Psych · Forensic psychiatry — sexual offending
Sexual offending
Also known as Sexual offender assessment · Sex offender risk assessment · Static-99R · STABLE-2007 ACUTE-2007 · Sexual recidivism · Paraphilic disorders forensic · Child sexual offending psychiatry · Motivation facilitation model · WFSBP paraphilic treatment · Forensic sex offence treatment
Exam-exhaustive fellowship reference on sexual offending for forensic psychiatry — legal vs clinical constructs; pedophilia vs child sexual offending; motivation–facilitation model; static/dynamic/protective risk (Static-99R, STABLE/ACUTE concepts); multi-source assessment; RNR-informed psychological treatment; WFSBP-aligned pharmacotherapy principles for high-risk paraphilic pathways; multi-agency public protection; ethics. Clinical and non-sensational. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Sexual offending covers behaviours defined as criminal by statute: non-consensual sexual contact or acts, sexual offences against children (including many online offences involving child sexual exploitation material), and related non-contact offences depending on jurisdiction. The legal definition is primary for courts; psychiatry does not “diagnose sexual offender” as a disease entity.[5][18]
The fellowship task is precise and non-sensational: (1) assess the person comprehensively; (2) appraise risk of further sexual harm (and often general violence or rule-breaking) with structured methods; (3) formulate who is at risk of what, when, under which circumstances; (4) design proportionate treatment and supervision; (5) communicate clearly to courts, tribunals, and multi-agency partners without false precision or stigma theatre.[2][13][15]
This topic is distinct from the specialty monograph on sexual dysfunction and paraphilias (clinical sexual medicine and paraphilic disorders with lighter forensic pointer) and from general forensic risk assessment (HCR-20-style SPJ with only a light sexual pointer). Here the examiner depth is sexual-offence pathways, sexual-specific risk tools, and sexual-offence treatment principles.[2][5]

Operational vocabulary:
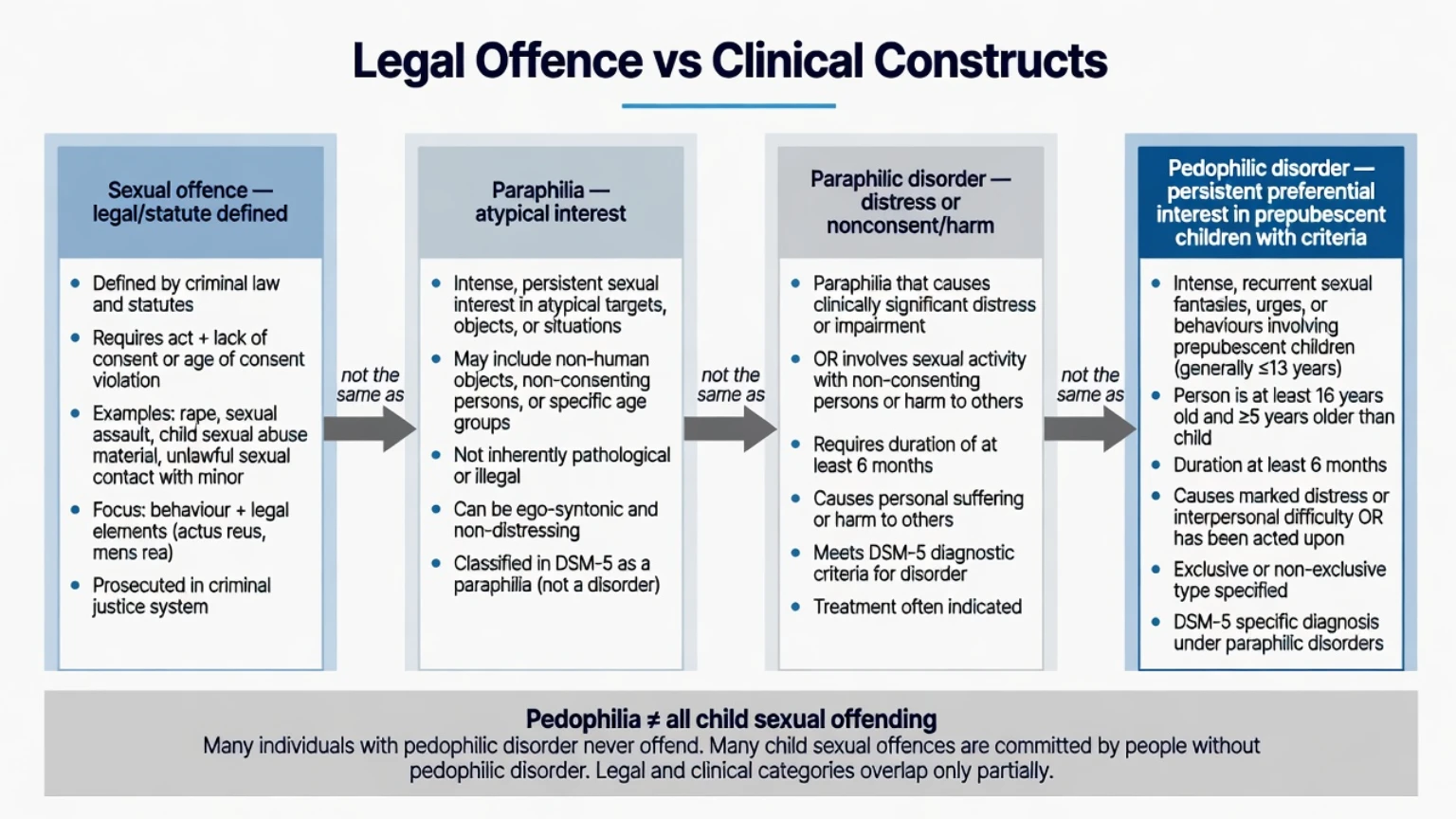
- Sexual offence — legally defined criminal behaviour.
- Paraphilia — intense persistent atypical sexual interest; not automatically a disorder.
- Paraphilic disorder — paraphilia with marked distress/impairment or involving nonconsenting persons / risk of harm.
- Pedophilic disorder — persistent preferential sexual interest in prepubescent children meeting diagnostic criteria — not synonymous with all child sexual offending.
- Sexual recidivism — further sexual offence after an index offence (definition varies by study: charge, conviction, self-report).
- Criminogenic need — changeable risk factor linked to reoffending and therefore a treatment target.[1][4][18]
Classification — legal category vs clinical constructs
Typology useful in exams (not exhaustive)
| Axis | Examiner distinctions |
|---|---|
| Contact vs non-contact | Physical sexual offences vs exhibitionism, some online offences |
| Victim age | Child vs adult; developmental status matters for pedophilic preference |
| Relationship | Intrafamilial vs extrafamilial |
| Preference | Preferential deviant interest vs opportunistic/antisocial |
| Setting | Community, institutional, online |
| Mental state | Patterned sexual offending vs mania/psychosis/intoxication-driven sexual behaviour |
| These axes organise formulation; they are not mutually exclusive diagnoses. Preferential vs opportunistic pathways matter because metas emphasise both sexual deviance and antisocial orientation as core predictors.[1][5] |
ICD-11 and DSM-5-TR retain harm, consent, and distress framing for paraphilic disorders. Consensual adult atypical sexual interests without distress or nonconsent must not be pathologised.[18]
Epidemiology and base-rate humility
Meta-analyses of sexual-offence recidivism research identify deviant sexual interests and antisocial orientation as the major predictors of sexual recidivism across adult and adolescent samples. Clinical presentation variables such as denial or low victim empathy are often weak or inconsistent predictors compared with these two domains — a classic viva trap.[1][4]
Across large instrument meta-analyses, empirically derived actuarial measures outperform unstructured professional judgement for sexual, violent, and general recidivism prediction at the group level. Accuracy is moderate, not deterministic; SPJ sits between pure actuarial and unstructured approaches in aggregate reviews.[2][14]
Static-99R and related static tools map score bands to observed sexual recidivism rates in multi-sample work. Overall rates in many normative samples are lower than public stereotype implies — communicate relative elevation without implying inevitability.[3]
People convicted of sexual offences frequently show higher rates of non-sexual general recidivism than sexual recidivism in follow-up studies. Always specify the outcome you are predicting (sexual vs any violence vs any reoffending).[1][2]
Pathophysiology and mechanisms — motivation and facilitation
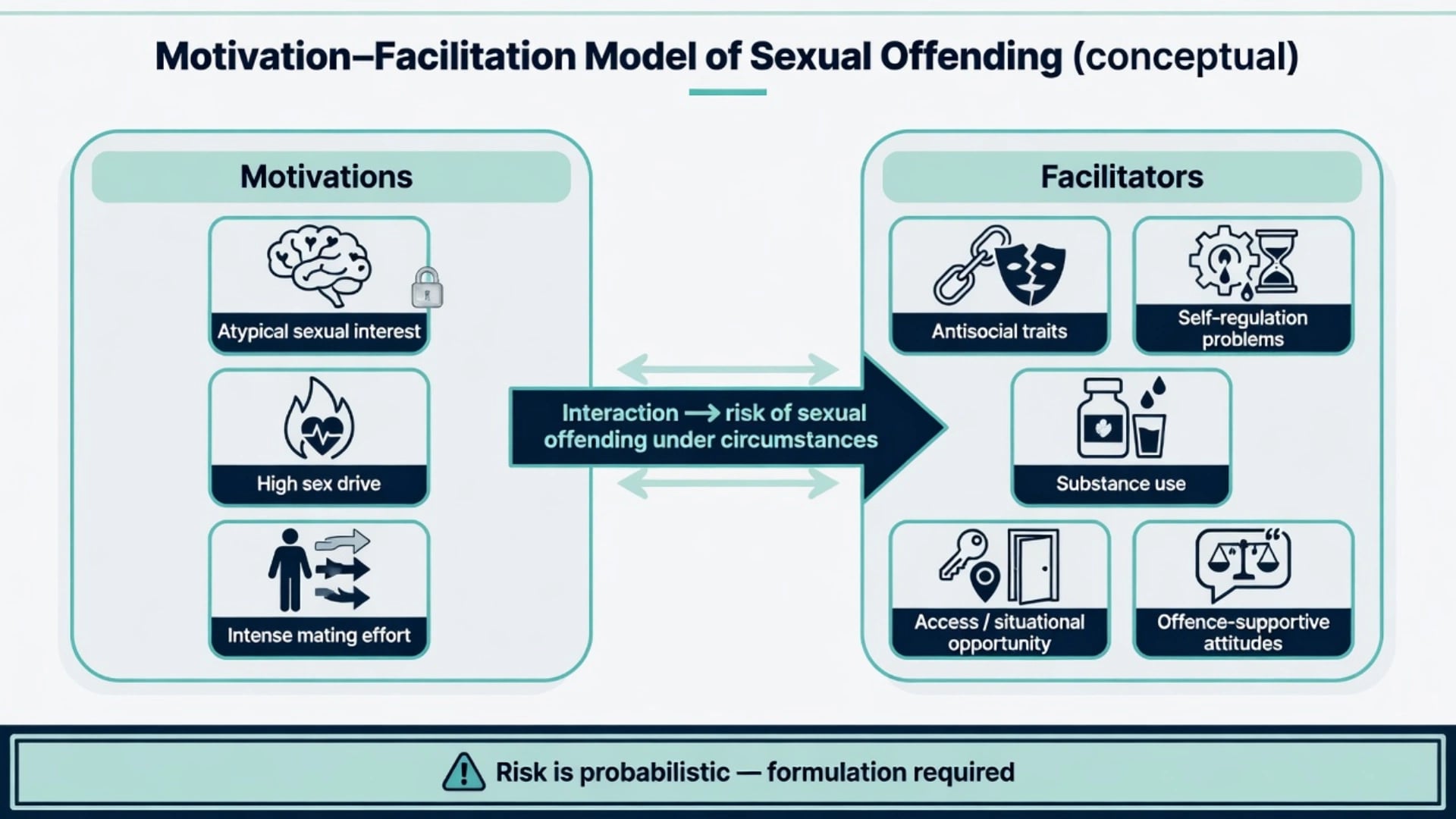
Seto’s motivation–facilitation model organises sexual offending risk as an interaction between:
- Motivations — paraphilic interests (including pedophilia), high sex drive, intense mating effort / impersonal sexuality.
- Facilitators — antisocial traits and attitudes, self-regulation problems, substance intoxication, situational opportunity/access, offence-supportive beliefs.[5]
Dual-pathway teaching model
Examiners reward a clean dual (and mixed) pathway framing:
- Preferential / sexually deviant pathway — persistent atypical sexual interest with high sexual preoccupation; risk rises when facilitators remove brakes.
- General antisocial / opportunistic pathway — sexual offences as part of broader rule-breaking, impulsivity, and exploitation without preferential pedophilic interest.
- Mixed — both elevated deviance and antisocial facilitation (often higher concern for sexual recidivism in metas).[1][5]
Psychologically meaningful dynamic factors
Mann, Hanson, and Thornton argue risk factors should be psychologically meaningful — plausible mechanisms that can guide treatment, not only statistical correlates. Domains repeatedly highlighted in sexual risk literature include sexual preoccupation, offence-supportive attitudes, intimacy deficits, emotional congruence with children (where relevant), lifestyle impulsivity, resistance to rules/supervision, and poor problem-solving.[4]
Protective and desistance processes
Protective factors (SAPROF-class concepts applied to sexually violent offending) add incremental information beyond risk-only tools in research samples and should feed strength-based supervision and treatment goals. Improvements in dynamic risk and protective factors during forensic treatment relate to better post-discharge outcomes in violence research — the same logic applies when managing sexual risk pathways.[9][10]
Clinical presentation in forensic pathways
Typical stems:
- Sentencing or parole report after conviction for a sexual offence.
- Secure hospital admission with dual diagnosis (e.g. psychosis plus sexual index offence).
- Community forensic review before leave, conditional discharge, or reduced supervision.
- First detection of online child sexual exploitation material without known contact offences.
- Person with pedophilic interest seeking help before any known offence (prevention ethics).
- Institutional sexual risk review after boundary breaches on a ward or in prison.[11][12]
Interview stance: calm, non-collusive, non-humiliating. Expect minimisation, partial disclosure, or shame-driven withdrawal. File evidence (index offence brief, prior convictions, digital forensic summaries provided lawfully by investigators) is mandatory — not optional background colour.[13][15]
Parallel suicide risk after arrest or media exposure is common and must be managed without abandoning public-protection duties.[13][15]
Differential diagnosis of the “sexual risk picture”
- Persistent interest in prepubescent children
- May have no adult partners
- Risk if access + weak control
- Not automatic offending
- Broader criminal history
- Substance facilitation
- Less preferential pattern
- RNR general needs heavy
- Mania / psychosis / delirium
- Intoxication timeline
- Treat state urgently
- Reassess when stable
Also separate:
- Consensual adult atypical interest without distress or nonconsent (not a disorder).
- Intellectual disability / autism with boundary problems, suggestibility, or social naivety — adapted formulation required.
- New late-life sexual boundary violations with neurocognitive change — organic work-up.[5][18]
Clinical and multi-source assessment
Forensic sexual risk assessment is file-heavy:
- Index offence brief and victim statements where lawful.
- Prior sexual and non-sexual convictions; institutional behaviour.
- Developmental, sexual, relationship, and substance history.
- Mental illness, personality, trauma, and neurodevelopmental history.
- MSE with quoted ideation, planning, insight, and attitudes (without graphic detail in notes beyond clinical necessity).
- Collateral (family, keyworkers, probation/corrections where lawful).
- Prior risk tools with dates — revalidate; do not copy blindly.
- Parallel suicide and vulnerability risk.[2][13]
Confidentiality limits apply when identifiable children or named persons are at imminent risk. Mandatory reporting and multi-agency information-sharing rules are jurisdiction-specific — state principles (necessity, proportionality, child protection primacy); do not invent section numbers.[15]
Investigations and risk tools — match tool to decision
Static actuarial (sexual)
Static-99R-class tools remain the most widely examined static instruments for adult male sexual recidivism ranking. Score bands associate with observed sexual recidivism rates across samples; age weighting is a core revision concept. Strengths: transparent historical items, research base. Limits: weak as a sole management plan, sample and outcome dependent, limited dynamic sensitivity.[2][3]
Dynamic tools (stable and acute)
STABLE-2007 (stable dynamic needs) and ACUTE-2007 (acute community supervision factors) concepts track changeable risk for men with sexual offences, including research extension to child sexual exploitation material adjudications. Predictive validity supports use for supervision and progress monitoring; recent scores often outperform outdated ones — reassess.[12]
SPJ and multi-outcome tools
Sexual violence SPJ manuals (SVR-20 / RSVP-class concepts) and general violence SPJ (HCR-20) apply when violence co-occurs or institutional aggression is the decision horizon. START-class multi-outcome tools and Static-99R have been studied for institutional aggression among people with sexual offence histories — match tool to institutional vs community outcome.[11]
Protective factors
SAPROF-class protective assessment for sexually violent offending supports balanced formulation and targets for strengthening supports, coping, and professional care.[9]
Medical work-up before pharmacotherapy
Before antiandrogen or GnRH pathways: cardiovascular/metabolic baseline, hormone levels as indicated, bone-density planning for longer-term androgen suppression, mood and VTE risk appraisal, and capacity/consent documentation. This is specialist work, not an ED reflex.[6][7][8]
Management — immediate public protection
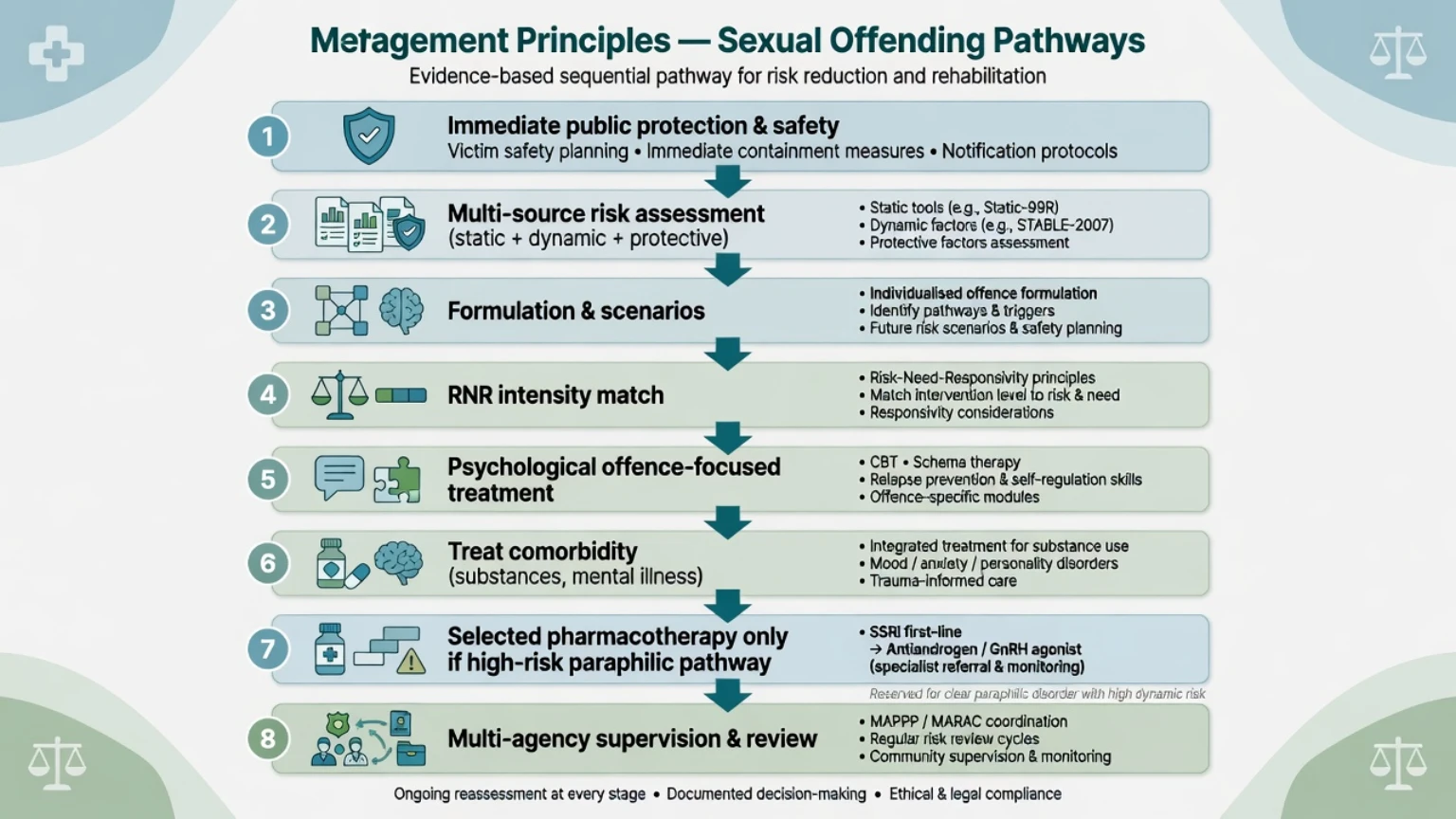
Immediate priorities (clinical, not theatrical):
- Restrict unsupervised access to potential victims; enforce no-contact conditions already in place.
- Environmental safety in ward/prison (observation, rooming, visitor rules).
- Treat acute psychiatric emergency (suicidality, psychosis, severe intoxication).
- Multi-agency notification principles when imminent risk to a named person or children exists under local law.
- Suspend leave or community privileges if dynamic risk has spiked (new access, substances, treatment dropout, new disclosures).[10][15]
Do not initiate antiandrogen/GnRH as emergency “chemical restraint” outside a specialist framework with consent/capacity process and monitoring.[6][7]
Management — definitive treatment principles
Risk–Need–Responsivity (RNR)
RNR remains the organisational logic for correctional and forensic rehabilitation intensity:
- Risk — more intensive services for higher risk.
- Need — target criminogenic needs (sexual and general), not only non-criminogenic distress.
- Responsivity — adapt to learning style, cognitive ability, culture, language, and engagement barriers.[17]
Real-world community supervision studies show incomplete but meaningful RNR application; examiners reward linking formulation to actionable needs, not inventory worship.[17]
Psychological interventions
Core evidence-informed psychological approach for people who have sexually offended is structured cognitive-behavioural, offence-focused work with relapse-prevention skills: identifying high-risk situations, challenging offence-supportive thinking, building intimacy and problem-solving skills, and strengthening self-management. Strengths-based engagement models (Good Lives Model principles) are often used as adjuncts to improve motivation without abandoning risk targets. Denial is managed as an engagement problem, not as a sole risk score item.[1][4]
Treat comorbidity (substance use, mood/anxiety disorders, psychosis, ADHD, personality pathology) as both clinical care and risk management when it impairs control, judgment, or supervision compliance.[4][17]
Pharmacological principles (selected pathways)
WFSBP guidelines for paraphilic disorders describe a stepped pharmacological approach for selected adult males with paraphilic disorders and elevated risk — not for all people with sexual offences and not for consensual adult atypical interests.[6][7]
Conceptual steps examiners expect (agent selection and dosing are specialist and regional; cite principles, not cookbook improvisation):
- SSRIs (e.g. high-serotonergic agents used for drive reduction / compulsive sexual behaviours in milder presentations) with standard psychiatric monitoring for mood, suicidality, and sexual side-effects.[6][8]
- Antiandrogens (e.g. cyproterone acetate or medroxyprogesterone where used regionally) for higher-risk persistent paraphilic disorders when psychological care alone is insufficient — baseline labs, liver function, metabolic parameters, and thromboembolic risk as relevant; informed consent emphasising side-effects (hypogonadism, metabolic effects, mood change).[6][7][8]
- GnRH analogues for highest-risk persistent pathways under specialist supervision with bone-density and endocrine monitoring plans.[7][8]
Pharmacotherapy goals are usually risk reduction and symptom control, not guaranteed “cure of interest”. Pair always with psychological work and supervision — medication is not a stand-alone public-protection plan.[7]
Multi-agency public protection
MAPPA-like multi-agency frameworks (UK-origin concept), registration/notification schemes, and ANZ public-protection arrangements are jurisdiction-specific. In exams: name the principle (information sharing, risk tiers, victim safety planning, review cycles) without inventing statutory section numbers. US civil commitment for sexually violent predators is a regional legal pathway — know it exists; do not export it as universal law.[15]
Specific subtypes and scenarios
- Preferential pedophilic contact pathway — high sexual deviance load; access control and specialised treatment central.
- Opportunistic antisocial pathway — general RNR needs (substances, impulsivity, criminal attitudes) may dominate.
- Online CSEM without known contact — heterogeneous contact risk; STABLE/ACUTE-class dynamic assessment still useful; do not assume zero contact risk or inevitable contact risk.[12]
- Intrafamilial — family systems, child-protection interfaces, no unsupervised contact rules.
- Female sexual offending — lower base rates; male-normed tools often poorly validated; formulation over tool worship.
- Youth — developmental sexual behaviour vs entrenched paraphilic pattern; different instruments; child protection paramount.
- Intellectual disability / autism — adapted communication, capacity, vulnerability to abuse and risk of boundary violations.
- Help-seeking non-offending pedophilic interest — ethics of prevention, confidentiality limits, non-stigmatising care without collusion.
Complications and pitfalls
- Conflating legal offence with psychiatric diagnosis.
- Assuming all child sexual offenders have pedophilic disorder.
- False precision from static scores; ignoring dynamic and protective change.[3][15]
- Colluding with secrecy that endangers children.
- Humiliating interviews that destroy engagement without improving risk data.
- Prescribing antiandrogens without baseline, monitoring, or consent process.[7]
- Pathologising LGBTQ+ identities or consensual adult kink.[18]
- Dual-role confusion (treating clinician vs court expert) and invented statute numbers.
- Cultural bias and Indigenous over-classification concerns — apply tools with equity caution.
Prognosis and disposition
Outcomes are heterogeneous. Many people with sexual offence histories do not sexually reoffend in the follow-up windows studied; elevated static plus dynamic load and weak protective factors justify more intensive supervision and treatment.[2][3]
Goals for persistent paraphilic preference often emphasise risk reduction, harm prevention, and functional desistance supports rather than eradication of interest. Disposition ladder: prison vs secure hospital vs community forensic vs general services with multi-agency oversight. Step-down when dynamic risk falls, protective factors strengthen, victim access is controlled, substances are managed, and engagement is sustained.[9][10]
Special populations
- Women — lower base rates; limited tool validation; individualised formulation.
- Youth / emerging adults — developmental caution; specialised youth frameworks.
- Older adults — aging may lower some actuarial risk; new late-life offences need neurocognitive assessment.
- Intellectual disability / autism — adapted assessment and treatment; capacity and vulnerability.
- Indigenous and minority populations — culturally safe practice; tool equity caution.
- Major mental illness — treat illness fully; formulate how symptoms interact with sexual risk (rarely the sole cause). Population-specific validation gaps mean formulation and multi-source assessment matter more than uncritical tool transfer; base-rate and equity caution apply throughout.[2][3][15]
Evidence, guidelines, and regional differences
- Predictors and tools: Hanson & Morton-Bourgon 2005 and 2009 metas; Static-99R rate studies; Mann/Hanson/Thornton dynamic factor proposals; STABLE/ACUTE validation including CSEM samples.[1][2][3][4][12]
- Theory: Seto motivation–facilitation model.[5]
- Protective factors: SAPROF sexual violence literature; dynamic/protective change and recidivism.[9][10]
- Pharmacotherapy: WFSBP 2010 and 2020; Assumpção review.[6][7][8]
- RNR practice reality: community supervision implementation literature.[17]
- Classification: ICD-11 paraphilic proposals.[18]
Public-protection, child-protection mandatory reporting, and forensic service pathways are state/territory and NZ jurisdiction-specific. Use principles: child safety primacy, multi-agency information sharing when lawful, least restrictive security consistent with risk. Do not invent Mental Health Act or Crimes Act section numbers in exams unless the stem supplies them. Registration/notification schemes exist in some jurisdictions — label as local law.[15]
Forensic report structure (sexual risk)
- Instructions and questions answered.
- Sources (and gaps).
- Background, index offence (clinically necessary detail only), and history.
- Mental state examination.
- Method (tools used, training limits, dates).
- Formulation: motivations, facilitators, protective factors.
- Risk scenarios (who/what/when/circumstances).
- Opinion and recommendations (treatment, supervision, victim-access rules).
- Limitations and reassessment triggers.[13][15]
Exam pearls
SEX-RISK (viva skeleton)
References
- [1]Hanson RK, Morton-Bourgon KE The characteristics of persistent sexual offenders: a meta-analysis of recidivism studies J Consult Clin Psychol, 2005.PMID 16392988
- [2]Hanson RK, Morton-Bourgon KE The accuracy of recidivism risk assessments for sexual offenders: a meta-analysis of 118 prediction studies Psychol Assess, 2009.PMID 19290762
- [3]Hanson RK, Thornton D, Helmus LM, et al. What Sexual Recidivism Rates Are Associated With Static-99R and Static-2002R Scores? Sex Abuse, 2016.PMID 25810478
- [4]Mann RE, Hanson RK, Thornton D Assessing risk for sexual recidivism: some proposals on the nature of psychologically meaningful risk factors Sex Abuse, 2010.PMID 20363981
- [5]Seto MC The Motivation-Facilitation Model of Sexual Offending Sex Abuse, 2019.PMID 28715948
- [6]Thibaut F, De La Barra F, Gordon H, et al. The World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the biological treatment of paraphilias World J Biol Psychiatry, 2010.PMID 20459370
- [7]Thibaut F, Cosyns P, Fedoroff JP, et al. The World Federation of Societies of Biological Psychiatry (WFSBP) 2020 guidelines for the pharmacological treatment of paraphilic disorders World J Biol Psychiatry, 2020.PMID 32452729
- [8]Assumpção AA, Garcia FD, Garcia HD, et al. Pharmacologic treatment of paraphilias Psychiatr Clin North Am, 2014.PMID 24877704
- [9]de Vries Robbé M, de Vogel V, Koster K, et al. Assessing protective factors for sexually violent offending with the SAPROF Sex Abuse, 2015.PMID 25210106
- [10]De Vries Robbé M, de Vogel V, Douglas KS, et al. Changes in dynamic risk and protective factors for violence during inpatient forensic psychiatric treatment: predicting reductions in postdischarge community recidivism Law Hum Behav, 2015.PMID 24933171
- [11]Cartwright JK, Desmarais SL, Hazel J, et al. Predictive validity of HCR-20, START, and static-99R assessments in predicting institutional aggression among sexual offenders Law Hum Behav, 2018.PMID 28857580
- [12]Babchishin KM, Dibayula S, McCulloch C, et al. ACUTE-2007 and STABLE-2007 predict recidivism for men adjudicated for child sexual exploitation material offending Law Hum Behav, 2023.PMID 37616071
- [13]Buchanan A Risk of violence by psychiatric patients: beyond the "actuarial versus clinical" assessment debate Psychiatr Serv, 2008.PMID 18245161
- [14]Fazel S, Singh JP, Doll H, et al. Use of risk assessment instruments to predict violence and antisocial behaviour in 73 samples involving 24 827 people: systematic review and meta-analysis BMJ, 2012.PMID 22833604
- [15]Large MM, Ryan CJ, Nielssen OB Helpful and unhelpful risk assessment practices Psychiatr Serv, 2010.PMID 20439381
- [16]Gregório Hertz P, Eher R, Etzler S, et al. Cross-Validation of the Revised Version of the Violence Risk Appraisal Guide (VRAG-R) in a Sample of Individuals Convicted of Sexual Offenses Sex Abuse, 2021.PMID 31010400
- [17]Dyck HL, Campbell MA, Wershler JL Real-world use of the risk-need-responsivity model and the level of service/case management inventory with community-supervised offenders Law Hum Behav, 2018.PMID 29620397
- [18]Krueger RB, Reed GM, First MB, et al. Proposals for Paraphilic Disorders in the International Classification of Diseases and Related Health Problems, Eleventh Revision (ICD-11) Arch Sex Behav, 2017.PMID 28210933