Psych · Foundations — developmental science
Attachment theory and early relationships
Also known as Attachment theory · Strange Situation · Adult Attachment Interview · Secure base · Internal working models · Reactive attachment disorder · Disinhibited social engagement disorder · Attachment styles
Exam-exhaustive fellowship reference on attachment theory — Bowlby secure base/safe haven, Ainsworth Strange Situation patterns (secure/insecure/disorganised), Adult Attachment Interview states of mind, internal working models and mentalization, clinical implications for personality/trauma/parenting, and the critical distinction between attachment styles and DSM/ICD attachment disorders (RAD/DSED). FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
2 MCQs with explanations
Target exams
Red flags
Attachment theory is foundational for FRANZCP/MRCPsych developmental and psychotherapy stations. Examiners punish three errors: treating every relationship problem as an attachment disorder, treating insecure style as destiny, and endorsing coercive attachment therapies.[15][17]
Definition and core constructs
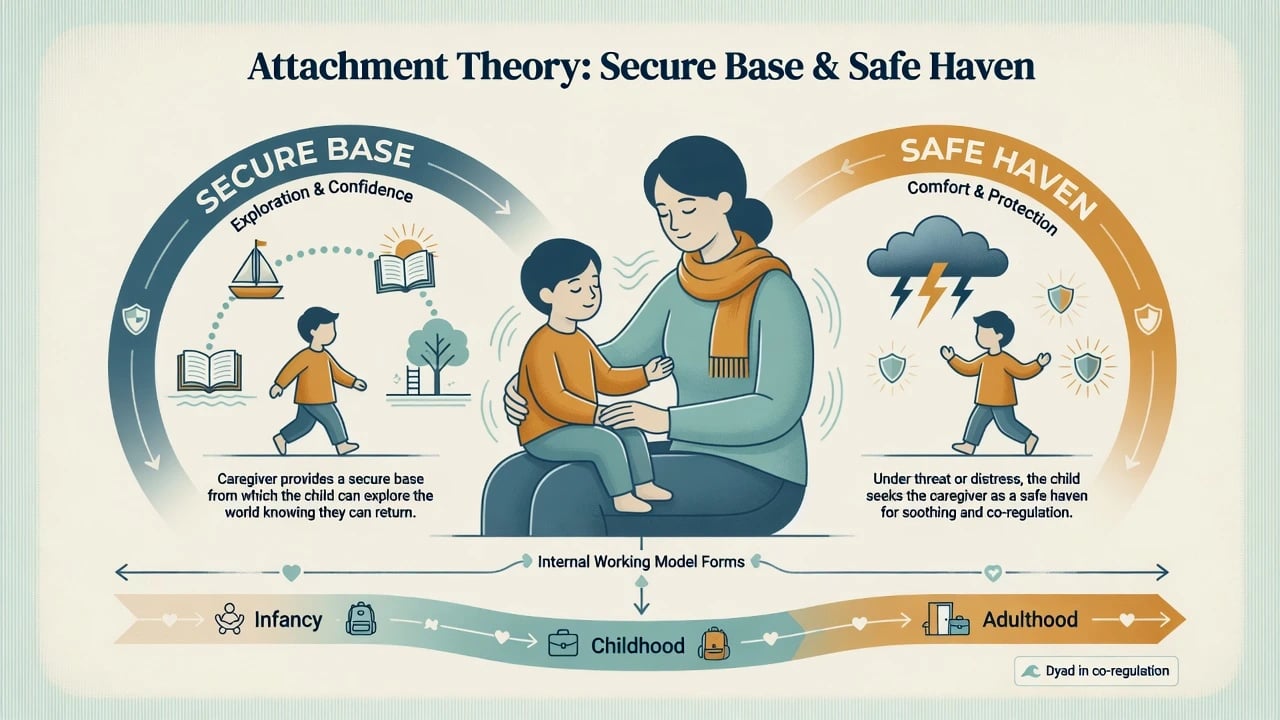
Bowlby framed attachment as a species-typical behavioural system selected to protect the young by maintaining proximity to a stronger, wiser figure when danger is signalled.[1][2] Caregivers function as:
- Secure base — a reliable platform from which the child explores the environment.
- Safe haven — a destination for comfort and co-regulation when distressed or threatened.[1][2]
Internal working models (IWMs) are cognitive–affective templates of “Am I worthy of care?” and “Are others available/responsive?” built from repeated interaction. They bias attention, emotion regulation, help-seeking, and later intimate relationships, while remaining open to revision through new relational experience (earned security).[2][3]
Bowlby’s developmental psychiatry writing argued that early relationship experience must be integrated with psychopathology without reducing adult illness to a single childhood event — the balanced stance expected at fellowship viva.[3]
Classification: infant patterns (Strange Situation)
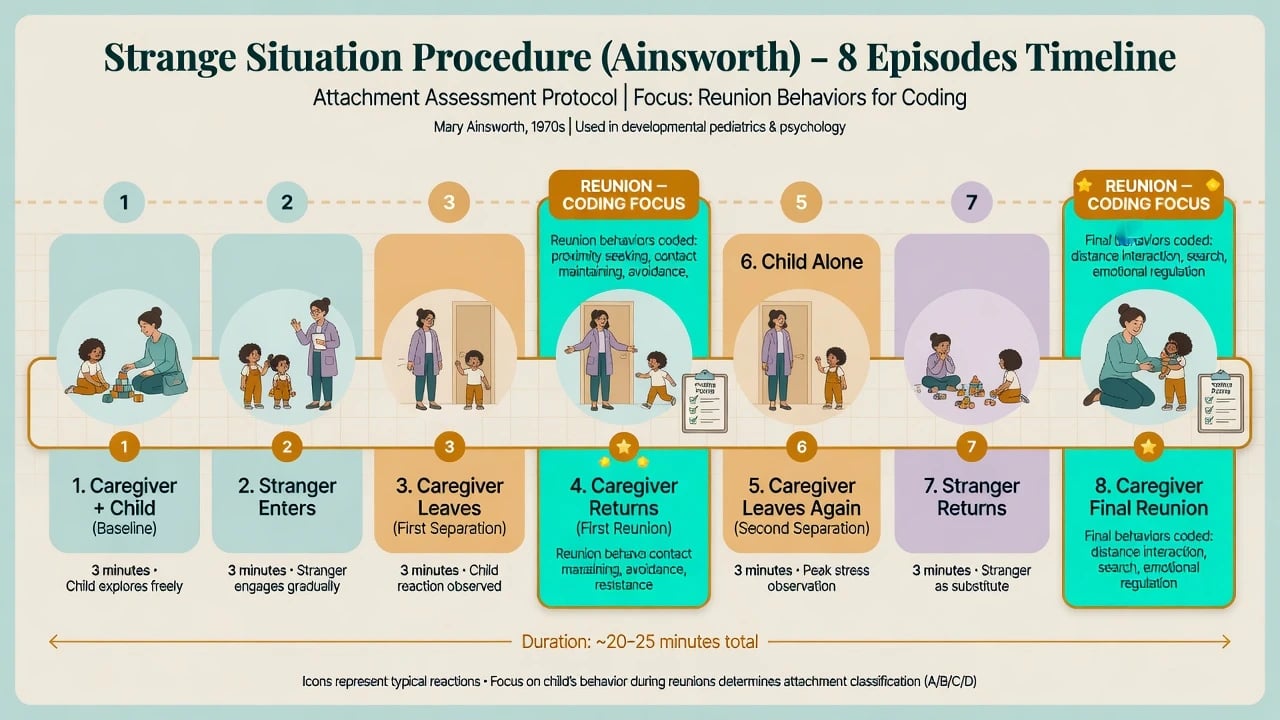
Mary Ainsworth’s observational programme established that attachment quality is visible in reunion behaviour after brief separations in a standardised laboratory protocol (Strange Situation Procedure, SSP), typically for infants around 12–18 months.[4]
Strange Situation Procedure (exam-level map)
Episodes alternate caregiver presence, stranger entry, separation, and reunion over roughly 20 minutes. Coding focuses on reunions, not how loudly the child cries in separation alone.[4]
A / B / C / D patterns
| Pattern | Classic label | Reunion strategy (simplified) | Caregiving association (probabilistic) |
|---|---|---|---|
| B | Secure | Seeks proximity/contact, soothes, returns to play | Sensitive, contingent, warm |
| A | Insecure-avoidant | Minimises distress, turns to environment, limited contact | Historically linked with rejecting or overstimulating care |
| C | Insecure-resistant / ambivalent | Intense distress, clingy/angry, hard to settle | Inconsistent responsiveness |
| D | Disorganised / disoriented | Contradictory, freezing, apprehension, collapse of strategy | Frightened/frightening care; unresolved caregiver trauma/loss; maltreatment risk |
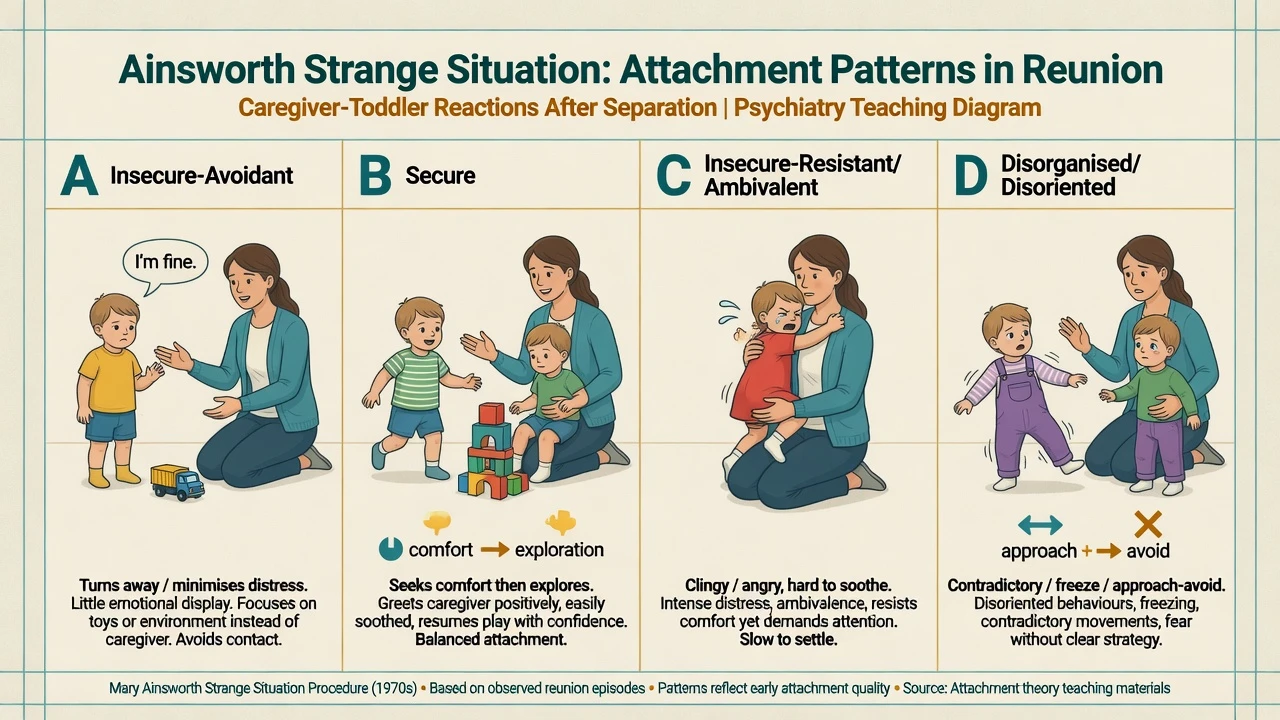
Disorganisation is not “the most severe avoidant type.” It is a collapse or contradiction of strategy — simultaneous approach and avoidance, freezing, stereotypies, or fearful orientation to the caregiver who is also the source of alarm.[6][8] Consensus reviews treat D as a clinically important risk marker and research construct, not a freestanding diagnosis of the child.[8]
Adult attachment: AAI and self-report styles
Adult Attachment Interview (AAI)
The AAI is a semi-structured interview about childhood experiences and their meaning. Classification rests on discourse coherence — how the story is told — not simply whether childhood was “good” or “bad.”[6]
| AAI state of mind | Code | Discourse markers (exam level) |
|---|---|---|
| Autonomous / secure | F | Coherent, balanced, collaborative; values attachment; specific examples |
| Dismissing | Ds | Minimises importance of attachment; idealises with sparse evidence; insistence on lack of memory |
| Preoccupied | E | Entangled, angry or passive; long run-on speech; still caught in past grievances |
| Unresolved / disorganised | U/d | Lapses in monitoring of reasoning or discourse specifically around loss or trauma |
| Cannot classify | CC | Mixed/contradictory strategies without a single dominant organised pattern |
Self-report adult styles (Hazan–Shaver and derivatives)
Hazan and Shaver conceptualised romantic love as an attachment process, opening a parallel adult literature of secure, anxious/preoccupied, and avoidant styles (later expanded to an anxiety × avoidance space including fearful avoidance).[5]
- Interview discourse about childhood attachment experiences
- Strong developmental research tradition linking caregiver state of mind to infant security
- Unresolved status is about lapses around loss/trauma, not general anxiety
- Questionnaires about current close relationships (anxiety and avoidance dimensions)
- Efficient; useful for formulation and couple-distress research
- Do not automatically equal childhood SSP classification or AAI code
- Prefer dimensional curiosity over pejorative labels in notes
- Use attachment language to explain help-seeking, alliance ruptures, and parenting
- Do not treat a questionnaire score as a formal diagnosis

Mechanisms: sensitivity, transmission, mentalization
Proximal caregiving mechanisms
Sensitivity — noticing, correctly interpreting, and contingently responding to infant signals — is the classic pathway to security.[4] Frightened or frightening parental behaviour links unresolved parental loss/trauma to infant disorganisation — name this pathway in viva.[7][6]
Mentalization / reflective function
Fonagy and Target linked attachment security to the development of reflective function — understanding behaviour in terms of intentional mental states (feelings, beliefs, desires).[9] Adversity and attachment disruption can impair mentalizing under interpersonal stress, contributing to emotion dysregulation and interpersonal hypersensitivity in borderline personality pathways.[10][11][12]
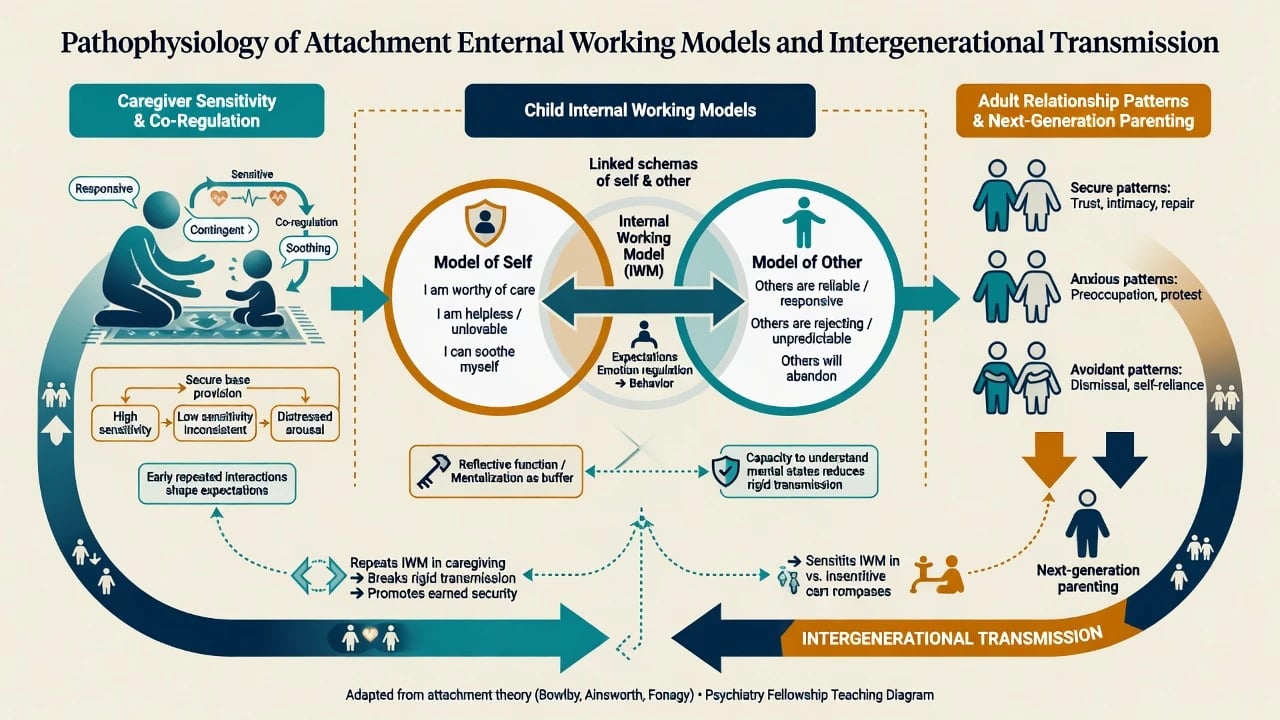
Exam mechanism sentence: inconsistent care builds ambivalent IWMs; rejection builds deactivating (avoidant) strategies; frightened/frightening care collapses strategy into disorganisation; mentalization failure under stress amplifies interpersonal crises in adulthood.[6][9][11]
Epidemiology and developmental risk
In normative samples, secure classification is typically the modal infant pattern; rates of avoidant versus resistant patterns vary by culture and sample, while disorganisation rises sharply with maltreatment and institutional care.[4][8][18]
Meta-analytic evidence links insecure and especially disorganised attachment to externalising behaviour problems; insecure and disorganised patterns also show associations with internalizing symptoms. Effect sizes are meaningful but not destiny — moderators and later experience matter.[13][14]
Severe early psychosocial deprivation (illustrated by the Bucharest Early Intervention Project tradition) disrupts attachment organisation and demonstrates that high-quality foster care, especially earlier, improves attachment and developmental outcomes compared with prolonged institutional care.[18]
Clinical presentations
Secure organisation
Effective help-seeking when distressed; capacity for repair after rupture; coherent narrative about relationships; flexible exploration when safe.[1][4]
Avoidant / dismissing presentations
Minimised affect; preference for self-reliance; sparse autobiographical detail; idealisation without supporting memories (AAI). In clinic: late presentation, under-reporting of need, abrupt disengagement when intimacy rises.[4][6]
Resistant / preoccupied presentations
Heightened distress signalling; anger or passive entanglement; difficulty settling after comfort. In adult clinic: crisis-prone help-seeking, fear of abandonment alternating with protest, long unresolved relational narratives.[4][6]
Disorganised / unresolved presentations
Contradictory strategies in childhood; adult discourse lapses around loss/trauma; dissociation cues under stress. Clinically often co-travels with complex trauma histories — still formulate carefully, do not equate U/d with a single DSM diagnosis.[6][8][11]
Attachment disorders vs attachment styles (high-yield)
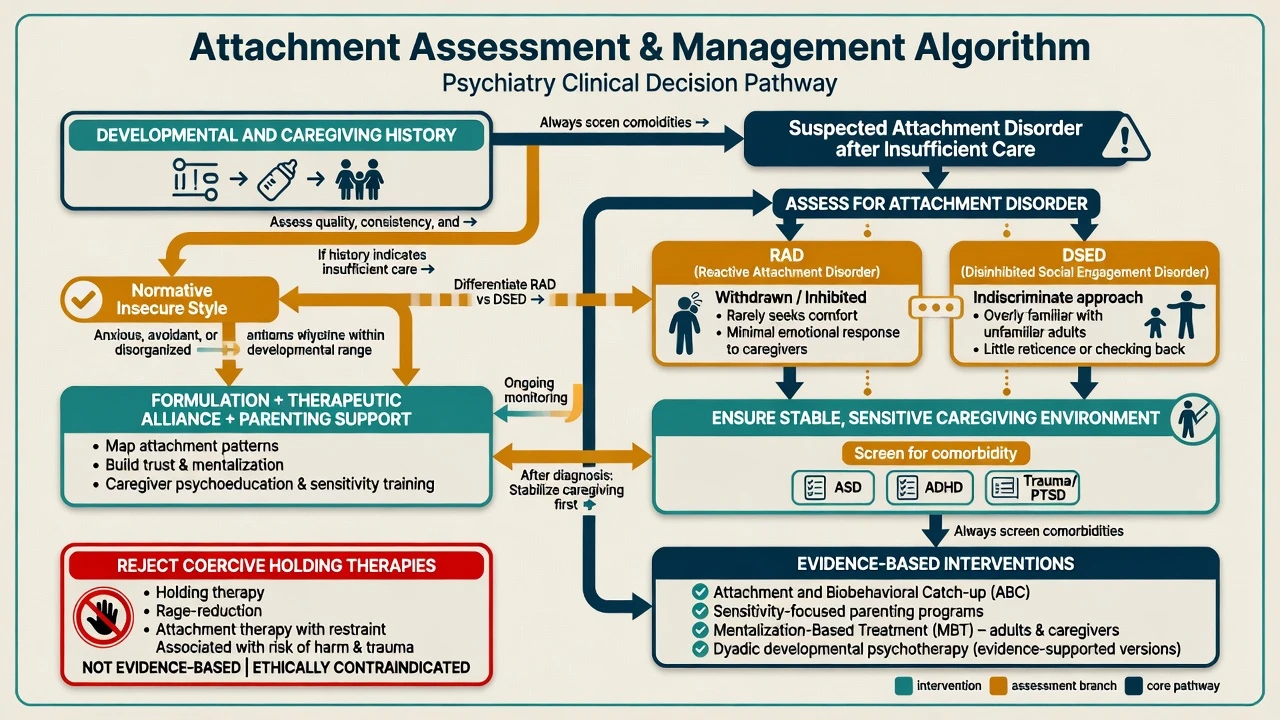
This is the single most examinable distinction: styles/patterns describe organised strategies and mental models, whereas RAD and DSED are clinical disorders that require a history of insufficient care plus specific phenotypes.[15][16][17]
| Attachment styles / patterns | Attachment disorders (RAD / DSED) | |
|---|---|---|
| What they are | Organised (or disorganised) strategies and mental models within the normal–risk continuum | DSM-5-TR / ICD-11 clinical disorders after insufficient care |
| Prevalence context | Common dimensional variation | Rare in general community; concentrated after severe neglect/institutional rearing |
| Core requirement | Observed strategy / discourse pattern | Pathogenic care history plus specific symptom clusters |
| Examples | Secure, avoidant, resistant, disorganised; AAI F/Ds/E/U | Emotionally withdrawn/inhibited (RAD); indiscriminate social approach (DSED) |
| Treatment focus | Formulation, alliance, parenting sensitivity, mentalization | Stabilise caregiving first; treat comorbidity; evidence-based dyadic/parenting work |
Reactive Attachment Disorder (RAD)
Emotionally withdrawn/inhibited pattern in young children: rarely seeks or responds to comfort, limited positive affect, unexplained irritability/sadness/fearfulness in nonthreatening interactions, in the context of extremes of insufficient care.[15][16]
Disinhibited Social Engagement Disorder (DSED)
Indiscriminate sociability: reduced reticence with unfamiliar adults, overly familiar verbal/physical behaviour, diminished checking back after venturing away, willingness to go off with strangers — again after insufficient care. DSED signs may be more persistent than RAD after placement improvement.[15][16][18]
Evidence-derived criteria support separating withdrawn/inhibited and indiscriminately social/disinhibited phenotypes rather than lumping all “attachment problems” together.[16]
Differential diagnosis (discriminators)
- ASD vs RAD/DSED: ASD has pervasive social-communication differences and restricted/repetitive behaviours independent of a single care history; RAD/DSED require pathogenic care and more selective attachment-related social abnormalities. Both can co-occur after institutional care — assess both.[15][16]
- ADHD social impulsivity vs DSED: ADHD impulsivity is broader and not defined by lack of reticence after insufficient care; still screen both.[15]
- PTSD / complex trauma vs unresolved AAI: related clinical territories; unresolved AAI is a discourse classification, not a trauma diagnosis.[6][11]
- Personality disorder vs adult attachment insecurity: attachment informs mechanisms and therapy stance; it does not replace PD diagnosis when criteria are met.[10][12]
- Cultural caregiving variation vs pathology: cross-cultural work warns against ethnocentric norms for physical closeness, multi-caregiver systems, or separation practices.[4][8]
Assessment
History that feeds attachment formulation
Structure developmental and caregiving history: pregnancy wantedness, postnatal mental health, separations, hospitalisations, foster/adoptive placements, institutional care, domestic violence, parental substance use, maltreatment, multiple caregivers, and current support network.[15][18]
Observation
In clinic, watch caregiver–child contingency, hostility, frightened/frightening behaviours, repair after rupture, and the child’s use of the caregiver as a secure base.[4][7]
Structured tools (know purpose and limits)
- SSP — research/gold-standard observational classification in infancy; not a routine outpatient “test” you order like a TSH.[4]
- AAI — specialised interview requiring training for formal coding; clinically, discourse features still inform formulation.[6]
- Self-report inventories — efficient for adult style dimensions; interpret as hypotheses.[5]
- RAD/DSED assessment — structured history of care quality plus multi-setting observation; AACAP practice parameter principles.[15]
There is no laboratory test for attachment pattern. Investigate organic/developmental differentials when indicated (hearing, language, cognitive assessment, ASD evaluation, medical sequelae of neglect).[15]
Acute management and safeguarding
Acute priorities override elegant attachment formulation: medical stabilisation, suicide/violence risk, and child protection thresholds when maltreatment or severe neglect is suspected. Statutes and reporting duties are jurisdiction-specific — know your local law, do not invent section numbers in exams without being asked for a named jurisdiction.[15][17]
Definitive management
Principles for attachment disorders
AACAP practice parameter core: ensure a stable, emotionally available caregiver; improve caregiver sensitivity; treat comorbid conditions; avoid pathologising the child as the sole problem.[15] Placement stability and reducing repeated disruptions are therapeutic, not “social work only.”[18]
Evidence-aligned interventions (name, do not invent doses)
- Sensitivity-focused parenting programmes and video-feedback approaches targeting caregiver responsiveness.[8][15]
- Attachment and Biobehavioral Catch-up (ABC) tradition — brief home-visiting model improving caregiving and reducing disorganisation risk in high-risk samples (cite as named intervention class; local availability varies).[8][18]
- Infant–parent / dyadic psychotherapies when trauma, parental mental illness, or relational rupture maintains insecurity.[15]
- Mentalization-based treatment (MBT) and a mentalizing clinical stance for adult personality/trauma presentations grounded in attachment theory.[11][12]
Pharmacotherapy
No medication treats attachment pattern or RAD/DSED as primary targets. Use psychotropics only for clearly indicated comorbid conditions (e.g. ADHD, severe anxiety, depression, psychosis), with usual monitoring — attachment work remains environmental and relational.[15]
Therapeutic relationship as secure base
In adult psychiatry, a predictable, boundaried, non-retaliatory clinician can function as a temporary secure base, allowing exploration of mental states and repair of ruptures — especially relevant in borderline and complex trauma care.[10][11][12]
Subtypes and clinical scenarios
Personality disorder and complex trauma
Attachment adversity and mentalizing impairment are central developmental accounts of borderline personality disorder; treatment models that restore mentalizing under stress are attachment-informed even when not labelled “attachment therapy.”[10][12]
Perinatal psychiatry
Parental unresolved loss/trauma and low reflective function raise intergenerational risk; support parental mental health and reflective parenting to protect infant security.[7][9]
Looked-after, foster, and post-institutional children
BEIP lessons: earlier high-quality family-based care improves attachment organisation versus prolonged institutional rearing; DSED features may linger and need specific social-boundary coaching alongside caregiving quality.[18][15]
Forensic interface
Attachment history may inform formulation of interpersonal risk contexts, but do not use style alone to predict violence or sexual offending. Use structured professional judgement tools where indicated and keep legal thresholds jurisdiction-specific; attachment labels are not risk instruments and must not replace safeguarding assessment.[8][15][17]
Complications and pitfalls
- Moralising insecure parents or pathologising cultural caregiving norms.[8]
- Missing autism/ADHD while over-diagnosing attachment disorder.[15]
- Missing maltreatment while calling everything “attachment issues.”[17]
- Iatrogenic harm from coercive attachment therapies.[17]
- Assuming lifelong fixity — developmental discontinuity and earned security occur.[2][3][18]
- Confusing adult self-report style with childhood SSP classification.[5][6]
Prognosis and disposition
Attachment patterns show both stability and lawful change. Intervention that improves caregiver sensitivity and placement stability can shift trajectories; institutional deprivation recovery is greater with earlier high-quality foster care.[8][18] Disposition priorities: protect the child, stabilise caregivers, treat parental psychiatric illness, reduce placement breakdown, and plan multi-agency support where needed.[15]
Special populations
- Infants/toddlers: highest leverage for sensitive caregiving and SSP-relevant observation.[4]
- School-age/adolescents: representational measures, peer/romantic transfer of IWMs.[5]
- Older adults: attachment strategies still shape help-seeking, grief, and care dependence across the lifespan working-model framework.[1][2]
- Intellectual disability: adapt assessment; do not over-interpret atypical social behaviour as DSED without care-history criteria.[15]
- Indigenous and culturally diverse families: use cultural humility; multi-caregiver systems are not automatically pathogenic.[8]
Evidence and guidelines (exam anchors)
| Anchor | Why examiners care |
|---|---|
| Bowlby affectional bonds / developmental psychiatry | Theoretical foundation of secure base, loss, and psychopathology links |
| Ainsworth patterns | Operational infant classification |
| Main/Hesse disorganisation; Schuengel frightening behaviour | Mechanism of D and intergenerational unresolved trauma |
| Fearon / Groh meta-analyses | Psychopathology pathway effect sizes |
| Fonagy reflective function / mentalizing | Bridge to adult PD and psychotherapy |
| Zeanah AACAP Practice Parameter | RAD/DSED assessment and treatment principles |
| APSAC task force | Reject harmful attachment therapies |
| BEIP tradition | Causal evidence on deprivation vs foster care for attachment |
Exam pearls
Attachment exam anchors
- Unresolved AAI status hinges on discourse lapses around loss/trauma, not general life stress.[6]
- DSED is not “a friendly child” as a strength — it is impaired social boundary after deprivation.[15][16]
- Attachment informs formulation and alliance; it does not replace risk assessment, capacity assessment, or diagnosis.[3][15]
- Cross-cultural rule: secure is modal; A/C ratios vary — do not pathologise culture.[4][8]
Worked micro-formulation (exam style)
Presenting problem: 16-year-old with self-harm, chaotic relationships, and crisis-driven service use after multiple foster placements and early neglect.[15][18]
Attachment lens: early insufficient care → disrupted secure base; possible DSED traits historically and unresolved relational trauma now; mentalizing collapses under rejection cues; self-harm as affect regulation and proximity protest.[11][12][15]
Plan implications: stable keyworker (secure base), mentalization-focused therapy, caregiver/network psychoeducation, treat depression/PTSD if present, explicit rejection of coercive therapies, multi-agency placement stability work.[11][12][15][17][18]
References
- [1]Bowlby J The making and breaking of affectional bonds. I. Aetiology and psychopathology in the light of attachment theory. An expanded version of the Fiftieth Maudsley Lecture, delivered before the Royal College of Psychiatrists, 19 November 1976 Br J Psychiatry, 1977.PMID 843768
- [2]Bowlby J Attachment and loss: retrospect and prospect Am J Orthopsychiatry, 1982.PMID 7148988
- [3]Bowlby J Developmental psychiatry comes of age Am J Psychiatry, 1988.PMID 3276225
- [4]Ainsworth MD Patterns of infant-mother attachments: antecedents and effects on development Bull N Y Acad Med, 1985.PMID 3864510
- [5]Hazan C, Shaver P Romantic love conceptualized as an attachment process J Pers Soc Psychol, 1987.PMID 3572722
- [6]Hesse E, Main M Disorganized infant, child, and adult attachment: collapse in behavioral and attentional strategies J Am Psychoanal Assoc, 2000.PMID 11212184
- [7]Schuengel C, Bakermans-Kranenburg MJ, Van IJzendoorn MH Frightening maternal behavior linking unresolved loss and disorganized infant attachment J Consult Clin Psychol, 1999.PMID 10028209
- [8]Granqvist P, Sroufe LA, Dozier M, et al. Disorganized attachment in infancy: a review of the phenomenon and its implications for clinicians and policy-makers Attach Hum Dev, 2017.PMID 28745146
- [9]Fonagy P, Target M Attachment and reflective function: their role in self-organization Dev Psychopathol, 1997.PMID 9449001
- [10]Fonagy P, Target M, Gergely G, et al. Attachment and borderline personality disorder. A theory and some evidence Psychiatr Clin North Am, 2000.PMID 10729934
- [11]Fonagy P, Bateman AW Adversity, attachment, and mentalizing Compr Psychiatry, 2016.PMID 26654293
- [12]Fonagy P, Luyten P A developmental, mentalization-based approach to the understanding and treatment of borderline personality disorder Dev Psychopathol, 2009.PMID 19825272
- [13]Fearon RP, Bakermans-Kranenburg MJ, van Ijzendoorn MH, et al. The significance of insecure attachment and disorganization in the development of children's externalizing behavior: a meta-analytic study Child Dev, 2010.PMID 20438450
- [14]Groh AM, Roisman GI, van Ijzendoorn MH, et al. The significance of insecure and disorganized attachment for children's internalizing symptoms: a meta-analytic study Child Dev, 2012.PMID 22235928
- [15]Zeanah CH, Chesher T, Boris NW Practice Parameter for the Assessment and Treatment of Children and Adolescents With Reactive Attachment Disorder and Disinhibited Social Engagement Disorder J Am Acad Child Adolesc Psychiatry, 2016.PMID 27806867
- [16]Gleason MM, Fox NA, Drury S, et al. Validity of evidence-derived criteria for reactive attachment disorder: indiscriminately social/disinhibited and emotionally withdrawn/inhibited types J Am Acad Child Adolesc Psychiatry, 2011.PMID 21334562
- [17]Chaffin M, Hanson R, Saunders BE, et al. Report of the APSAC task force on attachment therapy, reactive attachment disorder, and attachment problems Child Maltreat, 2006.PMID 16382093
- [18]Fox NA, Nelson CA 3rd, Zeanah CH The Effects of Psychosocial Deprivation on Attachment: Lessons from the Bucharest Early Intervention Project Psychodyn Psychiatry, 2017.PMID 29244624