Psych · Forensic psychiatry — victimology and trauma
Victimology and trauma in forensic settings
Also known as Victimology forensic psychiatry · Crime victim trauma · Secondary victimisation · Secondary victimization · Poly-victimisation · Victim-offender overlap · Intimate partner violence psychiatry · Sexual assault psychiatric sequelae · Trauma-informed forensic care · Victims of crime mental health
Exam-exhaustive fellowship reference on victimology in forensic settings: crime-related trauma spectra (ASD/PTSD/ICD-11 cPTSD), poly-victimisation and ACE dose-response, secondary victimisation by justice systems, victim–offender overlap, IPV and sexual-assault pathways, acute-to-definitive trauma care with doses, civil disability interface for victims, staff secondary traumatic stress, and trauma-informed forensic practice. Jurisdiction principles only. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Forensic victimology is not a separate DSM diagnosis. It is the interface between victimisation science and clinical–legal practice: who is harmed, how systems respond, what syndromes emerge, and how psychiatrists treat, protect, and opine without causing further harm.[6][7][19] It sits beside (but is not identical to) general PTSD monographs, perpetrator sexual-offending work, and pure civil-capacity work.
Key constructs — exam definitions:
| Construct | Meaning for exams |
|---|---|
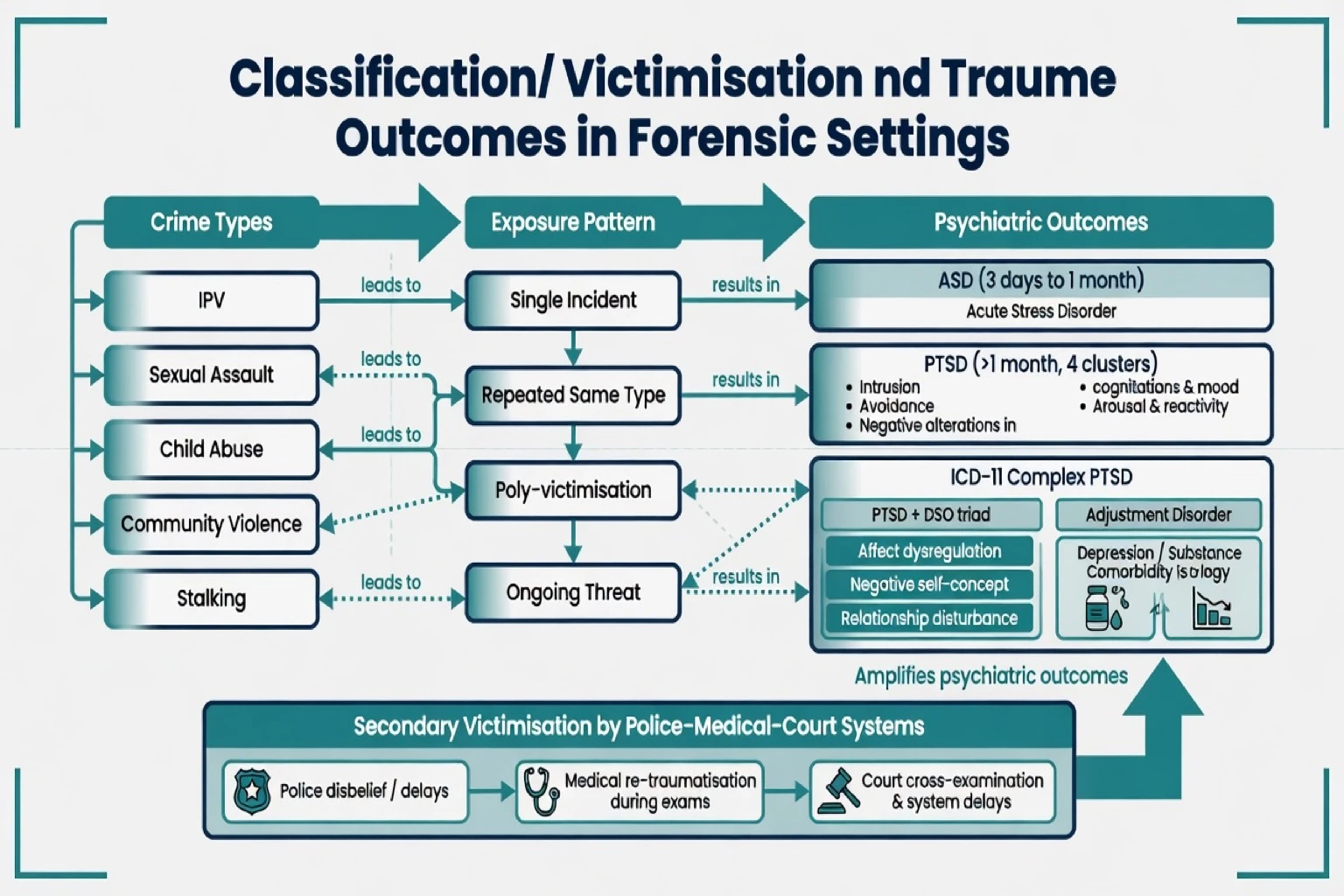
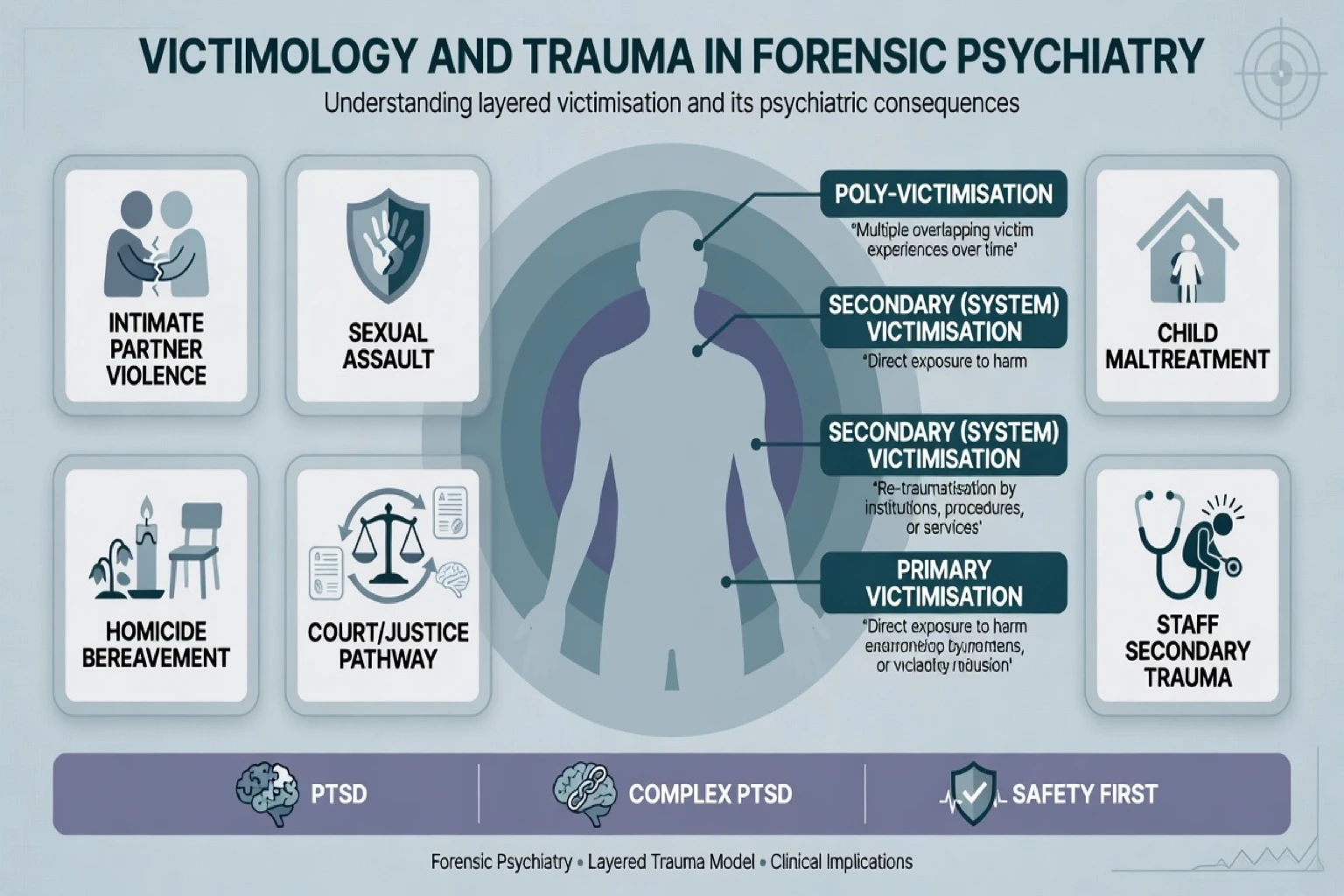
| Primary victimisation | Harm from the index crime/violence |
| Secondary victimisation | Harmful system responses after the crime (disbelief, blame, invasive retelling) |
| Poly-victimisation | Multiple different victimisation types, not only repeats of one type |
| Victim–offender overlap | Same people may be both harmed and harming over time — empirical pattern |
| Tertiary / secondary traumatic stress | Professional exposure to others' trauma |
Classification
Victimisation domains
- Intimate partner violence (IPV) and coercive control — global public-health scale; WHO multi-country lifetime physical/sexual partner violence ranged roughly 15–71% across sites.[9]
- Sexual assault — high conditional PTSD risk; system pathways (SARC/ED, police, courts) heavily studied for secondary victimisation.[2][6][7]
- Child maltreatment and ACE load — dose-response with adult mental and physical morbidity.[3]
- Community/stranger violence, stalking, homicide bereavement, institutional harm.
Psychiatric outcome map
| Outcome | Duration / structure | Forensic note |
|---|---|---|
| Acute stress disorder (ASD) | About 3 days to 1 month after trauma | Early intensive symptoms; not all become PTSD |
| PTSD (DSM-5-TR four clusters) | More than 1 month | Intrusion, avoidance, negative cognitions/mood, arousal |
| ICD-11 PTSD | Re-experiencing, avoidance, sense of current threat | Leaner core than DSM |
| ICD-11 complex PTSD | PTSD core plus disturbances of self-organisation (DSO): affect dysregulation, negative self-concept, relationship disturbance | Enriched after prolonged interpersonal trauma (IPV, childhood abuse) |
| Adjustment / depression / substance | Common comorbidity | Do not stop at a single label |
Epidemiology and risk
Community lifetime PTSD in classic NCS data was about 7.8%, higher in women, with interpersonal violence among the traumas most strongly linked to PTSD.[1] In a national sample of women, PTSD was significantly higher after crime than non-crime trauma.[2]
Poly-victimisation (multiple victimisation types) is highly predictive of trauma symptoms and often accounts for associations previously attributed to single crime categories.[4] Sexual revictimisation is robust: childhood sexual abuse elevates adult sexual-assault risk — association, not destiny, and not victim-blaming.[8] Victim–offender overlap is repeatedly demonstrated longitudinally: many justice-involved people have been victims as well as perpetrators.[5]
Mechanisms
Viva-depth mechanism map for interpersonal crime trauma:
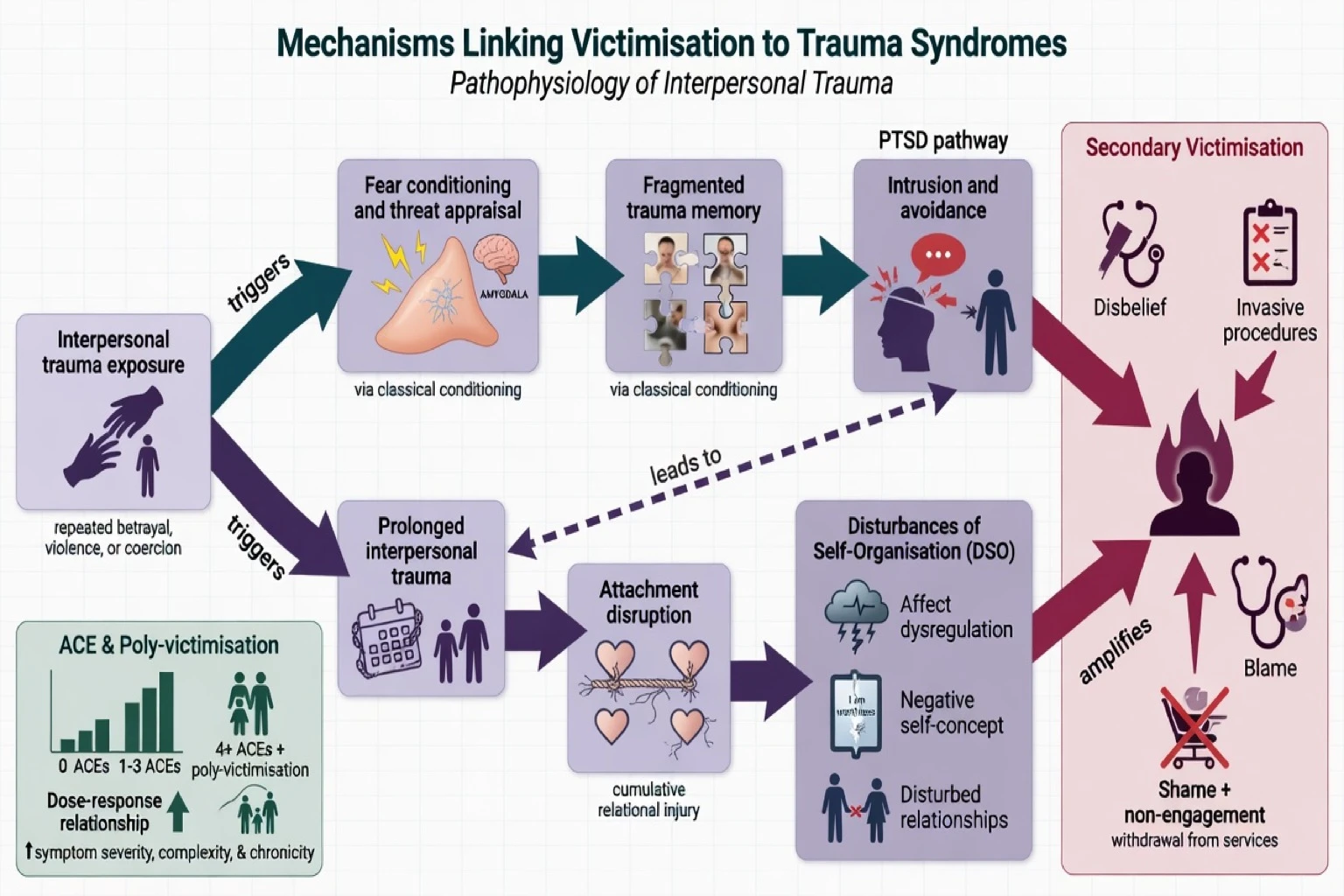
- Fear conditioning and threat appraisal — neutral cues (court buildings, male voices, night-time) acquire threat meaning after interpersonal crime trauma.[1][2]
- Autobiographical memory fragmentation — poorly integrated trauma memories fuel intrusion and incomplete narrative for legal process.[10]
- Shame and self-blame cognitions — especially after sexual assault and IPV; secondary victimisation intensifies them.[6][7]
- Attachment and self-organisation disruption after prolonged interpersonal harm → DSO features of ICD-11 complex PTSD.[10][11]
- ACE biological embedding — cumulative childhood adversity linked to adult disease and psychiatric burden.[3]
Clinical presentation
Common forensic stems
- ED or sexual-assault clinic after rape/drug-facilitated assault.
- IPV presentation labelled “anxiety” or “depression” until safety is asked.
- Court-related deterioration before testimony or family-violence hearings.
- Prisoner or forensic inpatient disclosing historical abuse or in-custody assault — dual victim–offender role.[5][19]
- Homicide-bereaved relative navigating coronial/criminal process.
- Civil claim after crime-related PTSD for disability/compensation (role ethics apply).[21]
MSE language examiners reward
Document trauma-congruent affect (tearfulness, numbing, or blunted shame), startle and hypervigilance, dissociation cues (spacing, time loss), trust rupture without assuming primary psychosis, and risk: suicide, self-harm, return to perpetrator, child safety, substance escalation, absconding from refuge.[2][7][19]
Differential
- 3 days to 1 month after trauma
- Intense early symptoms
- Watchful follow-up; not automatic PTSD
- Symptoms more than 1 month
- Four DSM clusters or ICD-11 lean core
- Trauma-focused therapy first-line when safe
- PTSD core + DSO triad
- Prolonged interpersonal trauma history
- May need skills + processing; avoid endless delay
Other discriminators: trauma-related paranoia versus primary psychosis (form, longitudinal course, non-trauma delusions); major depression without PTSD criteria; TBI after assault; ongoing IPV mislabelled as treatment-resistant anxiety; and invalid responding in high-stakes claims versus genuine disorder under litigation stress — assess validity without default hostility.[21]
Assessment
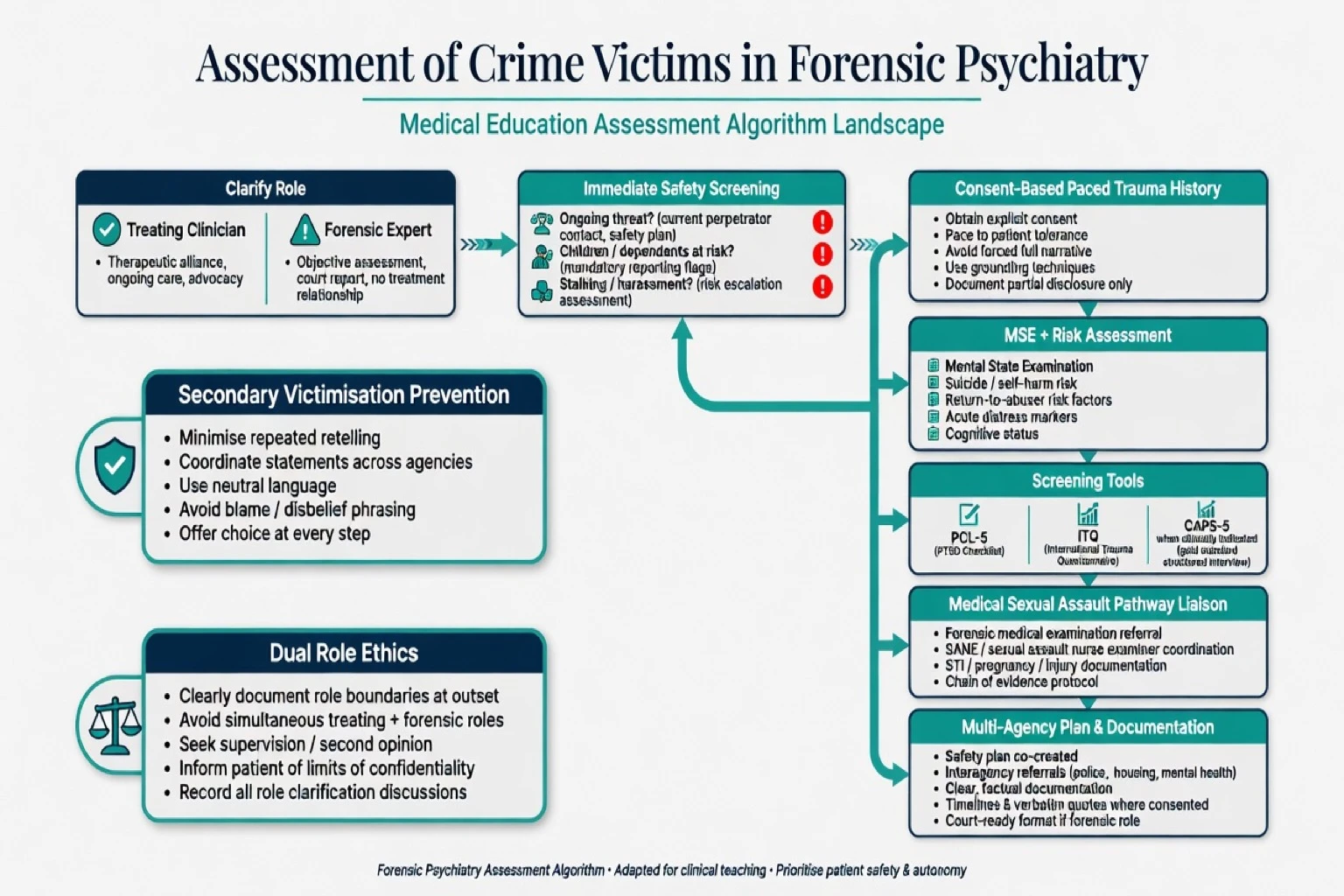
- Role and client — treating clinician versus forensic expert for court/insurer; disclose confidentiality limits.[21]
- Immediate safety — current perpetrator access, weapons, stalking, children, safe contact methods, protective-order status (local law; do not invent sections).
- Paced history — consent-based; avoid forced complete narrative on first contact when destabilising; coordinate so agencies do not re-traumatise through repetition.[6][7]
- MSE and risk — suicide, self-harm, return-to-abuser, child protection, substance, capacity for immediate decisions if relevant.
- Scales — PCL-5 for screening and monitoring; structured diagnostic interview (e.g. CAPS-5 concept) when certainty needed; ICD-11 PTSD/cPTSD screening concepts (ITQ literature line) when DSO is the question.[10][22]
- Collateral — ED/SARC, GP, prior psychiatry; police/court materials when authorised.
- Safeguarding — child and adult protection pathways are jurisdiction-specific and non-optional when thresholds met.
Investigations
Psychiatry rarely “proves” trauma with a scan. Medical/forensic sexual-assault examination is a forensic medicine pathway — protect the evidence chain while offering mental-health support. Toxicology if substance-facilitated assault is live. Baseline labs and pregnancy testing before pharmacotherapy when indicated. Neuroimaging only for organic red flags (focal neurology, severe TBI, new seizures). No investigation substitutes for a safety plan.[7][12][19]
Acute / emergency management
Acute priorities after crime victimisation:
- Medical stabilisation and physical safety.
- Psychological first aid principles: promote safety, calm, connectedness, self-efficacy, and hope — widely endorsed though RCT evidence is weaker than for later trauma-focused therapies; still preferred over universal single-session psychological debriefing.
- Crisis suicide pathway when indicated.
- Short-term benzodiazepines only if essential for severe acute agitation/insomnia — dependence and interference with extinction learning are exam traps; prefer non-benzo supports when feasible.
- Early linkage to sexual-assault counselling / IPV advocacy.
Definitive management
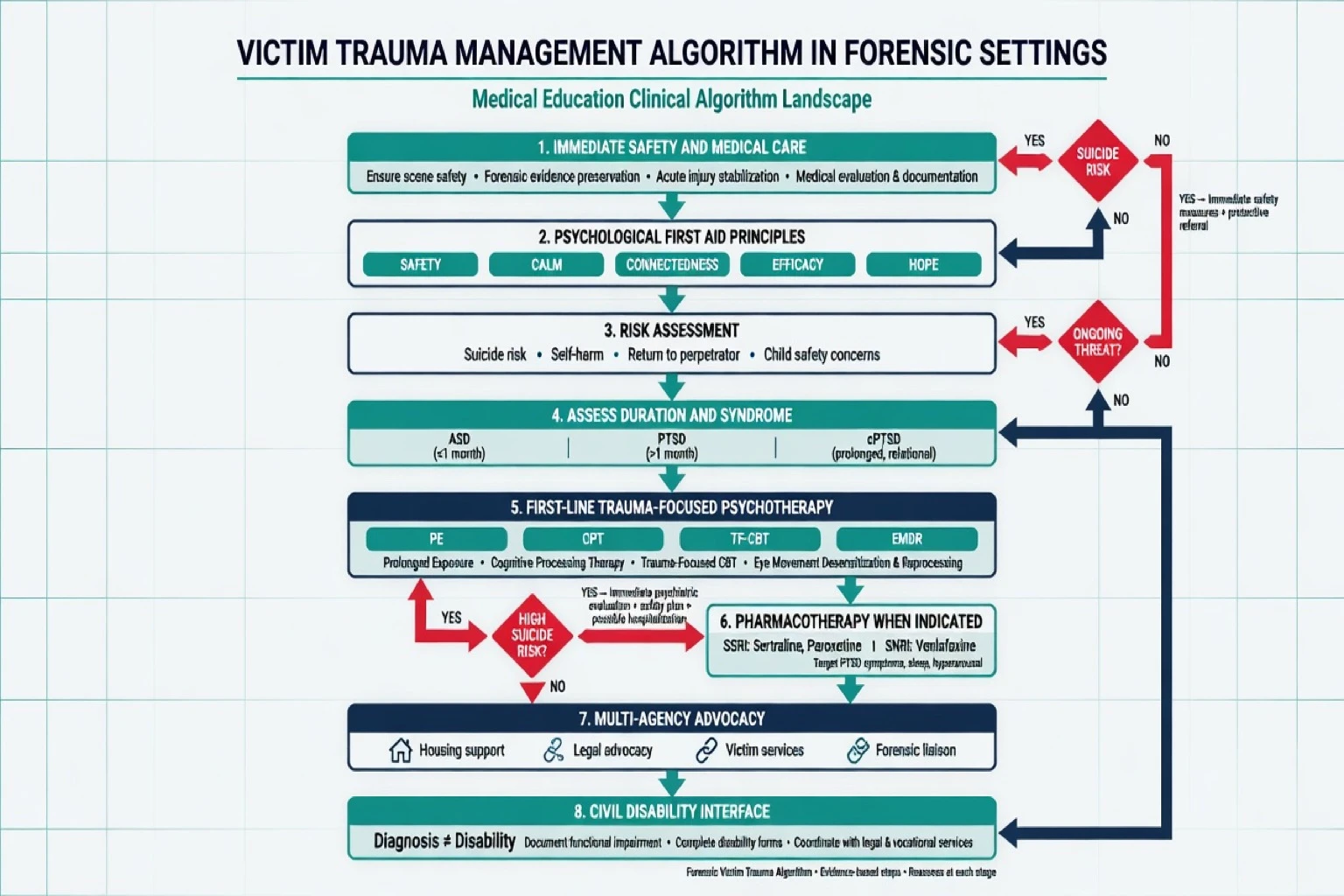
Psychological therapies (first-line)
Trauma-focused psychological therapies have the strongest evidence base for chronic PTSD. Named modalities examiners expect: prolonged exposure (PE), cognitive processing therapy (CPT) — including trials in female victims of interpersonal violence — trauma-focused CBT, and EMDR, with guideline strong/conditional patterns varying by body (APA summary; VA/DoD 2023 synopsis; Cochrane psychotherapies review).[14][15][16][17][18]
Do not keep a ready patient in indefinite “stabilisation only.” Phase-based skills work has a place for severe dysregulation and complex trauma presentations, but therapeutic drift that never reaches trauma processing is a recognised pitfall.[10][19]
Pharmacotherapy (with doses and monitoring)
When medication is used for PTSD (patient preference, severe comorbidity, limited therapy access, or partial response), use evidence-based oral SSRI/SNRI ranges with monitoring:
| Agent | Typical oral dosing (adult) | Monitoring / notes |
|---|---|---|
| Sertraline | Start 25–50 mg daily; titrate toward trial range often 50–200 mg/day | GI upset, sexual SE, hyponatraemia risk in older adults; suicide risk review early in treatment |
| Paroxetine | Often 20 mg daily, range about 20–50 mg/day in fixed-dose PTSD evidence | Sexual SE, discontinuation syndrome; pregnancy counselling |
| Venlafaxine XR | SNRI option used in PTSD practice (see general PTSD evidence base) | BP monitoring as dose rises; discontinuation caution |
| Sertraline and paroxetine have landmark positive RCTs in PTSD and remain the classic exam pharmacologic anchors; Cochrane-aligned pharmacotherapy syntheses support SSRI benefit as a class with modest effects relative to trauma-focused therapy.[12][13][17][18] |
Social and multi-agency care
Housing, legal advocacy, interpreters, cultural supports, child protection, and specialist sexual-assault or IPV services are treatment, not “optional extras.” Trauma-informed forensic mental-health principles emphasise safety, trust/transparency, collaboration, empowerment, and peer support — adapted carefully so security and accountability are not abandoned.[19]
Civil / compensation interface
Victims may seek psychiatric disability or compensation opinions. Use structured forensic disability method: clarify questions, sources, role ethics, diagnosis, functional analysis, causation reasoning, and validity consideration. PTSD on a letter is not total permanent disability. Do not invent compensation-scheme section numbers or universal percentage tables.[21]
Subtypes and scenarios
| Scenario | Exam focus |
|---|---|
| Acute sexual assault | SARC/ED pathway; secondary victimisation risk; early support |
| IPV / coercive control | Safety planning; children; repeated trauma → cPTSD risk |
| Child maltreatment survivors | ACE load; revictimisation risk; adult forensic/civil presentations |
| Prison / forensic inpatient victims | High trauma base rates; dual victim–offender; therapeutic security |
| Homicide bereavement | Complicated grief + PTSD features; court exposure |
| Stalking | Ongoing threat; hypervigilance may be reality-based |
| Witnesses | Trauma-informed court support; minimise retelling |
Complications and pitfalls
- Causing secondary victimisation through blame or procedural coldness.[6]
- Missing ongoing danger while treating “PTSD.”
- Moralising the victim–offender overlap or denying either role.[5]
- Default assumption of malingering in every civil claim.[21]
- Equating diagnosis with incapacity or total work unfitness.
- Inventing victims-of-crime statute numbers.
- Ignoring staff secondary traumatic stress — an occupational hazard in trauma workforces.[20]
- Indefinite stabilisation without offering trauma-focused therapy when indicated.
Prognosis and disposition
Many people improve substantially with trauma-focused therapy; chronicity is more likely with interpersonal trauma, poly-victimisation, ongoing threat, poor social support, and untreated comorbidity.[1][4][14] Disposition ranges from community trauma services to crisis teams, inpatient care for high suicide risk, multi-agency IPV plans, and forensic inpatient trauma-informed care. Reassess after major legal milestones (verdict, sentencing, family-court outcomes) when symptoms often spike.
Special populations
- Children/youth — developmentally adapted care; mandatory reporting interfaces.
- Older adults — elder abuse overlap; cognitive impairment complicates history.
- Intellectual disability — elevated victimisation risk; adapted communication.
- Indigenous and CALD — culturally safe care, interpreters, historical trauma context without stereotyping.
- Male and LGBTIQ+ sexual-assault survivors — under-recognition and shame barriers.
- Perinatal — IPV risk to mother and infant.
- Forensic/prison populations — dual roles; complex trauma common.[3][5][19]
Evidence and regional deltas
[17] [18] [21]Landmark anchors to name: Kessler NCS; Resnick crime-related PTSD; Felitti ACE; Finkelhor poly-victimisation; Classen revictimisation; Jennings victim–offender overlap; Campbell secondary victimisation; WHO IPV; ICD-11 PTSD/cPTSD evidence (Brewin, Cloitre); Bisson Cochrane; Foa PE; Resick CPT; Brady sertraline; Marshall paroxetine; Bride STS; Roy trauma-informed forensic care.[1][2][3][4][5][6][12][16][19]
Exam pearls
References
- [1]Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB Posttraumatic stress disorder in the National Comorbidity Survey Arch Gen Psychiatry, 1995.PMID 7492257
- [2]Resnick HS, Kilpatrick DG, Dansky BS, Saunders BE, Best CL Prevalence of civilian trauma and posttraumatic stress disorder in a representative national sample of women J Consult Clin Psychol, 1993.PMID 8113499
- [3]Felitti VJ, Anda RF, Nordenberg D, Williamson DF, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study Am J Prev Med, 1998.PMID 9635069
- [4]Finkelhor D, Ormrod RK, Turner HA Poly-victimization: a neglected component in child victimization Child Abuse Negl, 2007.PMID 17224181
- [5]Jennings WG, Higgins GE, Tewksbury R, Gover AR, Piquero AR A longitudinal assessment of the victim-offender overlap J Interpers Violence, 2010.PMID 20068116
- [6]Campbell R, Raja S Secondary victimization of rape victims: insights from mental health professionals who treat survivors of violence Violence Vict, 1999.PMID 10606433
- [7]Campbell R The psychological impact of rape victims Am Psychol, 2008.PMID 19014228
- [8]Classen CC, Palesh OG, Aggarwal R Sexual revictimization: a review of the empirical literature Trauma Violence Abuse, 2005.PMID 15753196
- [9]Garcia-Moreno C, Jansen HA, Ellsberg M, Heise L, Watts CH Prevalence of intimate partner violence: findings from the WHO multi-country study on women's health and domestic violence Lancet, 2006.PMID 17027732
- [10]Brewin CR, Cloitre M, Hyland P, Shevlin M, et al. A review of current evidence regarding the ICD-11 proposals for diagnosing PTSD and complex PTSD Clin Psychol Rev, 2017.PMID 29029837
- [11]Cloitre M, Garvert DW, Brewin CR, Bryant RA, et al. Evidence for proposed ICD-11 PTSD and complex PTSD: a latent profile analysis Eur J Psychotraumatol, 2013.PMID 23687563
- [12]Brady K, Pearlstein T, Asnis GM, Baker D, et al. Efficacy and safety of sertraline treatment of posttraumatic stress disorder: a randomized controlled trial JAMA, 2000.PMID 10770145
- [13]Marshall RD, Beebe KL, Oldham M, Zaninelli R Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebo-controlled study Am J Psychiatry, 2001.PMID 11729013
- [14]Bisson JI, Roberts NP, Andrew M, Cooper R, Lewis C Psychological therapies for chronic post-traumatic stress disorder (PTSD) in adults Cochrane Database Syst Rev, 2013.PMID 24338345
- [15]Foa EB, Hembree EA, Cahill SP, Rauch SA, et al. Randomized trial of prolonged exposure for posttraumatic stress disorder with and without cognitive restructuring J Consult Clin Psychol, 2005.PMID 16287395
- [16]Resick PA, Galovski TE, Uhlmansiek MO, Scher CD, et al. A randomized clinical trial to dismantle components of cognitive processing therapy for posttraumatic stress disorder in female victims of interpersonal violence J Consult Clin Psychol, 2008.PMID 18377121
- [17]Guideline Development Panel for the Treatment of PTSD in Adults, American Psychological Association Summary of the clinical practice guideline for the treatment of posttraumatic stress disorder (PTSD) in adults Am Psychol, 2019.PMID 31305099
- [18]Schnurr PP, Hamblen JL, Wolf J, et al. The Management of Posttraumatic Stress Disorder and Acute Stress Disorder: Synopsis of the 2023 U.S. Department of Veterans Affairs and U.S. Department of Defense Clinical Practice Guideline Ann Intern Med, 2024.PMID 38408360
- [19]Rodwell D, Edworthy R Using a trauma-informed care framework to explore social climate and borderline personality disorder in forensic inpatient settings Int J Ment Health Nurs, 2024.PMID 38291657
- [20]Bride BE Prevalence of secondary traumatic stress among social workers Soc Work, 2007.PMID 17388084
- [21]Gold LH, Anfang SA, Drukteinis AM, et al. AAPL Practice Guideline for the Forensic Evaluation of Psychiatric Disability J Am Acad Psychiatry Law, 2008.PMID 19092058
- [22]Blevins CA, Weathers FW, Davis MT, Witte TK, Domino JL The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation J Trauma Stress, 2015.PMID 26606250