Psych · Foundations — cognitive psychology
Cognitive psychology for psychiatry
Also known as Information processing psychiatry · Attention memory executive function · Working memory Baddeley · Cognitive biases psychopathology · Social cognition schizophrenia · MATRICS cognitive domains · Dual-process heuristics · Cognitive models CBT foundations
Exam-exhaustive fellowship reference on cognitive psychology for psychiatrists — attention networks, working and long-term memory, executive functions, dual-process judgment, cognitive models of depression and panic, overgeneral memory, schizophrenia cognition and social cognition, bedside assessment, CBT and remediation applications. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview
Cognitive science is core MRCPsych Paper A / FRANZCP foundational theory and the shared vocabulary of cognitive therapy, neuropsychology liaison, and psychosis rehabilitation. A candidate who masters this page should discriminate working-memory failure from “laziness,” design a behavioural experiment that tests a prediction rather than a vague homework task, and explain why verbal learning and social cognition predict community function better than residual positive symptoms alone.[2][12][14]
Definition and classification
Cognitive psychology is the scientific study of how people attend, encode, store, retrieve, reason, decide, and understand others. In psychiatry it supplies (1) models of symptom maintenance, (2) constructs for bedside and formal assessment, and (3) targets for CBT, remediation, and environmental supports.[2][8]
Core domains examiners test
| Domain | High-yield units | Clinical anchor |
|---|---|---|
| Attention | Selective, divided, sustained; Posner alerting/orienting/executive | Hypervigilance, distractibility, dual-task failure |
| Working memory | Phonological loop, visuospatial sketchpad, central executive, episodic buffer | Losing conversational thread; multi-step instructions fail |
| Long-term memory | Episodic, semantic, procedural/implicit | Overgeneral autobiographical recall; skill preservation |
| Executive function | Updating, shifting, inhibition (Miyake); planning/monitoring | Disorganisation, perseveration, impulsivity |
| Judgment | Heuristics and dual-process thinking | Clinical and patient decision traps |
| Social cognition | Emotion processing, theory of mind, attribution, social perception | Misreading intent; interpersonal disability |
Attention
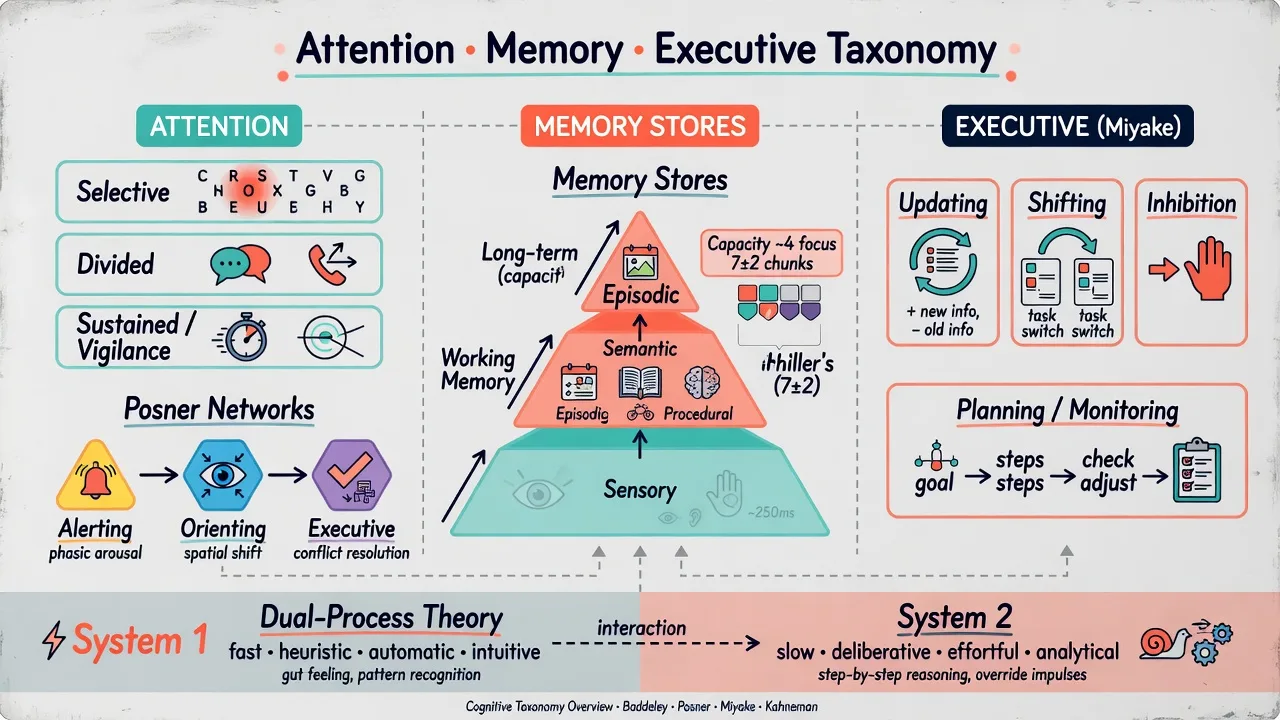
- Selective attention prioritises task-relevant input and filters competitors — threat bias in anxiety is selective attention gone clinical.
- Divided attention supports dual-task performance; failure appears when patients cannot talk while packing, or drive while using phone.
- Sustained attention / vigilance maintains readiness over time — impaired in ADHD, delirium, and many psychoses.
- Posner networks: alerting (readiness), orienting (spatial shift), executive (conflict resolution) provide a neural-cognitive map still used in exam teaching.[4]
Capacity limits and working memory
Miller’s classic 7±2 describes approximate limits on immediate memory when material is organised into chunks.[1] Cowan’s reconsideration emphasises a smaller pure focus of attention (~4 items) when chunking and long-term memory supports are constrained.[3] Examiners love stems that distinguish “chunked capacity” from pure storage span.
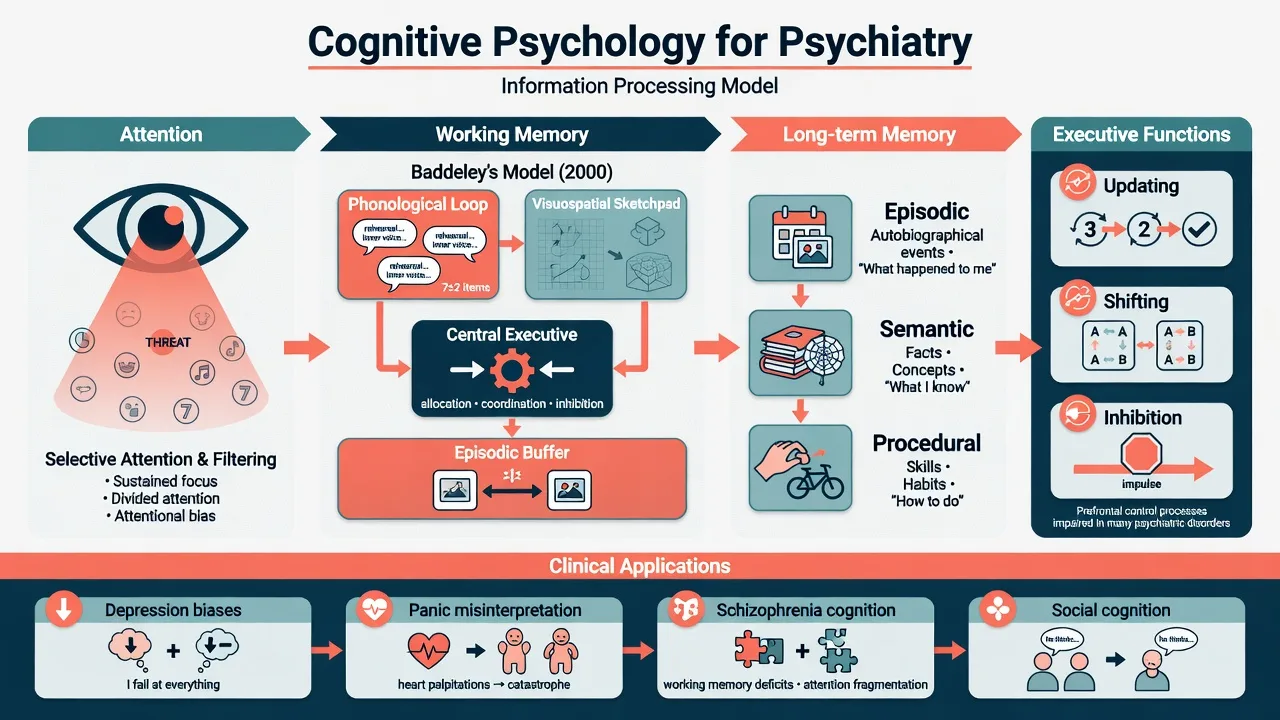
Baddeley’s multi-component working memory remains the fellowship standard: a central executive coordinating a phonological loop, visuospatial sketchpad, and episodic buffer that binds multimodal episodes for conscious manipulation — not a single short-term “box.”[2]
Long-term memory systems
- Episodic: personally timed events (“what happened to me”).
- Semantic: facts and concepts (“what I know”).
- Procedural/implicit: skills and habits (“how I do”) — often relatively preserved when declarative systems fail. Overgeneral (category-level) autobiographical retrieval is a key affective-disorder marker rather than simple amnesia.[11]
Executive functions (Miyake)
Latent-variable work supports unity and diversity: three related but separable functions — updating working-memory contents, shifting mental sets, and inhibition of prepotent responses — plus planning/monitoring as higher-order applications.[5] Saying only “frontal lobe dysfunction” without naming these processes is an undergraduate answer.
Dual-process judgment and heuristics
Tversky and Kahneman described systematic heuristics under uncertainty: representativeness, availability, and anchoring-and-adjustment — biases that distort both patient appraisal and clinician reasoning.[6] Dual-process teaching frames fast automatic (System 1) vs slow deliberative (System 2) thinking; heuristics are efficient until base rates, sample size, or regression to the mean are ignored.
Pathophysiology and clinical mechanisms
Information-processing chain
Stimulus → attention → encoding into working memory → consolidation/retrieval in long-term stores, all gated by executive control. Bottlenecks (capacity, threat bias, executive load) produce the clinical phenotypes of distractibility, forgetting multi-step plans, and rigid thinking.[2][4][5]
Beck’s cognitive model of depression
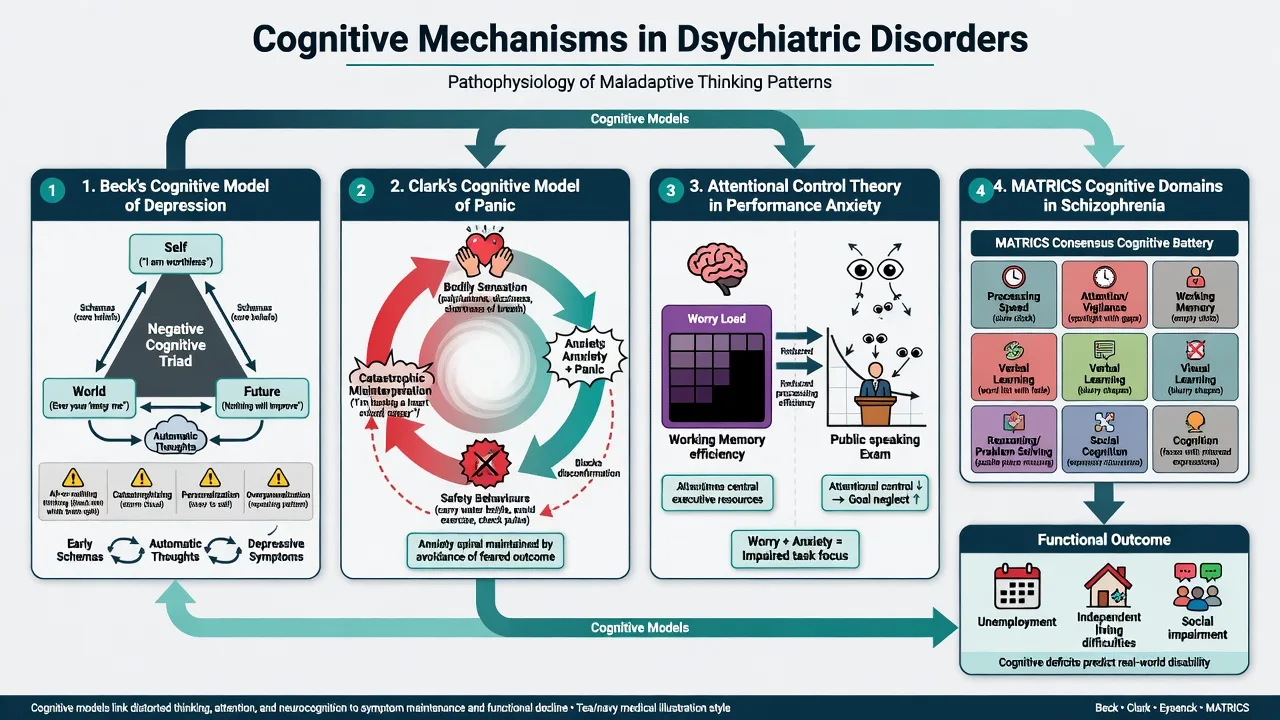
Beck’s model evolved from early formulations of distorted thinking and therapy to a layered architecture of automatic thoughts, intermediate beliefs, core schemas, and the cognitive triad (self, world, future), later integrated with neurobiological correlates.[7][8] Classic distortions (all-or-nothing thinking, catastrophising, personalisation, overgeneralisation) are examinable content, not optional jargon.
Clark’s cognitive model of panic
Panic is maintained by catastrophic misinterpretation of bodily sensations plus safety behaviours that prevent disconfirmation of threat beliefs (e.g. sitting down, carrying unused benzodiazepine, checking pulse).[9] This is cognitive science wearing a clinical coat — the same collaborative empiricism that drives behavioural experiments.
Anxiety and performance — attentional control theory
Attentional control theory holds that anxiety often impairs processing efficiency (more effort for the same accuracy) via worry loading the central executive, with goal-directed attentional control reduced and stimulus-driven attention relatively increased under threat.[10] Effectiveness may be preserved until load is high — the exam distinction between “can do it with huge effort” and true incompetence.
Overgeneral autobiographical memory
Emotionally disordered patients frequently retrieve categories of events rather than specific episodes; reduced specificity associates with depression, trauma-related conditions, and impaired problem-solving about the personal past and future.[11]
Schizophrenia cognition and social cognition
Green’s synthesis established that neurocognitive deficits — especially secondary verbal memory and related domains — carry functional consequences for community outcome beyond positive symptoms alone.[12] Consensus factor work supporting MATRICS-style batteries identified separable domains including speed of processing, attention/vigilance, working memory, verbal and visual learning, reasoning/problem solving, and social cognition.[13] Keefe and Harvey summarise the profile as spanning attention, memory, reasoning, and processing speed as core illness features, not mere medication artefacts.[15] An NIMH workshop formalised social cognition domains (emotion processing, theory of mind/mentalising, attributional style, social perception) as assessment and research priorities.[14]
Clinical presentation (how cognition shows up)
- Attention: threat spotting, startle to phone buzz, cannot finish forms in busy clinics.
- Working memory: loses the second half of a three-part instruction; “I forget mid-sentence.”
- Executive: unfinished tasks, rigid routines, impulsive replies, poor sequencing of self-care.
- Biased content: negative automatic thoughts; catastrophic bodily appraisals; hostile attribution in paranoia-spectrum presentations.
- Memory style: “always been a failure” (overgeneral) rather than dated episodes.
- Social cognition: misses sarcasm, misreads neutral faces as hostile, concrete answers to proverb/mental-state questions. These signs should be recorded as cognitive phenomenology, not only as “insight” or “personality.”[8][9][11][14]
Differential — process discrimination
| Presentation | Cognitive frame | Competing frame | Exam action |
|---|---|---|---|
| Missed appointments and forms | WM/executive load; instruction complexity | Avoidance; secondary gain | Simplify plans; test capacity for multi-step tasks |
| Blank mind in exams/interviews | ACT: efficiency loss under anxiety load | Global intellectual disability | Reduce dual-task load; retest when calm |
| Can't work despite 'stable positive symptoms' | Verbal memory / processing speed / social cognition | Laziness; family expressed emotion alone | Screen cognition; rehab referral |
| Vague past history | Overgeneral autobiographical memory | Dissimulation only | Cue for specificity; consider depression/trauma |
| Fluctuating focus over hours | Delirium / medical | Primary ADHD only | Medical work-up first |
Also discriminate depression-related cognitive complaints from major neurocognitive disorder, and ADHD from anxiety-driven concentration failure — complementary assessments, not single labels.[10][11]
Bedside assessment
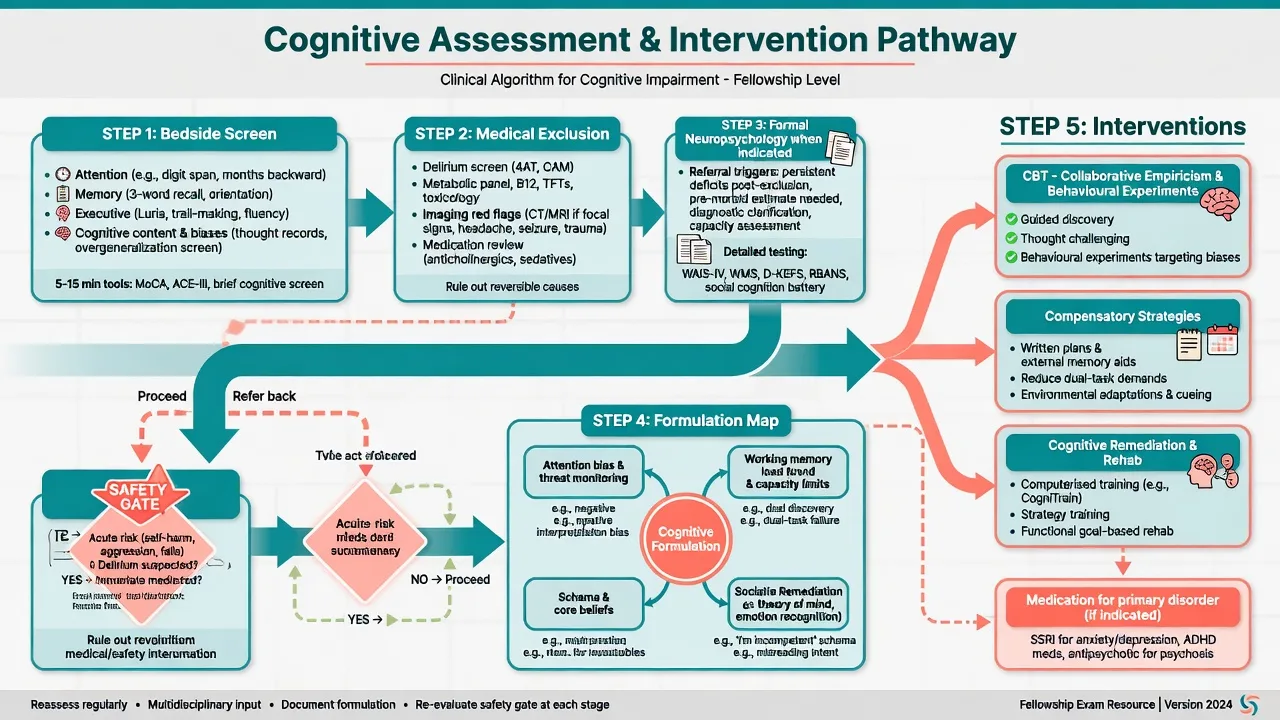
- Orientation and attention (months reverse, digit span, vigilance to conversation).
- Registration and delayed recall (3–5 words); note encoding vs retrieval pattern.
- Working memory probes (spell reverse, serial subtraction) with education/language caveats.
- Executive (clock, verbal fluency, Luria-type sequencing, proverb/abstraction carefully).
- Cognitive content: automatic thoughts, threat expectancies, safety behaviours.[9]
- Social cognition bedside: emotion labelling, simple false-belief/irony probes where culturally valid.[14]
- Functional history and collateral — work, money, meds, technology, driving.
- Brief tools (e.g. MoCA) when indicated; know ceiling/floor and education effects.
- Refer formal neuropsychology for diagnostic clarification, baseline before rehab, medico-legal, or treatment-resistant functional failure.
- Capacity lens: understand, retain, weigh, communicate — each maps to attention/WM/executive integrity. Assessment thus operationalises process before technique choice.[2][5][12]
Investigations
No blood test diagnoses a cognitive bias. Investigate delirium and reversible causes when attention fluctuates: metabolic panel, B12/folate/TFTs as indicated, toxicology, medication review (anticholinergics, sedatives), imaging/EEG for focal signs, seizure concern, or encephalitis red flags. Formal batteries in psychosis programmes often sample MATRICS-like domains; therapy process measures (thought records, homework quality, expectancy logs) test formulation continuously.[12][13][15]
Acute / emergency management
Stabilisation can still use cognitive supports: one instruction at a time, written plans, reduce dual-task load, remove lethal means, involve carers as external executive aids — matching limited working-memory and executive capacity under acute load.[2][10]
Definitive management (application)
CBT as applied cognitive science
Collaborative empiricism, guided discovery, cognitive restructuring, and behavioural experiments (predict → test → review) are direct applications of information-processing models. Meta-analytic CBT efficacy literature supports these packages across many disorders; mechanism teaching still needs Beck/Clark precision rather than generic “talk therapy.”[7][8][9]
Attention and threat bias work
Fade safety behaviours that block disconfirmation; train attention away from exclusive threat monitoring when indicated; design exposures/experiments that violate catastrophic expectancies (links to learning-theory topic).[9][10]
Memory-informed care
Cue specific autobiographical retrieval when overgenerality dominates problem-solving; structure trauma-focused work within competent protocols; use spaced retrieval and external memory aids for encoding failures.[11]
Schizophrenia: remediation and compensation
Cognitive remediation, strategy coaching, supported employment/education, and environmental simplification target domains that drive function; social cognition training addresses mentalising and emotion processing gaps.[12][14][15] Antipsychotics treat psychosis but are not a full cognitive cure — set realistic shared goals.
Compensatory toolkit
Written step lists, single-task instructions, phone reminders, pill organisers, quieter interview rooms, shorter sessions with teach-back — cheap interventions that respect capacity limits.[1][2][3]
Guidelines (regional deltas)
NICE / APA / RANZCP-aligned practice prioritises CBT-informed psychological care for depression and anxiety disorders, early assessment of cognition and functioning in psychosis pathways, and recovery-oriented rehabilitation. Exact commissioning routes and tool kits differ by jurisdiction; quote local pathways in viva while keeping mechanism language shared.[8][12][15]
Subtypes and scenarios
| Scenario | Dominant cognitive levers |
|---|---|
| Major depression | Triad, distortions, rumination, overgeneral memory |
| Panic / health anxiety | Catastrophic misinterpretation; safety behaviours |
| Performance anxiety | ACT efficiency loss under executive load |
| OCD (cognitive content) | Threat overestimation; intolerance of uncertainty; fusion beliefs |
| PTSD | Intrusive episodic memory; appraisal bias; overgenerality |
| Schizophrenia | MATRICS domains; social cognition; functional prediction |
| Bipolar inter-episode | Residual attention/executive/memory complaints |
| ADHD | Sustained attention and executive control |
| Older adult clinic | Dual-task failure; dementia vs depression differential |
| Capacity / forensic | Heuristic traps under load; need for supported decision-making |
| Across scenarios, process models (attention bias, WM load, schema activation, social cognition) remap to protocol choice without inventing new disorders.[5][8][12][14] |
Complications and pitfalls
- IQ as total cognition — misses social cognition and specific domain profiles.
- Blame language for WM/executive failure (“non-compliant personality”).
- Over-reading one MoCA without culture, education, sensory, effort context.
- Verbal CBT only without experiments that test predictions.[9]
- Complex discharge instructions to patients at span capacity limits.[1][3]
- Ignoring social cognition when “symptoms improved” but relationships collapse.[14]
Prognosis and disposition
Cognitive impairment in schizophrenia is a relatively stable contributor to long-term function and vocational outcome; plan rehab early rather than waiting for perfect positive-symptom remission.[12][15] Residual cognitive symptoms after depression may lag mood recovery and impair problem-solving; booster CBT and memory-specificity work can be disposition levers.[8][11] Step up formal NP and intensive rehab when community function lags symptomatic improvement.
Special populations
- Children/adolescents: developmental norms; school as the attention/executive stress test.
- Older adults: hearing/vision confounds; medication anticholinergic load; NCD differential.
- Intellectual disability: change-from-baseline matters more than absolute scores; adapt communication.
- Cultural/linguistic minorities: interpreter standards; education-adjusted interpretation; avoid ethnocentric proverb tests.
- Indigenous contexts: culturally safe assessment; strengths-based formulation; community supports as external executive scaffolds. Developmental and cultural context changes which tasks are valid, not whether cognition matters.[5][14]
Evidence pearls (named)
- Miller 1956 — chunked capacity ~7±2.[1]
- Baddeley 2003 — multi-component working memory synthesis.[2]
- Cowan 2001 — focus-of-attention ~4.[3]
- Posner & Petersen 1990 — attention networks.[4]
- Miyake 2000 — updating, shifting, inhibition.[5]
- Tversky & Kahneman 1974 — representativeness, availability, anchoring.[6]
- Beck 1964/2008 — cognitive model of depression.[7][8]
- Clark 1986 — panic misinterpretation and safety behaviours.[9]
- Eysenck et al. 2007 — attentional control theory.[10]
- Williams et al. 2007 — overgeneral autobiographical memory.[11]
- Green 1996; Nuechterlein 2004; Green et al. 2008; Keefe & Harvey 2012 — schizophrenia cognition and social cognition lines.[12][13][14][15]
Exam pearls
A-WEMSS — cognitive domains viva map
- Miller chunks vs Cowan ~4 pure focus — both examinable.[1][3]
- Anxiety may spare effectiveness but tax efficiency under load.[10]
- Schizophrenia: cognition predicts function.[12]
- Safety behaviours protect the patient from learning they are safe.[9]
- Legal frameworks for involuntary treatment are jurisdiction-specific — do not invent section numbers; capacity still requires understanding, retention, weighing, and communication under real cognitive load.[2][5]
Summary
Master attention networks, Baddeley working memory, Miyake executive functions, dual-process heuristics, and the Beck/Clark clinical models. Map MATRICS-style and social-cognitive domains to disability in psychosis. Assess process at the bedside, exclude delirium, then deliver CBT experiments, compensation, and remediation with risk and capacity always in view. That combination is what fellowship examiners reward.[2][8][12][14]
References
- [1]Miller GA The magical number seven plus or minus two: some limits on our capacity for processing information Psychol Rev, 1956.PMID 13310704
- [2]Baddeley A Working memory: looking back and looking forward Nat Rev Neurosci, 2003.PMID 14523382
- [3]Cowan N The magical number 4 in short-term memory: a reconsideration of mental storage capacity Behav Brain Sci, 2001.PMID 11515286
- [4]Posner MI, Petersen SE The attention system of the human brain Annu Rev Neurosci, 1990.PMID 2183676
- [5]Miyake A, Friedman NP, Emerson MJ, et al. The unity and diversity of executive functions and their contributions to complex "Frontal Lobe" tasks: a latent variable analysis Cogn Psychol, 2000.PMID 10945922
- [6]Tversky A, Kahneman D Judgment under Uncertainty: Heuristics and Biases Science, 1974.PMID 17835457
- [7]Beck AT Thinking and depression. II. Theory and therapy Arch Gen Psychiatry, 1964.PMID 14159256
- [8]Beck AT The evolution of the cognitive model of depression and its neurobiological correlates Am J Psychiatry, 2008.PMID 18628348
- [9]Clark DM A cognitive approach to panic Behav Res Ther, 1986.PMID 3741311
- [10]Eysenck MW, Derakshan N, Santos R, Calvo MG Anxiety and cognitive performance: attentional control theory Emotion, 2007.PMID 17516812
- [11]Williams JM, Barnhofer T, Crane C, et al. Autobiographical memory specificity and emotional disorder Psychol Bull, 2007.PMID 17201573
- [12]Green MF What are the functional consequences of neurocognitive deficits in schizophrenia? Am J Psychiatry, 1996.PMID 8610818
- [13]Nuechterlein KH, Barch DM, Gold JM, et al. Identification of separable cognitive factors in schizophrenia Schizophr Res, 2004.PMID 15531405
- [14]Green MF, Penn DL, Bentall R, et al. Social cognition in schizophrenia: an NIMH workshop on definitions, assessment, and research opportunities Schizophr Bull, 2008.PMID 18184635
- [15]Keefe RS, Harvey PD Cognitive impairment in schizophrenia Handb Exp Pharmacol, 2012.PMID 23027411