Psych · Forensic psychiatry — stalking and harassment
Stalking and harassment
Also known as Stalking risk assessment · Obsessional harassment · Mullen typology stalkers · RECON stalking typology · Cyberstalking forensic · Erotomania and stalking · Intimate partner stalking · Stalking Risk Profile · Harassment psychiatry · Victim impact stalking
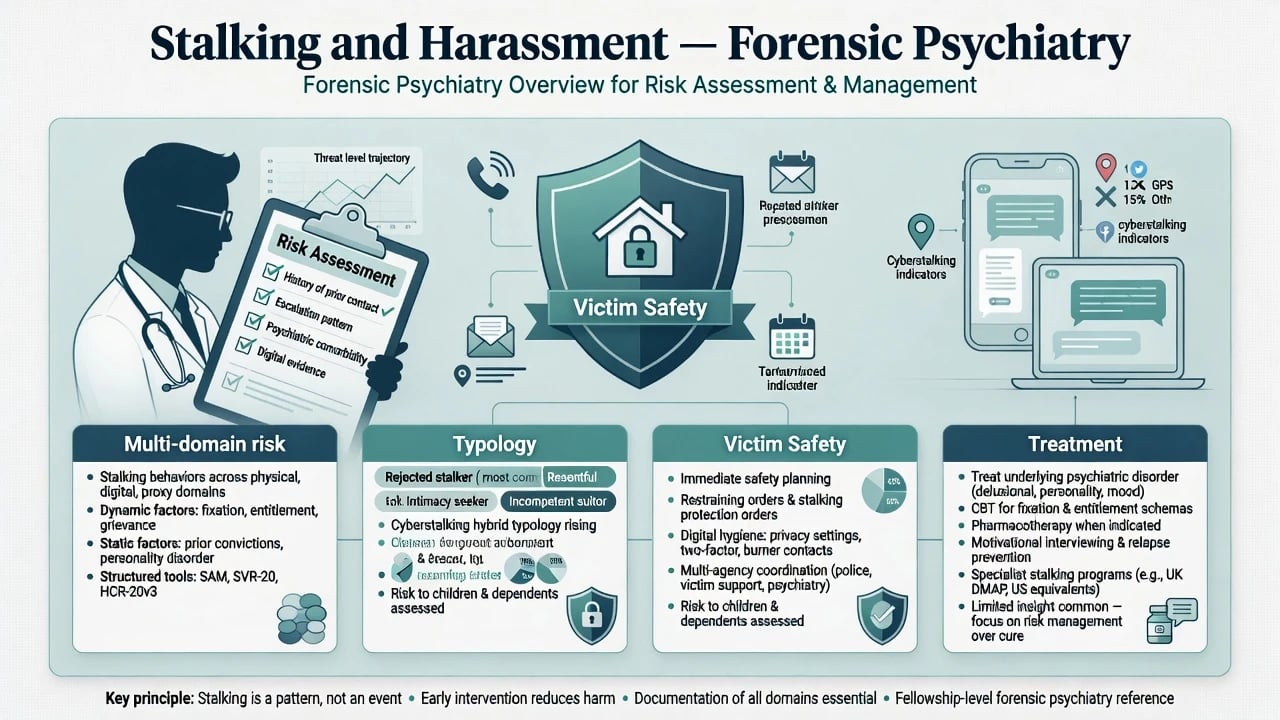
Exam-exhaustive fellowship reference on stalking and harassment for forensic psychiatry — legal vs clinical constructs; Mullen and RECON typologies; epidemiology and victim harm; multi-domain risk (violence, persistence, recurrence, psychosocial damage); multi-source assessment; management of stalker and victim safety; psychosis/erotomania interface; duty-to-protect principles; ethics. Non-sensational. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Stalking entered modern criminal codes late but is ancient as behaviour. For psychiatry, the key move is to stop treating it as a single diagnosis and start treating it as a course of conduct with heterogeneous motives, psychopathology, and risk profiles.[12][13]
Working clinical definition. A pattern of unwanted attention or intrusion directed at a person that is repeated and causes fear or significant distress. Jurisdictions differ on minimum number of acts, duration thresholds, intent requirements, and whether fear must be "reasonable". Teach principles; verify local harassment/stalking statutes and protection-order schemes — never invent section numbers.[12][3]
Related terms. Harassment is often the broader legal umbrella. Cyberstalking is technology-mediated pursuit (messages, tracking, spoofed identities, image-based abuse) assessed with the same multi-domain risk frame. Obsessional harassment is older North American clinical language still seen in the literature.[13][7]
What stalking is not. A single awkward message; mutual high-conflict contact without unilateral pursuit and fear; or a psychiatric diagnosis in DSM-5-TR/ICD-11. Mental illness may drive or facilitate stalking but is neither necessary nor sufficient.[1][17]
Classification — typologies examiners expect
Mullen clinical typology (exam gold)
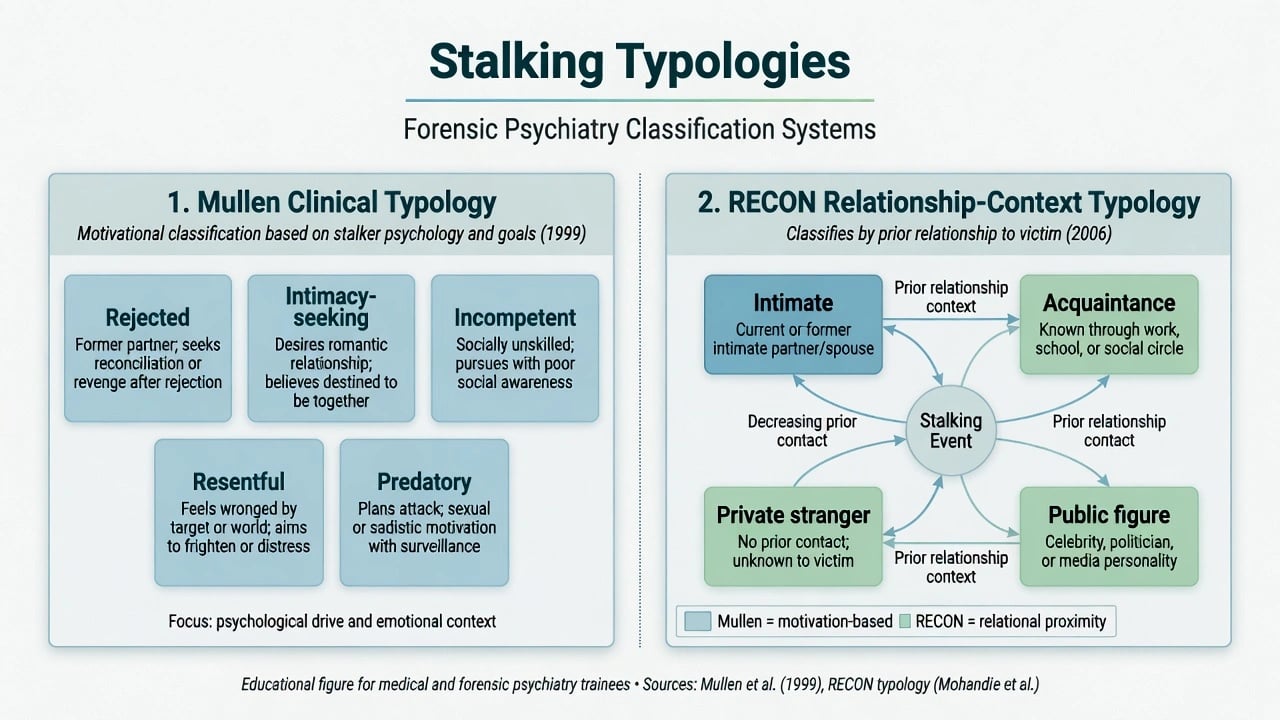
From a large clinical series, five motivational types organise formulation and risk hypotheses:[1]
| Type | Core motivation | Typical notes |
|---|---|---|
| Rejected | Reconciliation and/or revenge after relationship breakdown | Often ex-intimate; high violence association in literature |
| Intimacy-seeking | Belief that a relationship exists or is destined | Includes erotomanic presentations; can be highly persistent |
| Incompetent | Socially inept pursuit; misreads cues | Less organised psychopathology; still harmful |
| Resentful | Grievance and intimidation | Workplace/service/neighbour contexts common |
| Predatory | Preparation for sexual or other attack | Public-protection priority; sexual-violence interface |
Types can blend over time (e.g. rejected becomes resentful). Always state the dominant current motivation and evidence.[1][7]
RECON relationship-context typology
Mohandie and colleagues proposed RECON (relationship and context): Intimate, Acquaintance, Public figure, Private stranger. Prior intimacy strongly shapes base rates of approach and violence risk in large North American samples.[9]
Historical Zona types
Classic forensic categories — erotomanic, love-obsessional, simple-obsessional — remain examinable historical anchors; map them onto modern Mullen/RECON language in answers.[10]
- Rejected
- Intimacy-seeking
- Incompetent
- Resentful
- Predatory
- Drives treatment targets
- Intimate
- Acquaintance
- Public figure
- Private stranger
- Shapes access and base rates
- Course of conduct
- Fear/distress threshold
- Jurisdiction-specific
- Not a DSM diagnosis
Epidemiology and risk context
Community surveys show stalking is common, not exotic. In an Australian random community sample, almost one in four respondents (23.4%) reported repeated, fear-provoking unwanted behaviour; about one in ten described a protracted course spanning at least one month, with women about twice as likely as men to report victimisation.[3]
European community data similarly find substantial lifetime prevalence (around 11–12% in a German city sample) with measurable psychological impact among victims.[4]
Sex patterns. Men predominate as perpetrators in many forensic series; women who stalk are clinically important, often target people they know, and are not free of violence risk.[11][1]
Violence base rates. Violence occurs in a substantial minority of stalking episodes (estimates vary by sample and definition; higher in criminal-justice and ex-intimate series). Serious injury is less common than lower-level assault, threats, or property damage — but homicide, though rare, is the high-consequence tail examiners discuss without fatalism.[6][8][13]
Key empirical signal for violence. Across reviews and primary studies, a prior intimate relationship between stalker and victim is among the most consistent correlates of stalking violence — more useful than "psychosis present/absent" as a single flag.[6][8][9]
Persistence vs violence. Predictors of long campaigns are not identical to predictors of assault. Intimacy-seeking and certain psychotic presentations may show high persistence with lower relative violence rates than rejected ex-intimate stalkers — still severe for victim harm.[5][1][17]
Mechanisms and pathophysiology
Motivational engines
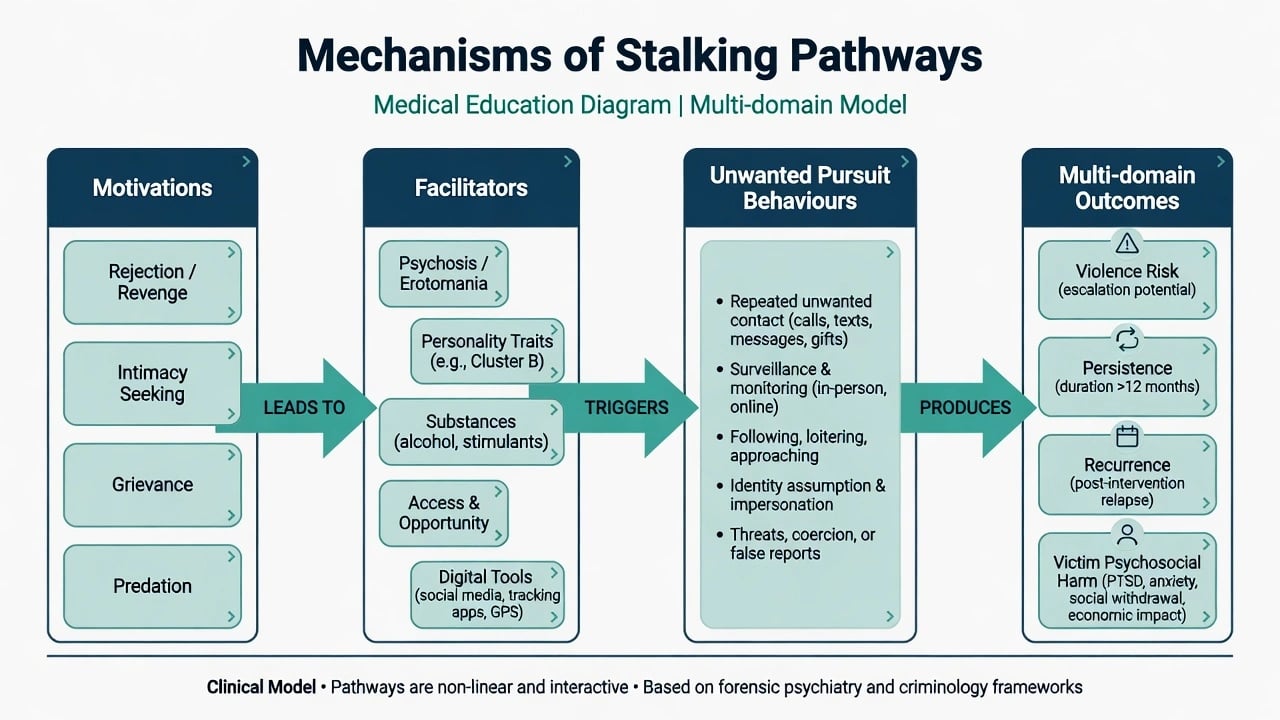
- Rejection pathway: attachment injury, entitlement, revenge, hope of reunion.
- Intimacy pathway: erotomanic certainty or non-delusional fantasy of destined love.
- Incompetence pathway: poor social cognition, loneliness, misread reciprocal interest.
- Resentment pathway: grievance, humiliation, desire to intimidate or "teach a lesson".
- Predatory pathway: instrumental surveillance for sexual or other attack.[1][12]
Facilitators
Psychosis (erotomania, persecutory or jealous delusions), personality pathology (narcissistic injury, borderline abandonment rage, antisocial disregard), substance intoxication, social isolation, and access (shared children, workplace, digital traces) facilitate continuation.[17][7][1]
Psychotic and nonpsychotic stalkers differ in clinical profile; psychosis is enriched in some intimacy-seeking stranger pursuits but is not the majority driver of all community stalking.[17][1]
Victim harm mechanisms
Pathé and Mullen documented major social and psychological damage: anxiety, depression, post-traumatic symptoms, lifestyle restriction, and occupational disruption. Community association studies link stalking victimisation with elevated psychiatric morbidity.[2][14]
Reinforcement loops
Intermittent contact, ambiguous responses, algorithmic social-media cues, delayed legal processes, and rumination maintain pursuit. Legal "wins" for the victim can paradoxically escalate some rejected/resentful campaigns — plan for post-order risk, not only pre-order risk.[7][8]
Clinical presentation
Forensic stems. Court-ordered assessment after breaches of protection orders; community patient who discloses following an ex-partner; workplace threat assessment; public-figure fixation; clinician stalked by a former patient.[7][12]
Stalker interview cues. Minimisation ("just trying to talk"); justificatory narratives; calm erotomanic certainty; grievance dossiers; detailed knowledge of victim routines; dual substance use; prior intimate-partner violence.[1][6]
Victim presentation. Hypervigilance, sleep loss, depression, PTSD symptoms, shame, under-reporting, pressure to "sort it privately", financial costs of relocation/security.[2][14]
Cyber pattern. Multiple accounts, location tracking, workplace email floods, non-consensual image threats — same multi-domain formulation with technology as the means, not a separate disease.[13][7]
False victimisation. Rare but recognised presentations of people who falsely claim to be stalked; require careful multi-source review, not cynical default.[18]
Differential diagnosis
Discriminators include patterned stalking versus isolated unwanted contact or mutual conflict; erotomanic delusional disorder or schizophrenia-spectrum pursuit versus non-psychotic intimacy-seeking; morbid jealousy surveillance of a current partner versus post-separation rejected stalking (overlap common); autism or intellectual disability social misreading with persistence versus intentional fear campaign (formulate both disability and risk — disability is not automatic excuse or automatic high risk); and genuine victimisation versus false claims after multi-source review.[10][17][18][1]
Assessment
Multi-source is non-negotiable
Interview alone under-detects. Use victim statements, police summaries, order/breach history, digital evidence provided lawfully, prior mental health notes, collateral, and MSE. Do not rely on the stalker's self-report of "no contact".[7][15]
Multi-domain risk framework (Mullen group)
Risks in stalking are not confined to violence. Structure assessment across violence (assault, sexual assault, homicide tail), persistence (duration and intensity of the campaign), recurrence (new campaign after cessation, same or new victim), psychosocial damage to the victim even without physical assault, and stalker self-harm or suicide risk especially after arrest, shame, or failed reunion.[7][8]
Practical domains to cover
- Relationship context (RECON) and Mullen type
- Chronology of behaviours (including cyber)
- Threats, weapons, prior IPV/violence
- Access map (home, work, school, children, online)
- Psychopathology and substances
- Response to prior legal interventions
- Victim vulnerability and support
- Protective factors (new goals, treatment engagement, supervised structure, no access)[7][15][6]
Structured tools
The Stalking Risk Profile (SRP) operationalises multi-domain, typology-informed assessment; reliability and predictive validity data support structured use as an aid, not a crystal ball.[15][7]
General violence instruments (e.g. HCR-20 class) may inform co-occurring violence risk but do not replace stalking-specific attention to persistence, recurrence, and victim psychosocial harm. Group-level predictive accuracy of violence tools is only moderate — communicate scenarios, not destiny labels.[21][20][22]
Investigations and information gathering
- Primary: behaviour chronology and legal documents.
- Toxicology when substances facilitate approaches.
- Organic work-up for new psychosis or cognitive change as clinically indicated.
- Personality/psychopathy measures only as formulation adjuncts.
- Lawful multi-agency information sharing when public protection requires it — local policy, not invented statutes.[7][15]
Acute / emergency management
Immediate priorities. Secure the interview setting if the stalker is present; reduce victim access now; do not coach "one last meeting to explain"; activate police/protection pathways per local process when imminence is high; treat acute psychosis/mania/intoxication driving pursuit; document.[7][19]
Duty-to-protect interface. When a patient poses a serious risk of violence to an identifiable third party, confidentiality is not absolute. Appelbaum's assess → select protective course → implement and document model applies. Protective steps may include hospitalisation, intensified treatment, weapons pathways, warning/police notification — jurisdiction-specific thresholds; never export one state's case name as universal statute.[19][7]
Clinician as target. Use institutional security, transfer of care where dual-role is compromised, documentation, and organisational support — personal bravery is not a risk plan.[7]
Definitive management
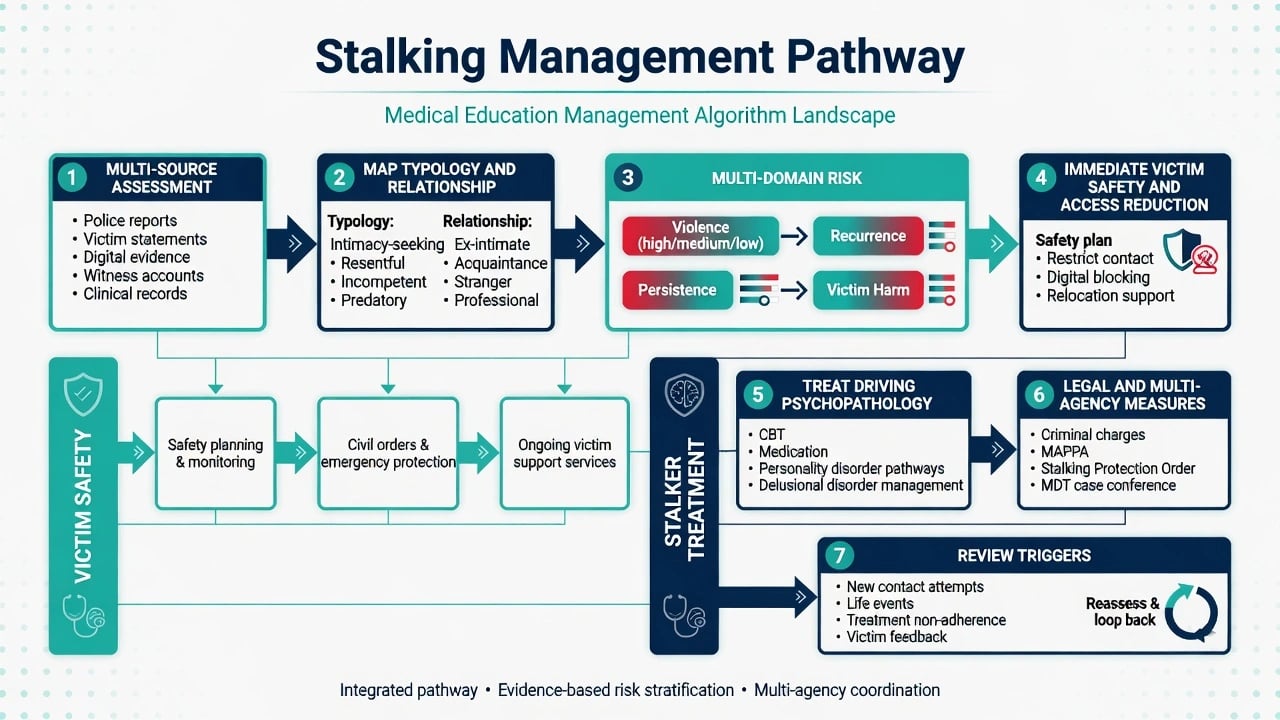
Parallel tracks
Track A — Victim safety. Access reduction; workplace/home security principles; no-contact enforcement; protection-order processes (local); support for mental health sequelae; avoid victim-blaming "digital hygiene only" frames.[2][7]
Track B — Stalker treatment and control. Match intensity to multi-domain risk; treat driving illness; psychological work on beliefs and emotion regulation; substance treatment; legal sanctions and supervision as external control.[4][16]
By typology (high-yield)
- Rejected: emotion regulation, grief/revenge work, substance care, strict no-contact; high vigilance for violence after setbacks.[1][6]
- Intimacy-seeking / erotomanic: antipsychotic treatment when psychotic; hospital when risk/access high; do not collude with delusional "relationship"; persistence planning.[1][10][17]
- Incompetent: social skills, alternative attachment goals, clear legal boundaries.[1]
- Resentful: address legitimate grievances via proper channels where safe; firm consequences for intrusion; do not reward contact.[1][7]
- Predatory: public protection and sexual-violence risk pathways; least "therapeutic only" posture.[1][7]
Psychological treatment evidence signal
A randomised controlled study of dialectical behaviour therapy (DBT) for people who stalk found signals for reduced renewed stalking behaviour and improvements in impulsivity/anger-related domains relative to control — promising for selected non-psychotic emotion-dysregulation pathways, not a universal protocol for all types.[16]
Pharmacotherapy principles
- Treat psychosis driving pursuit with antipsychotics per usual standards (agent choice individualised; monitor metabolic/EPS/QTc as for any antipsychotic pathway) — the forensic goal is risk reduction via illness control, not "chemical restraint" theatre.[17][1]
- Treat comorbid depression, anxiety, ADHD, or substance use disorders on their merits.
- There is no first-line "anti-stalking pill" for non-psychotic rejected stalking.
Review triggers
New contact or digital escalation; order breach; substance relapse; relationship-adjacent triggers (court dates, anniversaries); treatment dropout; new weapons access; victim relocation failure; stalker suicidality after legal loss.[7][15]
Subtypes and scenarios
- Cyberstalking — same typology/risk frame; technology as means.
- Public-figure — lower average approach violence than intimate samples in RECON data, but high psychosocial and rare catastrophic tails; specialised threat assessment principles.[9]
- Health professional victims — institutional response; boundary and security.
- Women who stalk — often known victims; assess violence seriously.[11]
- Youth — developmental caution; school safety interfaces.
- False victimisation — multi-source verification without automatic disbelief of all victims.[18]
Complications and pitfalls
- Assuming all stalkers are psychotic (most community cases are not)
- Equating "no assault yet" with low harm
- Using only general violence tools and missing persistence/recurrence
- Colluding with justificatory narratives
- Victim-blaming and "just block them" as sole plan
- Encouraging contact to "calm them down"
- Inventing harassment statute section numbers
- Ignoring stalker suicide risk after legal consequences
- False precision from a single risk label without scenarios
Prognosis and disposition
Outcomes are heterogeneous. Many campaigns end when access is removed, legal constraints bite, driving psychopathology is treated, and alternative goals emerge. Intimacy-seeking psychotic and some rejected patterns may be highly persistent or recurrent despite interventions — plan long enough follow-up.[5][7][15]
Disposition ladder. Community general or forensic services with conditions → voluntary or compulsory inpatient care when mental illness plus risk criteria met under local law → criminal justice custody when indicated. Step-down only after multi-domain reassessment, not after a calm interview alone.[7][19]
Special populations
- Women who stalk — distinct patterns; violence not rare.[11]
- Adolescents — developmental formulation; education settings.
- Intellectual disability / autism — adapted communication; capacity; risk still assessed.
- Older adults — late-life erotomania; cognitive change; elder-victim vulnerability.
- Indigenous and cultural minority contexts — culturally safe practice without minimising fear or over-pathologising.
- Clinician victims — organisational duty of care.
Evidence and guidelines
Anchor viva answers to: Mullen typology clinical study; Pathé victim impact; Purcell prevalence and morbidity; Dressing European prevalence; McEwan persistence and violence papers; Mullen multi-domain risk framework; SRP reliability work; Mohandie RECON; Zona and Kienlen historical comparisons; Rosenfeld DBT RCT; Sheridan review; Appelbaum duty-to-protect; Large/Fazel risk-communication humility.[1][2][3][6][7][15][16][20]
Regional deltas. ANZ candidates use local stalking/harassment and family-violence frameworks plus RANZCP ethics (rare confidentiality breach for safety of patient or others) as principles. UK candidates may reference Protection from Harassment-type frameworks by name only. US candidates note state variation in criminal definitions and Tarasoff-type duties. Never invent section numbers in exams or reports.[19][12]
Exam pearls
Stalking is a behaviour/legal pattern — diagnosis is optional for recognition and essential for treatment targeting when illness drives pursuit. Use Mullen five types plus RECON relationship context as the examiner skeleton. Multi-domain risk covers violence, persistence, recurrence, victim psychosocial harm, and stalker suicide. Prior intimacy is the standout violence signal; psychosis more often signals persistence than universal violence. Run parallel tracks for victim safety and stalker treatment. Duty to protect may apply (Appelbaum three steps; local law). Prefer scenarios and management plans over a lone medium-risk label. Keep language clinical and non-sensational; never fabricate statutes.[1][7][6][19][20]
References
- [1]Mullen PE, Pathé M, Purcell R, et al. Study of stalkers Am J Psychiatry, 1999.PMID 10450267
- [2]Pathé M, Mullen PE The impact of stalkers on their victims Br J Psychiatry, 1997.PMID 9068768
- [3]Purcell R, Pathé M, Mullen PE The prevalence and nature of stalking in the Australian community Aust N Z J Psychiatry, 2002.PMID 11929447
- [4]Dressing H, Kuehner C, Gass P Lifetime prevalence and impact of stalking in a European population: epidemiological data from a middle-sized German city Br J Psychiatry, 2005.PMID 16055829
- [5]McEwan TE, Mullen PE, MacKenzie R A study of the predictors of persistence in stalking situations Law Hum Behav, 2009.PMID 18626757
- [6]McEwan TE, Mullen PE, MacKenzie RD, et al. Violence in stalking situations Psychol Med, 2009.PMID 19215627
- [7]Mullen PE, Mackenzie R, Ogloff JR, et al. Assessing and managing the risks in the stalking situation J Am Acad Psychiatry Law, 2006.PMID 17185471
- [8]McEwan T, Mullen PE, Purcell R Identifying risk factors in stalking: a review of current research Int J Law Psychiatry, 2007.PMID 17157379
- [9]Mohandie K, Meloy JR, McGowan MG, et al. The RECON typology of stalking: reliability and validity based upon a large sample of North American stalkers J Forensic Sci, 2006.PMID 16423242
- [10]Zona MA, Sharma KK, Lane J A comparative study of erotomanic and obsessional subjects in a forensic sample J Forensic Sci, 1993.PMID 8355005
- [11]Purcell R, Pathé M, Mullen PE A study of women who stalk Am J Psychiatry, 2001.PMID 11729025
- [12]Mullen PE, Pathé M, Purcell R Stalking: new constructions of human behaviour Aust N Z J Psychiatry, 2001.PMID 11270463
- [13]Sheridan LP, Blaauw E, Davies GM Stalking: knowns and unknowns Trauma Violence Abuse, 2003.PMID 14697120
- [14]Purcell R, Pathé M, Mullen PE Association between stalking victimisation and psychiatric morbidity in a random community sample Br J Psychiatry, 2005.PMID 16260815
- [15]McEwan TE, Shea DE, Daffern M, et al. The Reliability and Predictive Validity of the Stalking Risk Profile Assessment, 2018.PMID 27305931
- [16]Rosenfeld B, Galietta M, Foellmi M, et al. Dialectical behavior therapy (DBT) for the treatment of stalking offenders: A randomized controlled study Law Hum Behav, 2019.PMID 31204832
- [17]Kienlen KK, Birmingham DL, Solberg KB, et al. A comparative study of psychotic and nonpsychotic stalking J Am Acad Psychiatry Law, 1997.PMID 9323658
- [18]Pathé M, Mullen PE, Purcell R Stalking: false claims of victimisation Br J Psychiatry, 1999.PMID 10211173
- [19]Appelbaum PS Tarasoff and the clinician: problems in fulfilling the duty to protect Am J Psychiatry, 1985.PMID 3976915
- [20]Large MM, Ryan CJ, Nielssen OB Helpful and unhelpful risk assessment practices Psychiatr Serv, 2010.PMID 20439381
- [21]Fazel S, Singh JP, Doll H, et al. Use of risk assessment instruments to predict violence and antisocial behaviour in 73 samples involving 24 827 people: systematic review and meta-analysis BMJ, 2012.PMID 22833604
- [22]Buchanan A Risk of violence by psychiatric patients: beyond the "actuarial versus clinical" assessment debate Psychiatr Serv, 2008.PMID 18245161