Psych · Forensic psychiatry — young offenders
Young offenders
Also known as Youth justice mental health · Juvenile offenders · Justice-involved youth · Youth detention psychiatry · Adolescent forensic psychiatry · CAMHS forensic liaison · Young people who offend · Juvenile detention mental health
Exam-exhaustive fellowship reference on young offenders and youth justice mental health — detention prevalence, Moffitt developmental pathways, trauma and neurodevelopmental comorbidity, SAVRY-informed assessment, suicide/self-harm, diversion, MST/FFT/TFCO principles, multi-agency care, and transition risk. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
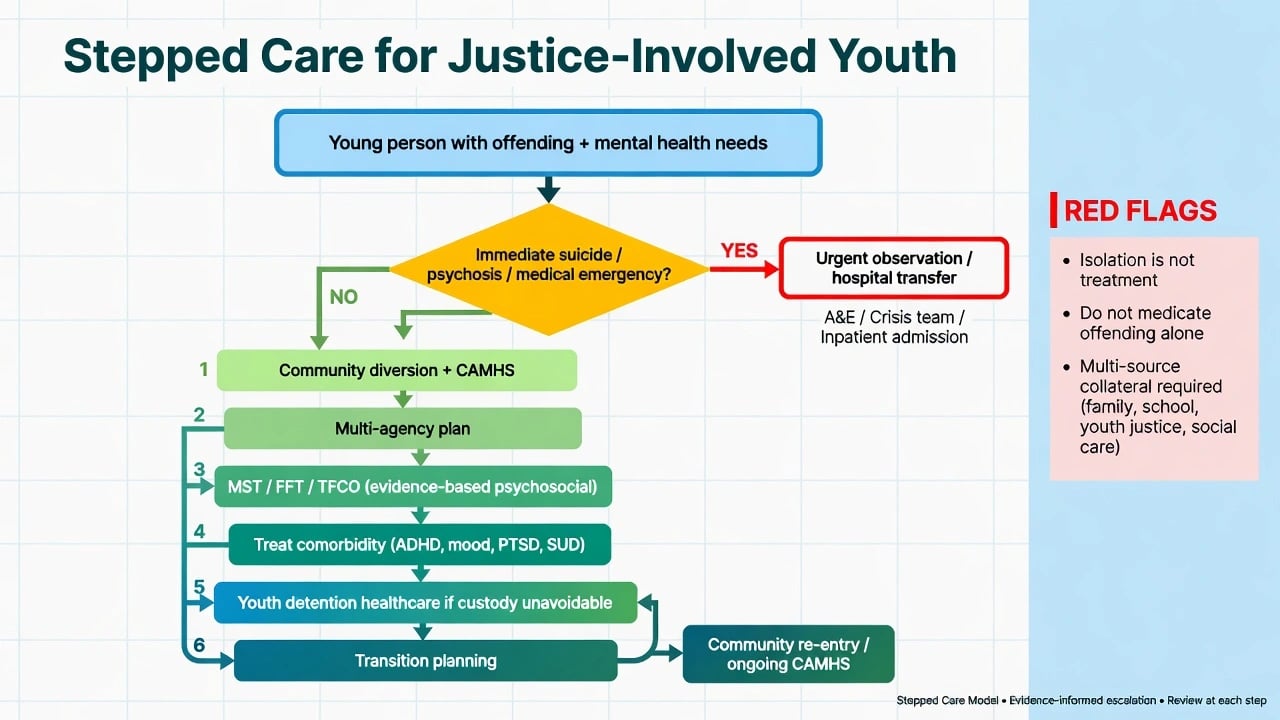
Red flags
Overview and definition
Young offender / justice-involved youth is a legal-service construct: a child or adolescent in contact with police, diversion schemes, youth courts, community youth justice orders, or detention. It is not a DSM-5-TR or ICD-11 diagnosis. Clinical work sits at the interface of CAMHS, forensic psychiatry, youth justice, education, and often child protection.[16]
Operational map:
- Diversion — pathways away from formal prosecution into health/social interventions when risk and public interest allow.
- Community youth justice — orders, supervision, and multi-agency plans outside custody.
- Youth detention / juvenile correctional facilities — secure custody for remand or sentenced youth (terminology varies by jurisdiction).
- Secure welfare / welfare pathways — in some systems, welfare-driven secure placements distinct from pure criminal custody.
- Transition — moving into adult criminal justice or adult mental health at the age threshold (often 18; local rules vary).[16]
Age of criminal responsibility, doli incapax (or equivalent developmental competence presumptions), and specific youth justice orders are jurisdiction-specific. Fellowship answers use principles (developmental maturity, least restrictive response, welfare–justice balance) and do not invent section numbers or universal ages.[16]
Clinical frameworks that commonly co-travel with youth justice status include DSM-5-TR oppositional defiant disorder and conduct disorder (with limited prosocial emotions specifier where applicable) and ICD-11 oppositional defiant / conduct-dissocial constructs. Adult antisocial personality disorder is not diagnosed before age 18; premature psychopathy language is an exam pitfall.[7][16]
This topic is distinct from adult prison mental health, pure community CD/ODD monographs, adult ASPD/psychopathy, and adult HCR-20-centric risk assessment — though all intersect at transfer and dual-diagnosis edges.[16]
Epidemiology — base rates examiners expect
Youth in detention and correctional facilities have markedly elevated psychiatric morbidity compared with community adolescents. Fazel and colleagues’ 2008 systematic review and metaregression of 25 surveys established the modern base-rate picture; Beaudry and colleagues (2021) updated the meta-regression across broader international samples.[1][2]
Order-of-magnitude anchors for exams (exact percentages vary by sex, instrument, remand vs sentenced status, and country):
- Conduct disorder — often the modal externalising diagnosis in detention samples.
- Substance use disorders — very high; frequently comorbid rather than isolated.
- ADHD — substantially enriched versus community peers.
- Major depression — elevated; under-detected when “behaviour” dominates the referral.
- Psychotic illness — less common than CD/SUD but still elevated relative to community adolescents.
- PTSD and trauma exposure — highly prevalent; Abram and colleagues documented substantial PTSD and trauma burden in the Northwestern Juvenile Project detention samples.[1][2][3][5][9]
Teplin and colleagues’ Northwestern Juvenile Project remains a landmark US detention epidemiology series: high absolute rates of multiple disorders in detained youth, with comorbidity as the rule rather than the exception.[3][4] Fifteen-year longitudinal follow-up shows continuity of psychiatric disorder into adulthood for many justice-involved youths — youth justice contact is a marker for long-term mental health need, not a brief legal inconvenience.[6]
Colins and colleagues’ systematic review of detained male adolescents consolidates high rates of disruptive behaviour disorders, substance use, and affective disorders across European and international samples.[9]
ADHD in childhood associates with elevated long-term criminal outcomes in longitudinal data (Dalsgaard et al.) — examiners use this to justify neurodevelopmental assessment, not to claim ADHD “causes” crime in a simple sense.[15]
Girls in justice settings often show particularly high internalising disorders, PTSD, and self-harm relative to justice-involved boys in many samples; gender-responsive assessment is mandatory.[3][5][16]
Indigenous and minority youth are over-represented in many youth justice systems. Frame this as structural and historical drivers (poverty, racism, child-protection pathways, policing patterns), not racialised psychopathology. Cultural safety is clinical competence.[16]
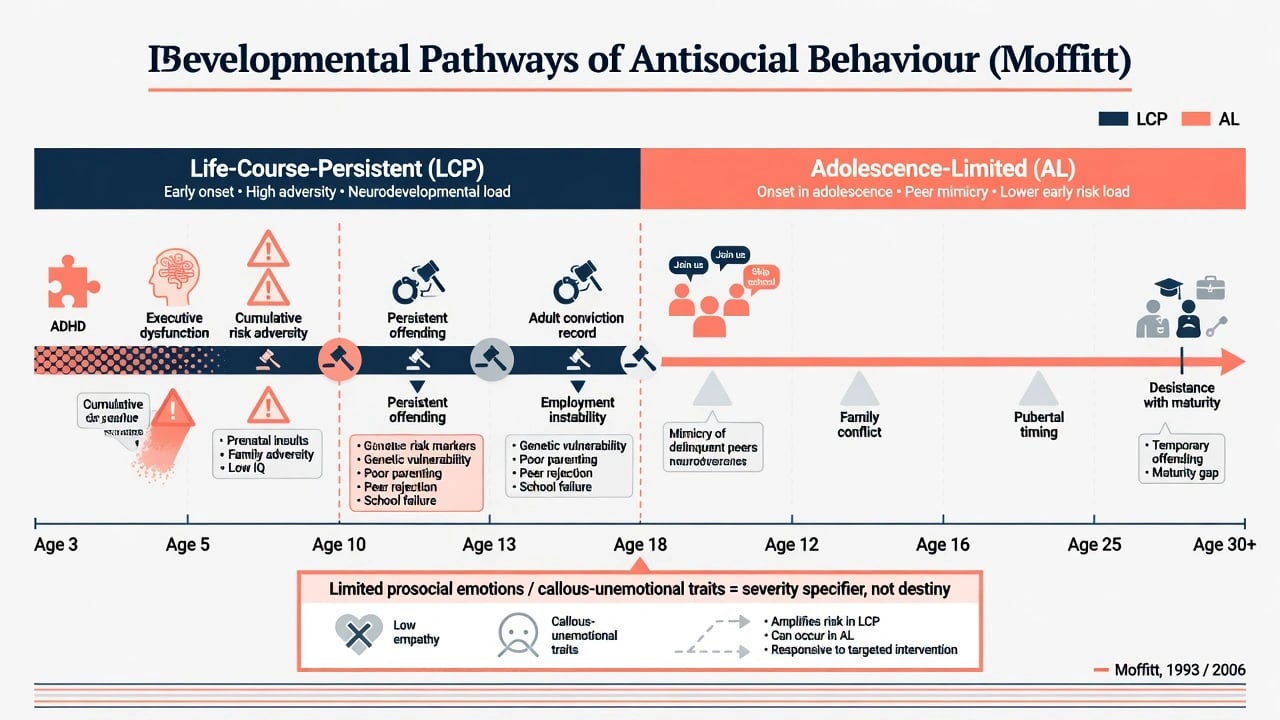
Developmental mechanisms — Moffitt taxonomy
Moffitt’s developmental taxonomy remains the highest-yield conceptual frame for fellowship exams:[7][8]
- Life-course-persistent (LCP) antisocial behaviour — early onset, high early adversity and neurodevelopmental load (impulsivity, cognitive/executive difficulties, harsh or disrupted caregiving), more persistent adult antisocial and health burden.
- Adolescence-limited (AL) antisocial behaviour — onset nearer adolescence, more peer-driven “maturity gap” and mimicry of delinquent peers, higher rates of desistance with adult roles and reduced deviant peer exposure.[7][8]
Follow-up to age 26 supports differentiation of pathways in males on key adult outcomes — use as probabilistic formulation, not fatalism.[8]
Limited prosocial emotions / callous-unemotional traits (DSM-5-TR CD specifier territory) mark severity and treatment complexity for some youth. They are dimensional risk markers, not a licence to abandon care or to diagnose adult psychopathy in a 14-year-old.[7][16]
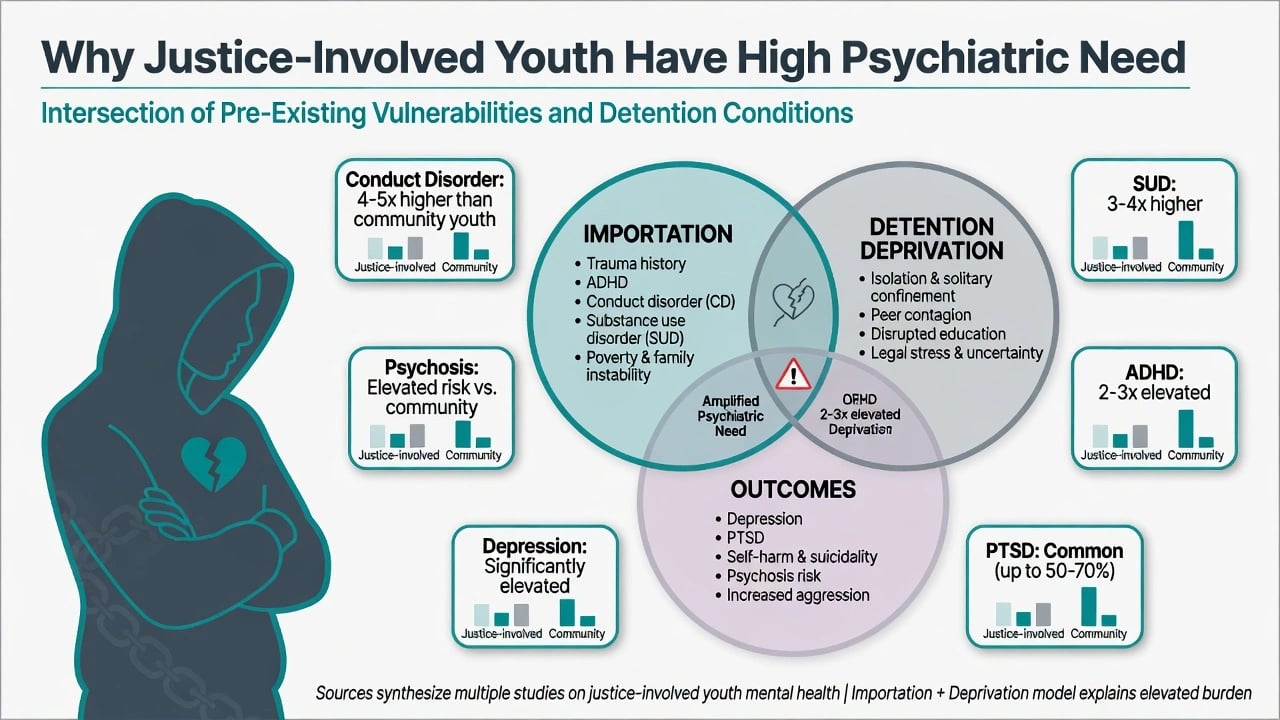
Complementary custody models (borrowed from prison literature and adapted to youth):
- Importation — trauma, CD, ADHD, SUD, poverty, and disrupted care enter detention with the young person.
- Deprivation — isolation, peer contagion, legal uncertainty, disrupted education, and loss of family contact worsen mental health and self-harm risk inside custody.[2][16]
Clinical presentation
Reception to youth detention — first hours/days: intoxication or withdrawal, untreated ADHD or mood disorder, active suicidal ideation, post-arrest hyperarousal, aggression after peer provocation, and fear or shame after first custody. First nights are a high-risk suicide/self-harm window analogous to adult remand peaks — systems must not defer urgent reviews to “morning clinic” when ideation or severe withdrawal is present.[2][16]
Community youth justice — school exclusion, truancy, substance use, family conflict, property or violent offences with untreated CD/ADHD, running away, and exploitation risk. Referrals often frame the problem as “non-compliance”; the psychiatric task is formulation of drivers.[2][16]
MSE adapted to development — plain language, developmental age (not only chronological), time for rapport, attention to literacy and language, and explicit limits of confidentiality (safety/harm). Quote risk content. Observe impulsivity, affective range, trauma cues, psychotic symptoms, and cognitive style.[16][3]
Collateral is non-negotiable — caregivers, school, youth justice workers, prior CAMHS, and child-protection records (lawful access). Single-source youth self-report underestimates externalising and trauma history in many cases.[3][14]
Differential diagnosis
| Presentation | Prefer | Discriminators |
|---|---|---|
| Defiance, fights, rule-breaking | CD / ODD spectrum | Duration, settings, intent, limited prosocial emotions features |
| Inattention, impulsivity from early childhood | ADHD | Onset, school history, not only custody behaviour |
| Flashbacks, hyperarousal, avoidance | PTSD | Trauma chronology; aggression may be defensive |
| Grandiosity, decreased sleep, pressure | Mania / mixed | Episodic change from baseline; family bipolar history |
| Hallucinations, delusions, thought disorder | Psychosis spectrum vs substance-induced | Onset relative to substances; persistence when abstinent |
| Social naivety, rigidity, sensory issues | Autism | Developmental history; “non-compliance” may be misunderstanding |
| Global adaptive deficits | Intellectual disability | Adaptive function, not IQ alone; vulnerability and suggestibility |
| Distress only after arrest | Situational stress | Still screen suicide; do not skip major depression |
Differential work in detention must actively separate situational stress, substance-induced states, neurodevelopmental drivers, trauma, mood/psychosis, and CD-spectrum behaviour rather than collapsing everything into “attitude.” Malingering for placement is possible but should be a late hypothesis — false negatives on suicide and psychosis cost lives.[3][5][9][15]
Assessment structure
- Context — police diversion, community order, remand, sentenced detention, transfer risk.
- Developmental and family history — pregnancy/perinatal, milestones, ADHD/learning, trauma, attachment disruptions, parental mental illness/SUD.
- Offending pattern — onset, versatility, weapons, victims, planning vs impulsive, peer vs solo, escalation.
- Psychiatric review of systems — mood, psychosis, PTSD, OCD, eating, neurodevelopmental.
- Substances — onset, type, withdrawal risk, dealing/coercion context.
- Risk triad — suicide/self-harm; violence to others; vulnerability (victimisation, exploitation, bullying, trafficking).
- Protective factors — attachments, education engagement, prosocial activities, motivation, cultural supports.
- Legal/developmental competence issues — fitness/capacity principles for youth; do not invent local statutes.
- Safeguarding — child-protection thresholds are parallel duties, not optional extras.[14][16][3]
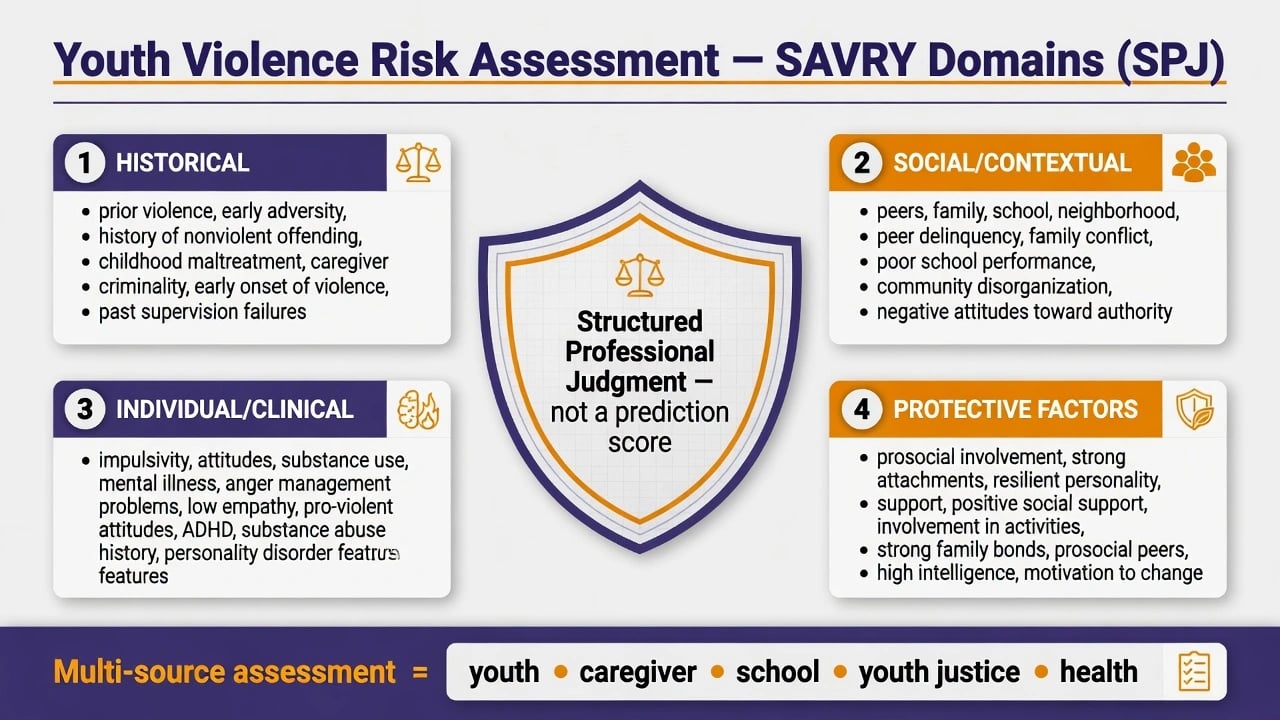
Youth violence risk tools — SAVRY concept
The Structured Assessment of Violence Risk in Youth (SAVRY) is the classic exam-named structured professional judgment (SPJ) framework for adolescent violence risk. Domain clusters: historical, social/contextual, individual/clinical, plus explicit protective factors. Predictive validity has been studied in residential/treatment samples; use as structured judgment, not a false-precision actuarial “score that replaces thinking”.[14]
Investigations
- UDS and breath/alcohol as indicated; pregnancy testing when clinically relevant.
- Baseline metabolic panel and ECG before stimulants or QT-prolonging antipsychotics when those agents are considered.
- Neurodevelopmental screens and formal cognitive/adaptive assessment when history suggests ID/ASD/learning disability.
- Trauma and depression/suicidality instruments appropriate to age.
- Imaging/EEG only for organic red flags (not routine for CD).
- Obtain school psychometrics and prior assessments when available.[15][16]
Acute and emergency management
Suicide and self-harm in youth custody — enhanced or constant observation as indicated; means restriction (ligature-aware environments); urgent psychiatric review; treat underlying depression/psychosis/PTSD/SUD; hospital transfer when needs exceed detention healthcare capacity. Self-harm is a clinical signal, not pure manipulation or a discipline-only event.[2][16]
Acute behavioural disturbance — de-escalation first; sensory and relational approaches; least restrictive containment; avoid adult-style prolonged isolation sold as “treatment.” Rapid tranquillisation principles, if ever required, follow youth-adapted local protocols with monitoring — examiners want restraint on medication-as-behaviour-control, not inventing doses.[16][2]
Withdrawal at reception (alcohol, benzodiazepines, opioids) is a medical pathway. Stimulant crash can unmask depression and suicide risk after the acute phase.[16]
Safeguarding emergencies — disclosures of abuse, trafficking, or imminent community harm require parallel child-protection and multi-agency action.[5][16]
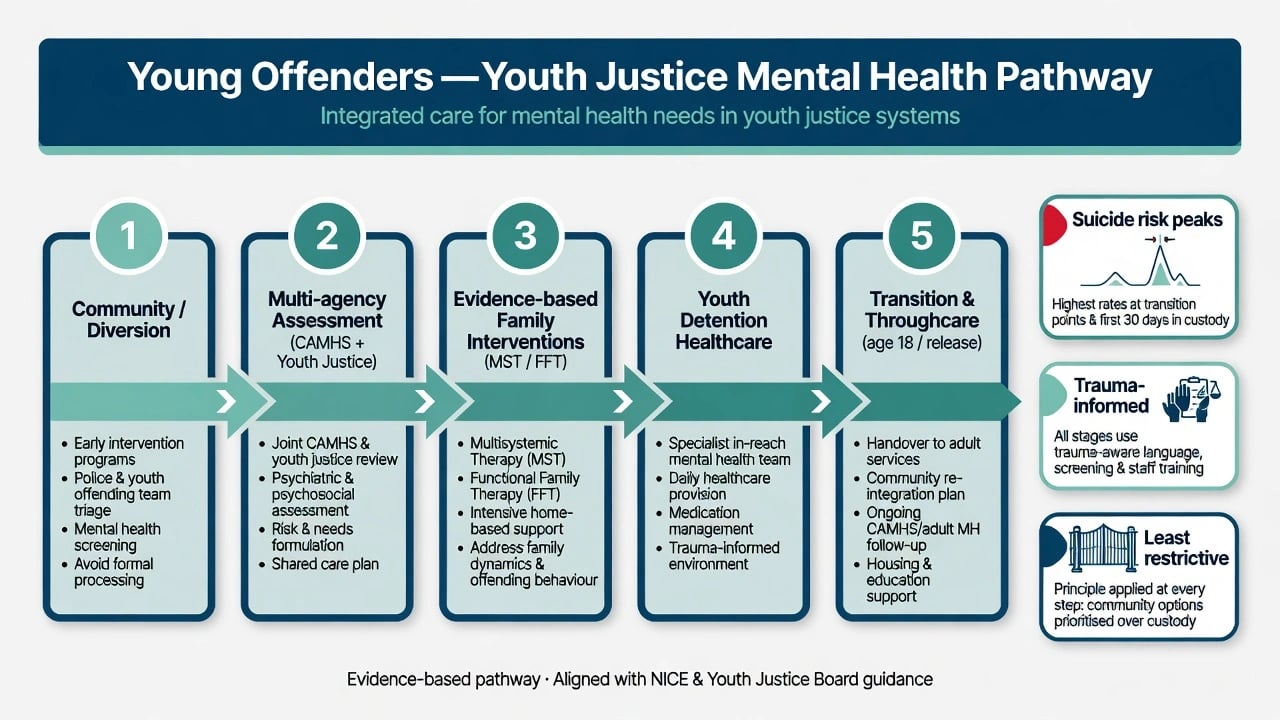
Definitive management — stepped, multi-system care
Principles
- Least restrictive youth justice response compatible with safety and public protection.
- Treat disorders and systems — family, school, peers, substances — not “offending” as a standalone disease.
- Multi-agency shared plan with clear roles and risk communication (need-to-know, lawful).
- Pharmacotherapy targets diagnosed conditions (ADHD, depression, psychosis, etc.), never as primary anti-offending chemotherapy.
- Throughcare from first contact through release or adult transfer.[10][11][13][16]
Named psychosocial interventions (high-yield)
Multisystemic Therapy (MST) — intensive, home- and community-based, ecological intervention addressing family, school, peer, and individual drivers of serious antisocial behaviour. Meta-analytic and programme literature support reduced out-of-home placement and antisocial outcomes when implemented with fidelity; Henggeler’s overviews summarise clinical model and implementation science.[10][11]
Functional Family Therapy (FFT) — structured family therapy for youth with behaviour problems; systematic review and meta-analysis evidence is mixed-to-positive depending on outcome and implementation quality — know the name, target population, and family focus for exams.[12]
Multidimensional Treatment Foster Care / Treatment Foster Care Oregon (TFCO) principles — therapeutic foster care alternative to group residential placement for high-need justice-involved youth, with caregiver training and multi-system coordination (exam-level concept; local programme names vary). Non-institutional multi-system alternatives sit in the same evidence family as other psychosocial recidivism-prevention programmes reviewed in meta-analysis.[13][10]
Non-institutional psychosocial interventions overall show modest average effects on juvenile recidivism in meta-analysis — effect sizes depend on programme type and fidelity; examiners want realistic evidence literacy, not miracle claims.[13]
Treating comorbidity
- ADHD — confirm diagnosis multi-source; consider methylphenidate or amphetamine-class stimulants or non-stimulants (e.g. atomoxetine) per youth guidelines and local formulary; monitor appetite, sleep, growth, BP/HR, and diversion risk in justice settings. Treating ADHD may improve self-regulation and school engagement; it is not a recidivism panacea.[15][16]
- Depression — psychological therapies first-line for mild–moderate; SSRIs (e.g. fluoxetine where licensed/indicated) with close monitoring for activation, suicidal ideation, and adherence — youth antidepressant cautions apply.[16]
- PTSD — trauma-focused psychological therapies when safe and stabilised; do not force exposure work in chaotic detention without stabilisation and skilled therapists.[5][16]
- SUD — integrated concurrent care; motivational approaches; family involvement; avoid sequential “fix substances first forever.”[1][16]
- Psychosis — urgent specialist pathway; antipsychotic choice and dosing follow youth psychosis protocols with metabolic/ECG monitoring; early transfer if detention cannot deliver safe care.[2][16]
Exact doses are protocol- and licence-specific; viva answers emphasise agent class, monitoring, diversion risk, and consent/assent frameworks, not invented universal milligram tables.[16]
Stepped disposition ladder
- Community diversion + CAMHS
- Multi-agency intensive community plan
- MST / FFT / TFCO-type programmes
- Optimise comorbidity treatment
- Youth detention healthcare if custody unavoidable
- Hospital transfer when acuity exceeds detention capacity
- Transition planning (release or adult estate)[10][11][13]
Subtypes and high-yield scenarios
- First-remand night with suicidal ideation after first charge.
- Community intensive supervision with untreated ADHD, cannabis use, and CD.
- Girl in detention with PTSD, repeated self-harm, and sexual exploitation history.
- Indigenous youth — cultural formulation, family, structural over-representation.
- ID/ASD dual diagnosis — communication adaptations, vulnerability, fitness interfaces.
- Emerging psychosis versus substance-induced psychosis in detention.
- Age-18 transfer to adult prison without medicine or appointment continuity.
- Harmful sexual behaviour pathway — specialist forensic CAMHS, not generic wing advice alone.[5][6][16]
Complications and pitfalls
- Adultifying adolescents with ASPD/psychopathy labels.
- CD-only formulations that miss ADHD, trauma, ID, mood, or psychosis.
- Isolation-as-care; punitive responses to self-harm.
- Inventing age-of-criminal-responsibility ages or youth justice sections as universal facts.
- Sedation for behaviour without environmental or trauma formulation.
- Breaking multi-agency information-sharing duties in either direction (over-share full notes vs under-share critical risk).
- Stopping community ADHD or antipsychotic medicines at reception without plan.[7][15][16]
Prognosis and disposition
Many AL-pathway youths desist with maturation, reduced deviant peer exposure, education/employment, and family support. LCP-pathway youths carry higher cumulative risk into adult antisocial behaviour, substance use, and health burden — they need intensive multi-system intervention, not therapeutic nihilism.[7][8]
Psychiatric continuity after juvenile justice involvement is substantial over 15 years in longitudinal data — plan long-horizon care, not single court-report episodes.[6]
Disposition is a clinical intensity ladder matched to risk and need. Successful step-down associates with engagement, substance control, family/school stabilisation, and treated comorbidity — probabilistic, not guaranteed.[10][13]
Special populations
Special populations needing adapted pathways include girls and young women (trauma, self-harm, reproductive health), Indigenous youth (cultural safety, family leadership, structural context), intellectual disability and autism, LGBTQ+ youth (placement safety, minority stress), very young adolescents near local age-of-criminal-responsibility thresholds, and refugee/asylum-seeking youth (trauma, language, legal status stress).[3][5][16]
Youth justice is state/territory-based; Indigenous over-representation and Closing-the-Gap context are viva-critical. CAMHS–forensic liaison and dual-involvement (care and protection plus youth justice) are common. Cite principles of least restrictive intervention and cultural safety; do not invent Children/Young Offenders Act section numbers.[16]
Beaudry/Fazel updates show the detention morbidity problem is international. Resource limits change delivery, not the duty to screen for suicide, psychosis, withdrawal, and trauma, and to prefer community multi-system interventions where available.[2]
Evidence and guidelines
Landmark evidence clusters: Fazel 2008 and Beaudry 2021 detention meta-analyses; Teplin/Abram Northwestern series; Moffitt taxonomy; MST meta-analysis and programme science; FFT systematic review; Olsson 2021 noninstitutional intervention meta-analysis; SAVRY predictive validity studies; Dalsgaard ADHD criminal outcome; Underwood overview of mental illness in juvenile offenders.[1][2][3][7][10][12][13][14][15][16]
Guideline stance for exams: RANZCP child/adolescent and forensic interface principles; NICE conduct/antisocial and criminal justice mental health principles; AACAP practice parameters — always as principles, with local service pathways varying. Primary evidence anchors remain the detention meta-analyses, Northwestern series, Moffitt taxonomy, MST/FFT literature, and SAVRY SPJ studies cited above.[1][2][10][16]
Exam pearls
- Detention = high base-rate psychiatry — CD, SUD, ADHD, depression, PTSD dominate; psychosis elevated but not modal.[1][2][3]
- Quote Moffitt AL vs LCP unprompted in developmental stems.[7][8]
- Comorbidity is the rule (Abram/Teplin).[4]
- SAVRY = youth SPJ with protective factors.[14]
- Name MST and FFT as multi-system/family interventions.[10][12]
- Do not medicate offending; treat disorders and change systems.[11][16]
- Isolation is not treatment; first nights and transitions are suicide risk peaks.[16]
- Never invent youth justice statute sections or universal ages of criminal responsibility.
- Longitudinal continuity: youth justice contact predicts ongoing psychiatric need into adulthood.[6]
Related topics
Cross-links: prison mental health (adult custody); conduct and oppositional disorders; antisocial personality disorder; risk assessment in forensic settings; fitness to stand trial; deliberate self-harm. Young offenders is the youth justice leaf at their intersection.[16]
References
- [1]Fazel S, Doll H, Långström N Mental disorders among adolescents in juvenile detention and correctional facilities: a systematic review and metaregression analysis of 25 surveys J Am Acad Child Adolesc Psychiatry, 2008.PMID 18664994
- [2]Beaudry G, Yu R, Långström N, Fazel S An Updated Systematic Review and Meta-regression Analysis: Mental Disorders Among Adolescents in Juvenile Detention and Correctional Facilities J Am Acad Child Adolesc Psychiatry, 2021.PMID 32035113
- [3]Teplin LA, Abram KM, McClelland GM, et al. Psychiatric disorders in youth in juvenile detention Arch Gen Psychiatry, 2002.PMID 12470130
- [4]Abram KM, Teplin LA, McClelland GM, Dulcan MK Comorbid psychiatric disorders in youth in juvenile detention Arch Gen Psychiatry, 2003.PMID 14609885
- [5]Abram KM, Teplin LA, Charles DR, et al. Posttraumatic stress disorder and trauma in youth in juvenile detention Arch Gen Psychiatry, 2004.PMID 15066899
- [6]Teplin LA, Potthoff LM, Aaby DA, et al. Prevalence, Comorbidity, and Continuity of Psychiatric Disorders in a 15-Year Longitudinal Study of Youths Involved in the Juvenile Justice System JAMA Pediatr, 2021.PMID 33818599
- [7]Moffitt TE Adolescence-limited and life-course-persistent antisocial behavior: a developmental taxonomy Psychol Rev, 1993.PMID 8255953
- [8]Moffitt TE, Caspi A, Harrington H, Milne BJ Males on the life-course-persistent and adolescence-limited antisocial pathways: follow-up at age 26 years Dev Psychopathol, 2002.PMID 11893092
- [9]Colins O, Vermeiren R, Vreugdenhil C, et al. Psychiatric disorders in detained male adolescents: a systematic literature review Can J Psychiatry, 2010.PMID 20416149
- [10]Curtis NM, Ronan KR, Borduin CM Multisystemic treatment: a meta-analysis of outcome studies J Fam Psychol, 2004.PMID 15382965
- [11]Henggeler SW, Schaeffer CM Multisystemic Therapy: Clinical Overview, Outcomes, and Implementation Research Fam Process, 2016.PMID 27370172
- [12]Littell JH, Pigott TD, Nilsen KH, et al. Functional Family Therapy for families of youth (age 11-18) with behaviour problems: A systematic review and meta-analysis Campbell Syst Rev, 2023.PMID 37475879
- [13]Olsson TM, Långström N, Skoog T, et al. Systematic review and meta-analysis of noninstitutional psychosocial interventions to prevent juvenile criminal recidivism J Consult Clin Psychol, 2021.PMID 34264699
- [14]Lodewijks HP, Doreleijers TA, de Ruiter C, Borum R Predictive validity of the Structured Assessment of Violence Risk in Youth (SAVRY) during residential treatment Int J Law Psychiatry, 2008.PMID 18508122
- [15]Dalsgaard S, Mortensen PB, Frydenberg M, Thomsen PH Long-term criminal outcome of children with attention deficit hyperactivity disorder Crim Behav Ment Health, 2013.PMID 23576439
- [16]Underwood LA, Washington A Mental Illness and Juvenile Offenders Int J Environ Res Public Health, 2016.PMID 26901213