations — interpret cautiously and prefer formulation over mechanical cut-offs.
- Copying an old report without reassessing dynamic factors after treatment change.[5][8][9][15][16][17][19]
Prognosis and disposition ladder
Disposition typically moves high secure → medium/low secure → community forensic → general services when dynamic risk falls and protective factors and supports strengthen. Predictors of safer step-down include treatment response, substance control, stable housing, engagement, reduced clinical risk items, and stronger protective scores — not static history alone.[9][18]
Base-rate humility remains mandatory: most people labelled "moderate risk" will not commit rare catastrophic violence in any given short window; still act on preventable dynamic drivers.[1][6]
Special populations
- Women in forensic services — different base rates and validation caveats; avoid male-normed cut-offs without thought.[2]
- Youth / emerging adults — developmental tools and family systems; shorter static histories.
- Older adults — neurocognitive disorders, frailty, different aggression drivers.
- Intellectual disability / autism — adapted communication and tools; environmental triggers.
- Indigenous and cultural minorities — documented concerns about tool equity; prioritise culturally informed formulation and local expertise.[8]
- Sexual vs general violence pathways — different instruments and victim-safety logic.[11][12]
Evidence, guidelines, and regional differences
FRANZCP candidates should describe SPJ-informed forensic practice, least-restrictive secure care principles under state/territory mental health and forensic legislation (name principles, not invented sections), and local community forensic / multi-agency partnerships for higher-risk cases. Align clinical language with RANZCP professional standards for reports and expert evidence where applicable.[4][5][8]
Landmark evidence anchors for exams:
- Instrument performance metas (Fazel 2012; Singh 2011; Yang 2010).
- Actuarial vs clinical debate moved beyond false dichotomies (Buchanan).
- Critiques of unhelpful risk categorisation (Large and Ryan).
- HCR-20 V3 evaluation and legal-context reflection.
- Protective factors and treatment change (SAPROF-linked studies).
- Sexual risk accuracy and Static-99R rates (Hanson).
- RNR real-world use.[1][2][3][4][5][6][7][8][9][10][11][12][14]
Forensic report structure
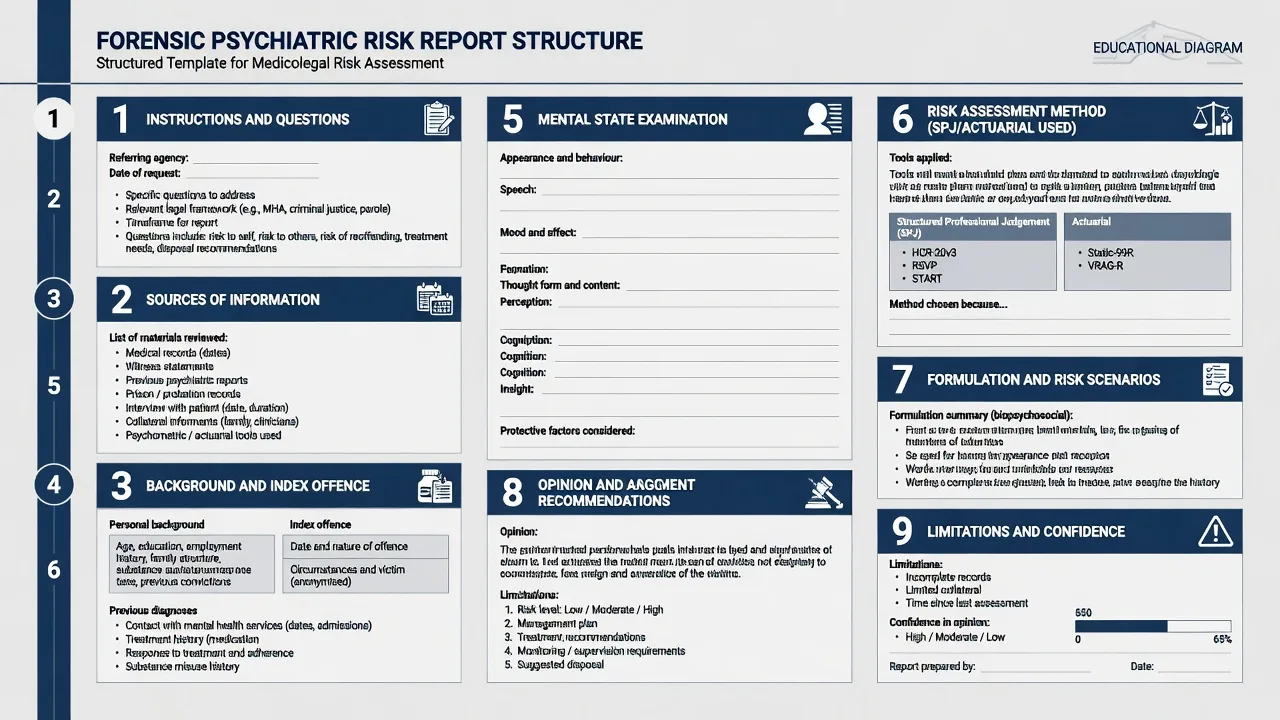
A high-scoring forensic risk report typically includes:
- Instructions and questions asked (and questions not asked).
- Sources of information and interviews conducted (and missing sources).
- Background and index offence narrative from primary documents.
- Psychiatric, substance, and personality history and treatment response.
- Mental state at assessment with quotations for risk-relevant content.
- Method — which SPJ/actuarial tools were used, training, and dates.
- Formulation — static, dynamic, protective factors; risk scenarios.
- Opinion answering the legal-clinical questions with reasoning.
- Recommendations (security, treatment, supervision, victim safety) proportionate to risk.
- Limitations, confidence bounds, and need for reassessment if circumstances change.[5][8][15]
Risk communication research using SPJ frameworks emphasises clarity about nature of risk, not only a severity adjective, when speaking to teams and legal audiences.[15]
Exam pearls
SCENARIO
- SPJ = structure + judgement + plan, not a pure score.[8]
- Protective factors are examinable and evidence-linked to outcome change.[9]
- Static-99R-class for sexual pathways; do not blur with general violence tools without reason.[11][12]
- Never only low/medium/high — write scenarios.[5][6]
- Statutes are local — principles yes, invented sections no.[5]
Self-test: leave decision after methamphetamine relapse
A patient on medium secure leave has negative UDS for months, then tests positive for methamphetamine after a day leave, with rising irritability and no new offence. Answer outline: suspend further unescorted leave; reassess Clinical and Risk-management items; treat substance relapse as dynamic risk escalation; rebuild protective structure (supports, monitoring); document scenario (community aggression or victim contact under intoxication); multi-disciplinary review before restoring leave. Static history has not changed — dynamic and protective have.[9][18]
References
- [1]Fazel S, Singh JP, Doll H, et al. Use of risk assessment instruments to predict violence and antisocial behaviour in 73 samples involving 24 827 people: systematic review and meta-analysis BMJ, 2012.PMID 22833604
- [2]Singh JP, Grann M, Fazel S A comparative study of violence risk assessment tools: a systematic review and metaregression analysis of 68 studies involving 25,980 participants Clin Psychol Rev, 2011.PMID 21255891
- [3]Yang M, Wong SC, Coid J The efficacy of violence prediction: a meta-analytic comparison of nine risk assessment tools Psychol Bull, 2010.PMID 20804235
- [4]Buchanan A Risk of violence by psychiatric patients: beyond the "actuarial versus clinical" assessment debate Psychiatr Serv, 2008.PMID 18245161
- [5]Large MM, Ryan CJ, Nielssen OB Helpful and unhelpful risk assessment practices Psychiatr Serv, 2010.PMID 20439381
- [6]Large MM, Ryan CJ, Singh SP, et al. The predictive value of risk categorization in schizophrenia Harv Rev Psychiatry, 2011.PMID 21250894
- [7]Chen Y, Douglas KS, Zhang Z, et al. Evaluating the HCR-20(V3) violence risk assessment measure with mentally disordered offenders and civil psychiatric patients Behav Sci Law, 2023.PMID 36893019
- [8]de Vogel V, De Beuf T, Shepherd S, et al. Violence Risk Assessment with the HCR-20(V3) in Legal Contexts: A Critical Reflection J Pers Assess, 2022.PMID 35061555
- [9]De Vries Robbé M, de Vogel V, Douglas KS, et al. Changes in dynamic risk and protective factors for violence during inpatient forensic psychiatric treatment: predicting reductions in postdischarge community recidivism Law Hum Behav, 2015.PMID 24933171
- [10]de Vries Robbé M, de Vogel V, Koster K, et al. Assessing protective factors for sexually violent offending with the SAPROF Sex Abuse, 2015.PMID 25210106
- [11]Hanson RK, Morton-Bourgon KE The accuracy of recidivism risk assessments for sexual offenders: a meta-analysis of 118 prediction studies Psychol Assess, 2009.PMID 19290762
- [12]Hanson RK, Thornton D, Helmus LM, et al. What Sexual Recidivism Rates Are Associated With Static-99R and Static-2002R Scores? Sex Abuse, 2016.PMID 25810478
- [13]Gregório Hertz P, Eher R, Etzler S, et al. Cross-Validation of the Revised Version of the Violence Risk Appraisal Guide (VRAG-R) in a Sample of Individuals Convicted of Sexual Offenses Sex Abuse, 2021.PMID 31010400
- [14]Dyck HL, Campbell MA, Wershler JL Real-world use of the risk-need-responsivity model and the level of service/case management inventory with community-supervised offenders Law Hum Behav, 2018.PMID 29620397
- [15]Storey JE, Watt KA, Hart SD An examination of violence risk communication in practice using a structured professional judgment framework Behav Sci Law, 2015.PMID 25615811
- [16]Ogloff JR, Daffern M The dynamic appraisal of situational aggression: an instrument to assess risk for imminent aggression in psychiatric inpatients Behav Sci Law, 2006.PMID 17171770
- [17]Cartwright JK, Desmarais SL, Hazel J, et al. Predictive validity of HCR-20, START, and static-99R assessments in predicting institutional aggression among sexual offenders Law Hum Behav, 2018.PMID 28857580
- [18]Witt K, van Dorn R, Fazel S Risk factors for violence in psychosis: systematic review and meta-regression analysis of 110 studies PLoS One, 2013.PMID 23418482
- [19]Fazel S, Gulati G, Linsell L, et al. Schizophrenia and violence: systematic review and meta-analysis PLoS Med, 2009.PMID 19668362
- [20]Pollak C, Palmstierna T Reducing Risk for Future Violence From Forensic Psychiatric Patients by Using Critical Factors of the Short-Term Assessment of Risk and Treatability as a Caring Tool J Forensic Nurs, 2024.PMID 38048491