Psych · Forensic psychiatry — therapeutic security
Therapeutic security and secure care levels
Also known as Therapeutic security · Secure care levels · High medium low secure · Forensic secure hospital · Relational security · Physical procedural relational security · DUNDRUM triage security · Stratified forensic care · Forensic mental health security
Exam-exhaustive fellowship reference on therapeutic security and secure care levels — physical, procedural and relational domains; high/medium/low secure definitions; DUNDRUM-style triage and recovery; relational security practice; step-up/step-down; long-stay; discharge outcomes. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Therapeutic security is not a synonym for locks. It is the clinical system that makes forensic treatment possible: containing risk of serious harm to others (and, secondarily, managing abscond/escape) while delivering assessment, medication, psychological programmes, and rehabilitation. The dual purpose of secure forensic hospitals is treatment of mental disorder and public protection through risk reduction — not punishment.[1][11][18]
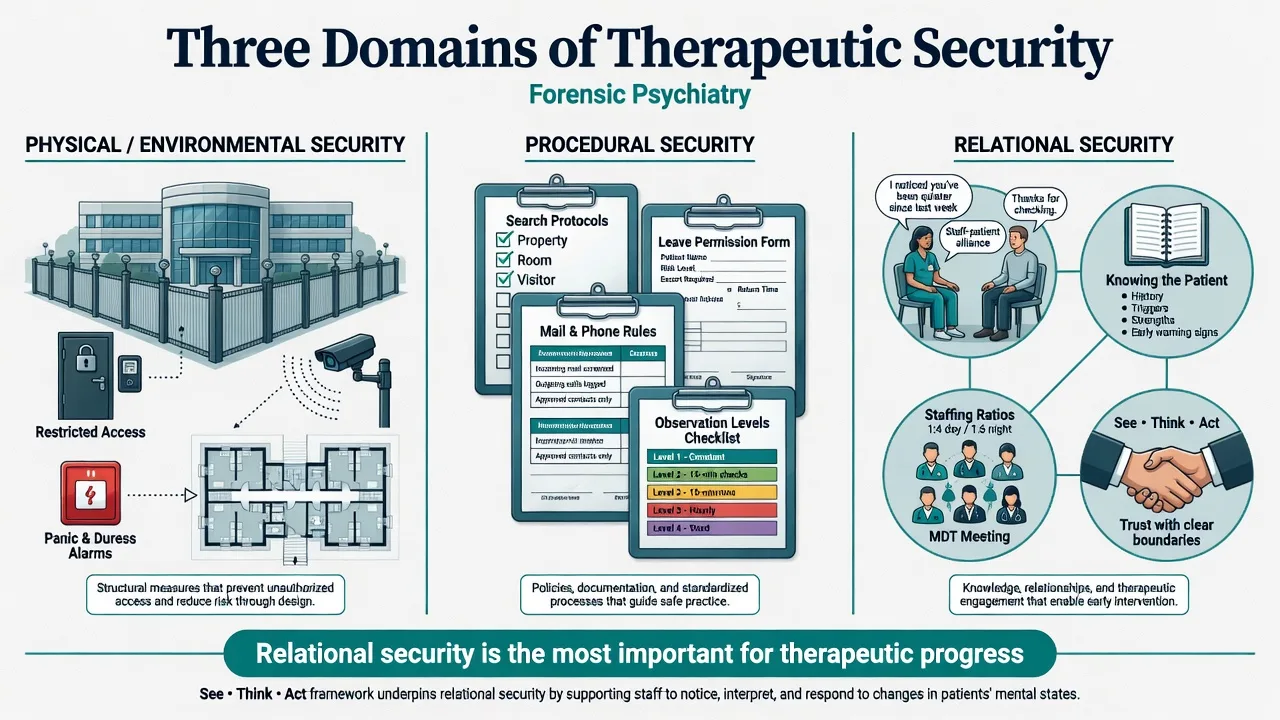
The classical teaching model (Kennedy) stratifies services by security and maps each unit by three domains:
- Physical / environmental security — buildings, perimeter, observation systems, alarms, design that limits weapons and escape.
- Procedural security — policies and practices that control risk-critical behaviours: leave, visitors, mail/phone, searches, money, contraband, observation levels, governance.
- Relational security — the quality of staff knowledge of the patient, therapeutic alliance with firm boundaries, staffing skill-mix and continuity, and culture of noticing change early.[1][6][8]
Relational security is repeatedly emphasised as the most important element for therapeutic progress. Physical and procedural measures without relational depth produce a prison-like shell that fails to predict deterioration or enable recovery.[6][7][8]
This topic is distinct from violence-risk SPJ tools as sole content (HCR-20 depth lives in the risk-assessment leaf), prison in-reach care, civil Mental Health Act principles, and episode-level seclusion/restraint algorithms — though all interface with secure placement decisions.[3][16][20]
Classification — three domains and secure care levels
Physical (environmental) security
Perimeter strength, building fabric, controlled exits, CCTV and alarms, room design, and observation sight-lines. Physical security must match the declared care level: high secure environments are designed so escape is not practicable; medium secure environments prevent escape; low secure environments impede escape. Physical measures are necessary but never sufficient alone.[1][13]
Procedural security
Written and lived policies that structure risk: who may leave and under what escort, search regimes, item and substance control, communication monitoring where lawful, visitor rules, financial controls, and incident/governance processes. Procedural security is how services operationalise risk management day to day.[1][5]
Relational security
Staff–patient knowledge and trust with professional boundaries; consistent MDT formulation; noticing subtle changes in mental state, alliances, and peer dynamics; adequate ratios and skilled teams. Tools such as the See Think Act (STA) framework and scale operationalise relational security culture for measurement and team reflection.[6][7][8]
- Perimeter and building
- Alarms and observation design
- Limits opportunity for escape/weapons
- Necessary shell, not therapy itself
- Leave and visitor rules
- Search and contraband control
- Observation levels and governance
- Policy that structures risk behaviour
- Know the patient deeply
- Alliance with firm boundaries
- Early detection of change
- Most important for therapeutic progress
Stratified secure care levels (exam definitions)
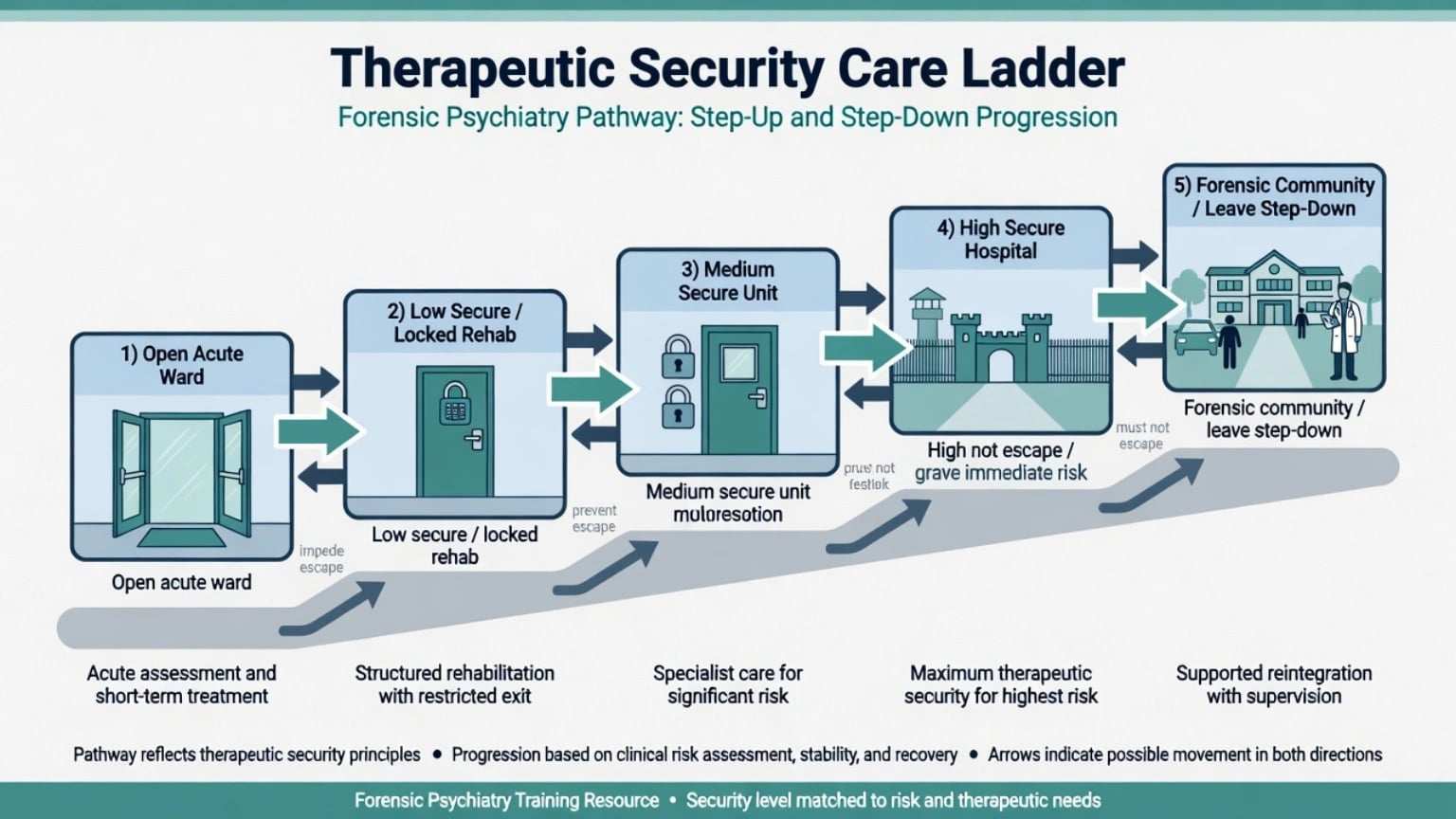
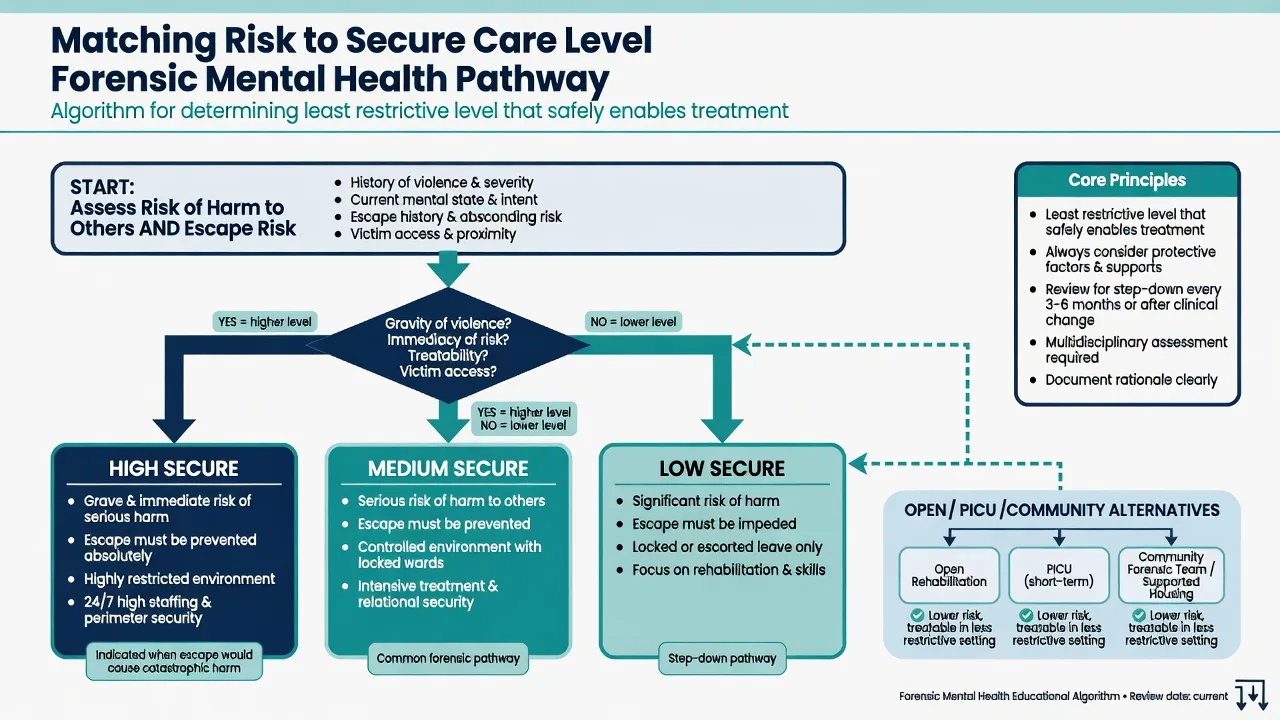
Stratified secure care maps risk of harm and escape principles onto high, medium, and low inpatient security plus open and community forensic steps. High secure addresses grave and immediate risk where escape must not be possible; medium addresses serious risk with escape prevented; low addresses significant risk with escape impeded. These are principles, not universal statutes — ANZ regional services may integrate levels without a separate high-secure estate.[1][13][18]
| Level | Risk principle (teachable wording) | Escape principle | Typical role |
|---|---|---|---|
| High secure | Grave and immediate risk to the public | Must not be able to escape | National/specialist high secure hospitals |
| Medium secure | Serious risk of harm to others | Escape must be prevented | Regional medium secure units |
| Low secure | Significant risk of harm to others | Escape must be impeded | Local low secure / locked forensic rehab |
| Open / step-down | Residual forensic needs at lower containment | Standard hospital security | Open forensic or rehab wards |
| Forensic community | Ongoing risk in community living | N/A — supervision and liaison | Outreach / FOLS-style aftercare |
Adjacent settings examiners love to confuse
- PICU — high nursing intensity for short-lived acute disturbance; not automatically medium/high forensic security.
- Prison healthcare wing — custody healthcare; transfer to hospital when needs exceed prison capacity (principles only; pathways jurisdiction-specific).
- Civil locked rehab — may impede abscond without forensic medium-secure perimeter standards.[5][13][18]
Epidemiology and system facts
Secure forensic inpatient care is high-cost, low-volume. Pathways include prison transfers, court-related admissions, step-up from open/low secure, and step-down from higher security.[5][18]
Long-stay is a core exam fact. In English high and medium secure samples, roughly one-fifth meet research long-stay definitions (commonly ≥10 years in high secure, ≥5 years in medium secure, or combined thresholds such as 15 years across levels). Long-stay groups share complex clinical and pathway features across high and medium settings.[9][10]
Length of stay in medium secure care is multi-factorial: offence seriousness, treatment resistance, personality pathology, substance issues, institutional culture, and discharge barriers (housing, aftercare, legal constraints) matter as much as admission risk alone.[19]
Australian complete-cohort forensic mapping shows patients stratified across security and recovery stages with heterogeneous risk/need profiles — reinforcing that secure care is a system, not a single ward type.[18]
Aotearoa New Zealand work examining putative high-secure need within a regional medium-secure service illustrates that not every high-risk patient requires high-secure fabric if therapeutic security (especially relational and procedural strength) is well configured — placement is about matching, not maximising locks.[13]
Mechanisms — how security enables (or blocks) recovery
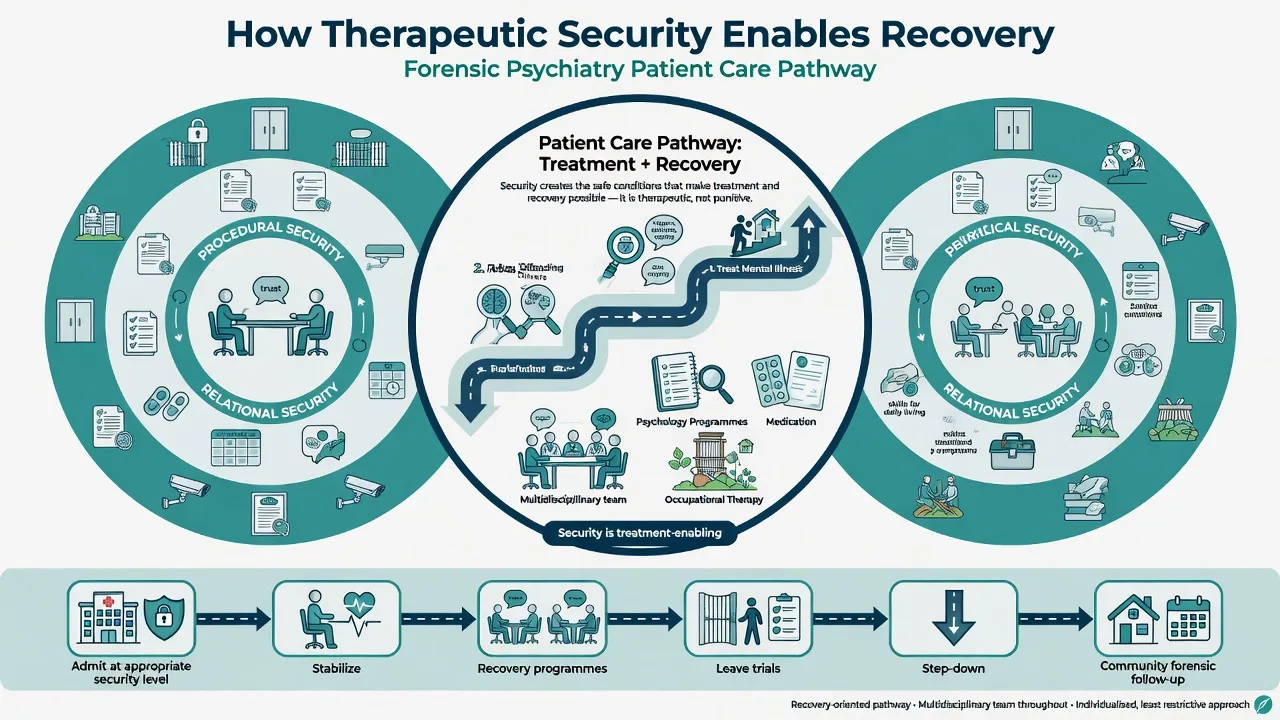
Risk in secure care is a product of imported vulnerability (prior violence, traits, illness history), clinical state (psychosis, mania, intoxication, despair), and opportunity (weapons, victim access, leave, peer dynamics). Physical and procedural measures reduce opportunity; relational security and treatment change clinical state and early detection.[3][4]
Prospective forensic work links structured recovery and programme-completion measures (DUNDRUM-3/4) and protective-factor thinking to institutional outcomes including violence/self-harm susceptibility and moves between security levels — security need is not static.[3][4][15]
Patient qualitative work on long-stay describes demoralisation, stalled hope, and the felt permanence of high containment when pathways out are unclear — clinical systems must counter this with active recovery planning, not passive warehousing.[17]
Clinical presentation and assessment
Who needs secure care (conceptual)
Candidates typically present with mental disorder plus serious harm-to-others risk that cannot be safely managed at a lower level: serious violence, sexual or fire-setting risk linked to mental disorder, or prison transfers requiring hospital-level care under security. Predominant self-harm without serious risk to others is usually not a medium/high secure indication alone (local exceptions may exist for custody-transfer constraints — principles only).[1][5][20]
Structured placement assessment
Fellowship standard is structured professional judgement, not a single score or gut feel. Systematic review evidence supports SPJ approaches for adult secure admission assessment processes, while warning that tools must be used as intended — multi-source history, criteria mapping, and documented reasoning.[20]
DUNDRUM toolkit (conceptual roles — teach the functions): DUNDRUM-1 triages level of therapeutic security needed; DUNDRUM-2 rates urgency/priority for admission from waiting lists; DUNDRUM-3 tracks programme completion; DUNDRUM-4 tracks recovery readiness for move-through and community transition. These SPJ roles are the validated teaching skeleton of the DUNDRUM suite.[1][2][3]
Validation studies support use for triage security and for predicting moves between levels when combined with clinical SPJ and HCR-20-style risk assessment; UK forensic services have validated toolkit use in referral triage pathways.[1][2][3][5]
Assessment sources: index offence and pattern of prior violence; escape/abscond history; victim profile and access; substances; mental state and insight; prison/hospital behaviour; prior leave outcomes; treatability and engagement; legal status principles (do not invent section numbers).[5][18][20]
Differential decisions examiners test
| Decision | Prefer higher security when… | Prefer lower / alternative when… |
|---|---|---|
| High vs medium | Grave + immediate public risk; escape must be impossible | Serious but not grave/immediate; medium can prevent escape |
| Medium vs low | Serious harm risk needing escape prevention | Significant risk manageable if escape impeded |
| Secure vs PICU | Enduring forensic risk + mental disorder needing secure pathway | Brief acute disturbance without forensic security need |
| Hospital vs prison health | Needs exceed prison clinical capacity | Can be safely treated in custody with equivalence of care |
| Stay vs step-down | Unstable dynamic risk, incomplete programmes, failed leave | Stabilised illness, recovery metrics, leave success, aftercare ready |
Management — placement, treatment, step-through
Acute / emergency frame
If imminent serious violence or escape risk exceeds the unit's physical/procedural capacity: immediate containment within lawful local procedures, medical review for organic contributors, and emergency step-up consideration. Restrictive practices (seclusion, restraint, enhanced observation) must be necessary, proportionate, and time-limited — Kennedy's DRILL framework conceptualises restriction, intrusion, and liberty ladders for evaluating proportionality in forensic settings.[16]
Definitive care at the right level
- Place at least restrictive secure level that safely enables treatment.[1][3]
- Treat the mental disorder with evidence-based psychopharmacology and psychological care (doses and agents follow general psychiatry standards with secure-setting monitoring).
- Deliver offence-related and recovery programmes (violence, sexual, fire-setting, substance, social cognition as indicated) — progress tracked with programme/recovery measures.[3][4]
- Build relational security — STA culture: see early signs, think formulation, act consistently as a team.[6][7][8]
- Leave ladder — graded community exposure under procedural controls as recovery allows.
- Step-down high → medium → low → open → forensic community when security need falls; document the evidence (dynamic risk, leave success, programme completion).[3][15]
- Aftercare — forensic or general community follow-up intensity matched to residual risk; aftercare model influences outcomes.[11][14]
Subtypes and high-yield scenarios
- Prison-to-hospital transfer — untreated psychosis or high self-harm/violence needs exceeding prison care; place by security need, not by sentence length alone.[5][18]
- High-to-medium step-down — recovery and risk metrics guide moves; high secure services use structured outcome pathways toward medium secure.[15]
- Failed leave / abscond — temporary procedural tightening and security review; not automatic permanent high secure branding.
- Women's secure pathways — smaller estate, higher self-harm comorbidity in many series; avoid defaulting women to over-secure beds for self-harm alone.
- Intellectual disability — long-stay comparisons show distinct needs; security matching must include communication and developmental supports.[9]
- Regional ANZ medium-secure services — integrated models may manage high-need patients without separate high-secure campuses when therapeutic security is strong.[13][18]
Complications and pitfalls
- Over-secure placement (rights, cost, demoralisation, delayed recovery).[9][17]
- Under-secure placement (escape, serious harm).
- Confusing restrictive practices with secure care level.
- Neglecting relational security while polishing the perimeter.[6]
- Treating security level as permanent identity rather than dynamic need.[3]
- Inventing Mental Health Act or Ministry of Justice section numbers in viva.
- Discharge without forensic aftercare planning.[11][14]
Prognosis and disposition
Many patients move down the security ladder with treatment; a substantial minority become long-stay and need dedicated pathway redesign rather than endless "another year".[9][10][15]
Meta-analysis of outcomes after discharge from secure psychiatric hospitals shows material rates of reoffending, readmission, and excess mortality (including suicide). Absolute reoffending rates vary by era and sample; the exam point is humility plus aftercare, not claims of zero risk.[11]
Clinical prediction rules such as FoVOx estimate group-level risk of violent crime after discharge from secure hospitals — useful for communication and resource planning, not individual certainty.[12]
Comparative work suggests forensic specialist aftercare can influence post-discharge trajectories relative to generic pathways; design follow-up intensity deliberately.[14]
Disposition ladder for viva: High secure → medium secure → low secure → open forensic/rehab → forensic community outreach, with parallel civil pathways when residual risk no longer requires forensic fabric.[3][15][18]
Special populations
- Women — pathway equity; avoid over-security for self-harm without other-directed risk.
- Youth transitioning to adult secure — developmental framing; avoid adult high secure by default.
- Older forensic patients — frailty, cognition, victim vulnerability, and medical comorbidity reshape physical/procedural needs.
- ID/autism — adapted programmes; long-stay risk; specialist secure ID services where available.[9]
- Indigenous and CALD patients — cultural safety within secure environments; family engagement without compromising procedural security.
- ANZ regional models — map local high/medium/low equivalents honestly; do not import English three-hospital high-secure geography as universal fact.[13][18]
Evidence and regional deltas
| Anchor | Take-home |
|---|---|
| DUNDRUM-1/2 validation | SPJ triage of security level and admission urgency |
| Davoren move-through study | Programme completion + recovery + HCR-20 linked to security moves |
| Freestone UK toolkit | DUNDRUM usable in real referral pathways |
| Chester / STA validations | Relational security is measurable, not mystical |
| Völlm / Hare Duke long-stay | ~1/5 long-stay; system problem not anecdote |
| Fazel discharge meta | Non-zero reoffending, readmission, mortality after discharge |
| FoVOx | Group-level discharge violence prediction |
| Kennedy DRILL | Proportionality of restrictive practices |
| Jewell NZ / Adams Australia | Regional forensic systems and high-need matching |
| Bowden SPJ review | Admission assessment should be structured |
Exam pearls
- Three domains: physical + procedural + relational (most important for therapy).[6]
- High / medium / low: grave+immediate / serious / significant — paired with escape impossible / prevented / impeded.[1]
- Least restrictive level that still enables safe treatment.[3]
- DUNDRUM: security triage (1), urgency (2), programmes (3), recovery (4).[1][2][3]
- Security level is dynamic — always plan step-down criteria.[2][15]
- Long-stay ≈ one in five in English high/medium research samples.[9][10]
- Discharge ≠ zero risk — aftercare and dynamic factors matter.[11][14]
- Never invent statute section numbers; name principles.
SECURE ladder
References
- [1]Flynn G, O'Neill C, McInerney C, et al. The DUNDRUM-1 structured professional judgment for triage to appropriate levels of therapeutic security: retrospective-cohort validation study BMC Psychiatry, 2011.PMID 21410967
- [2]Flynn G, O'Neill C, Kennedy HG. DUNDRUM-2: Prospective validation of a structured professional judgment instrument assessing priority for admission from the waiting list for a forensic mental health hospital BMC Res Notes, 2011.PMID 21722397
- [3]Davoren M, O'Dwyer S, Abidin Z, et al. Prospective in-patient cohort study of moves between levels of therapeutic security: the DUNDRUM-1 triage security, DUNDRUM-3 programme completion and DUNDRUM-4 recovery scales and the HCR-20 BMC Psychiatry, 2012.PMID 22794187
- [4]Abidin Z, Davoren M, Naughton L, et al. Susceptibility (risk and protective) factors for in-patient violence and self-harm: prospective study of structured professional judgement instruments START and SAPROF, DUNDRUM-3 and DUNDRUM-4 in forensic mental health services BMC Psychiatry, 2013.PMID 23890106
- [5]Freestone M, Bull D, Brown R, et al. Triage, decision-making and follow-up of patients referred to a UK forensic service: validation of the DUNDRUM toolkit BMC Psychiatry, 2015.PMID 26446536
- [6]Chester V, Alexander RT, Morgan W. Measuring relational security in forensic mental health services BJPsych Bull, 2017.PMID 29234515
- [7]Siu BW, Au-Yeung CC, Chan AW, et al. Measuring the profiles of the security needs of forensic psychiatric inpatients: Validation of the See, Think, Act Scale Asia Pac Psychiatry, 2019.PMID 30378764
- [8]de Vries MG, Verkes RJ, Bulten BH. See think act scale: Validation of the Dutch version of a measure of relational security in high secure forensic psychiatric care Front Psychiatry, 2022.PMID 36262628
- [9]Völlm BA, Edworthy R, Huband N, et al. Characteristics and Pathways of Long-Stay Patients in High and Medium Secure Settings in England; A Secondary Publication From a Large Mixed-Methods Study Front Psychiatry, 2018.PMID 29713294
- [10]Hare Duke L, Furtado V, Guo B, et al. Long-stay in forensic-psychiatric care in the UK Soc Psychiatry Psychiatr Epidemiol, 2018.PMID 29387921
- [11]Fazel S, Fimińska Z, Cocks C, et al. Patient outcomes following discharge from secure psychiatric hospitals: systematic review and meta-analysis Br J Psychiatry, 2016.PMID 26729842
- [12]Wolf A, Fanshawe TR, Sariaslan A, et al. Prediction of violent crime on discharge from secure psychiatric hospitals: A clinical prediction rule (FoVOx) Eur Psychiatry, 2018.PMID 29161680
- [13]Jewell M, Pillai K, Cavney J, et al. Examining the need for a high level of therapeutic security at a regional forensic mental health service in Aotearoa New Zealand Psychiatr Psychol Law, 2024.PMID 38628253
- [14]Coid JW, Hickey N, Yang M. Comparison of outcomes following after-care from forensic and general adult psychiatric services Br J Psychiatry, 2007.PMID 17541111
- [15]McCullough S, Stanley C, Smith H, et al. Outcome measures of risk and recovery in Broadmoor High Secure Forensic Hospital: stratification of care pathways and moves to medium secure hospitals BJPsych Open, 2020.PMID 32684202
- [16]Kennedy HG, Mullaney R, McKenna P, et al. A tool to evaluate proportionality and necessity in the use of restrictive practices in forensic mental health settings: the DRILL tool (Dundrum restriction, intrusion and liberty ladders) BMC Psychiatry, 2020.PMID 33097036
- [17]Holley J, Weaver T, Völlm B. The experience of long stay in high and medium secure psychiatric hospitals in England: qualitative study of the patient perspective Int J Ment Health Syst, 2020.PMID 32256688
- [18]Adams J, Thomas SDM, Mackinnon T, et al. The risks, needs and stages of recovery of a complete forensic patient cohort in an Australian state BMC Psychiatry, 2018.PMID 29415683
- [19]Zagham W, Kisely S, Stedman T, et al. Factors associated with length of stay in medium secure units: A realist review Australas Psychiatry, 2024.PMID 39318046
- [20]Bowden J, Logan C, Robinson L, et al. Clinicians' use of the structured professional judgement approach for adult secure psychiatric service admission assessments: A systematic review PLoS One, 2024.PMID 39325743